
Neuroevolution of Convolutional Neural Networks for Breast Cancer Diagnosis Using Western Blot Strips

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Western Blot Strips Database
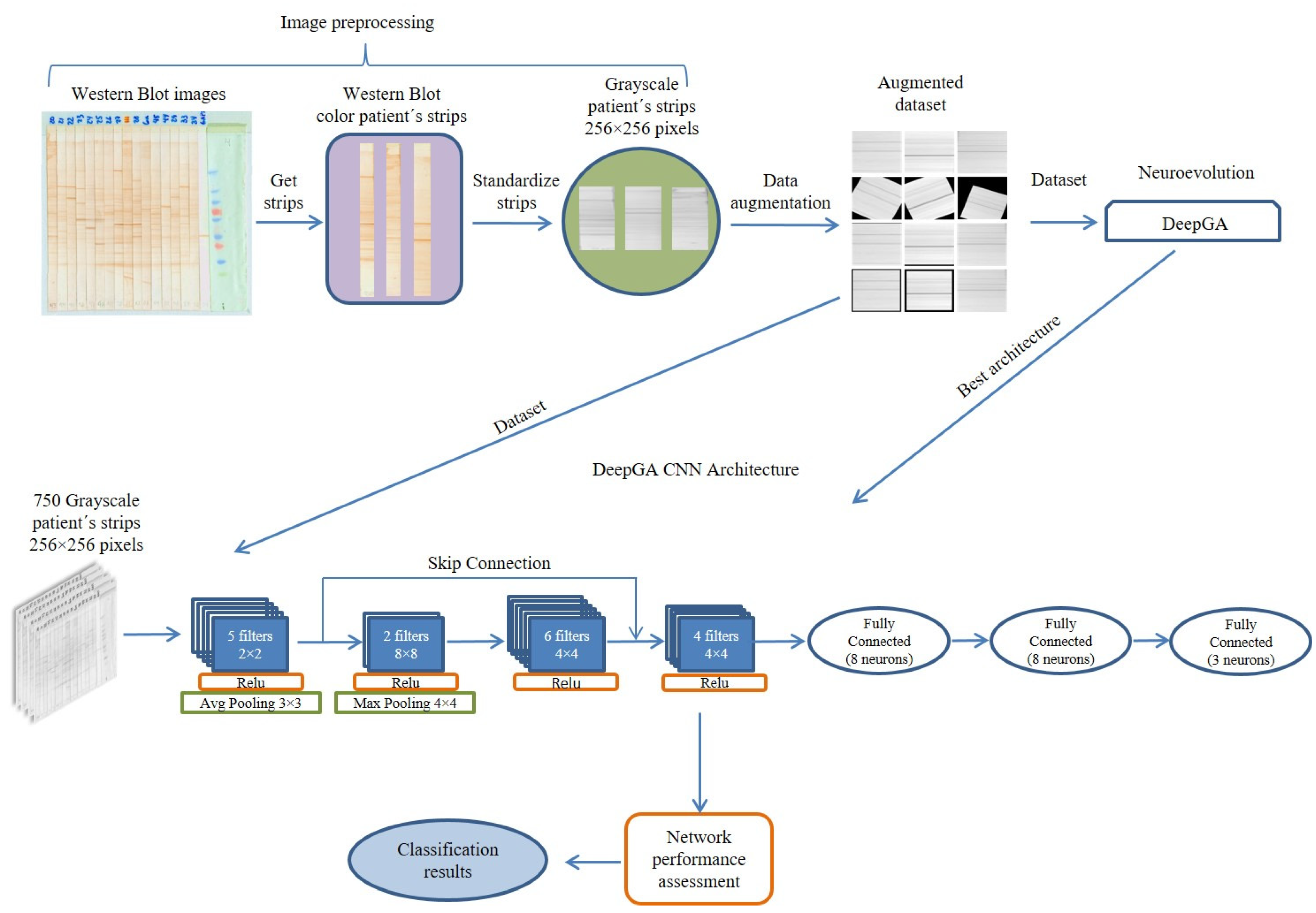
2.2. Image Preprocessing
2.3. Data Augmentation
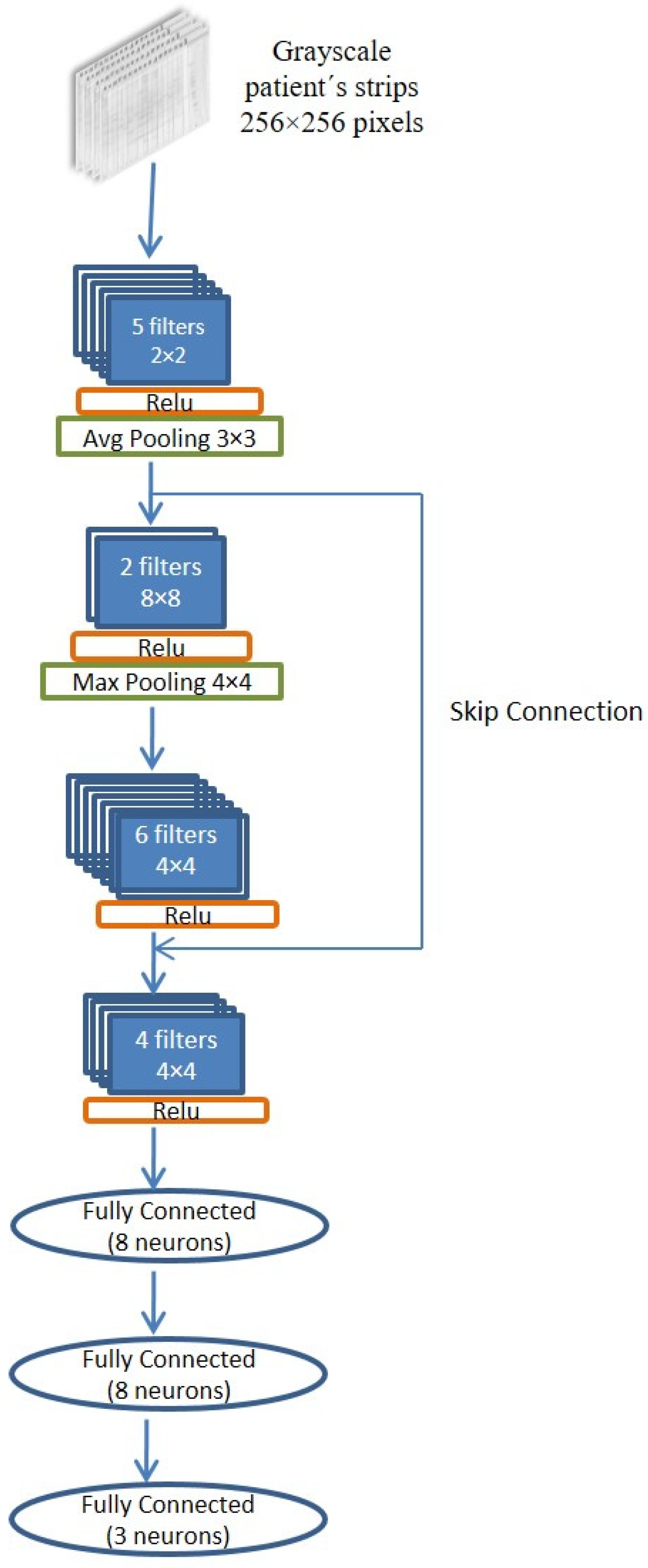
2.4. CNN Neuroevolution
2.5. Evaluation of the Convolutional Neural Network
2.6. Comparison and Statistical Analysis
3. Experimentation and Results
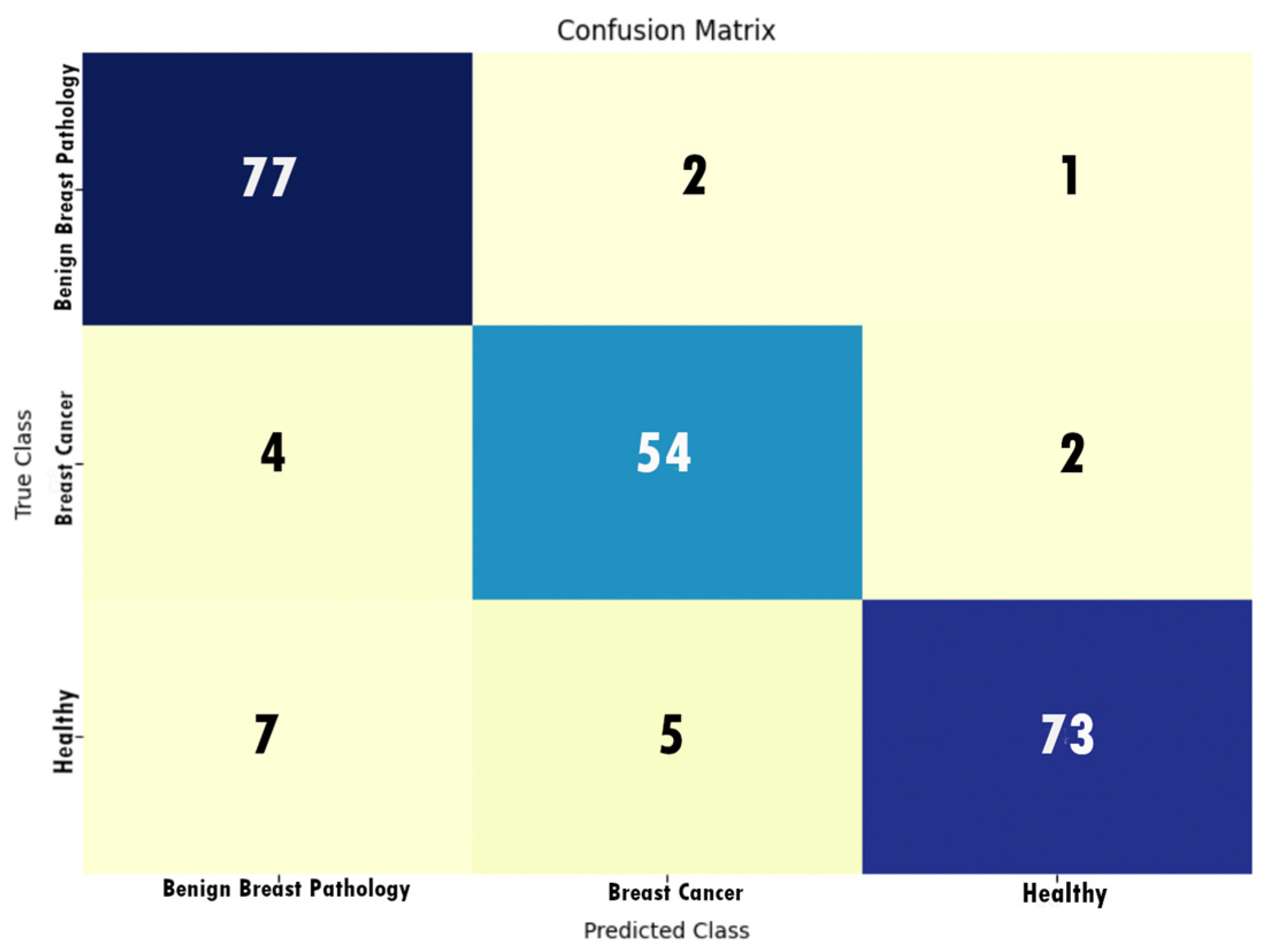
- The CNN obtained through the DeepGA neuroevolution algorithm (CNN-DeepGA) was trained, taking as input data the database of 750 Western blot strips; 250 belong to the class of healthy patients, 250 to the class of patients with benign pathology, and 250 to the class of patients with cancer. The parameters with which CNN-DeepGA was executed have been shown in Table 1;
