
Long-Term Efficacy of the Combination of Active Vision Therapy and Occlusion in Children with Strabismic and Anisometropic Amblyopia


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Examination Protocol
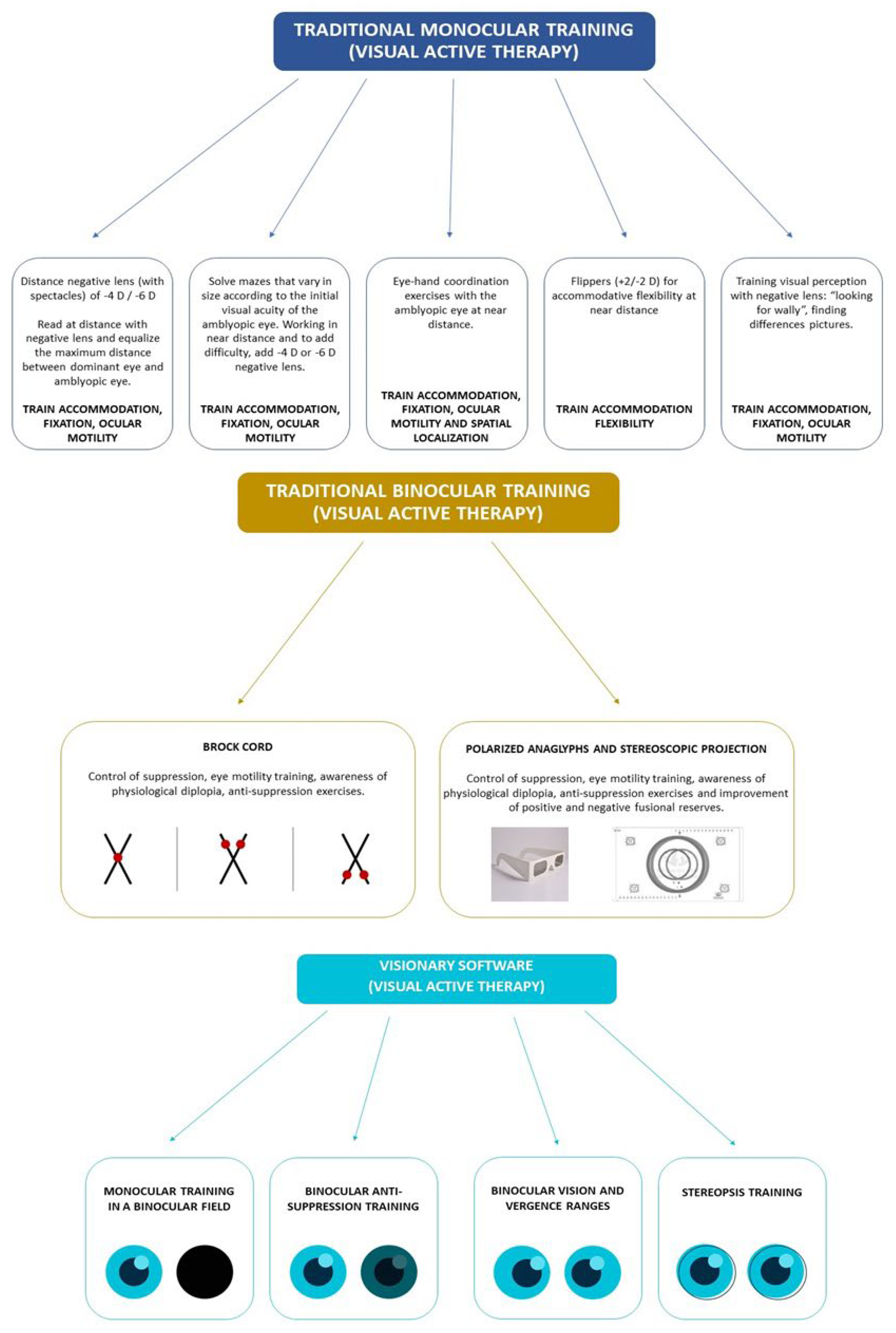
2.3. Active Vision Therapy
2.4. Statistical Analysis
3. Results
3.1. Sample Size Calculations
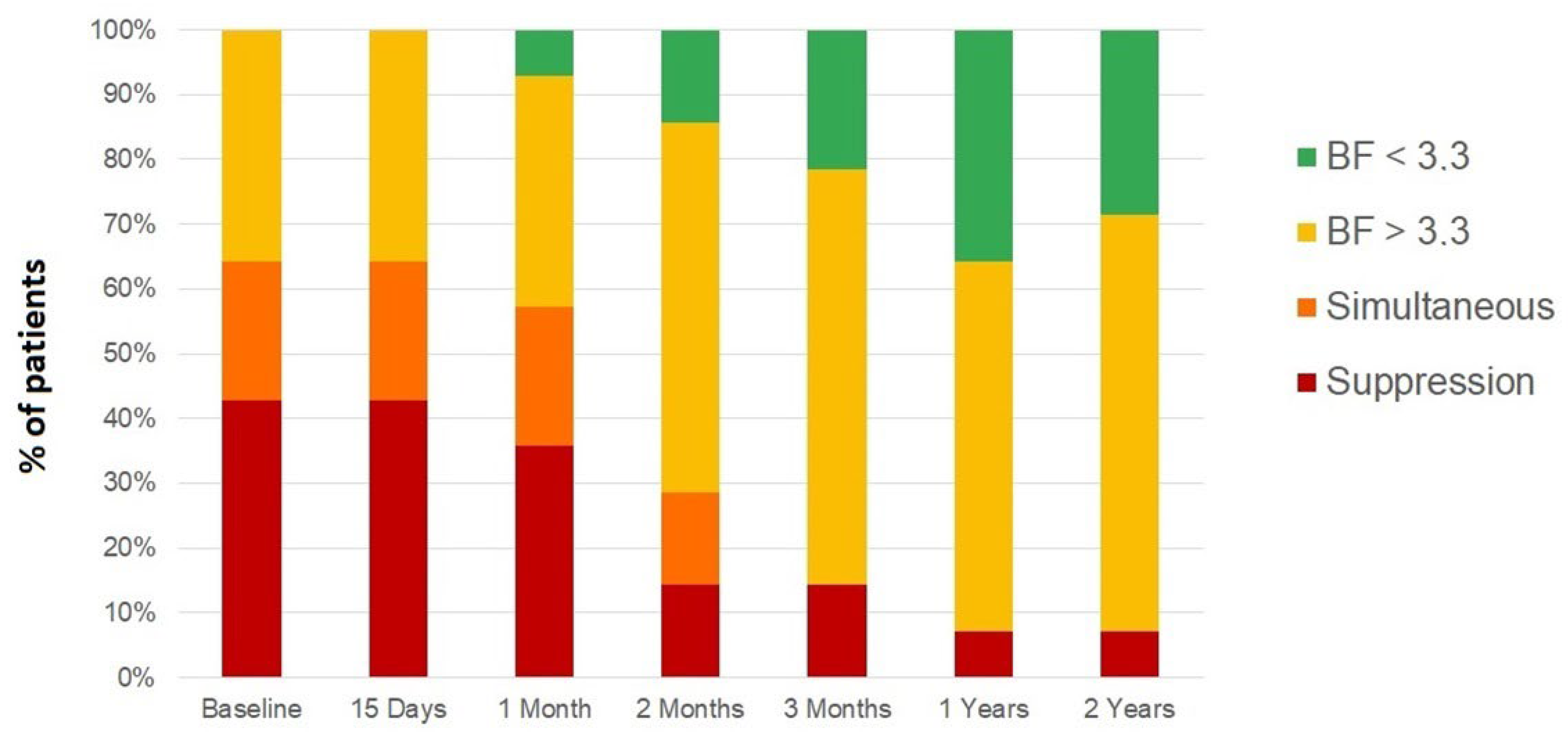
3.2. Strabismic Amblyopia
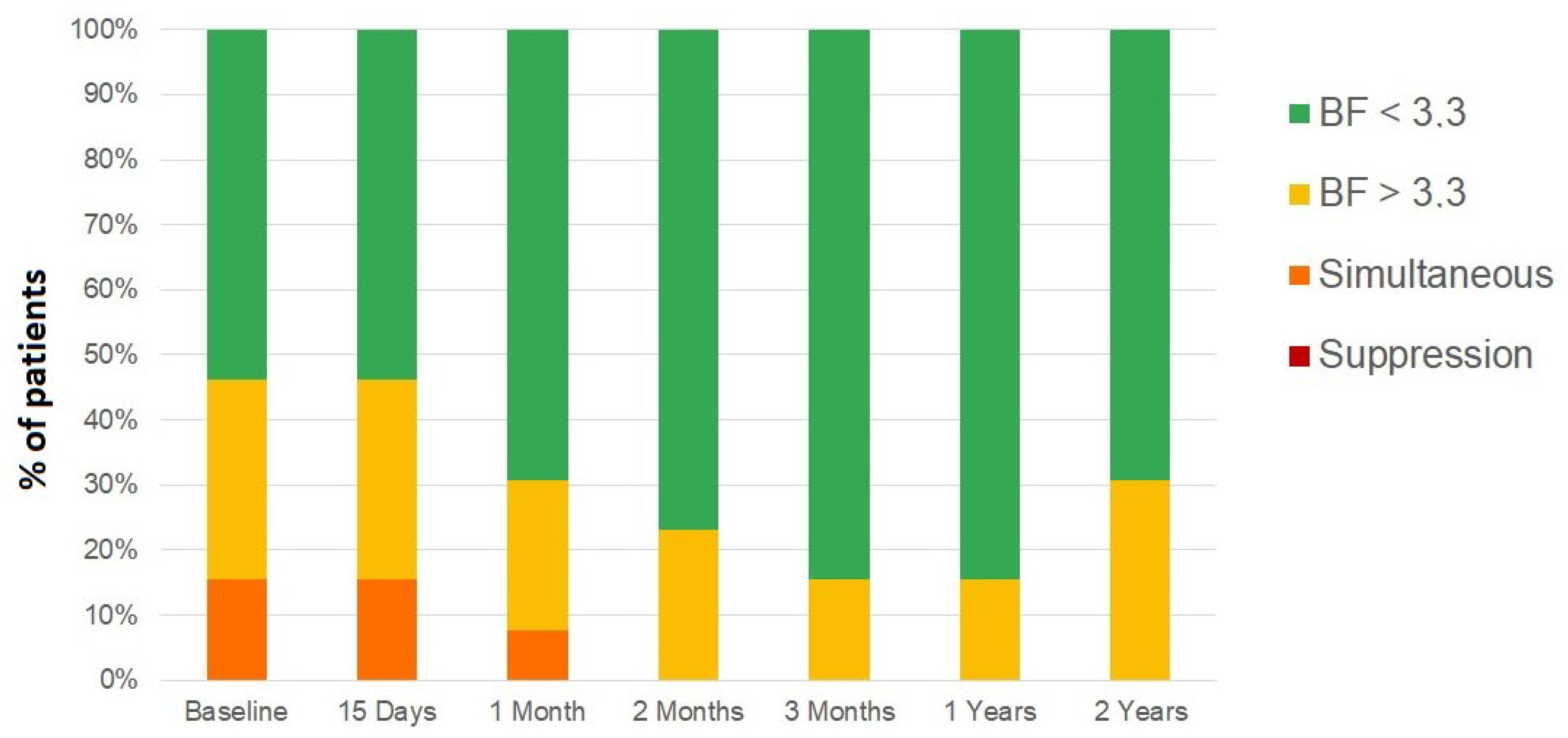
3.3. Anisometropic Amblyopia
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Scheiman, M.M.; Hertle, R.W.; Kraker, R.T.; Beck, R.W.; Birch, E.E.; Felius, J.; Holmes, J.M.; Kundart, J.; Morrison, D.G.; Repka, M.X.; et al. Patching vs. atropine to treat amblyopia in children aged 7 to 12 years: A randomized trial. Arch. Ophthalmol. 2008, 126, 1634–1642. [Google Scholar] [PubMed] [Green Version]
- Hu, B.; Liu, Z.; Zhao, J.; Zeng, L.; Hao, G.; Shui, D.; Mao, K. The global prevalence of amblyopia in children: A systematic review and meta-analysis. Front. Pediatr. 2022, 10, 819998. [Google Scholar] [CrossRef] [PubMed]
- Barrett, B.T.; Bradley, A.; McGraw, P.V. Understanding the neural basis of amblyopia. Neuroscientist 2004, 10, 106–117. [Google Scholar] [CrossRef] [PubMed]
- Milla, M.; Piñero, D.P. Characterization. passive and active treatment in strabismic amblyopia: A narrative review. Int. J. Ophthalmol. 2020, 13, 1132–1147. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Rodríguez, C.J.; Piñero, D.P. Active Vision Therapy for Anisometropic Amblyopia in Children: A Systematic Review. J. Ophthalmol. 2020, 2020, 4282316. [Google Scholar] [CrossRef] [Green Version]
- Ulrich, K.; Palmowski-Wolfe, A. Comparing three different contrast sensitivity tests in adults and in children with and without amblyopia. Klin. Mon. Augenheilkd. 2019, 236, 434–437. [Google Scholar] [CrossRef]
