
Synergistic Effect of Medical Information Systems Integration: To What Extent Will It Affect the Accuracy Level in the Reports and Decision-Making Systems?


Abstract
:1. Introduction
2. Related Works
3. Deployment of HIS and MIS
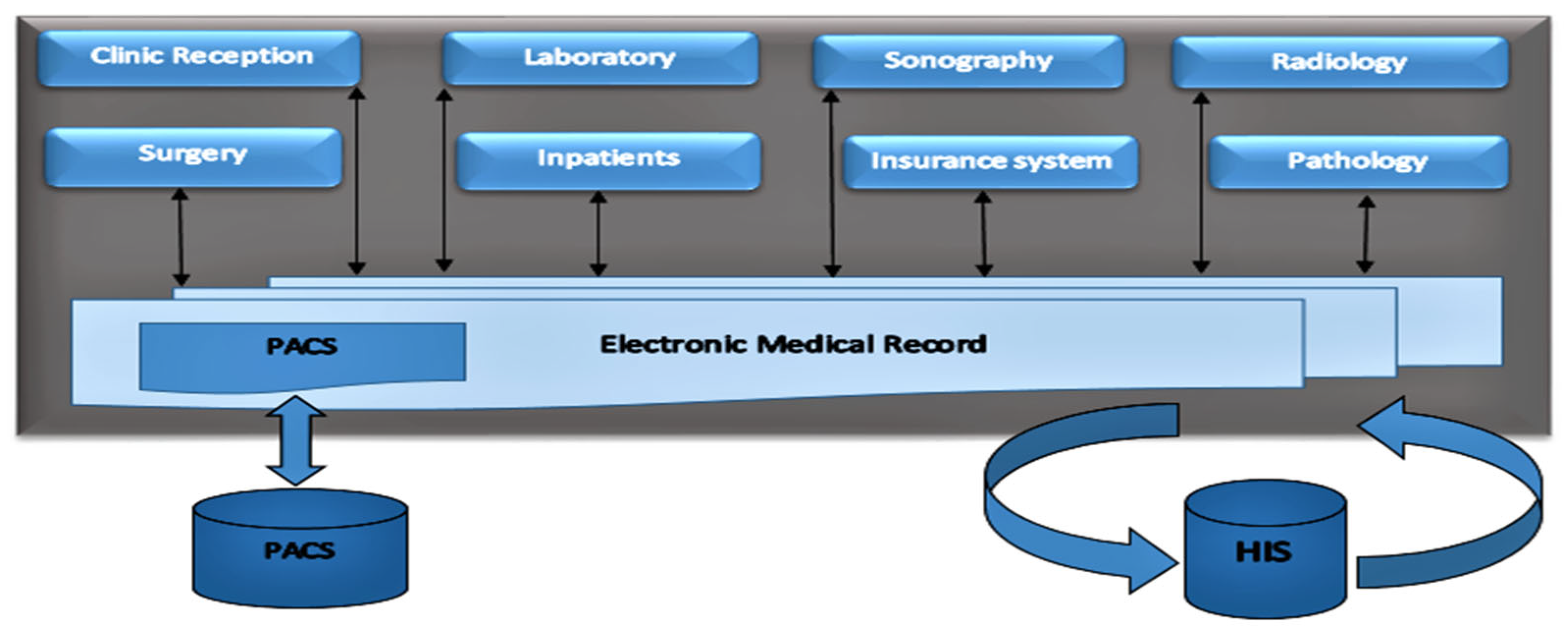
3.1. Hospital Information System
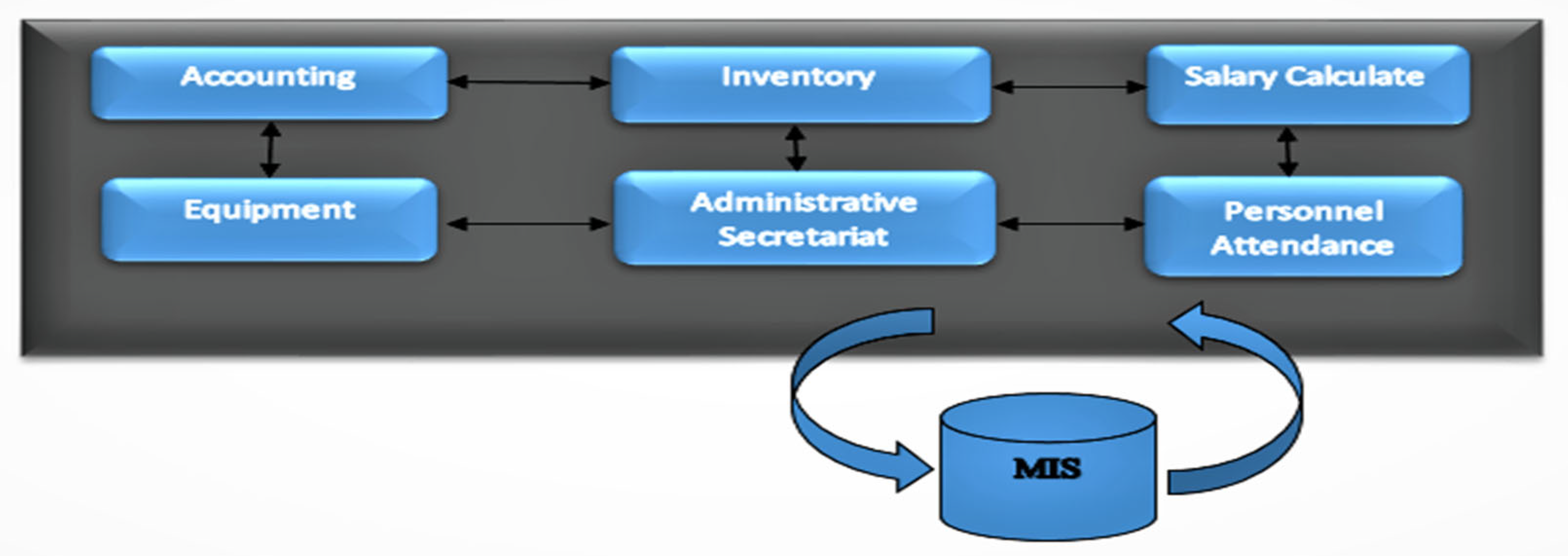
3.2. Management Information System
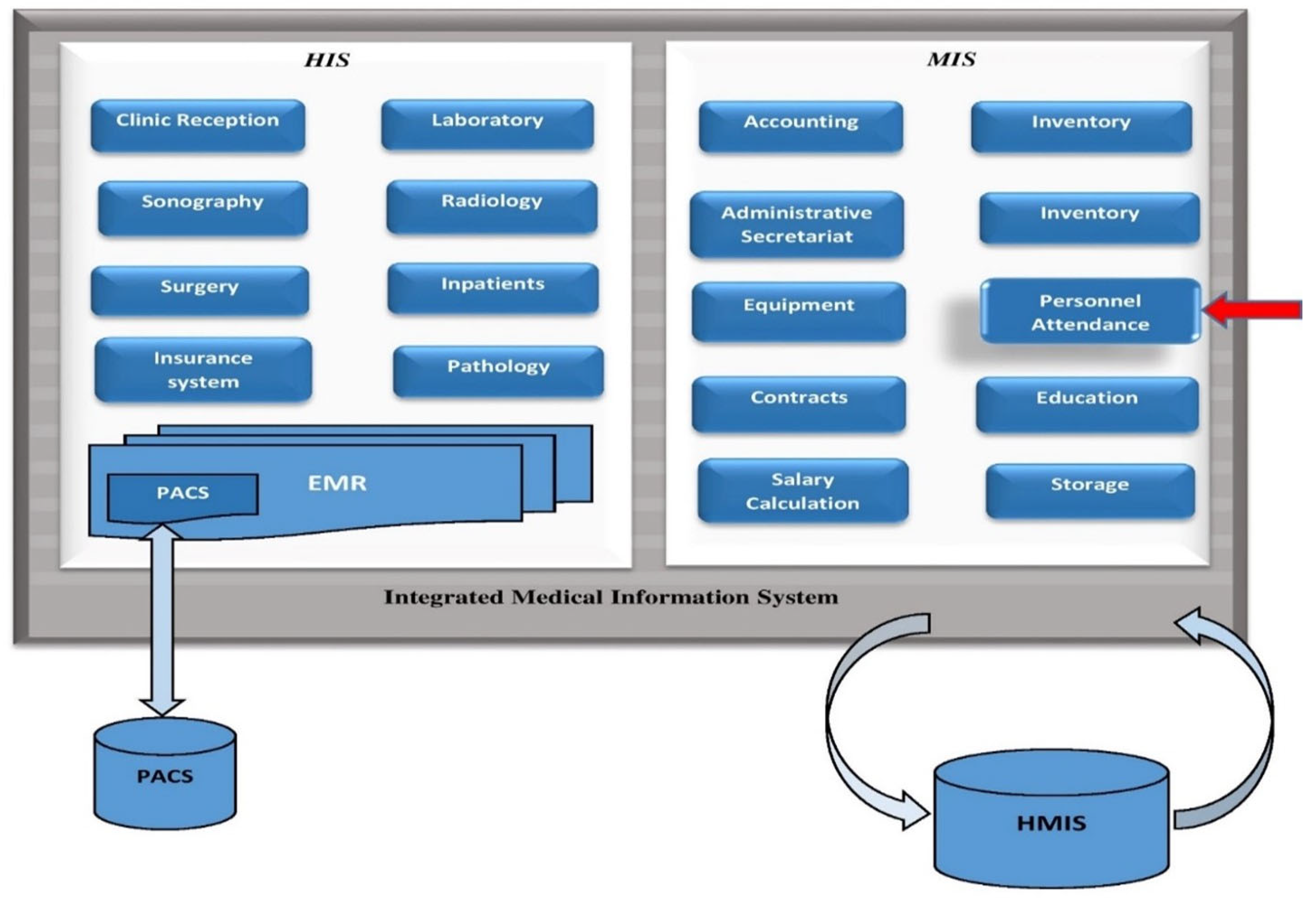
4. Transferring One Subsystem from MIS to HMIS
- o
- Performing fundamental definitions and professional expressions in the destination subsystem.
- o
- Connecting the attendance devices to the new subsystem.
- o
- Customizing the destination subsystem to prepare some features available in the MIS.
- o
- Carrying out the essential data entry such as identities, work shifts, leave, and mission authorizing also permitted delay and haste.
- o
- Building the necessary reports in the second personnel attendance subsystem.
