
A Point-of-Care Digital Workflow for 3D Printed Passive Presurgical Orthopedic Plates in Cleft Care
 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
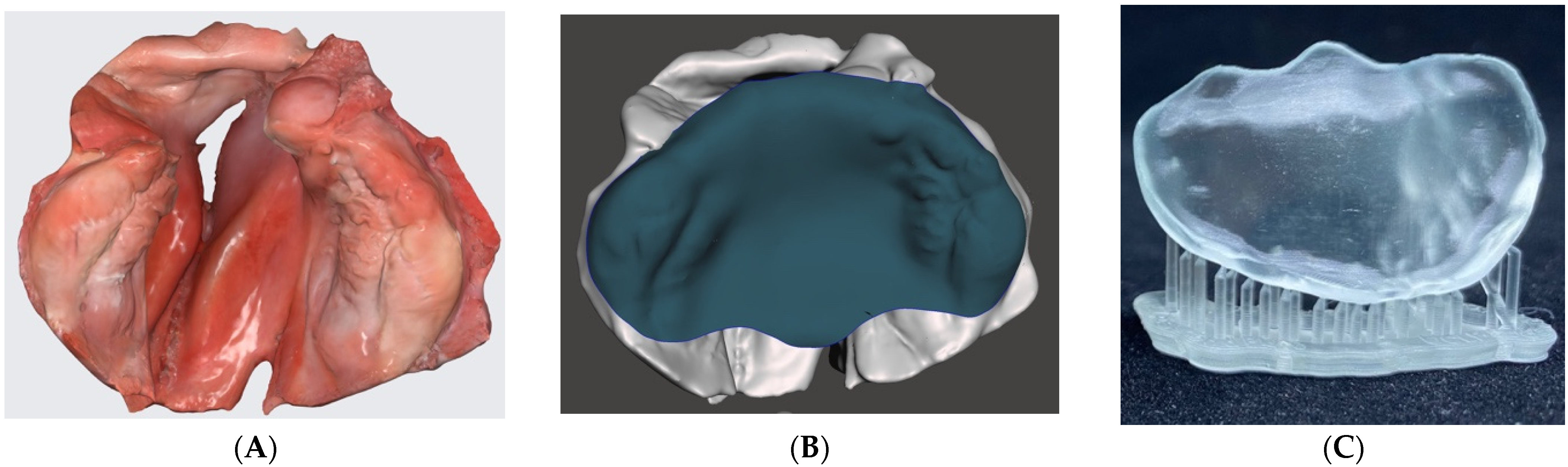
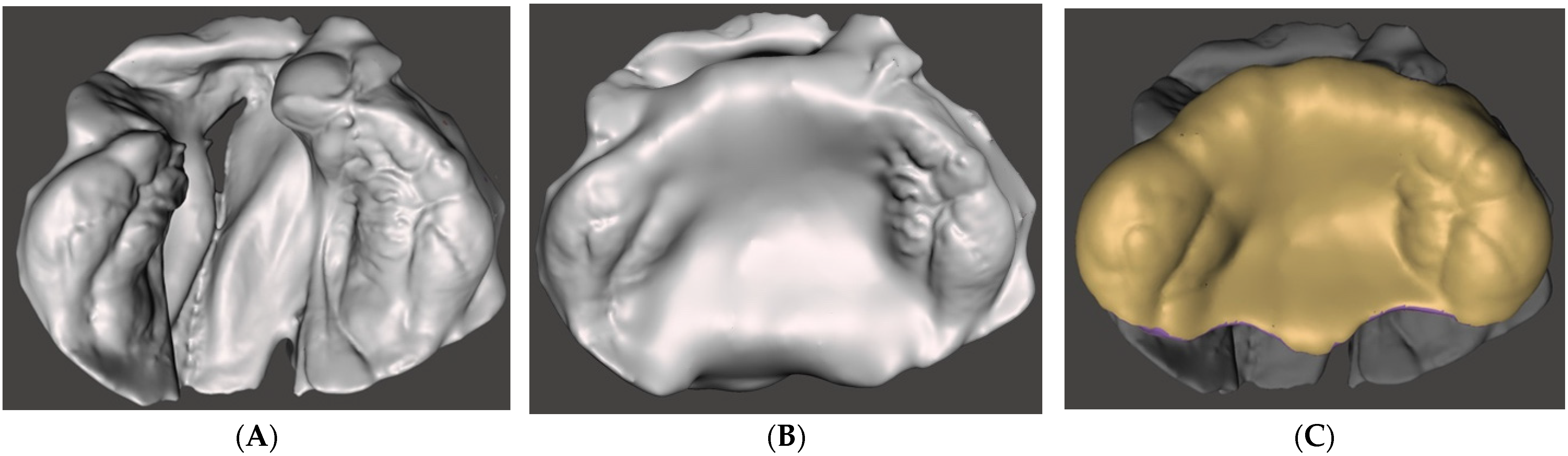
2.1. Three-Dimensional (3D) Digital Image Data Acquisition
2.2. Computer-Aided Design (CAD) Modeling
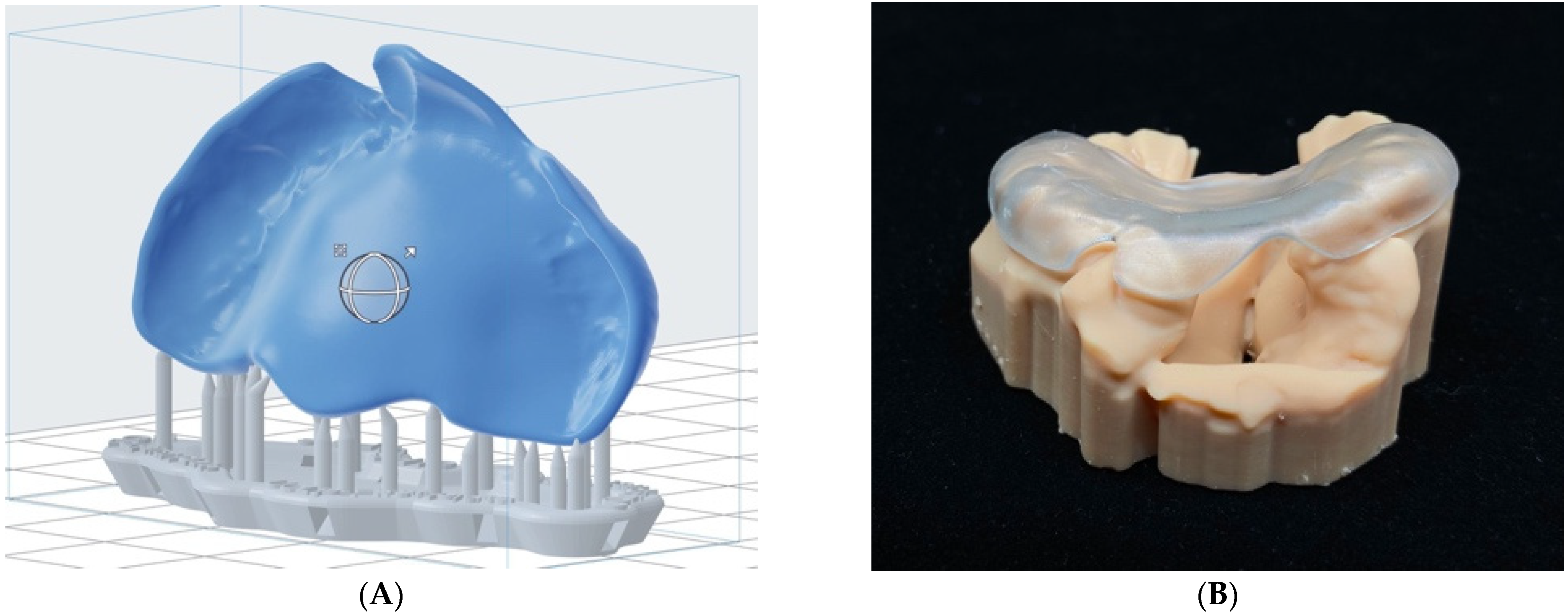
2.3. 3D Printing of Anatoical Cleft Model and Passive Presurgical Orthopedic Plate
3. Results
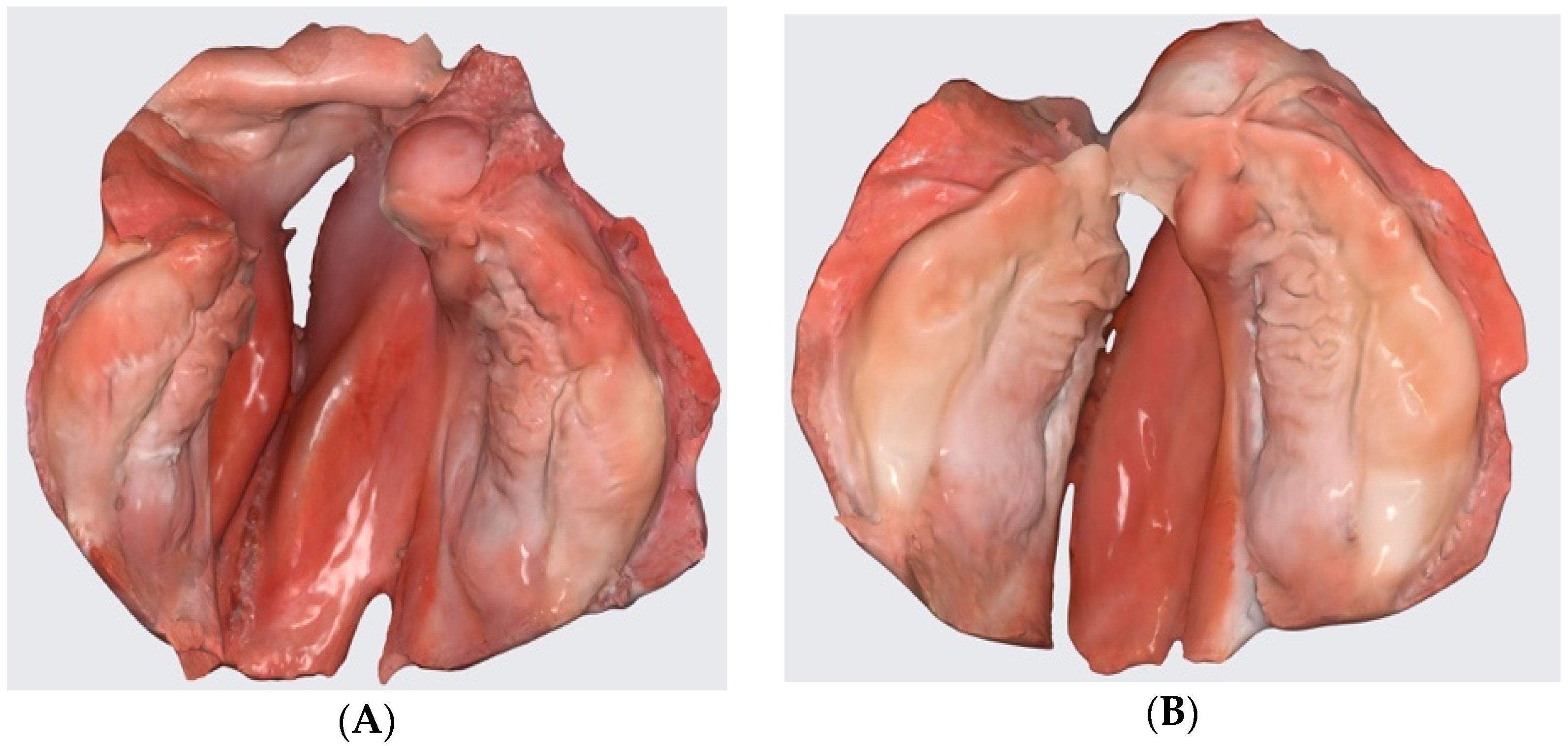
3.1. Three-Dimensional (3D) Digital Image Data Acquisition
3.2. Computer-Aided Design (CAD) Modeling
3.3. 3D Printing of Anatomical Cleft Model and Passive Presurgical Orthopedic Plate
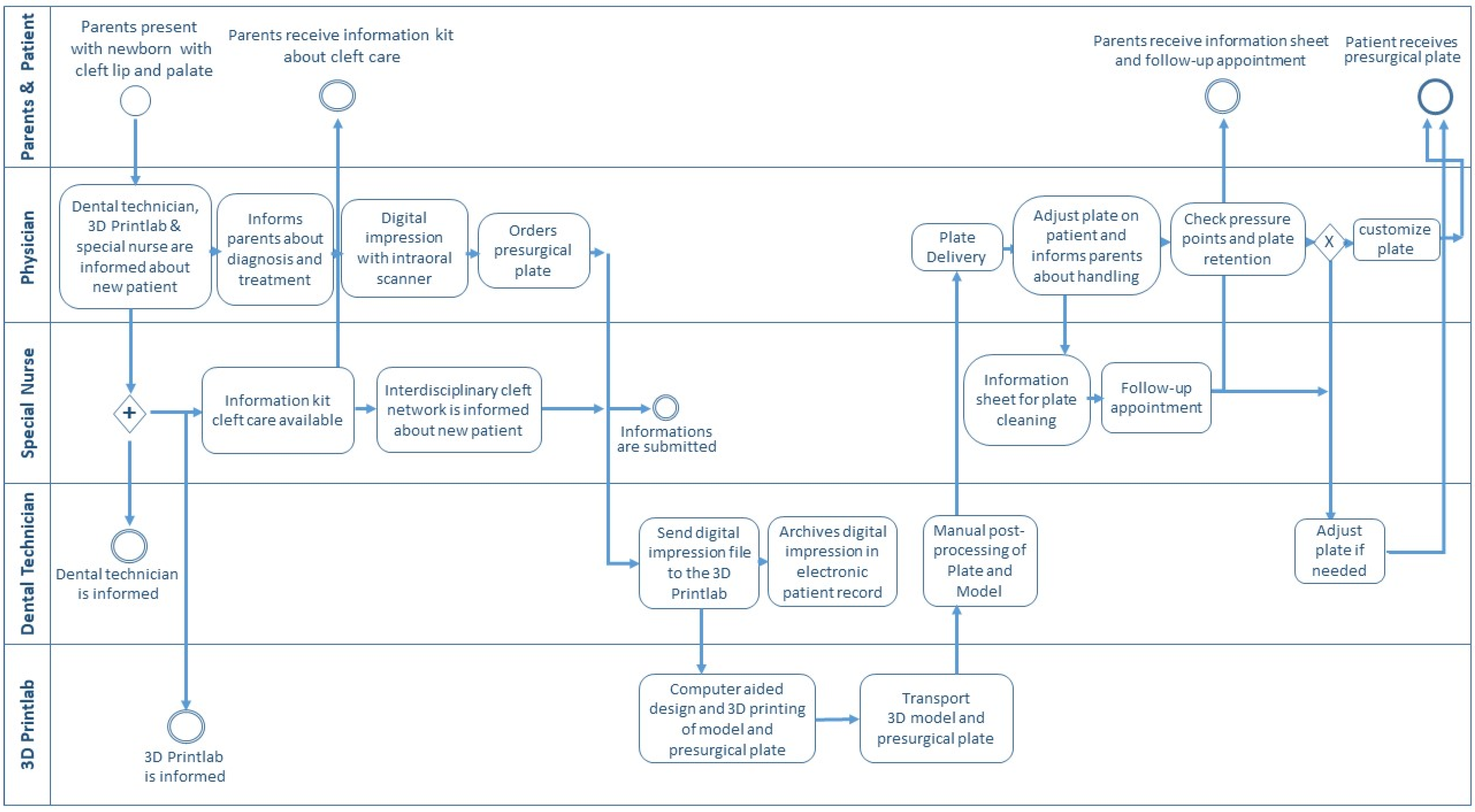
3.4. The Clinical Transition from Conventional to a Digital Workflow for Presurgical Treatment
4. Discussion
4.1. Clinical Relevance
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McNeil, C.K. Orthodontic procedures in the treatment of congenital cleft palate. Dent. Rec. 1950, 70, 126–132. [Google Scholar]
- Hotz, M.M.; Gnoinski, W.M.; Nussbaumer, H.; Kistler, E. Early maxillary orthopedics in CLP cases: Guidelines for surgery. Cleft Palate J. 1978, 15, 405–411. [Google Scholar]
