

An Integrated Approach to Addictive Behaviors: A Study on Vulnerability and Maintenance Factors
 , , , and
, , , and
Abstract
:1. Introduction
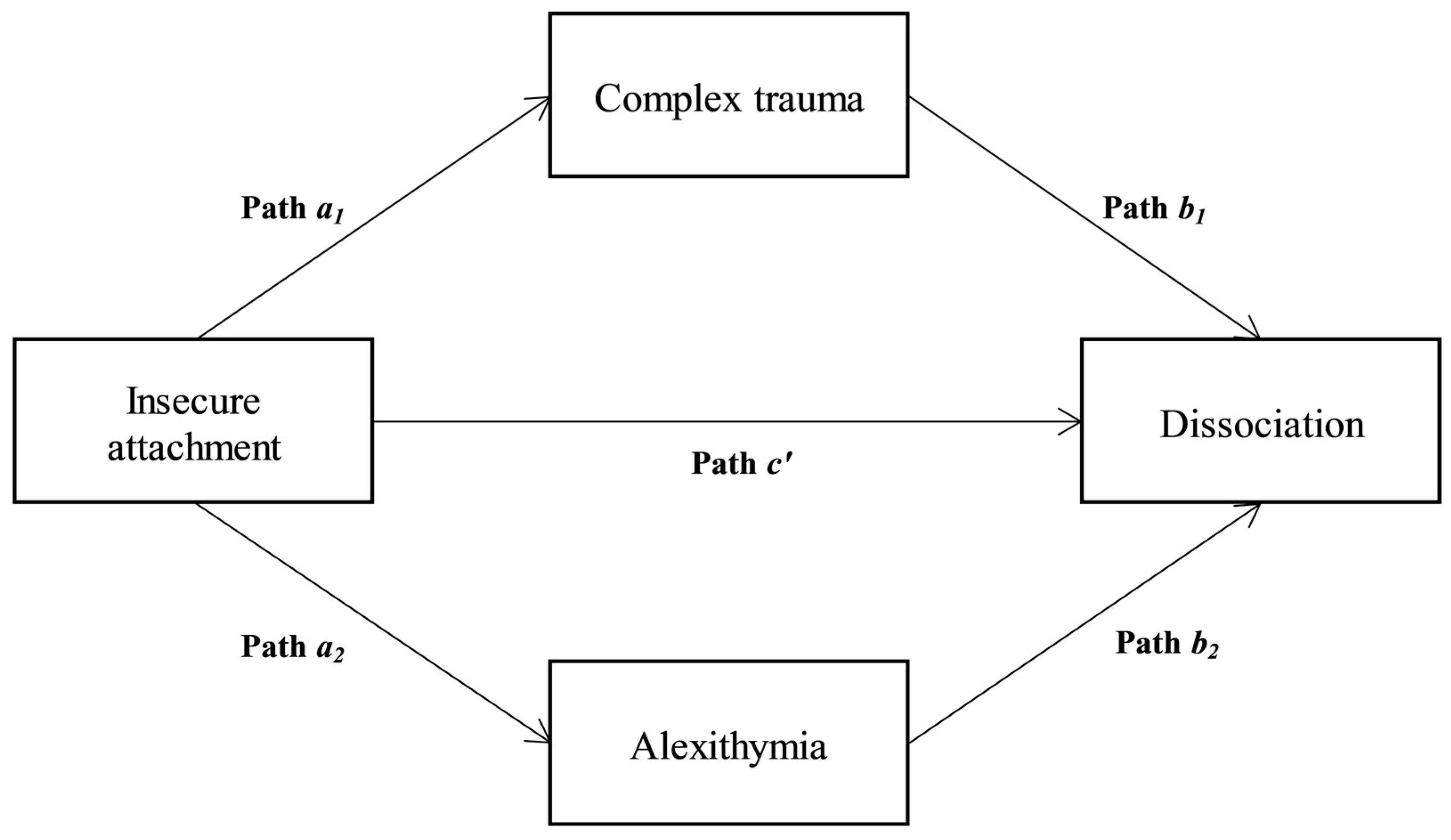
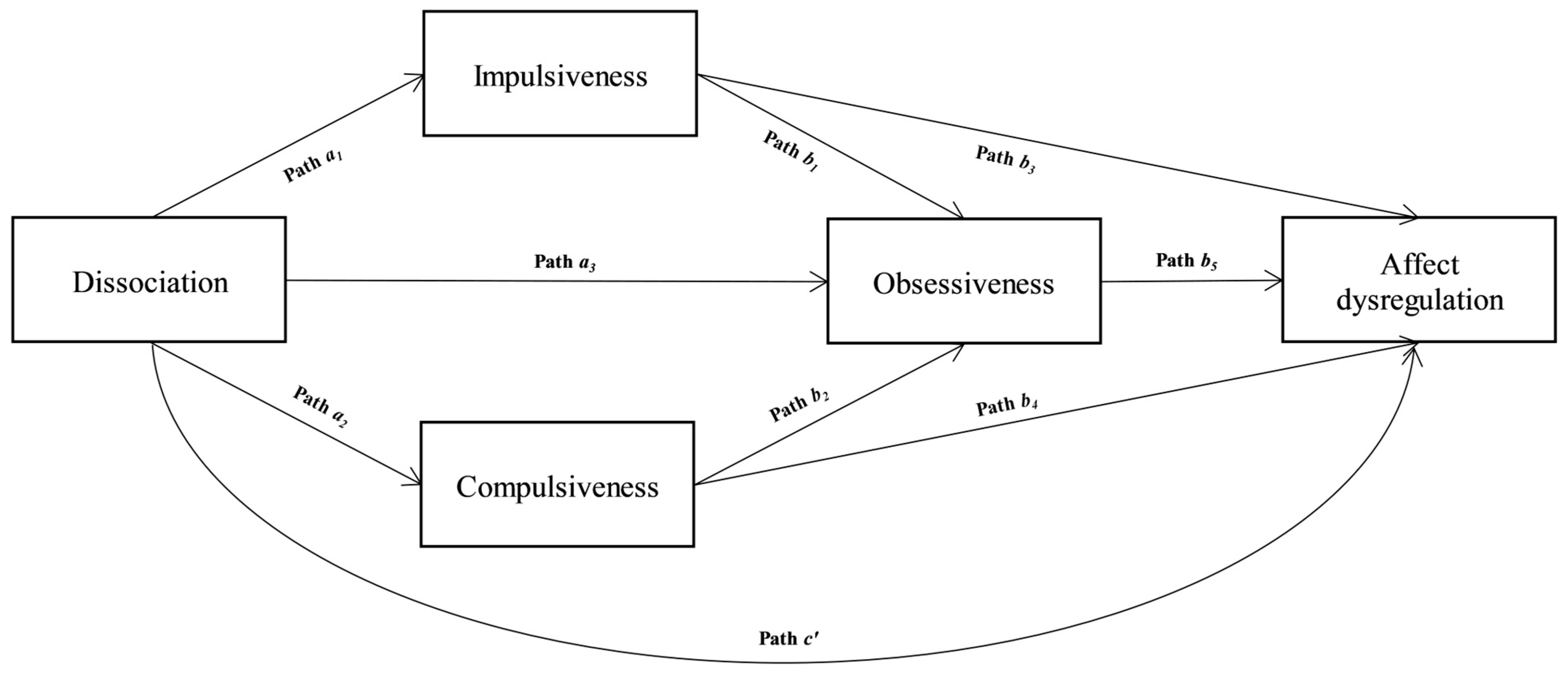
Aim and Hypotheses
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.2.1. Addictive Behavior Questionnaire (ABQ)
2.2.2. Psychological Treatment Inventory—Attachment Styles Scale (PTI-ASS)
2.2.3. Twenty-Items Toronto Alexithymia Scale (TAS-20)
2.2.4. Traumatic Experiences Checklist (TEC)
2.2.5. Dissociative Experience Scale-II (DES-II)
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Society of Addiction Medicine. Public Policy Statement: Definition of Addiction. Available online: https://www.asam.org/resources/definition-of-addiction (accessed on 6 November 2019).