5. Reception Rate
6. Data Analysis
6.1. Data Extraction
- o
- Calculating the reception rate (RR_19) through two separate information systems: HIS and MIS.
- o
- Calculating the reception rate (RR_20) in an integrated information system: HMIS.
- o
- As we introduced before, to calculate the reception rate, we need both “the number of admitted patients” and the “number of working hours”. The necessary data has been extracted from the available reports, but in 2019, a part of the data (number of admitted patients) was in the HIS, and another part (number of working hours) was extracted from the MIS. In contrast, in 2020, both parts of the reception rate came from an integrated information system (HMIS). To clarify this issue, the extracted information and the sources used are given in Table 1.
6.2. Statistical Analysis
6.3. Data Interpretation
7. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- García-Peñalvo, F.; Vázquez-Ingelmo, A.; García-Holgado, A.; Sampedro-Gómez, J.; Sánchez-Puente, A.; Vicente-Palacios, V.; Dorado-Díaz, P.I.; Sánchez, P.L. Application of Artificial Intelligence Algorithms Within the Medical Context for Non-Specialized Users: The CARTIER-IA Platform. Int. J. Interact. Multimed. Artif. Intell. 2021, 6, 46. [Google Scholar] [CrossRef]
- Hyla, T.; Pejaś, J. eHealth Integrity Model Based on a Permissioned Blockchain. In Proceedings of the 2019 Cybersecurity and Cyberforensics Conference (CCC), Melbourne, Australia, 8–9 May 2019; pp. 172–177. [Google Scholar]
- Hruby, G.W.; Matsoukas, K.; Cimino, J.J.; Weng, C. Facilitating biomedical researchers’ interrogation of electronic health record data: Ideas from outside of biomedical informatics. Biomed. Inform. 2016, 60, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Martin, M. Available online: https://www.guru99.com/mis-definition.html (accessed on 15 January 2022).
