
Hyponatremia—A New Diagnostic Marker for Complicated Acute Appendicitis in Children: A Systematic Review and Meta-Analysis

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
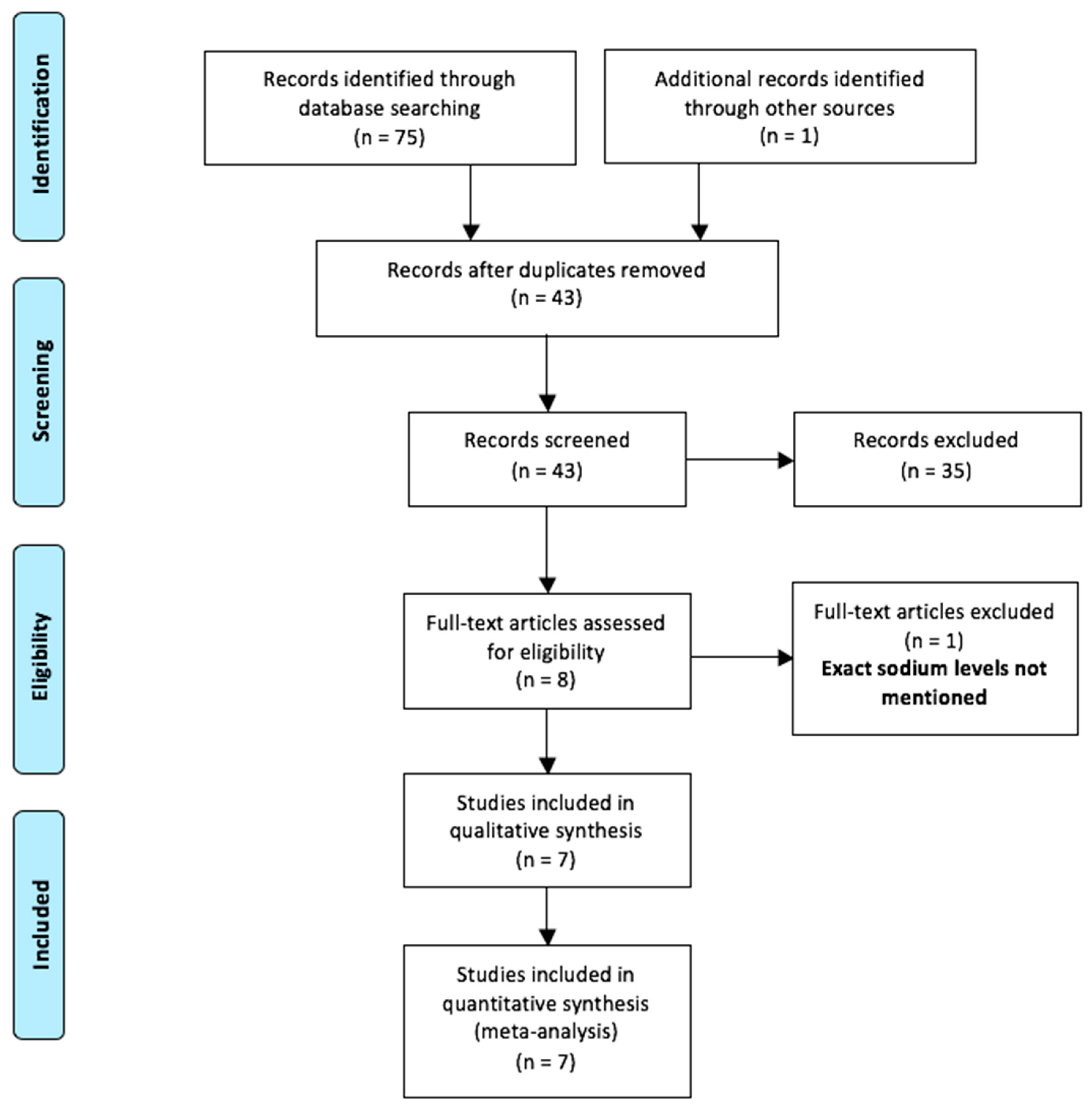
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Included Studies
3.2. Summary of the Included Studies
3.3. Methodological Quality Assessment
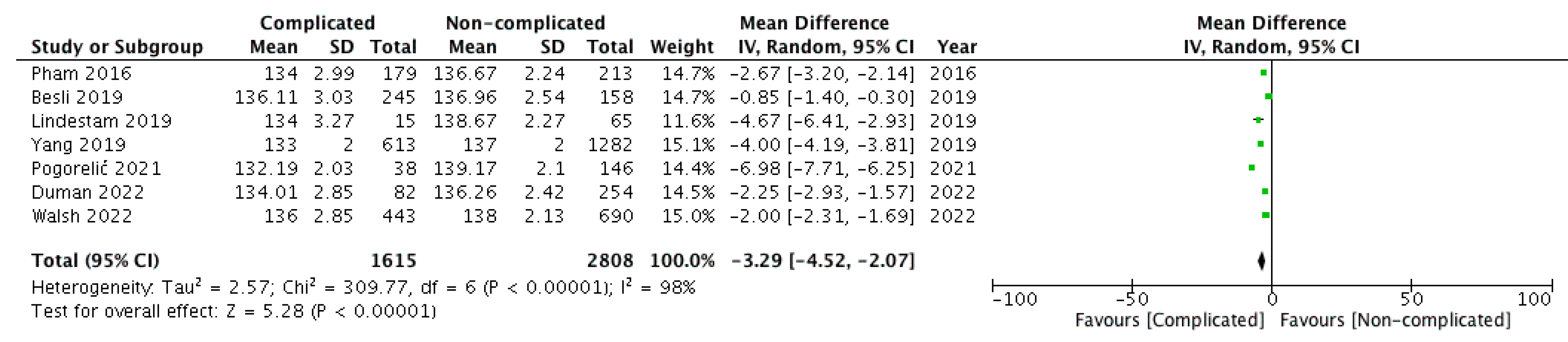
3.4. Outcome Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- PubMed: (hyponatremia) AND (appendicitis) AND (children)
- Embase: (‘hyponatremia’/exp OR hyponatremia) AND (‘appendicitis’/exp OR appendicitis) AND (‘child’/exp OR child)
- Scopus: (TITLE-ABS-KEY (hyponatremia) AND TITLE-ABS-KEY (appendicitis) AND TITLE-ABS-KEY (children))
- Web of Science: Query 1: ALL = (hyponatremia) AND Query 2: ALL = (appendicitis) AND Query 3: (children)

{kind=link}
{kind=link}
| Database | Studies |
|---|---|
| PubMed | 11 |
| Embase | 25 |
| Scopus | 26 |
| Web of Science | 13 |
| Additional records from other sources | 01 |
| Total | 76 |
| Duplications | 33 |
| After duplications removal | 43 |
References
- Howell, E.; Dubina, E.; Lee, S. Perforation risk in pediatric appendicitis: Assessment and management. Pediatr. Health Med. Ther. 2018, 9, 135–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pogorelić, Z.; Domjanović, J.; Jukić, M.; Poklepović Peričić, T. Acute appendicitis in children younger than five years of age: Diagnostic challenge for pediatric surgeons. Surg. Infect. 2020, 21, 239–245. [Google Scholar] [CrossRef]
- Araim, F.; Shmelev, A.; Kowdley, G.C. Incidence of complicated appendicitis as a metric of health care delivery. Am. Surg. 2022, 88, 597–607. [Google Scholar] [CrossRef]
- Gray, D.T.; Mizrahi, T. Trends in appendicitis and perforated appendicitis prevalence in children in the United States, 2001–2015. JAMA Netw. Open. 2020, 3, e2023484. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Rak, S.; Mrklić, I.; Jurić, I. Prospective validation of Alvarado score and Pediatric Appendicitis Score for the diagnosis of acute appendicitis in children. Pediatr. Emerg. Care 2015, 31, 164–168. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Mihanović, J.; Ninčević, S.; Lukšić, B.; Elezović Baloević, S.; Polašek, O. Validity of appendicitis inflammatory response score in distinguishing perforated from non-perforated appendicitis in children. Children 2021, 8, 309. [Google Scholar] [CrossRef] [PubMed]