- Training CNN-DeepGA consisted of only 10 epochs (as suggested by [30]); Adam’s optimizer was used with a learning rate of 1 × 10−4. For training, we used 70% of the data set (525 images out of 750 total), while accuracy/error was calculated using 30% (225 images out of 750 total) of the remaining set for testing;
- To evaluate the performance of CNN-DeepGA, 10 executions were carried out, obtaining the average and the standard deviation of the accuracy in each of the executions, as shown in Table 2;
- To handle biases, such as overfitting and underfitting, a data augmentation was performed by increasing the original size of examples for each class five times, going from 50 to 250 images in each class. On the other hand, the images were obtained in a controlled environment and an editing software program was used to improve them [11]. The hold-out technique was used for the evaluation of the model; 70% of the data were used for training the network and the remaining 30% for testing it;
- The performance of the Alexnet pretrained CNN [20] was tested with 150 Westen Blot strip images (50 healthy, 50 benign breast pathology, and 50 breast cancer). For the training consisting of 100 epochs, Adam’s optimizer was used with a learning range of 1 × 10−4. For the training set, 70% of the data set was used, while the accuracy/errors were calculated using 30% of the data set;
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Nájera, O.; Cahuana-Hurtado, L.; Ávila-Burgos, L. Costos de atención del cáncer de mama en el Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado, México. Salud Publica Mex. 2021, 63, 538–546. [Google Scholar] [CrossRef] [PubMed]
- Hablemos de El Cáncer de Mama. Available online: https://www.seom.org/seomcms/images/stories/recursos/infopublico/publicaciones/HABLEMOS_CANCER_MAMA.pdf (accessed on 15 February 2023).
