2. Materials and Methods
This Institutional Review Board (IRB)-approved study was based on a retrospective analysis of archival tissue. Surgical pathology specimens diagnosed with “microcystic adnexal carcinoma”, “eccrine carcinoma”, “hidradenocarcinoma”, “porocarcinoma”, “hidradenoma”, “poroma”, “cylindroma”, “spiradenoma”, and “syringoma” between 1 January 2005 and 31 December 2018 were selected for review. All selected cases were diagnosed by the dermatopathologists in our institution. The cases were reviewed by the authors for inclusion, with 10 eccrine carcinomas identified and recategorized based on histologic findings of the authors. Of these cases, 1 was defined as eccrine carcinoma not otherwise specified (NOS). Overall, 5 cases of microcystic adnexal carcinoma (MAC), 3 cases of eccrine adenocarcinoma, 2 cases of syringoid eccrine carcinoma, 4 cases of hidradenocarcinoma, 6 cases of porocarcinoma, 1 case of eccrine carcinoma NOS, 11 cases of hidradenoma, 9 cases of poroma, 7 cases of cylindroma, 3 cases of spiradenoma, and 10 cases of syringoma were included in this study.
Immunohistochemical studies were performed on 4 µm sections of formalin-fixed, paraffin-embedded tissue using a Leica Bond III instrument. The IHC assay consisted of a rabbit monoclonal antibody against human TRPS1 (clone EPR16171 from Abcam). Antigen retrieval was performed with Bond Solution #2 (pH 9.0). TRPS1 antibody with dilution 1:6000 was incubated for 8 min at room temperature. Tissue staining was performed on a Leica BOND III immunostainer with a Leica Refine Polymer Detection Kit. A breast carcinoma HER2 control kit was used as an external positive control for TRPS1.
The positivity of TRPS1 was defined as dark-brown nuclear staining. The percentage of immunoreactive cells was graded as follows: 0, <1%; 1, 1–10%; 2, 11–50%; 3, 51–100%. Staining intensity was graded as follows: 0, negative; 1, weak; 2, moderate; 3, strong. Immunoreactivity scores were calculated by multiplying the number corresponding to the percentage of immunoreactive cells by the number corresponding to staining intensity. The immunoreactivity scores were reported as negative (0–1), low positive (2), intermediate positive (3–4), or high positive (6 and 9) for TRPS1 expression [
5]. If more than one intensity group was present with different percentages, the highest score was given to those cases. Cylindroma and spiradenoma cases were not subjected to the reporting system due to their unique staining patterns.
3. Results
We evaluated TRPS1 IHC staining in a total of 61 skin biopsy specimens and report 51 of them based on the above criteria (
Table 1).
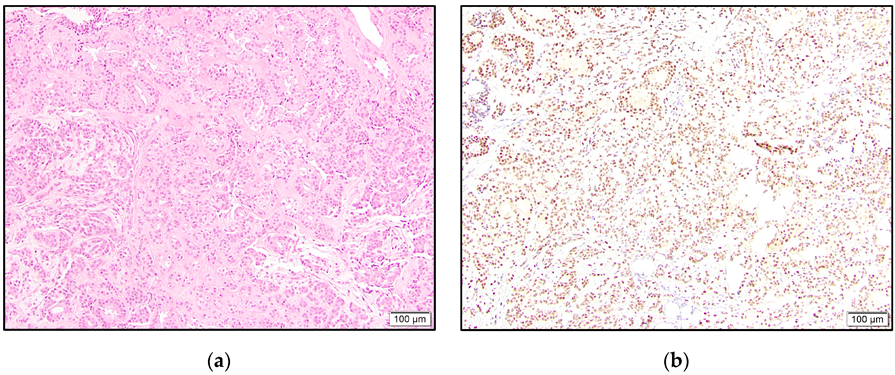
In the malignant tumors, all three eccrine adenocarcinomas showed intermediate to high positivity (
Figure 1). One of these cases revealed accentuated staining of the cells lining ductular spaces. The eccrine carcinoma NOS case was high positive.