- Almaramhy, H.H. Acute appendicitis in young children less than 5 years: Review article. Ital. J. Pediatr. 2017, 43, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez Otero, S.; Metzger, J.W.; Choi, B.H.; Ramaraj, A.; Tashiro, J.; Kuenzler, K.A.; Ginsburg, H.B.; Tomita, S.S.; Fisher, J.C. It’s time to deconstruct treatment-failure: A randomized controlled trial of nonoperative management of uncomplicated pediatric appendicitis with antibiotics alone. J. Pediatr. Surg. 2022, 57, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Pogorelić, Z.; Anand, S.; Žuvela, T.; Singh, A.; Križanac, Z.; Krishnan, N. Incidence of complicated appendicitis during the COVID-19 pandemic versus the pre-pandemic period: A systematic review and meta-analysis of 2782 pediatric appendectomies. Diagnostics 2022, 12, 127. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Lukšić, B.; Ninčević, S.; Lukšić, B.; Polašek, O. Hyponatremia as a predictor of perforated acute appendicitis in pediatric population: A prospective study. J. Pediatr. Surg. 2021, 56, 1816–1821. [Google Scholar] [CrossRef]
- Lindestam, U.; Almström, M.; Jacks, J.; Malmquist, P.; Lönnqvist, P.A.; Jensen, B.L.; Carlström, M.; Krmar, R.T.; Svensson, J.F.; Norberg, Å.; et al. Low plasma sodium concentration predicts perforated acute appendicitis in children: A prospective diagnostic accuracy study. Eur. J. Pediatr. Surg. 2020, 30, 350–356. [Google Scholar]
- Giannis, D.; Matenoglou, E.; Moris, D. Hyponatremia as a marker of complicated appendicitis: A systematic review. Surgeon 2020, 18, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Swart, R.M.; Hoorn, E.J.; Betjes, M.G.; Zietse, R. Hyponatremia and inflammation: The emerging role of interleukin-6 in osmoregulation. Nephron Physiol. 2011, 118, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Pham, X.D.; Sullins, V.F.; Kim, D.Y.; Range, B.; Kaji, A.H.; de Virgilio, C.M.; Lee, S.L. Factors predictive of complicated appendicitis in children. J. Surg. Res. 2016, 206, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Besli, G.E.; Çetin, M.; Durakbasa, C.U.; Ozkanli, S. Predictive value of serum sodium level in determining complicated appendicitis risk in children. Haydarpasa Numune Med. J. 2019, 59, 35–40. [Google Scholar] [CrossRef]
- Yang, J.; Liu, C.; He, Y.; Cai, Z. Laboratory markers in the prediction of acute perforated appendicitis in children. Emerg. Med. Int. 2019, 2019, 4608053. [Google Scholar] [CrossRef]