- Torres-Arreola, L.d.P.; Vladislavovna Doubova, S.C.d.M. Detección Oportuna En El Primer Nivel de Atención. Rev. Méd. Inst. Mex. Seguro Soc. 2007, 45, 157–166. [Google Scholar] [PubMed]
- Lara-Tamburrino, M.d.C.; Tapia-Vega, A.X.; Quiróz-Rojas, L.Y. Integración de la imagen en la patología mamaria. Gac. Mex. Oncol. 2013, 12, 116–123. [Google Scholar]
- Cadavid-Fernández, N.; Carretero-Barrio, I.; Moreno-Moreno, E.; Rodríguez-Villena, A.; Palacios, J.; Pérez-Mies, B. The Role of Core Needle Biopsy in Diagnostic Breast Pathology. Rev. Senol. Patol. Mamar. 2022, 35, S3–S12. [Google Scholar] [CrossRef]
- Chávarri-Guerra, Y.; Villarreal-Garza, C.; Liedke, P.E.; Knaul, F.; Mohar, A.; Finkelstein, D.M.; Goss, P.E. Breast Cancer in Mexico: A Growing Challenge to Health and the Health System. Lancet Oncol. 2012, 13, e335–e343. [Google Scholar] [CrossRef]
- Brandan, M.E. Detección del Cáncer de Mama: Estado de la Mamografía en México. Rev. Inst. Nac. Cancerol. 2006, 27, 16. [Google Scholar]
- Chapman, C.; Murray, A.; Chakrabarti, J.; Thorpe, A.; Woolston, C.; Sahin, U.; Barnes, A.; Robertson, J. Autoantibodies in Breast Cancer: Their Use as an Aid to Early Diagnosis. Ann. Oncol. 2007, 18, 868–873. [Google Scholar] [CrossRef]
- Desmetz, C.; Lacombe, J.; Mange, A.; Maudelonde, T.; Solassol, J. Autoanticorps et diagnostic précoce des cancers. Med. Sci. 2011, 27, 633–638. [Google Scholar] [CrossRef]
- Romo-González, T.; Esquivel-Velázquez, M.; Ostoa-Saloma, P.; Lara, C.; Zentella, A.; León-Díaz, R.; Lamoyi, E.; Larralde, C. The Network of Antigen-Antibody Reactions in Adult Women with Breast Cancer or Benign Breast Pathology or without Breast Pathology. PLoS ONE 2015, 10, e0119014. [Google Scholar] [CrossRef]
- Yue, W.; Wang, Z.; Chen, H.; Payne, A.; Liu, X. Machine Learning with Applications in Breast Cancer Diagnosis and Prognosis. Designs 2018, 2, 13. [Google Scholar] [CrossRef]
- Mahoro, E.; Akhloufi, M.A. Applying Deep Learning for Breast Cancer Detection in Radiology. Curr. Oncol. 2022, 29, 8767–8793. [Google Scholar] [CrossRef] [PubMed]
- Nasser, M.; Yusof, U.K. Deep Learning Based Methods for Breast Cancer Diagnosis: A Systematic Review and Future Direction. Diagnostics 2023, 13, 161. [Google Scholar] [CrossRef]
- Sánchez-Silva, D.M.; Acosta-Mesa, H.G.; Romo-González, T. Semi-Automatic Analysis for Unidimensional Immunoblot Images to Discriminate Breast Cancer Cases Using Time Series Data Mining. Int. J. Patt. Recogn. Artif. Intell. 2018, 32, 1860004. [Google Scholar] [CrossRef]
- Llaguno-Roque, J.-L.; Barrientos-Martínez, R.-E.; Acosta-Mesa, H.-G.; Romo, T. Western Blot Pattern Classification Using Convolutional Neural Networks for Breast Cancer Diagnosis. In Proceedings of the 4th Workshop on New Trends in Computational Intelligence and Applications (CIAPP 2022), Monterrey, Mexico, 24 October 2022. [Google Scholar]