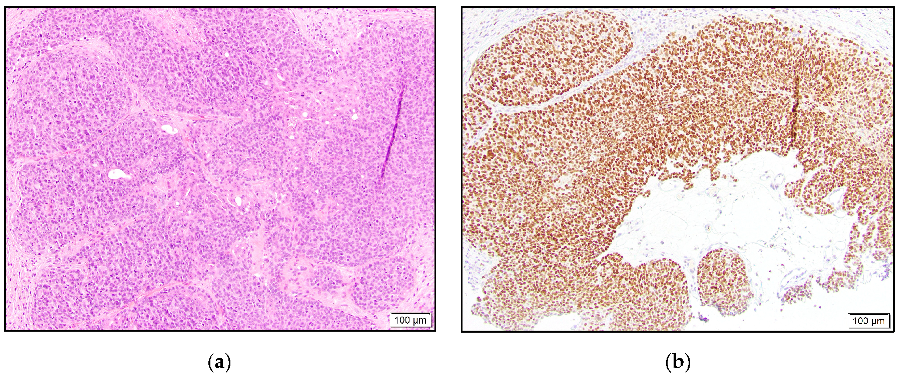
Of the two syringoid eccrine carcinomas, one was intermediate positive, and the other case was negative. Three of our hidradenocarcinomas were high positive (
Figure 2), and one case was negative for TRPS1 staining.
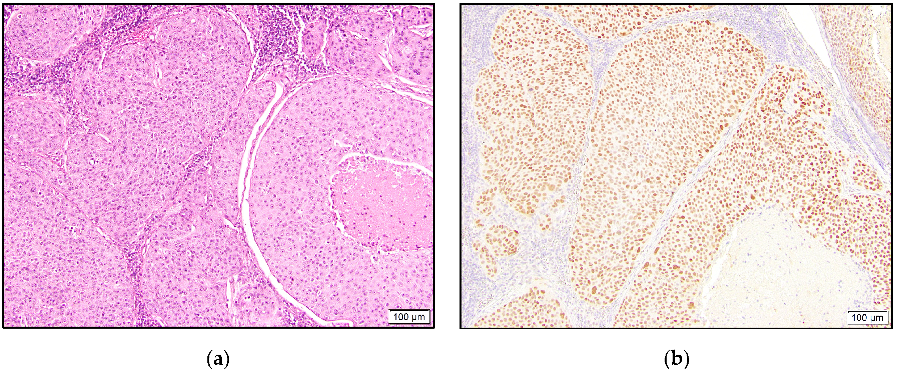
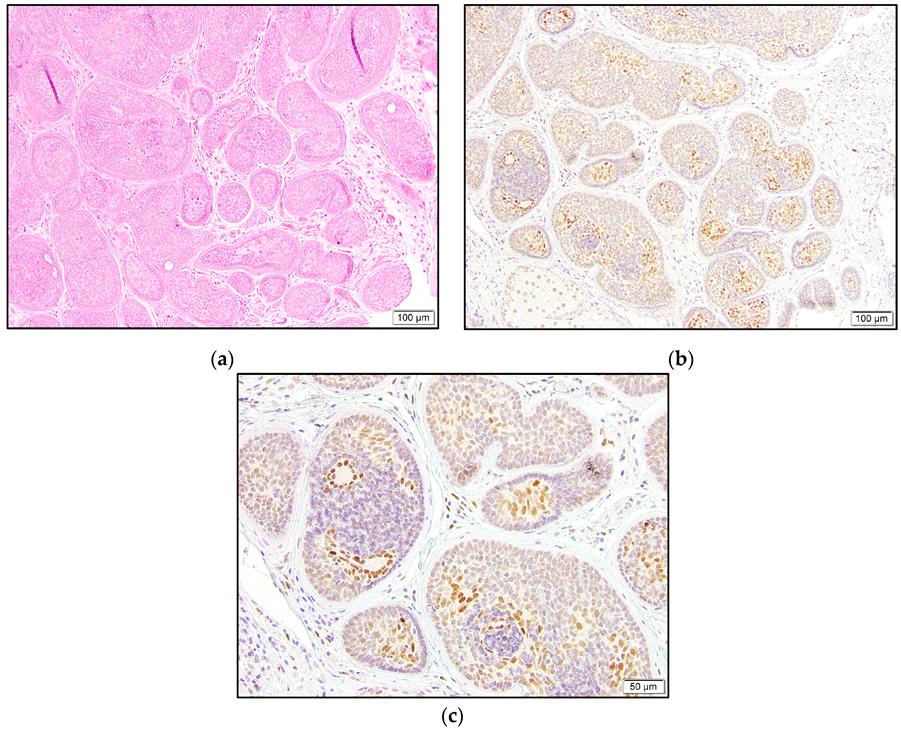
In the porocarcinoma group, all six cases demonstrated TRPS1 expression, with five being intermediate to high positive (
Figure 3).