- Mohammadi, A.; Hashemi, H.; Mirzajani, A.; Yekta, A.; Jafarzadehpur, E.; Valadkhan, M.; Khabazkhoob, M. Contrast and spatial frequency modulation for diagnosis of amblyopia: An electrophysiological approach. J. Curr. Ophthalmol. 2019, 31, 72–79. [Google Scholar] [CrossRef]
- Niechwiej-Szwedo, E.; Colpa, L.; Wong, A.M.F. Visuomotor behaviour in amblyopia: Deficits and compensatory adaptations. Neural. Plast. 2019, 2019, 6817839. [Google Scholar] [CrossRef] [Green Version]
- Suttle, C.M. Active treatments for amblyopia: A review of the methods and evidence base. Clin. Exp. Optom. 2010, 93, 287–299. [Google Scholar] [CrossRef]
- Miller, J.R.; Cibis, L. Clinical results with active amblyopia treatments. Am. Orthopt. J. 1960, 10, 28–32. [Google Scholar] [CrossRef]
- Dosher, B.; Lu, Z.L. Visual perceptual learning and models. Ann. Rev. Vis. Sci. 2017, 15, 343–363. [Google Scholar] [CrossRef]
- Levi, D.M.; Li, R.W. Perceptual learning as a potential treatment for amblyopia: A mini-review. Vis. Res. 2009, 49, 2535–2549. [Google Scholar] [CrossRef] [Green Version]
- Kraus, C.L.; Culican, S.M. New advances in amblyopia therapy I: Binocular therapies and pharmacologic augmentation. Br. J. Ophthalmol. 2018, 102, 1492–1496. [Google Scholar] [CrossRef] [Green Version]
- Žiak, P.; Holm, A.; Halička, J.; Mojžiš, P.; Piñero, D.P. Amblyopia treatment of adults with dichoptic training using the virtual reality oculus rift head mounted display: Preliminary results. BMC Ophthalmol. 2017, 17, 105. [Google Scholar] [CrossRef] [Green Version]
- West, S.; Williams, C. Amblyopia. BMJ Clin. Evid. 2011, 2011, 0709. [Google Scholar]
- Pediatric Eye Disease Investigator Group; Wallace, D.K.; Lazar, E.L.; Holmes, J.M.; Repka, M.X.; Cotter, S.A.; Chen, A.M.; Kraker, R.T.; Beck, R.W.; Clarke, M.P.; et al. A randomized trial of increasing patching for amblyopia. Ophthalmology 2013, 120, 2270–2277. [Google Scholar] [CrossRef] [Green Version]