- Grayson, B.H.; Cutting, C.B. Presurgical nasoalveolar orthopedic molding in primary correction of the nose, lip, and alveolus of infants born with unilateral and bilateral clefts. Cleft Palate Craniofacial J. 2001, 38, 193–198. [Google Scholar] [CrossRef]
- Latham, R.A.; Kusy, R.P.; Georgiade, N.G. An extraorally activated expansion appliance for cleft palate infants. Cleft Palate J. 1976, 13, 253–261. [Google Scholar]
- Koželj, V. Experience with presurgical nasal molding in infants with cleft lip and nose deformity. Plast. Reconstr. Surg. 2007, 120, 738–745. [Google Scholar] [CrossRef]
- Benitez, B.K.; Brudnicki, A.; Surowiec, Z.; Singh, R.K.; Nalabothu, P.; Schumann, D.; Mueller, A.A. Continuous circular closure in unilateral cleft lip and plate repair in one surgery. J. Cranio-Maxillofac. Surg. 2022, 50, 76–85. [Google Scholar] [CrossRef]
- Grayson, B.H.; Cutting, C.; Wood, R. Preoperative columella lengthening in bilateral cleft lip and palate. Plast. Reconstr. Surg. 1993, 92, 1422–1423. [Google Scholar]
- Grayson, B.H.; Santiago, P.E.; Brecht, L.E.; Cutting, C.B. Presurgical nasoalveolar molding in infants with cleft lip and palate. Cleft Palate Craniofacial J. 1999, 36, 486–498. [Google Scholar] [CrossRef]
