
The Effects of an Intervention Based on the Flipped Classroom on the Learning of Basic Life Support in Schoolchildren Aged 10–13 Years: A Quasi-Experimental Study
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
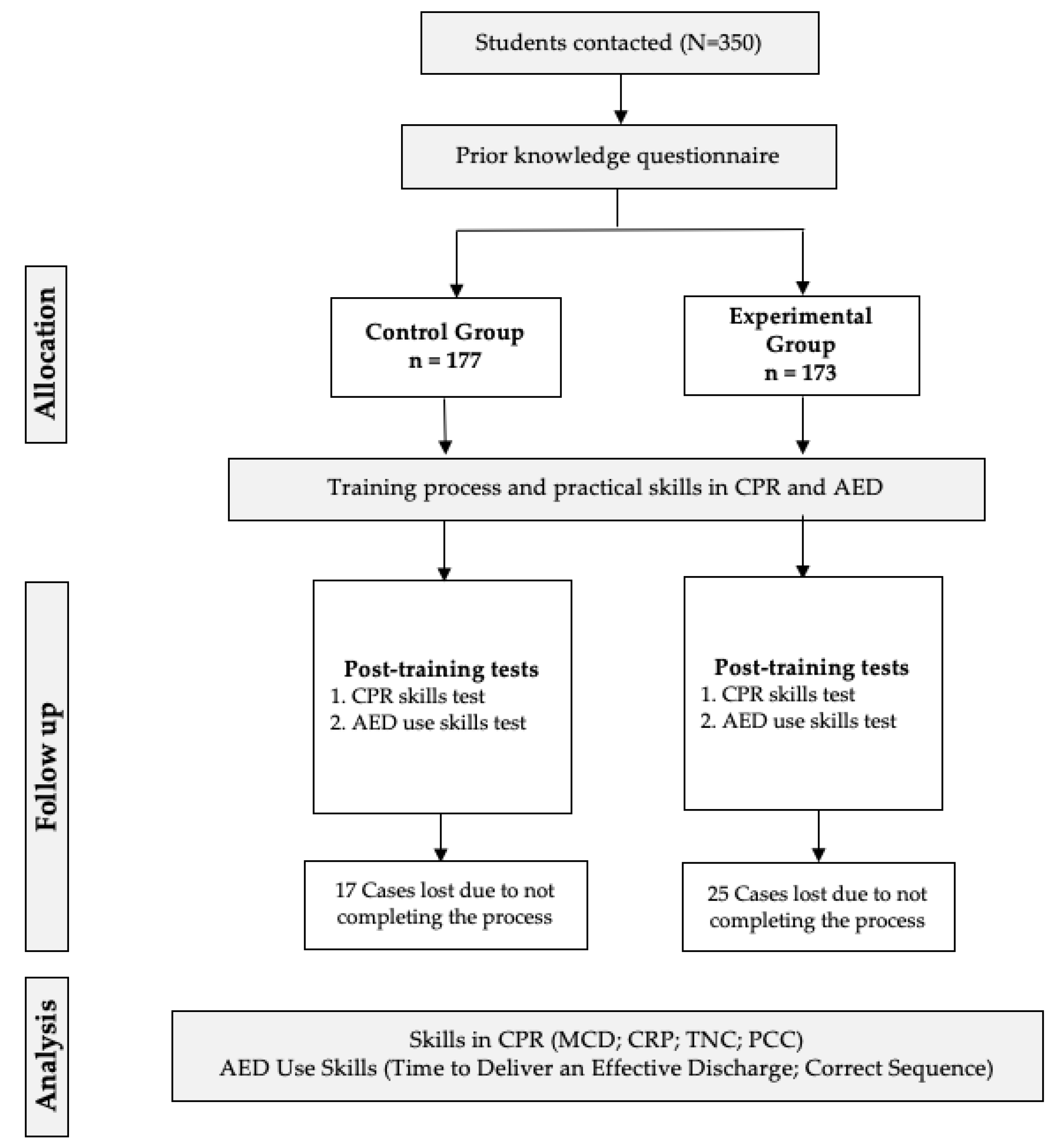
2.1. Study Design
2.2. Participants
2.3. Tools and Measurements
2.3.1. Ad Hoc Questionnaire
2.3.2. Anthropometric Data
2.3.3. CPR Data Collection
2.3.4. AED Data Collection
2.4. Procedures
2.5. Ethics
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. CPR Outcomes
3.2.1. BLS Action Sequence
3.2.2. CPR Quality
3.3. AED Outcomes
3.3.1. Results Obtained in DEA Application
3.3.2. Average Times to Apply an Effective Discharge
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hayashi, M.; Shimizu, W.; Albert, C.M. The Spectrum of Epidemiology Underlying Sudden Cardiac Death. Circ. Res. 2015, 116, 1887–1906. [Google Scholar] [CrossRef] [PubMed]
- Agerskov, M.; Nielsen, A.M.; Hansen, C.M.; Hansen, M.B.; Lippert, F.K.; Wissenberg, M.; Folke, F.; Rasmussen, L.S. Public Access Defibrillation: Great benefit and potential but infrequently used. Resuscitation 2015, 96, 53–58. [Google Scholar] [CrossRef]
- Onan, A.; Turan, S.; Elcin, M.; Erbil, B.; Bulut, Ş.Ç. The effectiveness of traditional Basic Life Support training and alternative technology-enhanced methods in high schools. Hong Kong J. Emerg. Med. 2018, 26, 44–52. [Google Scholar] [CrossRef]
- Bánfai, B.; Pandur, A.; Schiszler, B.; Pék, E.; Radnai, B.; Bánfai-Csonka, H.; Betlehem, J. Little lifesavers: Can we start first aid education in kindergarten?—A longitudinal cohort study. Health Educ. J. 2018, 77, 1007–1017. [Google Scholar] [CrossRef]
- AHA. Heartsaver CPR in the Schools: Student Manual; American Heart Association: Dallas, TX, USA, 2001. [Google Scholar]
- Nolan, J.P.; Soar, J.; Zideman, D.A.; Biarent, D.; Bossaert, L.L.; Deakin, C.; Koster, R.W.; Wyllie, J.; Böttiger, B. European Resuscitation Council Guidelines for Resuscitation 2010 Section 1. Executive summary. Resuscitation 2010, 81, 1219–1276. [Google Scholar] [CrossRef] [PubMed]
- Böttiger, B.W.; Bossaert, L.L.; Castrén, M.; Cimpoesu, D.; Georgiou, M.; Greif, R.; Grünfeld, M.; Lockey, A.; Lott, C.; Maconochie, I.; et al. Kids Save Lives—ERC position statement on school children education in CPR: “Hands that help—Training children is training for life”. Resuscitation 2016, 105, A1–A3. [Google Scholar] [CrossRef]
- Borovnik Lesjak, V.; Šorgo, A.; Strnad, M. Retention of Knowledge and Skills After a Basic Life Support Course for Schoolchildren: A Prospective Study. Inq. J. Health Care Organ. Provis. Financ. 2022, 59, 00469580221098755. [Google Scholar] [CrossRef]