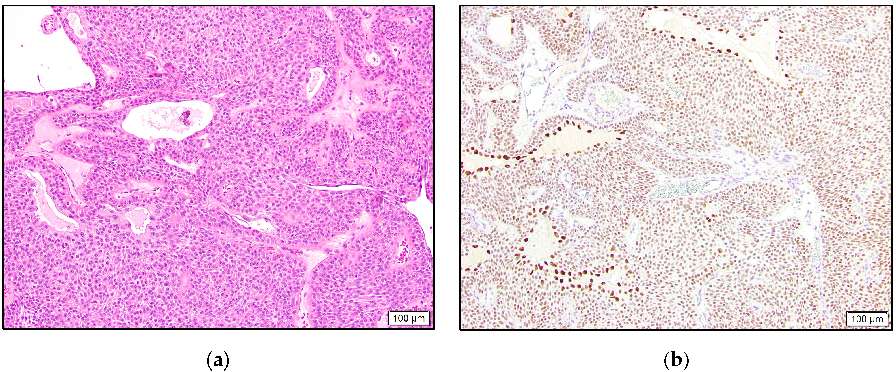
In the benign category, eight hidradenoma cases were intermediate to high positive, one was low positive, and two were negative. Similar to the eccrine adenocarcinoma case, four hidradenomas showed stronger staining in the cells lining cystic or ductular spaces (
Figure 4).
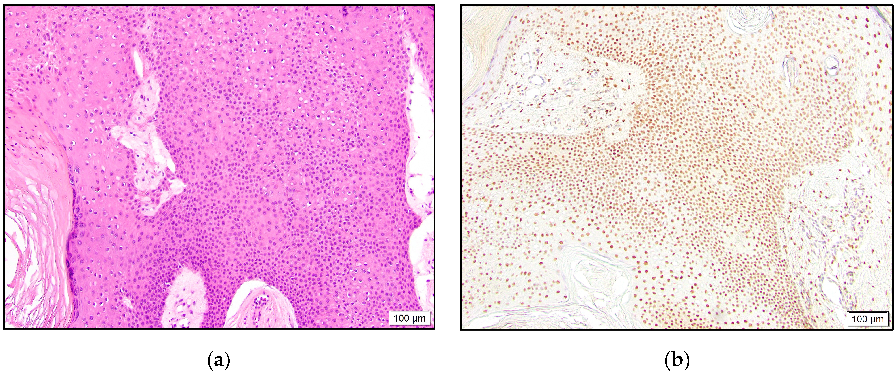
In the poroma group, six and two cases demonstrated intermediate to high and low positivity, respectively (
Figure 5). One poroma was negative for TRPS1 expression. In the majority of the positive cases, variable staining intensity was present in the tumor cells. This finding was more evident in the hidradenomas.