- Johns, M. Information Management for Health Professions, 2nd ed.; Cengage Learning: Boston, MA, USA, 2002. [Google Scholar]
- Greve, P. HealthTrek: Medical Malpractice Claim Trends in 2017; Willis Towers Watson: London, UK, 2017. [Google Scholar]
- Strepetova, V. Ten A.R. Medical errors. Colloquium 2019, 12, 68–70. [Google Scholar]
- Adenuga, O.A.; Kekwaletswe, R.M.; Coleman, A. eHealth integration and interoperability issues: Towards a solution through enterprise architecture. Health Inf. Sci. Syst. 2015, 3, 1. [Google Scholar] [CrossRef] [Green Version]
- Pandey, K.A.; Irshad Khan, A.; Abushark, Y.B.; Alam, M.; Agrawal, A.; Kumar, R.; Khan, R.A. Key Issues in Healthcare Data Integrity: Analysis and Recommendations. IEEE Access 2020, 8, 40612–40628. [Google Scholar] [CrossRef]
- Mantas, G.; Lymberopoulos, D.; Komninos, N. Integrity Mechanism for eHealth Tele-monitoring System in Smart Home Environment. In Proceedings of the 31st Annual International Conference of the IEEE EMBS, Minneapolis, MN, USA, 3–6 September 2009. [Google Scholar]
- Calì, A.; Calvanese, D.; De Giacomo, G.; Lenzerini, M. Data integration under integrity constraints. Inf. Syst. 2004, 29, 147–163. [Google Scholar] [CrossRef] [Green Version]
- Prasser, F.; Kohlbacher, O.; Mansmann, U.; Bauer, B.; Kuhn, K.A. Data integration for future medicine (DIFUTURE). Methods Inf. Med. 2018, 57, e57–e65. [Google Scholar] [CrossRef] [Green Version]
- Tsumoto, S.; Hirano, S. Healthcare IT: Integration of consumer healthcare data an electronic medical records for chronic disease management. In Proceedings of the 2014 IEEE International Conference on Granular Computing (GrC), Noboribetsu, Japan, 22–24 October 2014; pp. 310–315. [Google Scholar]
- Bowman, S. Impact of Electronic Health Record Systems on Information Integrity: Quality and Safety Implications. Perspect. Health Inf. Manag. 2013, 10, 1c. [Google Scholar]
- García-Holgado, A.; García-Peñalvo, F.J. Validation of the learning ecosystem metamodel using transformation rules. Future Gener. Comput. Syst. 2019, 91, 300–309. [Google Scholar] [CrossRef] [Green Version]
- Zarour, M.; Alenezi, M.; Ansari, T.J.; Oandey, A.P.; Ahmad, M.; Agrawal, A.; Kumar, R.; Ahamd Khan, R. Ensuring data integrity of healthcare information in the era of digital health. IET Inst. Eng. Technol. 2021, 8, 66–77. [Google Scholar] [CrossRef]
- Camach, A.; Merayo, M.; Nunez, M. A Formal Passive Testing Approach to Control the Integrity of Private Information in eHealth Systems. In Recent Developments in Intelligent Information and Database Systems; Springer: Berlin, Germany, 2021; pp. 221–231. [Google Scholar]
- Vázquez-Ingelmo, A.; García-Holgado, A.; García-Peñalvo, F.J.; Therón, R. A Meta-Model Integration for Supporting Knowledge Discovery in Specific Domains: A Case Study in Healthcare. Sensors 2020, 20, 4072. [Google Scholar] [CrossRef] [PubMed]
- Vimalachandran, P.; Wang, H.; Zhang, Y.; Heyward, B.; Whittaker, F. Ensuring Data Integrity in Electronic Health Records: A Quality Health Care Implication. In Proceedings of the International Confrence on Orange Technologies, Melbourne, Australia, 18–20 December 2016. [Google Scholar]
- Ward, M.J.; Froehle, C.M.; Hart, K.W.; Lindsell, C.J. Operational data integrity during electronic health record implementation in the ED. Am. J. Emerg. Med. 2013, 31, 1029–1033. [Google Scholar] [CrossRef] [PubMed]
- García-Holgado, A.; Marcos-Pablos, S.; Therón-Sánchez, R.; García-Peñalvo, F.J. Technological Ecosystems in the Health Sector: A Mapping Study of European Research Projects. J. Med. Syst. 2019, 43, 100. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, A.; Alharbe, N.R. Need and Importance of Healthcare Data Integrity. Int. J. Eng. Technol. 2019, 11, 854–859. [Google Scholar] [CrossRef] [Green Version]
- Heart, T.; Ben-Assuli, O.; Shabtai, I. A review of PHR, EMR and EHR integration: A more personalized health care and public policy. Health Policy Technol. 2017, 6, 20–25. [Google Scholar] [CrossRef]