- Navarro-Patón, R.; Freire-Tellado, M.; Basanta-Camiño, S.; Barcala-Furelos, R.; Arufe-Giraldez, V.; Rodriguez-Fernández, J.E. Effect of 3 basic life support training programs in future primary school teachers. A quasi-experimental design. Med. Intensiva 2018, 42, 207–215. [Google Scholar] [CrossRef]
- Pivač, S.; Gradišek, P.; Skela-Savič, B. The impact of cardiopulmonary resuscitation (CPR) training on schoolchildren and their CPR knowledge, attitudes toward CPR, and willingness to help others and to perform CPR: Mixed methods research design. BMC Public Health 2020, 20, 915. [Google Scholar] [CrossRef]
- Stroobants, J.; Monsieurs, K.G.; Devriendt, B.; Dreezen, C.; Vets, P.; Mols, P. Schoolchildren as BLS instructors for relatives and friends: Impact on attitude towards bystander CPR. Resuscitation 2014, 85, 1769–1774. [Google Scholar] [CrossRef]
- Watanabe, K.; Lopez-Colon, D.; Shuster, J.J.; Philip, J. Efficacy and retention of Basic Life Support education including Automated External Defibrillator usage during a physical education period. Prev. Med. Rep. 2017, 5, 263–267. [Google Scholar] [CrossRef] [PubMed]
- Bohn, A.; Van Aken, H.K.; Möllhoff, T.; Wienzek, H.; Kimmeyer, P.; Wild, E.; Döpker, S.; Lukas, R.P.; Weber, T.P. Teaching resuscitation in schools: Annual tuition by trained teachers is effective starting at age 10. A four-year prospective cohort study. Resuscitation 2012, 83, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Decety, J.; Bartal, I.B.-A.; Uzefovsky, F.; Knafo-Noam, A. Empathy as a driver of prosocial behaviour: Highly conserved neurobehavioural mechanisms across species. Philos. Trans. R. Soc. B Biol. Sci. 2016, 371, 20150077. [Google Scholar] [CrossRef] [PubMed]
- Maconochie, I.; Simpson, S.; Bingham, B. Teaching children basic life support skills. BMJ 2007, 334, 1174. [Google Scholar] [CrossRef] [PubMed]
- Patsaki, A.; Pantazopoulos, I.; Dontas, I.; Passali, C.; Papadimitriou, L.; Xanthos, T. Evaluation of Greek High School Teachers’ Knowledge in Basic Life Support, Automated External Defibrillation, and Foreign Body Airway Obstruction: Implications for Nursing Interventions. J. Emerg. Nurs. 2012, 38, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Plant, N.; Taylor, K. How best to teach CPR to schoolchildren: A systematic review. Resuscitation 2013, 84, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Lukas, R.-P.; Van Aken, H.; Mölhoff, T.; Weber, T.; Rammert, M.; Wild, E.; Bohn, A. Kids save lives: A six-year longitudinal study of schoolchildren learning cardiopulmonary resuscitation: Who should do the teaching and will the effects last? Resuscitation 2016, 101, 35–40. [Google Scholar] [CrossRef]
- Martínez-Isasi, S.; Abelairas-Gómez, C.; Pichel-López, M.; Barcala-Furelos, R.; Varela-Casal, C.; Vázquez-Santamariña, D.; Sánchez-Santos, L.; Rodríguez-Núñez, A. Learning to resuscitate at school. Study in 8–12 year-old schoolchildren. An. Pediatría Engl. Ed. 2022, 96, 17–24. [Google Scholar] [CrossRef]