- Duman, L.; Karaibrahimoğlu, A.; Büyükyavuz, B.İ.; Savaş, M.Ç. Diagnostic value of monocyte-to-lymphocyte ratio against other biomarkers in children with appendicitis. Pediatr. Emerg. Care 2022, 38, e739–e742. [Google Scholar] [CrossRef]
- Walsh, A.; Lala, S.; Wells, C.; Upadhyay, V. Hyponatremia an indicator of complicated appendicitis in children: Starship experience. ANZ J. Surg. 2022, 92, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Serradilla, J.; Bueno, A.; De la Torre, C.; Domínguez, E.; Sánchez, A.; Nava, B.; Álvarez, M.; López Santamaría, M.; Martínez, L. Predictive factors of gangrenous post-appendectomy intra-abdominal abscess. A case-control study. Cir. Pediatr. 2018, 31, 25–28. [Google Scholar] [PubMed]
- Glass, C.; Rangel, S. Overview and diagnosis of acute appendicitis in children. Semin. Pediatr. Surg. 2016, 25, 198–203. [Google Scholar] [CrossRef]
- Teoule, P.; de Laffolie, J.; Rolle, U.; Reissfelder, C. Acute appendicitis in childhood and adulthood. Dtsch. Arztebl. Int. 2020, 117, 764–774. [Google Scholar]
- Stringer, M. Acute appendicitis. J. Paediatr. Child Health 2017, 53, 1071–1076. [Google Scholar] [CrossRef]
- Livingston, E.H.; Woodward, W.A.; Sarosi, G.A.; Haley, R.W. Disconnect between incidence of nonperforated and perforated appendicitis. Ann. Surg. 2007, 245, 886–892. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Beara, V.; Jukić, M.; Rashwan, H.; Šušnjar, T. A new approach to laparoscopic appendectomy in children-clipless/sutureless harmonic scalpel laparoscopic appendectomy. Langenbecks Arch Surg. 2022, 407, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Peter, S.D.S.; Sharp, S.W.; Holcomb, G.W.; Ostlie, D.J. An evidence-based definition for perforated appendicitis derived from a prospective randomized trial. J. Pediatr. Surg. 2008, 43, 2242–2245. [Google Scholar] [CrossRef]
- Lee, S.L.; Ho, H.S. Acute appendicitis: Is there a difference between children and adults? Am Surg. 2006, 72, 409–413. [Google Scholar] [CrossRef]
- Pogorelic, Z.; Buljubasic, M.; Susnjar, T.; Jukic, M.; Pericic, T.P.; Juric, I. Comparison of open and laparoscopic appendectomy in children: A 5-year single center experience. Indian Pediatr. 2019, 56, 299–303. [Google Scholar] [CrossRef]
- Perko, Z.; Bilan, K.; Pogorelić, Z.; Druzijanić, N.; Srsen, D.; Kraljević, D.; Juricić, J.; Krnić, D. Acute appendicitis and ileal perforation with a toothpick treated by laparoscopy. Coll. Antropol. 2008, 32, 307–309. [Google Scholar] [PubMed]