- Reichert, F.; Amrhein, P.; Uhlemann, F. Unnoticed aspiration of palate plate impression material in a neonate: Diagnosis, therapy, outcome. Pediatr. Pulmonol. 2017, 52, E58–E60. [Google Scholar] [CrossRef]
- Chate, R.A.C. A report on the hazards encountered when taking neonatal cleft palate impressions (1983–1992). Br. J. Orthod. 1995, 22, 299–307. [Google Scholar] [CrossRef]
- Weise, C.; Frank, K.; Wiechers, C.; Weise, H.; Reinert, S.; Koos, B.; Xepapadeas, A.B. Intraoral scanning of neonates and infants with craniofacial disorders: Feasibility, scanning duration, and clinical experience. Eur. J. Orthod. 2022, 44, 279–286. [Google Scholar] [CrossRef]
- Gong, X.; Dang, R.; Xu, T.; Yu, Q.; Zheng, J. Full Digital Workflow of Nasoalveolar Molding Treatment in Infants with Cleft Lip and Palate. J. Craniofacial Surg. 2020, 31, 367–371. [Google Scholar] [CrossRef]
- Benitez, B.K.; Brudnicki, A.; Surowiec, Z.; Wieprzowski, Ł.; Rasadurai, A.; Nalabothu, P.; Lill, Y.; Mueller, A.A. Digital Impressions from Newborns to Preschoolers with Cleft Lip and Palate: A Two-Centers Experience. J. Plast. Reconstr. Aesthet. Surg. 2022. Accepted for Publication. [Google Scholar] [CrossRef]