- Webber, A.L.; Wood, J.M.; Thompson, B.; Birch, E.E. From suppression to stereoacuity: A composite binocular function score for clinical research. Ophthalmic Physiol. Opt. 2019, 39, 53–62. [Google Scholar] [CrossRef] [Green Version]
- Molina-Martín, A.; Martín-González, S.; Illarramendi-Mendicute, I.; Portela-Camino, J.A. Combined passive and active treatment in strabismic amblyopia with accommodative component. Clin. Exp. Optom. 2020, 103, 885–894. [Google Scholar] [CrossRef]
- Flom, M.C. The prognosis in strabismus. Am. J. Optom. Arch. Acad. Optom. 1958, 35, 509–514. [Google Scholar] [CrossRef]
- Portela-Camino, J.A.; Martín-González, S.; Ruiz-Alcocer, J.; Illarramendi-Mendicute, I.; Garrido-Mercado, R. A random dot computer video game improves stereopsis. Optom. Vis. Sci. 2018, 95, 523–535. [Google Scholar] [CrossRef]
- Walsh, L.A.; Hahn, E.K.; LaRoche, G.R. The method of treatment cessation and recurrence rate of amblyopia. Strabismus 2009, 17, 107–116. [Google Scholar] [CrossRef]
- Dupont, W.D.; Plummer, W.D. Power and sample size calculations: A review and computer program. Control. Clin. Trials 1990, 11, 116–128. [Google Scholar] [CrossRef]
- Chinn, R.N.; Michalak, S.M.; Shoshany, T.N.; Bishop, K.; Staffa, S.J.; Hunter, D.G. Effect of sequential and simultaneous patching regimens in unilateral amblyopia. Am. J. Ophthalmol. 2022, 233, 48–56. [Google Scholar] [CrossRef]
- Scaramuzzi, M.; Murray, J.; Nucci, P.; Shaikh, A.G.; Ghasia, F.F. Fixational eye movements abnormalities and rate of visual acuity and stereoacuity improvement with part time patching. Sci. Rep. 2021, 11, 1217. [Google Scholar] [CrossRef]