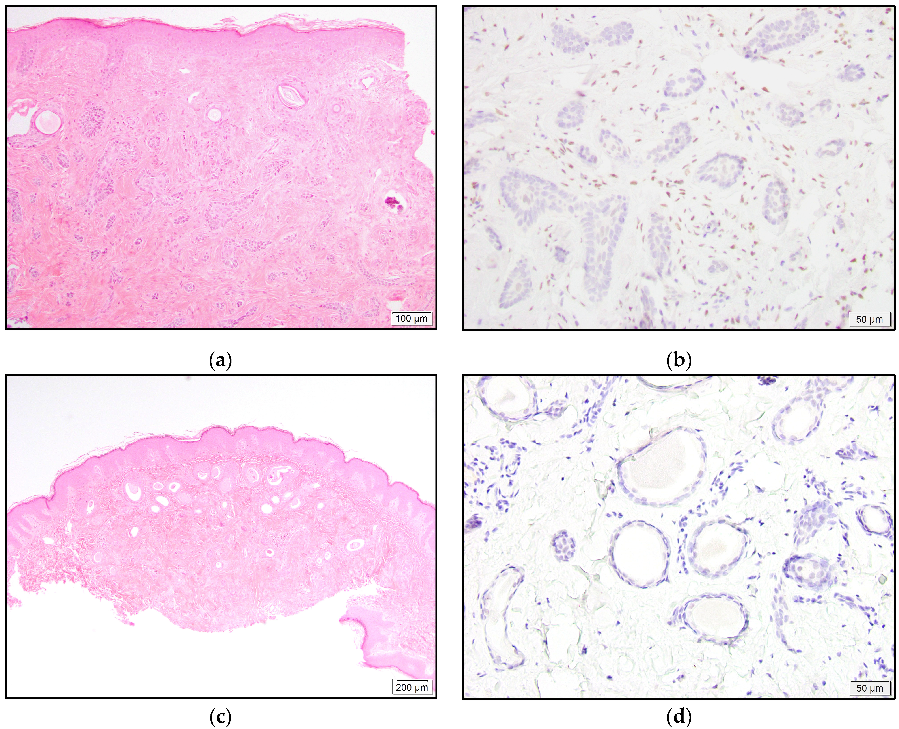
All MAC and syringoma cases were negative for TRPS1 expression (
Figure 6).
The majority of the cylindroma and spiradenoma cases showed distinctive staining patterns and were not categorized by the abovementioned reporting system. Only one spiradenoma was completely negative. The remaining two spiradenomas and all seven cylindromas revealed the strongest staining in the luminal cells and relatively weaker or negative staining in the surrounding neoplastic cells. The outermost layer with palisading cells was mostly negative for TRPS1 expression (
Figure 7).
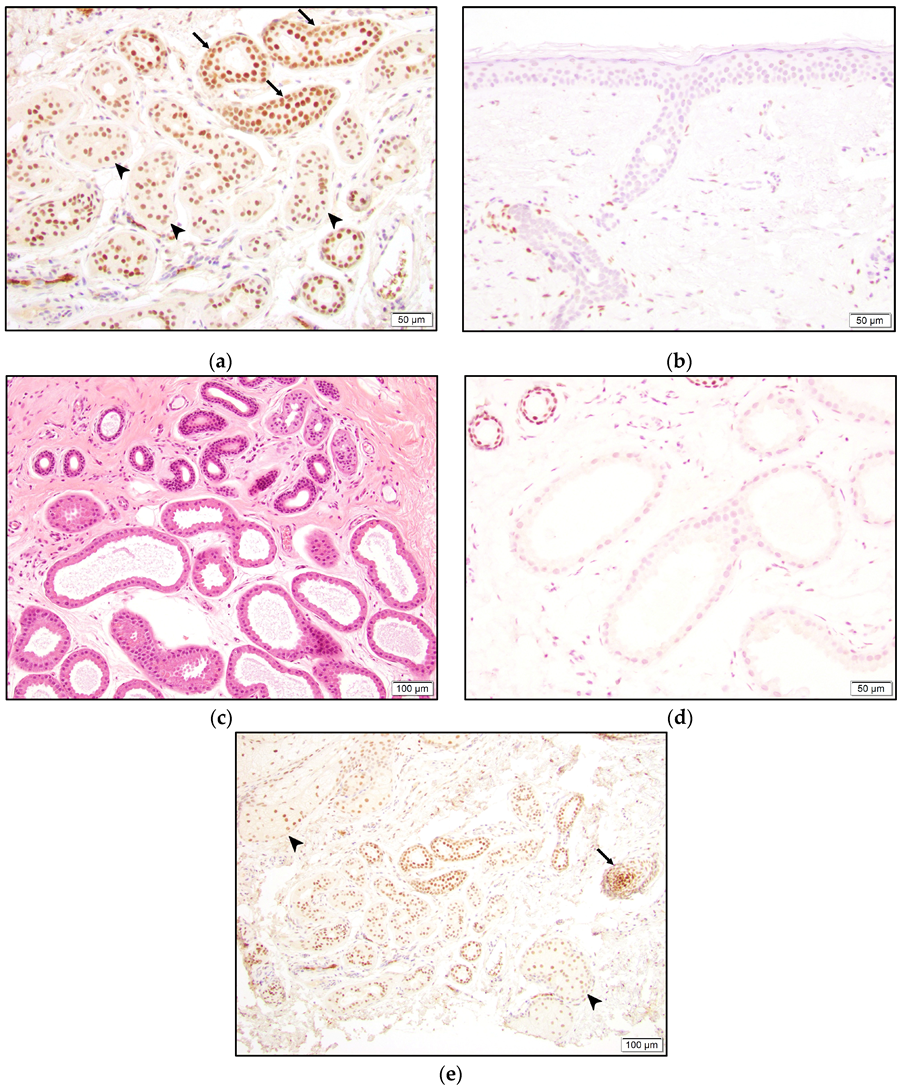
TRPS1 staining was also observed in normal structures. The inner cell layer of the eccrine gland secretory coils and the two cell layers of the eccrine ducts were positive for TRPS1. Ductular cells seemed to stain darker than secretory cells (
Figure 8). However, acrosyringium was negative for TRPS1 expression (
Figure 8). Interestingly, the apocrine glands did not stain with TRPS1 (
Figure 8). Strong staining was also present in hair follicles, especially in the bulb and papillary mesenchymal bodies (dermal papilla). Additionally, the majority of the squamous epithelium, sebaceous glands, and fibroblasts, mainly around hair follicles, demonstrated staining to varying intensities (
Figure 8).