- Otero-Agra, M.; Varela-Casal, C.; Castillo-Pereiro, N.; Casillas-Cabana, M.; San Román-Mata, S.; Barcala-Furelos, R.; Rodríguez-Núñez, A. Can we train the chain of survival while playing? Validation of the tool «Rescube». An. Pediatría Engl. Ed. 2021, 94, 213–222. [Google Scholar] [CrossRef]
- Baldi, E.; Bertaia, D. School children learn BLS better and in less time than adults. Resuscitation 2014, 85, S36–S37. [Google Scholar] [CrossRef]
- Garcia del Aguila, J.J.; López Rebollo, E.; Escamilla Pérez, R.; Luque Gutiérrez, M.; Fernández Valle, P.; García Sánchez, M.; Lucena Serrano, C.; Vivar Díaz, I.; Berbel González, F.; Pérez López, S.; et al. Formación de escolares en soporte vital básico por sus propios profesores. Emerg. Rev. Soc. Española Med. Urgenc. Y Emerg. 2019, 31, 185–188. [Google Scholar]
- Nakanishi, T.; Goto, T.; Kobuchi, T.; Kimura, T.; Hayashi, H.; Tokuda, Y. The effects of flipped learning for bystander cardiopulmonary resuscitation on undergraduate medical students. Int. J. Med. Educ. 2017, 8, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Sharma, N.; Lau, C.S.; Doherty, I.; Harbutt, D. How we flipped the medical classroom. Med. Teach. 2015, 37, 327–330. [Google Scholar] [CrossRef] [PubMed]
- Greif, R.; Lockey, A.; Breckwoldt, J.; Carmona, F.; Conaghan, P.; Kuzovlev, A.; Pflanzl-Knizacek, L.; Sari, F.; Shammet, S.; Scapigliati, A.; et al. European Resuscitation Council Guidelines 2021: Education for resuscitation. Resuscitation 2021, 161, 388–407. [Google Scholar] [CrossRef] [PubMed]
- Bauer-Ramazani, C.; Graney, J.M.; Marshall, H.W.; Sabieh, C. Flipped Learning in TESOL: Definitions, Approaches, and Implementation. TESOL J. 2016, 7, 429–437. [Google Scholar] [CrossRef]
- Schmidt, S.M.P.; Ralph, D.L. The flipped classroom: A twist on teaching. Contemp. Issues Educ. Res. 2016, 9, 1–6. [Google Scholar] [CrossRef]
- Ahmed, H.O.K. Flipped Learning As A New Educational Paradigm: An Analytical Critical Study. Eur. Sci. J. 2016, 12, 417. [Google Scholar] [CrossRef]
- Castellanos Sánchez, A.; Sánchez Romero, C.; Calderero Hernández, J.F. Nuevos modelos tecnopedagógicos. Competencia digital de los alumnos universitarios. Rev. Electrónica Investig. Educ. 2017, 19, 1–9. [Google Scholar] [CrossRef]
- Kelley, J.; Richman, P.B.; Ewy, G.A.; Clark, L.; Bulloch, B.; Bobrow, B.J. Eighth grade students become proficient at CPR and use of an AED following a condensed training programme. Resuscitation 2006, 71, 229–236. [Google Scholar] [CrossRef]
- Llanos García, G.; Bravo-Agapito, J. Flipped classroom como puente hacia nuevos retos en la educación primaria. Rev. Tecnol. Cienc. Educ. 2017, 8, 39–49. [Google Scholar] [CrossRef]
- Xunta de Galicia Proxecto E-Dixgal da Xunta de Galicia. Available online: http://www.edixgal.com/ (accessed on 27 July 2022).