- El-Ashmawi, N.A.; Fayed, M.M.S.; El-Beialy, A.; Attia, K.H. Evaluation of the Clinical Effectiveness of Nasoalveolar Molding (NAM) Using Grayson Method Versus Computer-Aided Design NAM (CAD/NAM) in Infants with Bilateral Cleft Lip and Palate: A Randomized Clinical Trial. Cleft Palate Craniofacial J. 2022, 59, 377–389. [Google Scholar] [CrossRef]
- Bauer, F.X.; Gau, D.; Gull, F.; Eblenkamp, M.; Loeffelbein, D.J. Automated detection of alveolar arches for nasoalveolar molding in cleft lip and palate treatment. Curr. Dir. Biomed. Eng. 2016, 2, 701–705. [Google Scholar] [CrossRef]
- Xepapadeas, A.B.; Weise, C.; Frank, K.; Spintzyk, S.; Poets, C.F.; Wiechers, C.; Arand, J.; Koos, B. Technical note on introducing a digital workflow for newborns with craniofacial anomalies based on intraoral scans—Part I: 3D printed and milled palatal stimulation plate for trisomy 21. BMC Oral Health 2020, 20, 20. [Google Scholar] [CrossRef]
- Sharma, N.; Cao, S.; Msallem, B.; Kunz, C.; Brantner, P.; Honigmann, P.; Thieringer, F.M. Effects of Steam Sterilization on 3D Printed Biocompatible Resin Materials for Surgical Guides-An Accuracy Assessment Study. J. Clin. Med. 2020, 9, 1506. [Google Scholar] [CrossRef]
- Formlabs. Available online: https://formlabs.com/de/shop/biomed-clear-resin/ (accessed on 3 May 2022).
- Formlabs. Available online: https://support.formlabs.com/s/article/Form-Cure-Time-and-Temperature-Settings?language=en_US#download (accessed on 3 May 2022).