- Pogorelić, Z.; Silov, N.; Jukić, M.; Elezović Baloević, S.; Poklepović Peričić, T.; Jerončić, A. Ertapenem Monotherapy versus Gentamicin Plus Metronidazole for Perforated Appendicitis in Pediatric Patients. Surg. Infect. 2019, 20, 625–630. [Google Scholar] [CrossRef]
- Bhangu, A.; Søreide, K.; Di Saverio, S.; Assarsson, J.H.; Drake, F.T. Acute appendicitis: Modern understanding of pathogenesis, diagnosis, and management. Lancet 2015, 386, 1278–1287. [Google Scholar] [CrossRef]
- Shogilev, D.; Duus, N.; Odom, S.; Shapiro, N. Diagnosing appendicitis: Evidence-based review of the diagnostic approach in 2014. West. J. Emerg. Med. 2014, 15, 859–871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frountzas, M.; Stergios, K.; Kopsini, D.; Schizas, D.; Kontzoglou, K.; Toutouzas, K. Alvarado or RIPASA score for diagnosis of acute appendicitis? A meta-analysis of randomized trials. Int. J. Surg. 2018, 56, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Ozkan, S.; Duman, A.; Durukan, P.; Yildirim, A.; Ozbakan, O. The accuracy rate of Alvarado score, ultrasonography, and computerized tomography scan in the diagnosis of acute appendicitis in our center. Niger. J. Clin. Pract. 2014, 17, 413–418. [Google Scholar] [CrossRef]
- Falor, A.E.; Zobel, M.; Kaji, A.; Neville, A.; De Virgilio, C. Admission variables predictive of gangrenous cholecystitis. Am. Surg. 2012, 78, 1075–1078. [Google Scholar] [CrossRef]
- O’Leary, M.P.; Neville, A.L.; Keeley, J.A.; Kim, D.Y.; de Virgilio, C.; Plurad, D.S. Predictors of ischemic bowel in patients with small bowel obstruction. Am. Surg. 2016, 82, 992–994. [Google Scholar] [CrossRef]
- Käser, S.A.; Furler, R.; Evequoz, D.C.; Maurer, C.A. Hyponatremia is a specific marker of perforation in sigmoid diverticulitis or appendicitis in patients older than 50 years. Gastroenterol. Res. Pract. 2013, 2013, 462891. [Google Scholar] [CrossRef]
- Yaghoubian, A.; de Virgilio, C.; Dauphine, C.; Lewis, R.J.; Lin, M. Use of admission serum lactate and sodium levels to predict mortality in necrotizing soft-tissue infections. Arch. Surg. Chic. 2007, 142, 840–846. [Google Scholar] [CrossRef] [Green Version]
- Wong, C.H.; Khin, L.W.; Heng, K.S.; Tan, K.C.; Low, C.O. The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: A tool for distinguishing necrotizing fasciitis from other soft tissue infections. Crit. Care Med. 2004, 32, 1535–1541. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.W.; Fatima, B.; Lahr, B.D.; Greason, K.L.; Schaff, H.V.; Dearani, J.A.; Daly, R.C.; Stulak, J.M.; Crestanello, J.A. Hyponatremia: An overlooked risk factor associated with adverse outcomes after cardiac surgery. Ann. Thorac. Surg. 2021, 112, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Crestanello, J.A.; Phillips, G.; Firstenberg, M.S.; Sai-Sudhakar, C.; Sirak, J.; Higgins, R.; Abraham, W.T. Preoperative hyponatremia predicts outcomes after cardiac surgery. J. Surg. Res. 2013, 181, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Sato, N.; Gheorghiade, M.; Kajimoto, K.; Munakata, R.; Minami, Y.; Mizuno, M.; Aokage, T.; Asai, K.; Sakata, Y.; Yumino, D.; et al. Hyponatremia and in-hospital mortality in patients admitted for heart failure (from the ATTEND registry). Am. J. Cardiol. 2013, 111, 1019–1025. [Google Scholar] [CrossRef]
- Zhang, G.; Lian, R.; Sun, L.; Liu, H.; Wang, Y.; Zhou, L. Redefined hyponatremia as a marker to exclude the diagnosis of anastomotic leakage after colorectal cancer surgery. J. Int. Med. Res. 2020, 48, 300060520950565. [Google Scholar] [CrossRef]
- Leung, A.A.; McAlister, F.A.; Rogers, S.O.; Pazo, V.; Wright, A.; Bates, D.W. Preoperative hyponatremia and perioperative complications. Arch. Intern. Med. 2012, 172, 1474–1481. [Google Scholar] [CrossRef]
- Asadollahi, K.; Beeching, N.; Gill, G. Hyponatraemia as a risk factor for hospital mortality. J. Assoc. Physicians 2006, 99, 877–880. [Google Scholar] [CrossRef]
- Gill, G.; Huda, B.; Boyd, A.; Skagen, K.; Wile, D.; Watson, I.; van Heyningen, C. Characteristics and mortality of severe hyponatraemia-a hospital-based study. Clin. Endocrinol. 2006, 65, 246–249. [Google Scholar] [CrossRef]
- Wald, R.; Jaber, B.L.; Price, L.L.; Upadhyay, A.; Madias, N.E. Impact of hospital-associated hyponatremia on selected outcomes. Arch. Intern Med. 2010, 170, 294–302. [Google Scholar] [CrossRef]
- Waikar, S.S.; Mount, D.B.; Curhan, G.C. Mortality after hospitalization with mild, moderate, and severe hyponatremia. Am. J. Med. 2009, 12, 857–865. [Google Scholar] [CrossRef] [Green Version]
- Zilberberg, M.D.; Exuzides, A.; Spalding, J.; Foreman, A.; Jones, A.G.; Colby, C.; Shorr, A.F. Epidemiology, clinical and economic outcomes of admission hyponatremia among hospitalized patients. Curr. Med. Res. Opin. 2008, 24, 1601–1608. [Google Scholar] [CrossRef] [PubMed]
- Symeonidis., N.G.; Pavlidis, E.T.; Psarras, K.K.; Stavrati, K.; Nikolaidou, C.; Marneri, A.; Geropoulos, G.; Meitanidou, M.; Andreou, E.; Pavlidis., T.E. Preoperative hyponatremia indicates complicated acute appendicitis. Surg. Res. Pract. 2022, 31, 1836754. [Google Scholar] [CrossRef] [PubMed]
