
Recurrence or de novo? Intradermal Basal Cell Carcinoma of the Scrotum: A Report of Two Cases

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Presentation
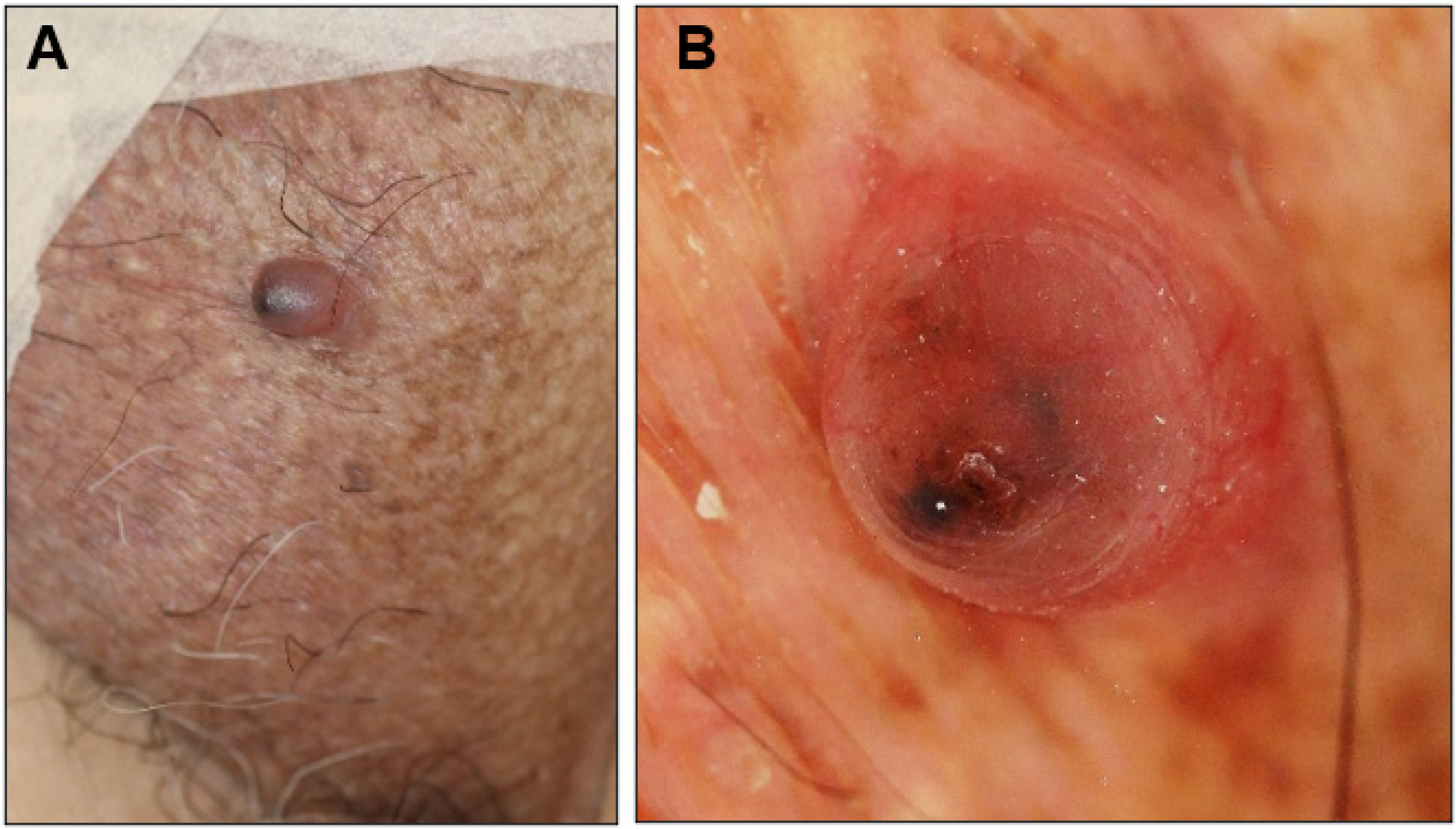
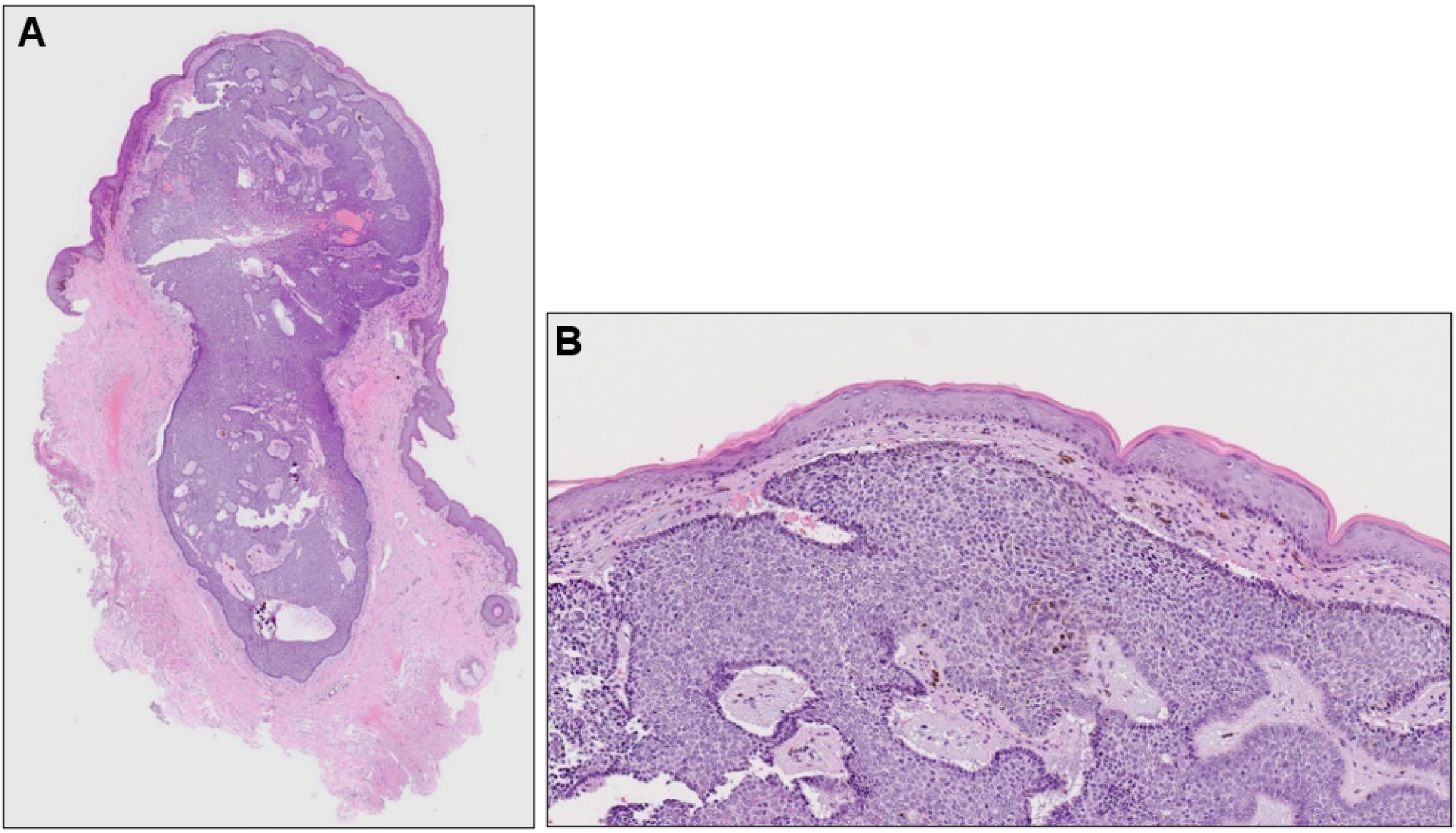
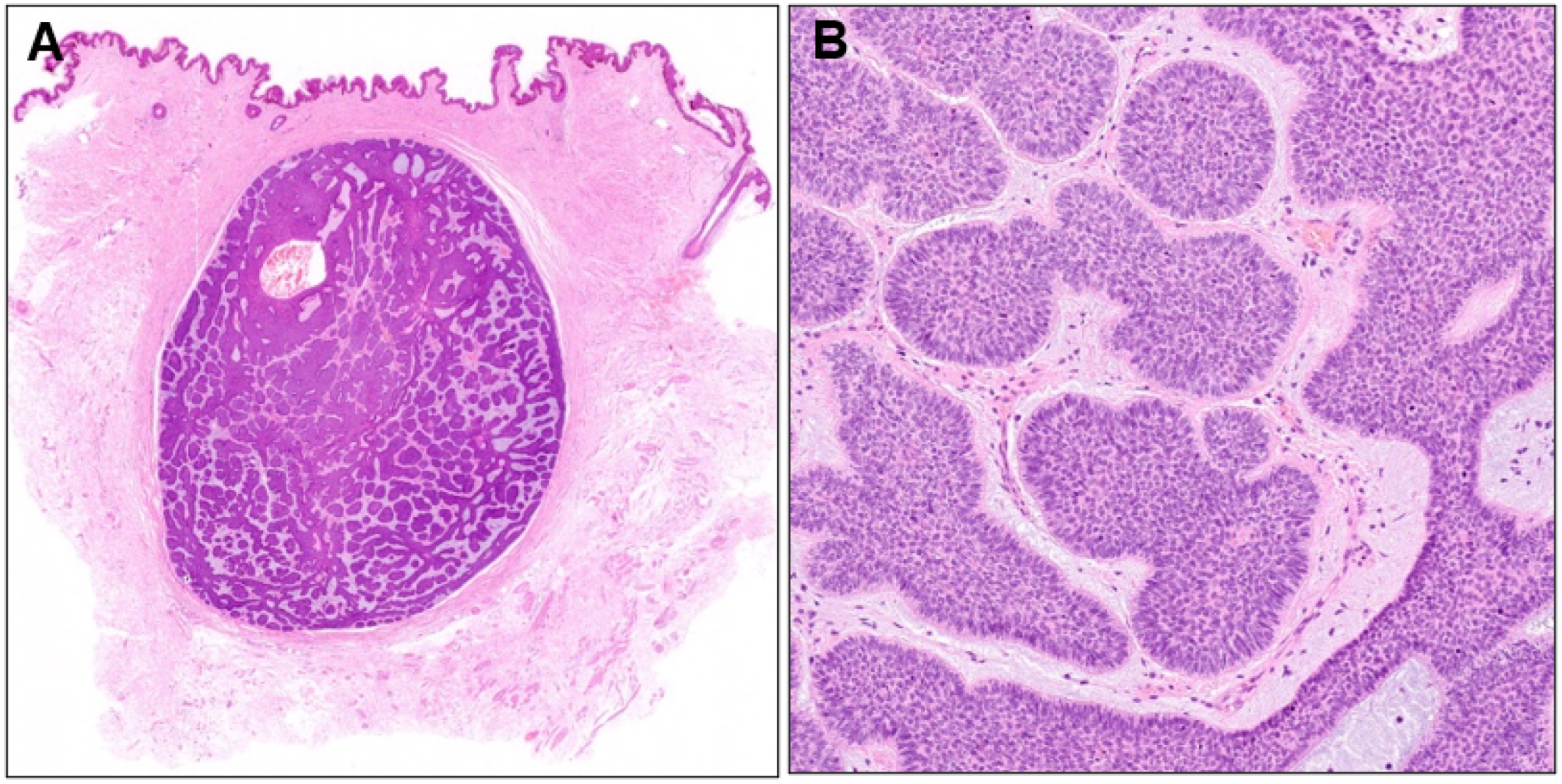
2.1. Case 1
2.2. Case 2
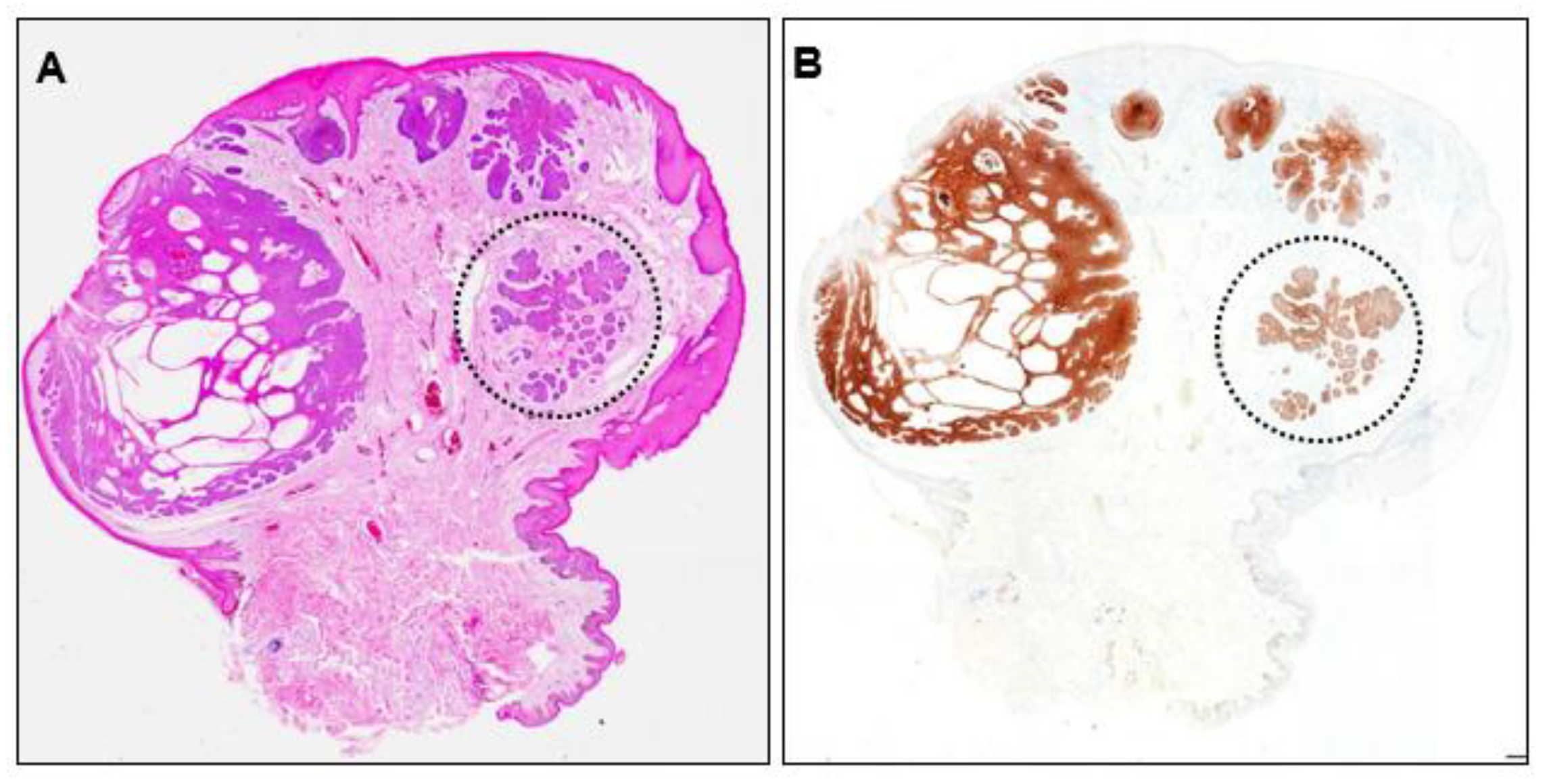
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cameron, M.C.; Lee, E.; Hibler, B.P.; Barker, C.A.; Mori, S.; Cordova, M.; Nehal, K.S.; Rossi, A.M. Basal cell carcinoma: Epidemiology; pathophysiology; clinical and histological subtypes; and disease associations. J. Am. Acad. Dermatol. 2019, 80, 303–317. [Google Scholar] [CrossRef] [Green Version]
- Rubin, A.I.; Chen, E.H. Basal cell carcinoma. N. Engl. J. Med. 2005, 353, 2262–2269. [Google Scholar] [CrossRef] [PubMed]
- Solimani, F.; Juratli, H.; Hoch, M.; Wolf, R.; Pfützner, W. Basal cell carcinoma of the scrotum: An important but easily overlooked entity. J. Eur. Acad. Dermatol. Venereol. 2018, 32, e254–e255. [Google Scholar] [CrossRef] [PubMed]
- Rahbari, H.; Mehregan, H.H. Basal Cell Epitheliomas in Usual and Unusual Sites. J. Cutan. Pathol. 1979, 6, 425–431. [Google Scholar] [CrossRef]