- Renne, W.; Ludlow, M.; Fryml, J.; Schurch, Z.; Mennito, A.; Kessler, R.; Lauer, A. Evaluation of the accuracy of 7 digital scanners: An in vitro analysis based on 3-dimensional comparisons. J. Prosthet. Dent. 2017, 118, 36–42. [Google Scholar] [CrossRef]
- Jensen, S.W.C.; Jensen, E.D.; Kaminer-Levin, G.; Caro, C.; Stevens, K. Presurgical Cleft Management of Infants: A Survey of ACPA Approved and International Cleft Palate and Craniofacial Teams. Cleft Palate Craniofacial J. 2022, 20, 10556656221109416. [Google Scholar] [CrossRef]
- Nalabothu, P.; Benitez, B.K.; Dalstra, M.; Verna, C.; Mueller, A.A. Three-Dimensional Morphological Changes of the True Cleft under Passive Presurgical Orthopaedics in Unilateral Cleft Lip and Palate: A Retrospective Cohort Study. J. Clin. Med. 2020, 9, 962. [Google Scholar] [CrossRef] [Green Version]
- Benitez, B.K.; Brudnicki, A.; Nalabothu, P.; Jackowski, J.A.V.; Bruder, E.; Mueller, A.A. Histologic Aspect of the Curved Vomerine Mucosa in Cleft Lip and Palate. Cleft Palate Craniofacial J. 2022, 59, 1048–1055. [Google Scholar] [CrossRef]
- Chiu, A.; Chen, Y.W.; Hayashi, J.; Sadr, A. Accuracy of CAD/CAM Digital Impressions with Different Intraoral Scanner Parameters. Sensors 2020, 20, 1157. [Google Scholar] [CrossRef] [Green Version]