- Siegel, A.J. Exercise-associated hyponatremia: Role of cytokines. Am. J. Med. 2006, 119, S74–S78. [Google Scholar] [CrossRef] [PubMed]
- Papanicolaou, D.A.; Wilder, R.L.; Manolagas, S.C.; Chrousos, G.P. The pathophysiologic roles of interleukin-6 in human disease. Ann. Intern. Med. 1998, 128, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Alsaleh, A.; Pellino, G.; Christodoulides, N.; Malietzis, G.; Kontovounisios, C. Hyponatremia could identify patients with intrabdominal sepsis and anastomotic leak after colorectal surgery: A systematic review of the literature. Updates Surg. 2019, 71, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Sharshar, T.; Blanchard, A.; Paillard, M.; Raphael, J.C.; Gajdos, P.; Annane, D. Circulating vasopressin levels in septic shock. Crit. Care Med. 2003, 31, 1752–1758. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Lukšić, A.M.; Mihanović, J.; Đikić, D.; Balta, V. Hyperbilirubinemia as an indicator of perforated acute appendicitis in pediatric population: A prospective study. Surg. Infect. 2021, 22, 1064–1071. [Google Scholar] [CrossRef]
- Rouzrokh, M.; Fard, F.E.; Momeni, N.; Tavassoli, A. Diagnostic role of ESR, CRP, leukocytosis and Neutrophil/Lymphocyte in peripheral blood smear in children under 14 with acute appendicitis. Pajoohandeh J. 2011, 16, 42–46. [Google Scholar]
- Stefanutti, G.; Ghirardo, V.; Gamba, P. Inflammatory markers for acute appendicitis in children: Are they helpful? J. Pediatr. Surg. 2007, 42, 773–776. [Google Scholar] [CrossRef]
- Anand, S.; Krishnan, N.; Jukic, M.; Krizanac, Z.; Llorente Munoz, C.M.; Pogorelic, Z. Utility of red cell distribution width (RDW) as a noninvasive biomarker for the diagnosis of acute appendicitis: A systematic review and meta-analysis of 5222 cases. Diagnostics 2022, 12, 1011. [Google Scholar] [CrossRef]


| Author | Study Design | Sample Size | Gender (% Males) | Other Biomarkers Investigated | ||
|---|---|---|---|---|---|---|
| Gp A | Gp B | Gp A | Gp B | |||
| Pham et al., 2016 [17] | Retro | 179 | 213 | 63% | 69% | WBC |
| Besli et al., 2019 [18] | Retro | 245 | 158 | 70% | 64% | WBC, NP, CRP |
| Lindestam et al., 2019 [11] | Pro | 15 | 65 | 80% | 63% | CRP, WBC, plasma glucose, BE, plasma AVP |
| Yang et al., 2019 [19] | Retro | 613 | 1282 | 54% | 52% | CRP, WBC, NP, PC, PCT, DLAC, Bilirubin, AST, ALT |
| Pogorelić et al., 2021 [10] | Pro | 38 | 146 | 71% | 63% | WBC, CRP, NP, potassium, chloride, glucose |