- Rajavi, Z.; Sabbaghi, H.; Amini Sharifi, E.; Behradfar, N.; Kheiri, B. Comparison between patching and interactive binocular treatment in amblyopia: A randomized clinical trial. J. Curr. Ophthalmol. 2019, 31, 426–431. [Google Scholar] [CrossRef]
- Pineles, S.L.; Aakalu, V.K.; Hutchinson, A.K.; Galvin, J.A.; Heidary, G.; Binenbaum, G.; VanderVeen, D.K.; Lambert, S.R. Binocular treatment of amblyopia: A report by the American Academy of Ophthalmology. Ophthalmology. 2020, 127, 261–272. [Google Scholar] [CrossRef] [Green Version]
- Hernández-Rodríguez, C.J.; Fukumitsu, H.; Ruiz-Fortes, P.; Soto-Negro, R.; Merino-Suárez, M.; Piñero, D.P. Efficacy of perceptual learning-based vision training as an adjuvant to occlusion therapy in the management of amblyopia: A pilot study. Vision 2021, 5, 15. [Google Scholar] [CrossRef]
- Xiao, S.; Angjeli, E.; Wu, H.C.; Gaier, E.D.; Gomez, S.; Travers, D.A.; Binenbaum, G.; Langer, R.; Hunter, D.G.; Repka, M.X. Luminopia Pivotal Trial Group. Randomized controlled trial of a dichoptic digital therapeutic for amblyopia. Ophthalmology 2022, 129, 77–85. [Google Scholar] [CrossRef]
- Huang, Y.T.; Lin, H.J.; Liao, W.L.; Tsai, Y.Y.; Hsieh, Y.C. Effects of vision therapy on bilateral amblyopia unresponsive to conventional treatment: A retrospective comparative study. Children 2022, 9, 205. [Google Scholar] [CrossRef]
- Manny, R.E.; Holmes, J.M.; Kraker, R.T.; Li, Z.; Waters, A.L.; Kelly, K.R.; Kong, L.; Crouch, E.R.; Lorenzana, I.J.; Alkharashi, M.S.; et al. Pediatric Eye Disease Investigator Group. A randomized trial of binocular Dig Rush game treatment for amblyopia in children aged 4 to 6 years. Optom. Vis. Sci. 2022, 99, 213–227. [Google Scholar]
- Jost, R.M.; Hudgins, L.A.; Dao, L.M.; Stager, D.R., Jr.; Luu, B.; Beauchamp, C.L.; Hunter, J.S.; Giridhar, P.; Wang, Y.Z.; Birch, E.E. Randomized clinical trial of streaming dichoptic movies versus patching for treatment of amblyopia in children aged 3 to 7 years. Sci. Rep. 2022, 12, 4157. [Google Scholar] [CrossRef] [PubMed]