- Agatsuma, S.; Hiroi, N. Genetic basis of drug dependence and comorbid behavioral traits. Nihon shinkei seishin yakurigaku zasshi. JPN J. Psychopharmacol. 2004, 24, 137–145. [Google Scholar]
- Brandon, T.H.; Vidrine, J.I.; Litvin, E.B. Relapse and relapse prevention. Annu. Rev. Clin. Psychol. 2007, 3, 257–284. [Google Scholar] [CrossRef]
- Caretti, V.; Gori, A.; Craparo, G.; Giannini, M.; Iraci-Sareri, G.; Schimmenti, A. A new measure for assessing substance-related and addictive disorders: The addictive behavior questionnaire (ABQ). J. Clin. Med. 2018, 7, 194. [Google Scholar] [CrossRef] [Green Version]
- Gori, A.; Topino, E.; Craparo, G.; Bagnoli, I.; Caretti, V.; Schimmenti, A. A comprehensive model for gambling behaviors: Assessment of the factors that can contribute to the vulnerability and maintenance of gambling disorder. J. Gambl. Stud. 2022, 38, 235–251. [Google Scholar] [CrossRef]
- Gori, A.; Craparo, G.; Caretti, V.; Giannini, M.; Iraci Sareri, G.; Bruschi, A.; Janiri, L.; Ponti, L.; Tani, F. Impulsivity, Alexithymia and Dissociation among pathological gamblers in different therapeutic settings: A multisample comparison study. Psychiatry Res. 2016, 246, 789–795. [Google Scholar] [CrossRef]
- Gori, A.; Ponti, L.; Tani, F.; Iraci Sareri, G.; Giannini, M.; Meringolo, P.; Craparo, G.; Bruschi, A.; Caretti, V.; Cacioppo, M.; et al. Psychopathological features in a sample of substance-abusing individuals with criminal history: Towards a definition of a personality prototype of an ‘Addict with Criminal Conduct’. Crim. Behav. Ment. Health 2017, 27, 312–325. [Google Scholar] [CrossRef]
- Flores, P.J. Addiction as an Attachment Disorder; Jason Aronson: Lanham, MD, USA, 2004. [Google Scholar]
- Musetti, A.; Corsano, P.; Boursier, V.; Schimmenti, A. Problematic Internet use in lonely adolescents: The mediating role of detachment from parents. Clin. Neuropsychiatry 2020, 17, 3–10. [Google Scholar] [CrossRef]
- Gori, A.; Russo, S.; Topino, E. Love Addiction, Adult Attachment Patterns and Self-Esteem: Testing for Mediation Using Path Analysis. J. Pers. Med. 2023, 13, 247. [Google Scholar] [CrossRef]
- Topino, E.; Cacioppo, M.; Gori, A. The Relationship between Attachment Styles and Compulsive Online Shopping: The Mediating Roles of Family Functioning Patterns. Int. J. Environ. Res. Public Health 2022, 19, 8162. [Google Scholar] [CrossRef]
- Gori, A.; Topino, E.; Griffiths, M.D. The associations between attachment, self-esteem, fear of missing out, daily time expenditure, and problematic social media use: A path analysis model. Addict. Behav. 2023, 141, 107633. [Google Scholar] [CrossRef]
- Schimmenti, A. The trauma factor: Examining the relationships among different types of trauma, dissociation, and psychopathology. J. Trauma Dissociation 2018, 19, 552–571. [Google Scholar] [CrossRef]
- Beebe, B.; Lachmann, F. Organizing principles of interaction from infant research and the lifespan prediction of attachment: Application to adult treatment. J. Infant Child Adolesc. Psychother. 2022, 2, 61–89. [Google Scholar] [CrossRef]
- Taylor, G.J.; Bagby, R.M.; Parker, J.D. Disorders of Affect Regulation: Alexithymia in Medical and Psychiatric Illness; Cambridge University Press: Cambridge, UK, 1999. [Google Scholar]