| Duman et al., 2022 [20] | Retro | 82 | 254 | 2:1 * | CRP, WBC, NP, MLR, NLR, PLR, MPV | |
| Walsh et al., 2022 [21] | Retro | 443 | 690 | 60% | 61.4% | - |
| Study | Reporting | External Validity | Internal Validity-Bias | Internal Validity- Confounding | Power | Total Scores |
|---|---|---|---|---|---|---|
| Quality assessment by observer 1 | ||||||
| Pham et al., 2016 [17] | 7 | 3 | 5 | 3 | 5 | 23 |
| Besli et al., 2019 [18] | 9 | 3 | 4 | 3 | 5 | 24 |
| Lindestam et al., 2019 [11] | 10 | 3 | 5 | 3 | 5 | 26 |
| Yang et al., 2019 [19] | 10 | 3 | 4 | 3 | 5 | 25 |
| Pogorelić et al., 2021 [10] | 11 | 3 | 5 | 4 | 5 | 28 |
| Duman et al., 2022 [20] | 9 | 3 | 5 | 3 | 5 | 25 |
| Walsh et al., 2022 [21] | 9 | 3 | 5 | 3 | 5 | 25 |
| Quality assessment by observer 2 | ||||||
| Pham et al., 2016 [17] | 9 | 3 | 5 | 3 | 5 | 25 |
| Besli et al., 2019 [18] | 9 | 3 | 5 | 3 | 5 | 25 |
| Lindestam et al., 2019 [11] | 11 | 3 | 4 | 4 | 5 | 27 |
| Yang et al., 2019 [19] | 11 | 3 | 4 | 4 | 5 | 27 |
| Pogorelić et al., 2021 [10] | 11 | 3 | 4 | 4 | 5 | 27 |
| Duman et al., 2022 [20] | 9 | 3 | 5 | 3 | 5 | 25 |
| Walsh et al., 2022 [21] | 9 | 3 | 4 | 3 | 5 | 24 |
| Total scores and inter-observer agreement | ||||||
| Study | Rater 1 | Rater 2 | Mean | Kappa value | p | |
| Pham et al., 2016 [17] | 23 | 25 | 24 | 0.91 | <0.0001 | |
| Besli et al., 2019 [18] | 24 | 25 | 24.5 | |||
| Lindestam et al., 2019 [11] | 26 | 27 | 26.5 | |||
| Yang et al., 2019 [19] | 25 | 27 | 26 | |||
| Pogorelić et al., 2021 [10] | 28 | 27 | 27.5 | |||
| Duman et al., 2022 [20] | 25 | 25 | 25 | |||
| Walsh et al., 2022 [21] | 25 | 24 | 24.5 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anand, S.; Krishnan, N.; Birley, J.R.; Tintor, G.; Bajpai, M.; Pogorelić, Z. Hyponatremia—A New Diagnostic Marker for Complicated Acute Appendicitis in Children: A Systematic Review and Meta-Analysis. Children 2022, 9, 1070. https://doi.org/10.3390/children9071070
Anand S, Krishnan N, Birley JR, Tintor G, Bajpai M, Pogorelić Z. Hyponatremia—A New Diagnostic Marker for Complicated Acute Appendicitis in Children: A Systematic Review and Meta-Analysis. Children. 2022; 9(7):1070. https://doi.org/10.3390/children9071070
Chicago/Turabian StyleAnand, Sachit, Nellai Krishnan, Jana Ròs Birley, Goran Tintor, Minu Bajpai, and Zenon Pogorelić. 2022. "Hyponatremia—A New Diagnostic Marker for Complicated Acute Appendicitis in Children: A Systematic Review and Meta-Analysis" Children 9, no. 7: 1070. https://doi.org/10.3390/children9071070