- Chen, X.; Hou, Y.; Chen, C.; Jiang, G. Basal Cell Carcinoma of the External Genitalia: A Population-Based Analysis. Front. Oncol. 2021, 10, 613533. [Google Scholar] [CrossRef]
- Verhoeven, R.H.A.; Aben, K.K.H.; van Rossum, M.M.; Reedijk, A.M.; Botterweck, A.A.; Veerbeek, L.; Visser, O.; van der Aa, M.A.; Ho, V.K.Y.; Coebergh, J.W.W.; et al. New insights into the aetiology of scrotal cancer, a nationwide case-control study in the Netherlands. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Dai, B.; Kong, Y.Y.; Ye, D.W.; Xu, X.W.; Yao, X.D.; Zhang, S.L. Basal Cell Carcinoma of the Scrotum: Clinicopathologic Analysis of 10 Cases. Dermatol. Surg. 2012, 38, 783–790. [Google Scholar] [CrossRef]
- Sexton, M.; Jones, D.B.; Maloney, M.E. Histologic pattern analysis of basal cell carcinoma: Study of a series of 1039 consecutive neoplasms. J. Am. Acad. Dermatol. 1990, 23, 1118–1126. [Google Scholar] [CrossRef]
- Reiter, O.; Mimouni, I.; Gdalevich, M.; Marghoob, A.A.; Levi, A.; Hodak, E.; Leshem, Y.A. The diagnostic accuracy of dermoscopy for basal cell carcinoma: A systematic review and meta-analysis. J. Am. Acad. Dermatol. 2019, 80, 1380–1388. [Google Scholar] [CrossRef]