- Evren, C.; Cınar, O.; Evren, B.; Ulku, M.; Karabulut, V.; Umut, G. The mediator roles of trait anxiety, hostility, and impulsivity in the association between childhood trauma and dissociation in male substance-dependent inpatients. Compr. Psychiatry 2013, 54, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Schimmenti, A. Dissociative experiences and dissociative minds: Exploring a nomological network of dissociative functioning. J. Trauma Dissociation 2016, 17, 338–361. [Google Scholar] [CrossRef] [PubMed]
- Schimmenti, A.; Caretti, V. Linking the overwhelming with the unbearable: Developmental trauma, dissociation, and the disconnected self. Psychoanal. Psychol. 2016, 33, 106–128. [Google Scholar] [CrossRef]
- Schimmenti, A.; Caretti, V. Video-terminal dissociative trance: Toward a psychodynamic understanding of problematic Internet use. Clin. Neuropsychiatry 2017, 14, 64–72. [Google Scholar] [CrossRef]
- Gioia, F.; Rega, V.; Boursier, V. Problematic internet use and emotional dysregulation among young people: A literature review. Clin. Neuropsychiatry 2021, 18, 41–54. [Google Scholar] [CrossRef]
- Giardina, A.; Di Blasi, M.; Schimmenti, A.; King, D.L.; Starcevic, V.; Billieux, J. Online gaming and prolonged self-isolation: Evidence from Italian gamers during the COVID-19 outbreak. Clin. Neuropsychiatry 2021, 18, 65. [Google Scholar] [CrossRef] [PubMed]
- Craparo, G.; Ardino, V.; Gori, A.; Caretti, V. The relationships between early trauma, dissociation, and alexithymia in alcohol addiction. Psychiatry Investig. 2014, 11, 330. [Google Scholar] [CrossRef] [Green Version]
- Schimmenti, A.; Billieux, J.; Santoro, G.; Casale, S.; Starcevic, V. A trauma model of substance use: Elaboration and preliminary validation. Addict Behav. 2022, 134, 107431. [Google Scholar] [CrossRef]
- Gori, A.; Topino, E.; Griffiths, M.D. A screening tool for exercise addiction: The psychometric properties of the Italian Exercise Addiction Inventory. Int. J. Ment. Health Addict. 2021. Online first. [Google Scholar] [CrossRef]
- Gori, A.; Topino, E.; Casale, S. Assessment of online compulsive buying: Psychometric properties of the Italian compulsive online shopping scale (COSS). Addict. Behav. 2022, 129, 107274. [Google Scholar] [CrossRef] [PubMed]
- Gori, A.; Topino, E.; Bagnoli, I.; Iraci-Sareri, G.; Craparo, G. Psychopathological features and drop-out predictors in a sample of individuals with substance use disorder under residenti al community treatment. Clin. Neuropsychiatry 2020, 17, 11–23. [Google Scholar] [CrossRef]
- Hayes, A.F. Beyond Baron and Kenny: Statistical mediation analysis in the new millennium. Commun. Monogr. 2009, 76, 408–420. [Google Scholar] [CrossRef]
- Baron, R.M.; Kenny, D.A. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173. [Google Scholar] [CrossRef] [PubMed]
- Giannini, M.; Gori, A.; De Sanctis, E.; Schuldberg, D. Attachment in psychotherapy: Psychometric properties of the Psychological Treatment Inventory Attachment Styles Scale (PTI-ASS). J. Psychother. Integr. 2021, 21, 363–381. [Google Scholar] [CrossRef]
- Gori, A.; Giannini, M.; Schuldberg, D. PTI—Psychological Treatment Inventory; Giunti OS–Organizzazioni Speciali: Florence, Italy, 2015. [Google Scholar]