- Griffin, R.; Botond, S.; Anthony, M.; Zachary, P.; Walter, R.; Mark, L.; János, V. Evaluation of complete-arch implant scanning with 5 different intraoral scanners in terms of trueness and operator experience. J. Prosthet. Dent. 2021, in press. [Google Scholar] [CrossRef]
- Aretxabaleta, M.; Unkovskiy, A.; Koos, B.; Spintzyk, S.; Xepapadeas, A.B. Accuracy evaluation of additively and subtractively fabricated palatal plate orthodontic appliances for newborns and infants-an in vitro study. Materials 2021, 14, 4103. [Google Scholar] [CrossRef]
- Poets, C.F.; Wiechers, C.; Koos, B.; Muzaffar, A.R.; Gozal, D. Pierre Robin and breathing: What to do and when? Pediatr. Pulmonol. 2022, 57, 1887–1896. [Google Scholar] [CrossRef]
- Xepapadeas, A.B.; Weise, C.; Frank, K.; Spintzyk, S.; Poets, C.F.; Wiechers, C.; Arand, J.; Koos, B. Technical note on introducing a digital workflow for newborns with craniofacial anomalies based on intraoral scans—Part II: 3D printed Tübingen palatal plate prototype for newborns with Robin sequence. BMC Oral Health 2020, 20, 171. [Google Scholar] [CrossRef]
- Botnar Research Center for Child Health Home Page. Available online: https://brc.ch/research/cleft-lip-and-palate/ (accessed on 5 August 2022).