- Xiao, S.; Gaier, E.D.; Wu, H.C.; Angjeli, E.; Nuth, P.L.; Bohra, L.I.; Miller, A.M.; Mazow, M.L.; Stout, A.U.; Morse, C.L.; et al. Digital therapeutic improves visual acuity and encourages high adherence in amblyopic children in open-label pilot study. J. AAPOS 2021, 25, 87.e1–87.e6. [Google Scholar] [CrossRef] [PubMed]
- Pang, P.C.K.; Lam, C.S.Y.; Hess, R.F.; Thompson, B. Effect of dichoptic video game treatment on mild amblyopia—A pilot study. Acta Ophthalmol. 2021, 99, e423–e432. [Google Scholar] [CrossRef] [PubMed]
- Raveendran, R.N.; Krishnan, A.K.; Thompson, B. Reduced fixation stability induced by peripheral viewing does not contribute to crowding. J. Vis. 2020, 20, 3. [Google Scholar] [CrossRef]
- Birch, E.E.; Jost, R.M.; De La Cruz, A.; Kelly, K.R.; Beauchamp, C.L.; Dao, L.; Stager, D., Jr.; Leffler, J.N. Binocular amblyopia treatment with contrast-rebalanced movies. J. AAPOS 2019, 23, 160.e1–160.e5. [Google Scholar] [CrossRef]
- Jia, W.; Lan, F.; Zhao, X.; Lu, Z.L.; Huang, C.B.; Zhao, W.; Li, M. The effects of monocular training on binocular functions in anisometropic amblyopia. Vis. Res. 2018, 152, 74–83. [Google Scholar] [CrossRef]
- Mezad-Koursh, D.; Rosenblatt, A.; Newman, H.; Stolovitch, C. Home use of binocular dichoptic video content device for treatment of amblyopia: A pilot study. J. AAPOS 2018, 22, 134–138.e4. [Google Scholar] [CrossRef]
- Bossi, M.; Tailor, V.K.; Anderson, E.J.; Bex, P.J.; Greenwood, J.A.; Dahlmann-Noor, A.; Dakin, S.C. Binocular therapy for childhood amblyopia improves vision without breaking interocular suppression. Investig. Ophthalmol. Vis. Sci. 2017, 58, 3031–3043. [Google Scholar] [CrossRef] [Green Version]