- Ato, M.; López, J.J.; Benavente, A. Un sistema de clasificación de los diseños de investigación en psicología. An. Psicol. 2013, 29, 1038–1059. [Google Scholar] [CrossRef] [Green Version]
- Perkins, G.D.; Handley, A.J.; Koster, R.W.; Castrén, M.; Smyth, M.A.; Olasveengen, T.; Monsieurs, K.G.; Raffay, V. European Resuscitation Council Guidelines for Resuscitation 2015 Section 2. Adult basic life support and automated external defibrillation. Resuscitation 2015, 95, 81–99. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Patón, R.; Cons-Ferreiro, M.; Mecías-Calvo, M.; Romo-Pérez, V. Acquisition of knowledge and skills on cardiopulmonary resuscitation and use of the automated external defibrillator after a training process by Galician schoolteachers. J. Hum. Sport Exerc. 2022; 17, in press. [Google Scholar] [CrossRef]
- Navarro-Paton, R.; Cons-Ferreiro, M.; Romo-Pérez, V. Schoolteacher´s theoretical and skills knowledge on cardiopulmonary resuscitation and use of the automated external defibrillator after a video-training process. Retos 2021, 42, 172–181. [Google Scholar] [CrossRef]
- Olasveengen, T.M.; Mancini, M.E.; Perkins, G.D.; Avis, S.; Brooks, S.; Castrén, M.; Chung, S.P.; Considine, J.; Couper, K.; Escalante, R.; et al. Adult Basic Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 2020, 142, S41–S91. [Google Scholar] [CrossRef]
- Lago-Ballesteros, J.; Basanta-Camiño, S.; Navarro-Paton, R. La enseñanza de los primeros auxilios en educación física: Revisión sistemática acerca de los materiales para su implementación. Retos 2018, 34, 349–355. [Google Scholar] [CrossRef]
- Yeung, J.; Kovic, I.; Vidacic, M.; Skilton, E.; Higgins, D.; Melody, T.; Lockey, A. The School Lifesavers Study—A randomised controlled trial comparing the impact of Lifesaver only, Lifesaver with face-to-face training and face-to-face training only on CPR knowledge, skills and attitudes in UK school children. Resuscitation 2017, 118, e12–e13. [Google Scholar] [CrossRef]
- Abelairas-Gómez, C.; Rodríguez-Núñez, A.; Casillas-Cabana, M.; Romo-Pérez, V.; Barcala-Furelos, R. Schoolchildren as life savers: At what age do they become strong enough? Resuscitation 2014, 85, 814–819. [Google Scholar] [CrossRef]
- Contri, E.; Cornara, S.; Somaschini, A.; Dossena, C.; Tonani, M.; Epis, F.; Zambaiti, E.; Fichtner, F.; Baldi, E. Complete chest recoil during laypersons’ CPR: Is it a matter of weight? Am. J. Emerg. Med. 2017, 35, 1266–1268. [Google Scholar] [CrossRef]
- Mathew, R.; Sahu, A.K.; Thakur, N.; Katyal, A.; Bhoi, S.; Aggarwal, P. Hands-only cardiopulmonary resuscitation training for schoolchildren: A comparison study among different class groups. Turkish J. Emerg. Med. 2020, 20, 186–192. [Google Scholar] [CrossRef]
- Neumar, R.W.; Shuster, M.; Callaway, C.W.; Gent, L.M.; Atkins, D.L.; Bhanji, F.; Brooks, S.C.; de Caen, A.R.; Donnino, M.W.; Ferrer, J.M.E.; et al. Part 1: Executive Summary. Circulation 2015, 132, S315–S367. [Google Scholar] [CrossRef] [Green Version]
- Labuschagne, M.J.; Arbee, A.; de Klerk, C.; de Vries, E.; de Waal, T.; Jhetam, T.; Piest, B.; Prins, J.; Uys, S.; van Wyk, R.; et al. A comparison of the effectiveness of QCPR and conventional CPR training in final-year medical students at a South African university. Afr. J. Emerg. Med. 2022, 12, 106–111. [Google Scholar] [CrossRef] [PubMed]