- Bagby, R.M.; Parker, J.D.; Taylor, G.J. The twenty-item Toronto Alexithymia Scale—I. Item selection and cross-validation of the factor structure. J. Psychosom. Res. 1994, 38, 23–32. [Google Scholar] [CrossRef]
- Bagby, R.M.; Taylor, G.J.; Parker, J.D. The twenty-item Toronto Alexithymia Scale—II. Convergent, discriminant, and concurrent validity. J. Psychosom. Res. 1994, 38, 33–40. [Google Scholar] [CrossRef]
- Bressi, C.; Taylor, G.; Parker, J.; Bressi, S.; Brambilla, V.; Aguglia, E.; Allegranti, I.; Bongiorno, A.; Giberti, F.; Bucca, M.; et al. Cross validation of the factor structure of the 20-item Toronto Alexithymia Scale: An Italian multicenter study. J. Psychosom. Res. 1996, 41, 551–559. [Google Scholar] [CrossRef]
- Nijenhuis, E.R.; Van der Hart, O.; Kruger, K. The psychometric characteristics of the Traumatic Experiences Checklist (TEC): First findings among psychiatric outpatients. Psychol. Psychother. 2022, 9, 200–210. [Google Scholar] [CrossRef]
- Carlson, E.B.; Putnam, F.W. An update on the Dissociative Experiences Scale. Dissociation 1993, 6, 16–27. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis Second Edition: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2018. [Google Scholar]
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef]
- Shafiee, S.A.; Razaghi, E.; Vedadhir, A.A. Multi-Level Approach to Theories of Addiction: A Critical Review. Iran J. Psychiatry Behav. Sci. 2019, 13, e88881. [Google Scholar] [CrossRef] [Green Version]
- Zdankiewicz-Ścigała, E.; Ścigała, D.K. Trauma, temperament, alexithymia, and dissociation among persons addicted to alcohol: Mediation model of dependencies. Front. Psychol. 2018, 9, 1570. [Google Scholar] [CrossRef] [PubMed]
- Midolo, L.R.; Santoro, G.; Ferrante, E.; Pellegriti, P.; Russo, S.; Costanzo, A.; Schimmenti, A. Childhood trauma, attachment and psychopathology: A correlation network approach. Mediterr. J. Clin. Psychol. 2020, 8, 2. [Google Scholar] [CrossRef]
- Bowlby, J. A Secure Base: Clinical Applications of Attachment Theory; Routledge: London, UK, 1988. [Google Scholar]
- Santoro, G.; Midolo, L.R.; Costanzo, A.; Schimmenti, A. The vulnerability of insecure minds: The mediating role of mentalization in the relationship between attachment styles and psychopathology. Bull. Menn. Clin. 2021, 85, 358–384. [Google Scholar] [CrossRef] [PubMed]
- Damasio, A.R. Looking for Spinoza: Joy, Sorrow, and the Feeling Brain; Houghton Mifflin Harcourt: Boston, MA, USA, 2003. [Google Scholar]
- Gedo, J. Conceptual Issues in Psychoanalysis; Analytic Press: Hillsdale, NJ, USA, 1986. [Google Scholar]
- Pellerone, M.; Cascio, M.I.; Costanzo, G.; Gori, A.; Pace, U.; Craparo, G. Alexithymia and psychological symptomatology: Research conducted on a non-clinical group of Italian adolescents. Int. J. Cult. Ment. Health 2017, 10, 300–309. [Google Scholar] [CrossRef]
- Schimmenti, A. The developmental roots of dissociation: A multiple mediation analysis. Psychoanal. Psychol. 2017, 34, 96–105. [Google Scholar] [CrossRef]
- Topino, E.; Gori, A.; Cacioppo, M. Alexithymia, dissociation, and family functioning in a sample of online gamblers: A moderated mediation study. Int. J. Environ. Res. Public Health 2021, 18, 13291. [Google Scholar] [CrossRef]