- Reiter, O.; Mimouni, I.; Dusza, S.; Halpern, A.C.; Leshem, Y.A.; Marghoob, A.A. Dermoscopic features of basal cell carcinoma and its subtypes: A systematic review. J. Am. Acad. Dermatol. 2021, 85, 653–664. [Google Scholar] [CrossRef]
- Niculet, E.; Craescu, M.; Rebegea, L.; Bobeica, C.; Nastase, F.; Lupasteanu, G.; Stan, D.J.; Chioncel, V.; Anghel, L.; Lungu, M.; et al. Basal cell carcinoma: Comprehensive clinical and histopathological aspects, novel imaging tools and therapeutic approaches (Review). Exp. Ther. Med. 2022, 23, 60. [Google Scholar] [CrossRef] [PubMed]
- Messina, J.; Epstein, E.H.J.; Kossard, S.; McKenzie, C.; Patel, R.M.; Patterson, J.W.; Scolyer, R.A. Basal cell carcinoma. In WHO Classification of Skin Tumors; Elder, D.E., Massi, D., Scolyer, R.A., Willemze, R., Eds.; WHO Press: Geneva, Switzerland, 2018; pp. 26–34. [Google Scholar]
- Esquivias Gomez, J.I.; Gonzalez-Lopez, A.; Velasco, E.; Pozo, T.; Del Villar, A. Basal cell carcinoma of the scrotum. Australas. J. Dermatol. 1999, 40, 141–143. [Google Scholar] [CrossRef] [PubMed]
- Younes, M.; Kouba, L.; Almsokar, H.; Badran, A. Micronodular basal cell carcinoma of the scrotum: A case report and review of the literature. J. Med. Case Rep. 2021, 15, 1–5. [Google Scholar] [CrossRef]