- Alanazi, S.A.; Kamruzzaman, M.M.; Islam Sarker, M.N.; Alruwaili, M.; Alhwaiti, Y.; Alshammari, N.; Siddiqi, M.H. Boosting Breast Cancer Detection Using Convolutional Neural Network. J. Healthc. Eng. 2021, 2021, 5528622. [Google Scholar] [CrossRef]
- Ekici, S.; Jawzal, H. Breast Cancer Diagnosis Using Thermography and Convolutional Neural Networks. Med. Hypotheses 2020, 137, 109542. [Google Scholar] [CrossRef] [PubMed]
- Yamlome, P.; Akwaboah, A.D.; Marz, A.; Deo, M. Convolutional Neural Network Based Breast Cancer Histopathology Image Classification. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; IEEE: Montreal, QC, Canada; pp. 1144–1147. [Google Scholar]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. ImageNet Classification with Deep Convolutional Neural Networks. Commun. ACM 2017, 60, 84–90. [Google Scholar] [CrossRef]
- Xu, Z.; Yang, Q.; Li, M.; Gu, J.; Du, C.; Chen, Y.; Li, B. Predicting HER2 Status in Breast Cancer on Ultrasound Images Using Deep Learning Method. Front. Oncol. 2022, 12, 829041. [Google Scholar] [CrossRef]
- Jabeen, K.; Khan, M.A.; Balili, J.; Alhaisoni, M.; Almujally, N.A.; Alrashidi, H.; Tariq, U.; Cha, J.-H. BC2NetRF: Breast Cancer Classification from Mammogram Images Using Enhanced Deep Learning Features and Equilibrium-Jaya Controlled Regula Falsi-Based Features Selection. Diagnostics 2023, 13, 1238. [Google Scholar] [CrossRef]
- Zhu, Z.; Wang, S.-H.; Zhang, Y.-D. A Survey of Convolutional Neural Network in Breast Cancer. Comput. Model. Eng. Sci. 2023, 136, 2127–2172. [Google Scholar] [CrossRef]
- Baldominos, A.; Saez, Y.; Isasi, P. Evolutionary Convolutional Neural Networks: An Application to Handwriting Recognition. Neurocomputing 2018, 283, 38–52. [Google Scholar] [CrossRef]
- Vargas-Hákim, G.-A.; Mezura-Montes, E.; Acosta-Mesa, H.-G. Hybrid Encodings for Neuroevolution of Convolutional Neural Networks: A Case Study. In Proceedings of the GECCO’21: Genetic and Evolutionary Computation Conference, Lille, France, 10–14 July 2021; Association for Computing Machinery: New York, NY, USA; pp. 1762–1770. [Google Scholar]
- Macdonald, I.K.; Parsy-Kowalska, C.B.; Chapman, C.J. Autoantibodies: Opportunities for Early Cancer Detection. Trends Cancer 2017, 3, 198–213. [Google Scholar] [CrossRef]
- Rauf, F.; Anderson, K.S.; LaBaer, J. Autoantibodies in Early Detection of Breast Cancer. Cancer Epidemiol. Biomark. Prev. 2020, 29, 2475–2485. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Han, Y.; Yi, W.; Long, Q. Autoantibodies as Biomarkers for Breast Cancer Diagnosis and Prognosis. Front. Immunol. 2022, 13, 1035402. [Google Scholar] [CrossRef] [PubMed]
- Stanley, K.O.; Clune, J.; Lehman, J.; Miikkulainen, R. Designing Neural Networks through Neuroevolution. Nat. Mach. Intell. 2019, 1, 24–35. [Google Scholar] [CrossRef]