- Gori, A.; Topino, E. The Association between Alexithymia and Social Media Addiction: Exploring the Role of Dysmorphic Symptoms, Symptoms Interference, and Self-Esteem, Controlling for Age and Gender. J. Pers. Med. 2023, 13, 152. [Google Scholar] [CrossRef] [PubMed]
- Gori, A.; Topino, E.; Pucci, C.; Griffiths, M.D. The Relationship between Alexithymia, Dysmorphic Concern, and Exercise Addiction: The Moderating Effect of Self-Esteem. J. Pers. Med. 2021, 11, 1111. [Google Scholar] [CrossRef]
- Klanecky, A.K.; Harrington, J.; McChargue, D.E. Child sexual abuse, dissociation, and alcohol: Implications of chemical dissociation via blackouts among college women. Am. J. Drug Alcohol Abus. 2008, 34, 277–284. [Google Scholar] [CrossRef]
- Faulkner, B.; Goldstein, A.L.; Wekerle, C. Pathways from childhood maltreatment to emerging adulthood: Investigating trauma-mediated substance use and dating violence outcomes among child protective services–involved youth. Child Maltreat 2014, 19, 219–232. [Google Scholar] [CrossRef] [PubMed]
- Gori, A.; Topino, E.; Fioravanti, G.; Casale, S. Exploring the Psychodynamics of Compulsive Shopping: Single and Moderated Mediation Analyses. Int. J. Ment Health Addiction 2022. Advanced Online Publication. [Google Scholar] [CrossRef]
- Sideli, L.; Di Forti, M.; Ferraro, L.; Montana, S.; Tripoli, G.; Quattrone, D.; Colizzi, M.; La Barbera, D.; La Cascia, C. The Relationship Between Dissociative Experiences and Cannabis Use: A Systematic Review. Curr. Addict. Rep. 2019, 6, 21–33. [Google Scholar] [CrossRef]
- Gold, M.S. Treating addiction as a human process. Am. J. Psychiatry 2000, 157, 1892–1894. [Google Scholar] [CrossRef]
- Khantzian, E.J. Understanding addictive vulnerability: An evolving psychodynamic perspective. Neuropsychoanalysis 2003, 5, 5–21. [Google Scholar] [CrossRef]
- Hollander, E. Obsessive-compulsive spectrum disorders: An overview. Psychiatr. Ann. 1993, 23, 355–358. [Google Scholar] [CrossRef]
- Potenza, M.N.; Hong, K.I.A.; Lacadie, C.M.; Fulbright, R.K.; Tuit, K.L.; Sinha, R. Neural correlates of stress-induced and cue-induced drug craving: Influences of sex and cocaine dependence. Am. J. Psychiatry 2012, 169, 406–414. [Google Scholar] [CrossRef] [Green Version]
- Baptiste-Roberts, K.; Hossain, M. Socioeconomic disparities and self-reported substance abuse-related problems. Addict. Health 2018, 10, 112–122. [Google Scholar] [CrossRef]
- Justo-Núñez, M.; Morris, L.; Berry, K. Self-report measures of secure attachment in adulthood: A systematic review. Clin. Psychol. Psychother. 2022, 29, 1812–1842. [Google Scholar] [CrossRef]
- George, C.; Kaplan, N.; Main, M. Adult Attachment Interview, Unpublished Manuscript; University of California at Berkeley: Berkeley, CA, USA, 1985. [Google Scholar] [CrossRef]
- Bartholomew, K.; Horowitz, L.M. Attachment styles among young adults: A test of a four-category model. J. Pers. Soc. Psychol. 1991, 61, 226–244. [Google Scholar] [CrossRef] [PubMed]
- Brennan, K.A.; Clark, C.L.; Shaver, P.R. Experiences in Close Relationships Inventory [Database Record]; APA PsycTests: Washington, DC, USA, 1998. [Google Scholar] [CrossRef]