- Li, S.L.; Reynaud, A.; Hess, R.F.; Wang, Y.Z.; Jost, R.M.; Morale, S.E.; De La Cruz, A.; Dao, L.; Stager, D., Jr.; Birch, E.E. Dichoptic movie viewing treats childhood amblyopia. J. AAPOS 2015, 19, 401–405. [Google Scholar] [CrossRef] [Green Version]
- Birch, E.E.; Li, S.L.; Jost, R.M.; Morale, S.E.; De La Cruz, A.; Stager, D., Jr.; Dao, L.; Stager, D.R., Sr. Binocular iPad treatment for amblyopia in preschool children. J. AAPOS 2015, 19, 6–11. [Google Scholar] [CrossRef] [Green Version]
- Agervi, P.; Kugelberg, U.; Kugelberg, M.; Zetterström, C. Two-year follow-up of a randomized trial of spectacles plus alternate-day patching to treat strabismic amblyopia. Acta Ophthalmol. 2013, 91, 678–684. [Google Scholar] [CrossRef]
- Wong-Kee-You, A.M.B.; Wei, H.; Hou, C. Feature counting under dichoptic viewing in anisometropic and strabismic amblyopia. Transl. Vis. Sci. Technol. 2020, 9, 13. [Google Scholar] [CrossRef]
- Liang, M.; Xie, B.; Yang, H.; Yin, X.; Wang, H.; Yu, L.; He, S.; Wang, J. Altered interhemispheric functional connectivity in patients with anisometropic and strabismic amblyopia: A resting-state fMRI study. Neuroradiology. 2017, 59, 517–524. [Google Scholar] [CrossRef]
- Agrawal, R.; Conner, I.P.; Odom, J.V.; Schwartz, T.L.; Mendola, J.D. Relating binocular and monocular vision in strabismic and anisometropic amblyopia. Arch. Ophthalmol. 2006, 124, 844–850. [Google Scholar] [CrossRef] [Green Version]
- Herbison, N.; MacKeith, D.; Vivian, A.; Purdy, J.; Fakis, A.; Ash, I.M.; Cobb, S.V.; Eastgate, R.M.; Haworth, S.M.; Gregson, R.M.; et al. Randomised controlled trial of video clips and interactive games to improve vision in children with amblyopia using the I-BiT system. Br. J. Ophthalmol. 2016, 100, 1511–1516. [Google Scholar] [CrossRef]
- Boniquet-Sanchez, S.; Sabater-Cruz, N. Current management of amblyopia with new technologies for binocular treatment. Vision 2021, 5, 31. [Google Scholar] [CrossRef]