- Alfonso, A.R.; Ramly, E.P.; Kantar, R.S.; Wang, M.M.; Eisemann, B.S.; Staffenberg, D.A.; Shetye, P.R.; Flores, R.L. What Is the Burden of Care of Nasoalveolar Molding? Cleft Palate Craniofacial J. 2020, 57, 1078–1092. [Google Scholar] [CrossRef]
- Gibson, E.; Pfeifauf, K.D.; Skolnick, G.B.; Kim, A.; Naidoo, S.D.; Snyder-Warwick, A.; Huebener, D.V.; Patel, K.B. Presurgical Orthopedic Intervention Prior to Cleft Lip and Palate Repair: Nasoalveolar Molding Versus Passive Molding Appliance Therapy. J. Craniofacial Surg. 2021, 32, 486–491. [Google Scholar] [CrossRef]
- Wlodarczyk, J.R.; Wolfswinkel, E.M.; Fahradyan, A.; Rhee, C.; Liu, A.; Gibreel, W.; Magee, W., 3rd; Urata, M.M.; Hammoudeh, J.A. Nasoalveolar Molding: Assessing the Burden of Care. J. Craniofacial Surg. 2021, 32, 574–577. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Conventional Workflow | Digital Workflow | |
|---|---|---|
| Impression | ||
| Available readiness of anesthesiology, neonatology team (some centers take an impression in the operating theater) | Yes | No |
| Involvement and presence of parents/caregivers; Parent education, demonstration of treatment progress | No | Yes |
| Known risk for the airway | Yes | No |
| Added stress for clinician | Yes | No |
| Time for setup material and impression taking | 30 min | 15 min |
| The time for impression taking by the physician (conventional vs digital) | 2–5 min | 1–2.5 min |
| Time to obtain a physical plaster cast model | 35 min (technician) | N/A |
| Detail accuracy of the model | Low | High |
| Digitalization of 3D model for archiving | 10 min (scanning required) | automatic |
| Presurgical Plate Fabrication | ||
| Computer-aided design modeling | N/A | 35 min |
| 3D printing time | N/A | 90–180min * |
| Postprocessing printed parts | N/A | 110min * |
| Hands-on plate manufacturing on the plaster cast model | 45 min | N/A |
| Final preparation and polishing of presurgical plate | 15 min | 10 min |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zarean, P.; Zarean, P.; Thieringer, F.M.; Mueller, A.A.; Kressmann, S.; Erismann, M.; Sharma, N.; Benitez, B.K. A Point-of-Care Digital Workflow for 3D Printed Passive Presurgical Orthopedic Plates in Cleft Care. Children 2022, 9, 1261. https://doi.org/10.3390/children9081261
Zarean P, Zarean P, Thieringer FM, Mueller AA, Kressmann S, Erismann M, Sharma N, Benitez BK. A Point-of-Care Digital Workflow for 3D Printed Passive Presurgical Orthopedic Plates in Cleft Care. Children. 2022; 9(8):1261. https://doi.org/10.3390/children9081261
Chicago/Turabian StyleZarean, Parichehr, Paridokht Zarean, Florian M. Thieringer, Andreas A. Mueller, Sabine Kressmann, Martin Erismann, Neha Sharma, and Benito K. Benitez. 2022. "A Point-of-Care Digital Workflow for 3D Printed Passive Presurgical Orthopedic Plates in Cleft Care" Children 9, no. 8: 1261. https://doi.org/10.3390/children9081261