- AHA. American Heart Association Basic Life Support (BLS) Provider Manual; American Heart Association: Dallas, TX, USA, 2020; ISBN 1616694742. [Google Scholar]
- Pavón-Prieto, M.d.P.; Navarro-Patón, R.; Basanta-Camiño, S.; Regueira-Méndez, C.; Neira-Pájaro, M.Á.; Freire-Tellado, M. Estudio cuasiexperimental para evaluar la capacidad de los escolares para utilizar un desfibrilador externo semiautomático a los 6 meses tras un proceso formativo. Emerg. Rev. Soc. Española Med. Urgenc. Y Emerg. 2016, 28, 114–116. [Google Scholar]
- Soar, J.; Monsieurs, K.G.; Ballance, J.H.W.; Barelli, A.; Biarent, D.; Greif, R.; Handley, A.J.; Lockey, A.S.; Richmond, S.; Ringsted, C.; et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 9. Principles of education in resuscitation. Resuscitation 2010, 81, 1434–1444. [Google Scholar] [CrossRef] [PubMed]
- Jorge-Soto, C.; Abelairas-Gómez, C.; Barcala-Furelos, R.; Garrido-Viñas, A.; Navarro-Patón, R.; Muiño-Piñeiro, M.; Díaz-Pereira, M.P.; Rodríguez-Núñez, A. Automated external defibrillation skills by naive schoolchildren. Resuscitation 2016, 106, 37–41. [Google Scholar] [CrossRef]
- Méndez-Martínez, C.; Martínez-Isasi, S.; García-Suárez, M.; De La Peña-Rodríguez, M.A.; Gómez-Salgado, J.; Fernández-García, D. Acquisition of Knowledge and Practical Skills after a Brief Course of BLS-AED in First-Year Students in Nursing and Physiotherapy at a Spanish University. Int. J. Environ. Res. Public Health 2019, 16, 766. [Google Scholar] [CrossRef]
- Basanta Camiño, S.; Navarro Patón, R.; Freire Tellado, M.; Barcala Furelos, R.; Pavón Prieto, M.P.; Fernández López, M.; Neira Pájaro, M.A. Evaluación del conocimiento y de las habilidades para el uso de un Desfibrilador Externo Automatizado (DEA) por estudiantes universitarios. Un diseño cuasiexperimental. Med. Intensiva 2017, 41, 270–276. [Google Scholar] [CrossRef]
- Navarro-Patón, R.; Freire-Tellado, M.; Pavón-Prieto, M.d.P.; Vázquez-López, D.; Neira-Pájaro, M.; Lorenzana-Bargueiras, S. Dispatcher assisted CPR: Is it still important to continue teaching lay bystander CPR? Am. J. Emerg. Med. 2017, 35, 569–573. [Google Scholar] [CrossRef]
- Navarro-Patón, R.; Freire-Tellado, M.; Mateos-Lorenzo, J.; Basanta-Camiño, S.; Rodríguez-López, A.; Lago-Ballesteros, J. Sports Activities with Musical Support: A New Way to Learn Cardiopulmonary Resuscitation? Rev. Int. Med. Ciencias Act. Física Deport. 2020, 20, 243–255. [Google Scholar] [CrossRef]
- De Buck, E.; Van Remoortel, H.; Dieltjens, T.; Verstraeten, H.; Clarysse, M.; Moens, O.; Vandekerckhove, P. Evidence-based educational pathway for the integration of first aid training in school curricula. Resuscitation 2015, 94, 8–22. [Google Scholar] [CrossRef]
- Pierce, R.; Fox, J. Vodcasts and Active-Learning Exercises in a “Flipped Classroom” Model of a Renal Pharmacotherapy Module. Am. J. Pharm. Educ. 2012, 76, 196. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variable | Control Group (n = 160) | Experimental Group (n = 148) | p-Value |
|---|---|---|---|
| Age (years) | 10.65 ± 0.71 | 10.70 ± 0.56 | 0.474 |