- Sun, Y.; Xue, B.; Zhang, M.; Yen, G.G. Automatically Designing CNN Architectures Using Genetic Algorithm for Image Classification. IEEE Trans. Cybern. 2020, 50, 3840–3854. [Google Scholar] [CrossRef]
- Zhou, L.-Q.; Wu, X.-L.; Huang, S.-Y.; Wu, G.-G.; Ye, H.-R.; Wei, Q.; Bao, L.-Y.; Deng, Y.-B.; Li, X.-R.; Cui, X.-W.; et al. Lymph Node Metastasis Prediction from Primary Breast Cancer US Images Using Deep Learning. Radiology 2020, 294, 19–28. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Values |
|---|---|
| Population Size | 20 |
| Number of Generation | 50 |
| Crossover Rate | 0.7 |
| Mutation Rate | 0.5 |
| Tournament Size | 4 |
| Accuracy | |
|---|---|
| 1 | 95.83 |
| 2 | 94.82 |
| 3 | 94.76 |
| 4 | 83.33 |
| 5 | 87.77 |
| 6 | 87.50 |
| 7 | 83.48 |
| 8 | 87.50 |
| 9 | 91.67 |
| 10 | 100.00 |
| Average | 90.67 |
| Standard deviation | 5.60 |
| Executions | KNN Time Series-Geometric Scaling [15] | Handcrafted CNN [16] | Alexnet [20] | CNN-DeepGA |
|---|---|---|---|---|
| 1 | 71.11 | 68.89 | 50.00 | 95.83 |
| 2 | 66.66 | 66.67 | 45.95 | 94.82 |
| 3 | 62.22 | 64.44 | 54.05 | 94.76 |
| 4 | 64.44 | 68.89 | 39.19 | 83.33 |
| 5 | 64.44 | 62.22 | 45.95 | 87.77 |
| 6 | 60.50 | 64.44 | 48.65 | 87.50 |
| 7 | 71.11 | 71.11 | 55.41 | 83.48 |
| 8 | 60.50 | 66.67 | 54.05 | 87.50 |
| 9 | 68.88 | 66.67 | 55.41 | 91.67 |
| 10 | 64.44 | 64.44 | 45.95 | 100.00 |
| Average | 65.43 | 66.44 | 49.46 | 90.67 |
| Stand. Dev. | 3.94 | 2.66 | 5.34 | 5.60 |
| Factor | N | Average | Stand. Dev. | 95% CI |
|---|---|---|---|---|
| KNN | 10 | 65.43 | 3.94 | (62.52, 68.35) |
| Handcrafted-CNN | 10 | 66.44 | 2.662 | (63.531, 69.357) |
| Alexnet pretrained CNN | 10 | 49.46 | 5.34 | (46.55, 52.37) |
| CNN-DeepGA | 10 | 90.67 | 5.60 | (87.75, 93.58) |
| Metric | % |
|---|---|
| Accuracy | 90.67 |
| Recall | 90.71 |
| Specificity | 95.34 |
| Precision | 90.69 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Llaguno-Roque, J.-L.; Barrientos-Martínez, R.-E.; Acosta-Mesa, H.-G.; Romo-González, T.; Mezura-Montes, E. Neuroevolution of Convolutional Neural Networks for Breast Cancer Diagnosis Using Western Blot Strips. Math. Comput. Appl. 2023, 28, 72. https://doi.org/10.3390/mca28030072
Llaguno-Roque J-L, Barrientos-Martínez R-E, Acosta-Mesa H-G, Romo-González T, Mezura-Montes E. Neuroevolution of Convolutional Neural Networks for Breast Cancer Diagnosis Using Western Blot Strips. Mathematical and Computational Applications. 2023; 28(3):72. https://doi.org/10.3390/mca28030072
Chicago/Turabian StyleLlaguno-Roque, José-Luis, Rocio-Erandi Barrientos-Martínez, Héctor-Gabriel Acosta-Mesa, Tania Romo-González, and Efrén Mezura-Montes. 2023. "Neuroevolution of Convolutional Neural Networks for Breast Cancer Diagnosis Using Western Blot Strips" Mathematical and Computational Applications 28, no. 3: 72. https://doi.org/10.3390/mca28030072