4. Discussion
Poroma and syringoma are categorized as benign eccrine SGTs [
6]. Hidradenoma represents a “nosological jungle” and comprises both eccrine- and apocrine-originated tumors [
7]. Cylindroma and spiradenoma are benign tumors with debatable eccrine gland or hair follicle origin [
6,
8]. Eccrine carcinomas (malignant SGTs) include syringoid eccrine carcinoma, eccrine adenocarcinoma, hidradenocarcinoma, porocarcinoma, and MAC, among others [
6]. These entities exhibit distinct histologic features [
7]. Excluding syringoma and MAC, the remaining tumors generally comprise single or multiple islands or nodules of round to polygonal cells with basophilic, eosinophilic, or clear cytoplasm [
7]. Syringoma and MAC both show strands or cords of cells, often with duct formation described as “tadpole” in shape [
7].
Malignant SGTs constitute the biggest pitfall in diagnosing CMBC [
2]. TRPS1 IHC was reported to show reactivity with breast carcinoma [
5]. Our study demonstrates a very high expression of TRPS1 in eccrine carcinomas other than MAC (88% overall; 81% intermediate to high positive). Although we used a different IHC clone than that in a previous study [
5], our findings show that TRPS1 is possibly not helpful in differentiating malignant eccrine tumors from CMBC. Another malignant SGT, MAC, did not show TRPS1 expression in any cases. Nevertheless, MAC is less likely to be in the differential of CMBC.
Eccrine glands comprise secretory coils and sweat ducts, which are further divided into intraglandular, intradermal, and intraepidermal (acrosyringium) segments [
9,
10]. The secretory coil comprises two main cell types: inner secretory cells and outer myoepithelial cells [
9]. CK7 is known to be a secretory cell-specific marker, while SMA (more sensitive) and CD10 selectively stain myoepithelial cells [
11]. On the other hand, sweat ducts are lined by two cell layers and show a different IHC profile compared to coils with CK6 and CK10 expressions [
11]. A comprehensive report on keratin expression in eccrine sweat glands also revealed divergent, complex keratin patterns in the various tissue units of the sweat gland [
10]. Each unit of the eccrine sweat gland, including the segments of the sweat duct, expresses at least one keratin family member that serves as a tissue-specific marker [
10]. One can conclude that differential expression of other antigens can be expected in each segment of the sweat duct and secretory coil. In this study, we observed TRPS1 positivity in secretory cells and (slightly stronger) in the two duct cell layers. However, acrosyringium appeared to be negative.
Eccrine tumors arise from secretory coils and/or ducts. There are multiple studies in the literature focusing on the derivation and differentiation of benign eccrine tumors with variable IHC stains [
11,
12,
13,
14]. In hidradenomas, both luminal cells and peripheral polygonal cells have shown concomitant secretory coil and inner ductular cell differentiation [
12]. The differentiation has shown to be more conspicuous in luminal cells [
12]. In this study, a total of nine hidradenoma cases, with eight intermediate to high positive, expressed TRPS1. We observed a more discernable spectrum of staining intensity among tumor cells in hidradenoma, which is possibly consistent with both secretory (weaker) and ductular (stronger) cell differentiation. In four cases, accentuated staining was prominent in either the entire or the majority of luminal cells, which may suggest relatively selective ductular differentiation in these areas. Myoepithelial cells are favored not to be involved in this entity [
12,
14]. Because myoepithelial cells are negative for expression, the TRPS1 stain does not contribute to this discussion.