- Kinoshita, R.; Yamamoto, O.; Yasuda, H.; Tokura, Y. Basal cell carcinoma of the scrotum with lymph node metastasis: Report of a case and review of the literature. Int. J. Dermatol. 2005, 44, 54–56. [Google Scholar] [CrossRef]
- Lara, F.; Santamaría, J.R.; de Melo Garbers, L.E.F. Recurrence rate of basal cell carcinoma with positive histopathological margins and related risk factors. An. Bras. Dermatol. 2017, 92, 58–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkham, N.; Low, S.E.; Aljefri, K. Basal cell carcinoma. In Lever’s Dermatopathology: Histopathology of the Skin; Elder, D.E., Ed.; Wolters Kluwer Health: Lake Cook Road Riverwoods, IL, USA, 2023; pp. 989–1001. [Google Scholar]
- Lever, W.F. Pathogenesis of benign tumors of cutaneous appendages and of basal cell epithelioma: I. Benign tumors of the cutaneous appendages. Arch. Dermatol. Syphilol. 1948, 57, 679–708. [Google Scholar] [CrossRef]
- Pinkus, H. Premalignant fibroepithelial tumors of skin. Arch. Dermatol. Syphilol. 1953, 67, 598–615. [Google Scholar] [CrossRef] [PubMed]