- Fraley, R.C.; Heffernan, M.E.; Vicary, A.M.; Brumbaugh, C.C. The experiences in close relationships—Relationship Structures Questionnaire: A method for assessing attachment orientations across relationships. Psychol. Assess. 2011, 23, 615–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gori, A.; Topino, E.; Cacioppo, M.; Craparo, G.; Schimmenti, A.; Caretti, V. An Addictive Disorders Severity model: A chained mediation analysis using structural equation modelling. J. Addict. Dis. 2022. Online first. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Sample | |
|---|---|---|
| Sex (%) | ||
| Males | 77.1 | |
| Females | 21.7 | |
| Age (M, SD) | 36.3 ± 12.2 | |
| Marital Status (%) | ||
| Single | 57.9 | |
| Married | 23.3 | |
| Cohabiting | 5.6 | |
| Separated | 6.7 | |
| Divorced | 4.9 | |
| Widowed | 1.4 | |
| Missing Values | 0.2 | |
| Education (%) | ||
| Elementary school (5 years) | 5.1 | |
| Middle School diploma (8 years) | 38.4 | |
| High School diploma (13 years) | 42.3 | |
| Bachelor’s degree (16 years) | 5.1 | |
| Master’s degree (18 years) | 6.0 | |
| Post-Lauream Specialization (22 years) | 2.3 | |
| Missing values | 0.7 | |
| Professional Condition (%) | ||
| Unemployed | 34.2 | |
| Looking for the first job | 2.8 | |
| Entrepreneur | 5.3 | |
| Employee | 15.6 | |
| Artisan | 4.9 | |
| Trader | 2.3 | |
| Armed forces | 0.5 | |
| Housewife | 1.9 | |
| Student | 13.7 | |
| Retired | 4.7 | |
| Other | 13.3 | |
| Missing values | 0.9 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (1) Secure attachment style | - | −0.109 * | −0.127 ** | −0.208 ** | −0.378 ** | −0.060 | −0.087 | −0.287 ** | −0.272 ** | −0.116 ** | −0.139 ** | −0.177 ** | −0.112 * | −0.211 ** |
| (2) Preoccupied attachment style | - | 0.007 | 0.355 ** | 0.376 ** | 0.255 ** | 0.340 ** | 0.658 ** | 0.480 ** | 0.345 ** | 0.203 ** | 0.367 ** | 0.372 ** | 0.451 ** | |
| (3) Avoidant attachment style | - | 0.198 ** | 0.149 ** | 0.149 ** | 0.170 ** | 0.081 | 0.111* | 0.154 ** | 0.131 ** | 0.193 ** | 0.142 ** | 0.177 ** | ||
| (4) Unresolved attachment style | - | 0.286 ** | 0.355 ** | 0.390 ** | 0.342 ** | 0.310 ** | 0.352 ** | 0.208 ** | 0.311 ** | 0.340 ** | 0.335 ** | |||
| (5) Alexithymia | - | 0.099 * | 0.425 ** | 0.439 ** | 0.579 ** | 0.476 ** | 0.119 ** | 0.424 ** | 0.364 ** | 0.498 ** | ||||
| (6) Traumatic experiences | - | 0.275 ** | 0.284 ** | 0.233 ** | 0.270 ** | 0.565 ** | 0.285 ** | 0.222 ** | 0.253 ** | |||||
| (7) Dissociation | - | 0.353 ** | 0.417 ** | 0.591 ** | 0.232 ** | 0.409 ** | 0.454 ** | 0.432 ** | ||||||
| (8) Separation anxiety | - | 0.650 ** | 0.455 ** | 0.319 ** | 0.466 ** | 0.448 ** | 0.590 ** | |||||||
| (9) Affect dysregulation | - | 0.523 ** | 0.285 ** | 0.621 ** | 0.567 ** | 0.706 ** | ||||||||
| (10) Somatoform and psychological dissociation | - | 0.242 ** | 0.496 ** | 0.531 ** | 0.524 ** | |||||||||
| (11) Childhood traumatic experiences | - | 0.251 ** | 0.229 ** | 0.272 ** | ||||||||||
| (12) Impulse dyscontrol | - | 0.577 ** | 0.710 ** | |||||||||||
| (13) Compulsive behavior and ritualization | - | 0.659 ** | ||||||||||||
| (14) Obsessive thoughts | - |
| Antecedent | Consequent | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M1 | M2 | Y | |||||||||||||