- Holmes, J.M.; Beck, R.W.; Kraker, R.T.; Astle, W.F.; Birch, E.E.; Cole, S.R.; Cotter, S.A.; Donahue, S.; Everett, D.F.; Hertle, R.W.; et al. Pediatric Eye Disease Investigator Group. Risk of amblyopia recurrence after cessation of treatment. J. AAPOS 2004, 8, 420–428. [Google Scholar]
- Tang, E.W.; Li, B.C.; Yeung, I.Y.; Li, K.K. Occlusion therapy in amblyopia: An experience from Hong Kong. Hong Kong Med. J. 2014, 20, 32–36. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| α | δ | σ | n | SP | |
|---|---|---|---|---|---|
| Strabismic amblyopia | |||||
| Distance BCVA | 0.05 | −0.21 | 0.16 | 14 | 99.2% |
| BF | 0.05 | −1.27 | 1.20 | 14 | 95.2% |
| Anisometropic amblyopia | |||||
| Distance BCVA | 0.05 | −0.26 | 0.16 | 13 | 99.8% |
| BF | 0.05 | −0.67 | 0.56 | 13 | 97.3% |
| Median [IQ] | Previous | 15 Days | 1 Month | 2 Months | 3 Months | 1 Year Post Avt | 2 Years Post Avt | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | ||||||||||||||||
| (Range) | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | p (0) | p (1) |
| Distance BCVA | 0.00 [0.03] | 0.19 [0.30] | 0.00 [0.02] | 0.11 [0.19] | 0.00 [0.01] | 0.07 [0.09] | 0.00 [0.02] | 0.03 [0.06] | 0.00 [0.01] | 0.02 [0.08] | 0.00 [0.02] | 0.02 [0.03] | 0.00 [0.02] | 0.02 [0.05] | 0.73 | <0.001 |
| (logMAR) | 0.03 ± 0.06 | 0.25 ± 0.17 | −0.01 ± 0.09 | 0.17 ± 0.15 | −0.00 ± 0.11 | 0.08 ± 0.06 | 0.01 ± 0.01 | 0.05 ± 0.05 | 0.01 ± 0.05 | 0.05 ± 0.07 | 0.01 ± 0.02 | 0.03 ± 0.03 | 0.00 ± 0.03 | 0.04 ± 0.05 | ||
| (0.00–0.15) | (0.05–0.52) | (−0.30–0.10) | (0.00–0.52) | (−0.30–0.22) | (0.00–0.19) | (0.00–0.05) | (0.00–0.15) | (−0.08–0.15) | (0.00–0.22) | (0.00–0.07) | (0.00–0.10) | (−0.08–0.05) | (0.00–0.19) | |||
| Near BCVA | 0.00 [0.10] | 0.20 [0.23] | 0.00 [0.10] | 0.15 [0.20] | 0.00 [0.02] | 0.10 [0.20] | 0.00 [0.10] | 0.10 [0.12] | 0.00 [0.10] | 0.00 [0.12] | 0.00 [0.02] | 0.00 [0.10] | 0.00 [0.00] | 0.00 [0.10] | 0.11 | <0.001 |