- Youssef, K.K.; Van Keymeulen, A.; Lapouge, G.; Beck, B.; Michaux, C.; Achouri, Y.; Sotiropoulou, P.A.; Blanpain, C. Identification of the cell lineage at the origin of basal cell carcinoma. Nat. Cell Biol. 2010, 12, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.Y.; Wang, J.; Mancianti, M.-L.; Epstein, E.H. Basal Cell Carcinomas Arise from Hair Follicle Stem Cells in Ptch1+/− Mice. Cancer Cell 2011, 19, 114–124. [Google Scholar] [CrossRef] [Green Version]
- Peterson, S.C.; Eberl, M.; Vagnozzi, A.N.; Belkadi, A.; Veniaminova, N.A.; Verhaegen, M.E.; Bichakjian, C.K.; Ward, N.L.; Dlugosz, A.A.; Wong, S.Y. Basal Cell Carcinoma Preferentially Arises from Stem Cells within Hair Follicle and Mechanosensory Niches. Cell Stem Cell 2015, 16, 400–412. [Google Scholar] [CrossRef] [Green Version]
- Sellheyer, K.; Krahl, D. Basal cell (trichoblastic) carcinoma: Common expression pattern for epithelial cell adhesion molecule links basal cell carcinoma to early follicular embryogenesis, secondary hair germ, and outer root sheath of the vellus hair follicle: A clue to the adnexal nature of basal cell carcinoma? J. Am. Acad. Dermatol. 2008, 58, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Camela, E.; Anca, P.I.; Lallas, K.; Papageorgiou, C.; Manoli, S.-M.; Gkentsidi, T.; Eftychidou, P.; Liopyris, K.; Sgouros, D.; Apalla, Z.; et al. Dermoscopic Clues of Histopathologically Aggressive Basal Cell Carcinoma Subtypes. Medicina 2023, 59, 349. [Google Scholar] [CrossRef] [PubMed]