- Hsiao, T.-C.; Wu, Z.-Y.; Chung, Y.-F.; Chen, T.-S.; Horng, G.-B. A Secure Integrated Medical Information System. Meical Syst. 2012, 36, 3103–3113. [Google Scholar] [CrossRef]
- Wang, S.; Mao, J.; Tang, J.; Cao, Y. Content Characteristics of Knowledge Integration in the eHealth Field: An analysis based on citation contexts. Data Inf. Sci. 2021, 6, 58–74. [Google Scholar] [CrossRef]
- Wu, Z.; Trigo, V. Impact of information system integration on the healthcare management and medical services. Healthc. Manag. 2021, 14, 1348–1356. [Google Scholar] [CrossRef]
- Raji, S. Regional Integration: Physician Perceptions on Electronic Medical Record Use and Impact in Souhth West Ontario. Ph.D. Thesis, Western University, London, ON, Canada, 2020. [Google Scholar]
- Franček, P.; Žagar, M.; Sruk, V. Interoperability Within E-Health Arena. Fac. Electr. Enginnering Comput. Unska Zagreb Croat. 2015. [Google Scholar] [CrossRef]
- Kumar, M.; Mostafa, J. Research evidence on strategies enabling integration of electronic health records in the health care systems of low- and middle-income countries: A literature review. Health Plan. Manag. 2019, 34, e1016–e1025. [Google Scholar] [CrossRef]
- Zhang, R.; Burgess, E.R.; Reddy, M.C.; Rothrock, N.E.; Bhatt, S.; Rasmussen, L.V.; Butt, Z.; Starren, J.B. Provider perspectives on the integration of patient-reported outcomes in an electronic health record. JAMIA 2019, 2, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Jetelina, K.K.; Woodson, T.T.; Gunn, R.; Muller, B.; Khaya, D.C.; DeVoe, J.E.; Balasubramanian, B.A.; Cohen, D.J. Evaluation of an Electronic Health Record (EHR) Tool for Integrated Behavioral Health in Primary Care. Am. Board Fam. Med. 2018, 31, 712–723. [Google Scholar] [CrossRef] [PubMed]
- Dalal, A.K.; Dykes, P.; Samal, L.; McNally, K.; Mlaver, E.; Yoon, C.S.; Lipsitz, S.R.; Bates, D.W. Potential of an Electronic Health Record-Integrated Patient Portal for Improving Care Plan Concordance during Acute Care. Clin. Inform. 2019, 10, 358–366. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Criteria | Number of Personnel | Sum | Average | Source of Data Extracting | Year of Data Extraction |
|---|---|---|---|---|---|
| Total working hours in a year | 21 | 352,878.75 | 16,803.75 | MIS | 2019 |
| Total admitted patients in a year | 21 | 119,153 | 5673.95 | HIS | 2019 |
| Total working hours in a year | 21 | 367,937.22 | 17,520.82 | HIS + MIS = HMIS | 2020 |
| Total admitted patients in a year | 21 | 156,392 | 7447.25 | HIS + MIS = HMIS | 2020 |
| 2019 | 2020 | |||
|---|---|---|---|---|
| Measurement Criteria | Average | Standard Deviation | Average | Standard Deviation |
| Number of Work hours | 16,803.75 | 2488 | 17,520.82 | 1308.82 |
| Number of Admitted Patients | 5673.95 | 1658.39 | 7447.25 | 1759.84 |
| Admission Rate | 0.3468 | 0.1153 | 0.4298 | 0.10909 |
| Year | Mean Rank | Sum of Ranks | Mann-Whitney | Z | p-Value | |
|---|---|---|---|---|---|---|
| Reception Rate | 2019 | 18.71 | 449.00 | 14,900 | −2.866 | 0.004 |
| 2020 | 30.29 | 727.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Azadi, A.; García-Peñalvo, F.J. Synergistic Effect of Medical Information Systems Integration: To What Extent Will It Affect the Accuracy Level in the Reports and Decision-Making Systems? Informatics 2023, 10, 12. https://doi.org/10.3390/informatics10010012
Azadi A, García-Peñalvo FJ. Synergistic Effect of Medical Information Systems Integration: To What Extent Will It Affect the Accuracy Level in the Reports and Decision-Making Systems? Informatics. 2023; 10(1):12. https://doi.org/10.3390/informatics10010012
Chicago/Turabian StyleAzadi, Ali, and Francisco José García-Peñalvo. 2023. "Synergistic Effect of Medical Information Systems Integration: To What Extent Will It Affect the Accuracy Level in the Reports and Decision-Making Systems?" Informatics 10, no. 1: 12. https://doi.org/10.3390/informatics10010012