| b | SE | p | 95% CI | b | SE | p | 95% CI | b | SE | p | 95% CI | ||||
| X | a1 | 18,527 | 2.181 | <0.001 | 14.242, 22.811 | a2 | 1.270 | 0.190 | <0.001 | 0.896, 1.644 | c′ | 0.971 | 0.173 | <0.001 | 0.631, 1.311 |
| M1 | - | - | - | - | - | - | - | - | b1 | 0.012 | 0.003 | <0.001 | 0.006, 0.019 | ||
| M2 | - | - | - | - | - | - | - | - | b2 | 0.315 | 0.037 | <0.001 | 0.244, 0.387 | ||
| Constant | iM1 | 30.719 | 18.156 | 0.091 | −4.953, 66.391 | iM2 | 39.832 | 1.545 | <0.001 | 36.718, 42.946 | iY | −11.834 | 1.953 | <0.001 | −15.670, −7.998 |
| R2 = 0.126 | R2 = 0.082 | R2 = 0.281 | |||||||||||||
| F(1, 428) = 72.181, p < 0.001 | F(1, 428) = 44.520, p < 0.001 | F(3, 426) = 64.878, p < 0.001 | |||||||||||||
| Antecedent | Consequent | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M1 | M2 | M3 | Y | |||||||||||||||||
| b | SE | p | 95% CI | b | SE | p | 95% CI | b | SE | p | 95% CI | b | SE | p | 95% CI | |||||
| X | a1 | 0.176 | 0.018 | <0.001 | 0.141, 0.210 | a2 | 0.178 | 0.016 | <0.001 | 0.148, 0.209 | a3 | 0.037 | 0.015 | <0.05 | 0.007, 0.067 | c′ | 0.038 | 0.001 | <0.05 | 0.009, 0.067 |
| M1 | - | - | - | - | - | - | b1 | 0.521 | 0.039 | <0.001 | 0.445, 0.596 | b3 | 0.195 | 0.044 | <0.001 | 0.109, 0.281 | ||||
| M2 | - | - | - | - | - | - | b2 | 0.414 | 0.043 | <0.001 | 0.329, 0.499 | b4 | 0.125 | 0.046 | <0.01 | 0.035, 0.214 | ||||
| M3 | - | - | - | - | - | - | - | - | - | - | b5 | 0.409 | 0.044 | <0.001 | 0.324, 0.495 | |||||
| Constant | iM | 8.084 | 0.321 | <0.001 | 7.454, 8.714 | iM2 | 5.687 | 0.287 | <0.001 | 5.124, 6.250 | iM3 | 2.404 | 0.377 | <0.001 | 1.663, 3.144 | iY | 3.354 | 0.381 | <0.001 | 2.606, 4.102 |
| R2 = 0.167, F(1, 428) = 100.390, p < 0.001 | R2 = 0.206, F(1, 428) = 129.465, p < 0.001 | R2 = 0.602, F(3, 426) = 251.129, p < 0.001 | R2 = 0.545, F(4, 425) = 148.503, p < 0.001 | |||||||||||||||||
| Model | Total Effect | Direct Effect | Indirect Effect | Partial Standardized Indirect Effect | Completely Standardized Indirect Effect | Bootstrapping 95% CI |
|---|---|---|---|---|---|---|
| Vulnerability model | 1.600 | 0.971 | 0.629 | 0.051 | 0.154 | (0.384, 0.918) |
| Maintenance model | 0.177 | 0.038 | 0.139 | 0.027 | 0.328 | (0.110, 0.176) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gori, A.; Topino, E.; Cacioppo, M.; Craparo, G.; Schimmenti, A.; Caretti, V. An Integrated Approach to Addictive Behaviors: A Study on Vulnerability and Maintenance Factors. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 512-524. https://doi.org/10.3390/ejihpe13030039
Gori A, Topino E, Cacioppo M, Craparo G, Schimmenti A, Caretti V. An Integrated Approach to Addictive Behaviors: A Study on Vulnerability and Maintenance Factors. European Journal of Investigation in Health, Psychology and Education. 2023; 13(3):512-524. https://doi.org/10.3390/ejihpe13030039
Chicago/Turabian StyleGori, Alessio, Eleonora Topino, Marco Cacioppo, Giuseppe Craparo, Adriano Schimmenti, and Vincenzo Caretti. 2023. "An Integrated Approach to Addictive Behaviors: A Study on Vulnerability and Maintenance Factors" European Journal of Investigation in Health, Psychology and Education 13, no. 3: 512-524. https://doi.org/10.3390/ejihpe13030039