- Yerly, L.; Pich-Bavastro, C.; Di Domizio, J.; Wyss, T.; Tissot-Renaud, S.; Cangkrama, M.; Gilliet, M.; Werner, S.; Kuonen, F. Integrated multi-omics reveals cellular and molecular interactions governing the invasive niche of basal cell carcinoma. Nat. Commun. 2022, 13, 4897. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamazaki, K.; Maejima, M.; Saeki, H.; Osada, S.-I. Recurrence or de novo? Intradermal Basal Cell Carcinoma of the Scrotum: A Report of Two Cases. Dermatopathology 2023, 10, 128-135. https://doi.org/10.3390/dermatopathology10020019
Yamazaki K, Maejima M, Saeki H, Osada S-I. Recurrence or de novo? Intradermal Basal Cell Carcinoma of the Scrotum: A Report of Two Cases. Dermatopathology. 2023; 10(2):128-135. https://doi.org/10.3390/dermatopathology10020019
Chicago/Turabian StyleYamazaki, Kaori, Maho Maejima, Hidehisa Saeki, and Shin-Ichi Osada. 2023. "Recurrence or de novo? Intradermal Basal Cell Carcinoma of the Scrotum: A Report of Two Cases" Dermatopathology 10, no. 2: 128-135. https://doi.org/10.3390/dermatopathology10020019