A previous study on the differentiation of poromas showed ductular-type staining (CK6 and CK10) of luminal cells within the tumor but failed to identify the origin of peripheral cells [
11]. A more comprehensive study proposed that poromas mainly arise from or differentiate towards the outer cells of eccrine ducts [
12]. The authors also hypothesized inner ductular cell or secretory cell differentiation during lumen formation based on the IHC panel used [
12]. Multiple studies have agreed on the absence of myoepithelial cells in poromas [
11,
12,
13]. In this study, the percentage of TRPS1-positive cases was highest in poromas (~90% in total). However, we did not notice any specific staining pattern to be able to comment on particular differentiations. This finding may be in keeping with the relatively exclusive differentiation towards outer ductular cells.
Cylindromas and spiradenomas display similar histologic and immunohistochemical features [
11,
12]. Some authors consider these two entities morphological variants of the same tumor [
15]. Although their origin is debatable, data that support eccrine lineage mostly indicate ductular differentiation in luminal cells and secretory coil differentiation in the surrounding neoplastic cells [
11,
12]. Multiple studies have shown myoepithelial marker expression at the periphery of tumors, especially in the outermost palisading cells [
12,
13,
14]. Although Missall et al. failed to show myoepithelial differentiation in cylindromas and spiradenomas, they reported negative staining of peripheral and palisading cells with multiple secretory coil and duct markers [
11]. In our study, luminal cells revealed stronger staining compared to the remaining tumor cells in all cylindromas and two spiradenomas. We also observed negative TRPS1 expression with peripheral arrangement in the majority of cases, which suggests possible myoepithelial or, at least, non-eccrine lineage in those cells. Considering the mild intensity difference between the secretory coil and ductal cells, our staining pattern also supports ductular differentiation in luminal cells and secretory coil differentiation in surrounding cells. On the other hand, another study showed hair-follicle stem cell marker expression in cylindromas and spiradenomas and postulated that these tumors originate from bulges in the hair follicle region [
8]. Our study revealed TRPS1 positivity in hair follicles and potentially indicates follicular differentiation in these entities as well.
Syringomas and MACs show similar histologic findings and are commonly in each other’s differentials [
7]. Syringomas are believed to derive from or differentiate towards eccrine ducts due to their staining pattern [
11,
12]. In contrast, MACs are known to express CK7 in luminal cells and SMA in peripheral cells, which suggests a secretory coil origin [
16]. Although we demonstrate TRPS1 staining in secretory cells and in ductular cell layers, none of our syringomas or MACs were positive for the expression. Alternatively, these two tumors may arise from the acrosyringium, which also showed negative expression of TRPS1. A consistent lack of TRPS1 staining in these entities may suggest a loss of expression during the neoplastic process. However, syringomas and MACs are well-differentiated tumors, which calls this hypothesis into question. A different cell of origin, such as myoepithelial cells, may also explain our findings, especially for MACs. Yet this theory seems to be less likely in syringomas, as multiple studies have shown the absence of myoepithelial differentiation by various markers [
11,
12,
13].
Mammary glands are often defined as “modified” apocrine glands. In light of normal TRPS1 staining in benign breast luminal cells [
5] and eccrine ducts, its negative expression in apocrine glands was an unexpected finding. Because the
TRPS1 gene is known to be important for the growth and differentiation of normal mammary epithelial cells, this gene may be the actor behind the “modification”. Nonetheless, this differential staining will pave the way for a more detailed investigation of sweat gland tumor origins. It may also help in the differentiation of CMBC from apocrine sweat gland tumors.
Lastly, the TRPS1 gene is known to be important in hair follicle development, and its expression was previously shown in the dermal papilla and the mesenchymal cells surrounding the hair follicle in murinae [
17]. Our study also shows TRPS1 expression in the dermal papilla and dermal mesenchymal cells, especially adjacent to hair follicles, and in the bulb of the hair follicle in humans.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}