| Gender (male/female) | 86/74 | 84/64 | 0.596 |
| Weight (Kg) | 46.17 ± 13.34 | 46.22 ± 11.04 | 0.969 |
| Height (cm) | 150.69 ± 14.49 | 150.56 ± 8.76 | 0.926 |
| Body mass index (kg·m−2) | 20.23 ± 4.46 | 20.28 ± 3.91 | 0.921 |
| Previous training received (yes/no) | 26/134 | 52/96 | <0.001 |
| CPR action sequence (correct/incorrect) | 0/308 | 0/160 | 1.000 |
| AED action sequence (correct/incorrect) | 0/308 | 0/160 | 1.000 |
| Control Group | Experimental Group | ||
|---|---|---|---|
| Scene security | No | 60 (19.5%) | 20 (6.5%) |
| Yes | 100 (32.5%) | 128 (41.6%) | |
| Consciousness assessment | No | 12 (3.9%) | 22 (7.1%) |
| Yes | 148 (48.1%) | 126 (40.9%) | |
| Respiration assessment | No | 6 (1.9%) | 0 (0.0%) |
| Yes | 154 (50.0%) | 148 (48.1%) | |
| Emergency call | No | 54 (17.5%) | 28 (9.1%) |
| Yes | 106 (34.4%) | 120 (39.0%) | |
| Hand placement | Incorrect | 2 (0.6%) | 0 (0.0%) |
| Correct | 158 (51.3%) | 148 (48.1%) |
| Control Group | Experimental Group | ||||
|---|---|---|---|---|---|
| Variable | M | SD | M | SD | |
| MCD (mm) | boys | 28.37 | 8.3 | 27.64 | 8.06 |
| girls | 29.41 | 9.34 | 26.63 | 7.60 | |
| Total | 28.85 | 8.80 | 27.20 | 7.86 | |
| CRP (%) | boys | 85.51 | 24.94 | 94.33 | 7.31 |
| girls | 89.22 | 18.93 | 88.84 | 17.83 | |
| Total | 87.23 | 22.37 | 91.96 | 13.19 | |
| TNC (2 min) | boys | 203.33 | 52.66 | 215.31 | 39.03 |
| girls | 225.27 | 63.30 | 219.34 | 41.11 | |
| Total | 213.48 | 58.58 | 217.05 | 39.86 | |
| PCC (%) | boys | 2.88 | 7.19 | 1.88 | 8.63 |
| girls | 4.43 | 12.25 | 0.75 | 2.39 | |
| Total | 3.60 | 9.86 | 1.39 | 6.79 | |
| Control Group | Experimental Group | ||
|---|---|---|---|
| Objective exceeded | No | 4 (2.5%) | 0 (0.0%) |
| Yes | 156 (97.5%) | 148 (100%) | |
| Security | No | 12 (7.7%) | 0 (0.00%) |
| Yes | 144 (92.3%) | 148 (100%) | |
| Quality objective | No | 12 (7.7%) | 0 (0.00%) |
| Yes | 144 (92.3%) | 148 (100%) |
| Variable | Boys | Girls | Total | ||||
|---|---|---|---|---|---|---|---|
| Group | Mean | SD | Mean | SD | Mean | SD | |
| AED application time (S) | Control | 64.95 | 14.02 | 63.75 | 10.39 | 64.40 | 12.45 |
| Experimental | 65.61 | 10.41 | 62.43 | 7.68 | 64.24 | 9.43 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cons-Ferreiro, M.; Mecías-Calvo, M.; Romo-Pérez, V.; Navarro-Patón, R. The Effects of an Intervention Based on the Flipped Classroom on the Learning of Basic Life Support in Schoolchildren Aged 10–13 Years: A Quasi-Experimental Study. Children 2022, 9, 1373. https://doi.org/10.3390/children9091373
Cons-Ferreiro M, Mecías-Calvo M, Romo-Pérez V, Navarro-Patón R. The Effects of an Intervention Based on the Flipped Classroom on the Learning of Basic Life Support in Schoolchildren Aged 10–13 Years: A Quasi-Experimental Study. Children. 2022; 9(9):1373. https://doi.org/10.3390/children9091373
Chicago/Turabian StyleCons-Ferreiro, Miguel, Marcos Mecías-Calvo, Vicente Romo-Pérez, and Rubén Navarro-Patón. 2022. "The Effects of an Intervention Based on the Flipped Classroom on the Learning of Basic Life Support in Schoolchildren Aged 10–13 Years: A Quasi-Experimental Study" Children 9, no. 9: 1373. https://doi.org/10.3390/children9091373