| (logMAR) | 0.03 ± 0.11 | 0.26 ± 0.20 | 0.03 ± 0.09 | 0.16 ± 0.13 | 0.01 ± 0.08 | 0.10 ± 0.10 | 0.01 ± 0.06 | 0.08 ± 0.10 | −0.01 ± 0.06 | 0.03 ± 0.10 | −0.01 ± 0.05 | 0.02 ± 0.06 | 0.01 ± 0.03 | 0.06 ± 0.08 | ||
| (0.30–0.40) | (0.00–0.70) | (−0.10–0.20) | (−0.10–0.30) | (−0.10–0.20) | (0.00–0.30) | (−0.10–0.10) | (−0.10–0.30) | (−0.10–0.10) | (−0.10–0.20) | (−0.10–0.10) | (−0.10–0.10) | (0.00–0.10) | (0.00–0.30) | |||
| Cycloplegic refraction (D) | 3.00 [2.25] | 4.94 [2.88] | 3.00 [2.25] | 4.94 [2.88] | 3.00 [2.25] | 4.94 [2.88] | 3.00 [2.25] | 4.94 [2.63] | 2.94 [2.67] | 4.75 [3.00] | 2.94 [3.19] | 5.13 [3.28] | 2.88 [4.00] | 5.00 [2.88] | 0.74 | 0.93 |
| 3.23 ± 1.83 | 4.12 ± 2.63 | 3.23 ± 1.83 | 4.12 ± 2.63 | 3.25 ± 1.86 | 4.08 ± 2.71 | 3.21 ± 1.87 | 4.10 ± 2.68 | 3.26 ± 1.90 | 4.11 ± 2.70 | 3.18 ± 1.94 | 4.13 ± 2.73 | 3.23 ± 2.18 | 4.11 ± 3.05 | |||
| (0.50–6.63) | (−2.38–7.38) | (0.50–6.63) | (−2.38–7.38) | (0.25–6.63) | (−2.38–7.38) | (0.25–6.63) | (−2.25–7.38) | (0.50–6.63) | (−2.25–7.38) | (0.50–6.88) | (−2.25–7.63) | (0.38–6.75) | (−3.38–7.50) | |||
| Subjective refraction | 2.37 [3.06] | 4.31 [3.38] | 2.86 [3.06] | 4.31 [3.72] | 2.75 [3.06] | 4.25 [3.06] | 2.75 [2.78] | 4.31 [3.16] | 2.50 [3.44] | 4.38 [3.41] | 2.63 [3.44] | 4.63 [3.38] | 2.50 [3.75] | 4.50 [3.19] | 0.02 | 0.93 |
| (D) | 2.64 ± 2.13 | 3.55 ± 2.96 | 2.71 ± 2.13 | 3.60 ± 3.00 | 2.80 ± 2.04 | 3.55 ± 2.81 | 2.72 ± 1.97 | 3.61 ± 2.66 | 3.02 ± 2.00 | 3.72 ± 2.68 | 3.04 ± 2.04 | 3.82 ± 2.69 | 3.13 ± 2.38 | 3.74 ± 3.06 | ||
| (−0.38–6.63) | (−3.00–7.50) | (−0.38–6.63) | (−3.00–7.50) | (0.00–6.63) | (−3.00–7.50) | (−0.13–6.63) | (−2.63–7.00) | (0.00–6.63) | (−2.38–7.00) | (0.00–6.50) | (−2.38–7.25) | (−0.50–6.75) | (−3.25–7.25) | |||
| Distance Cover Test | 3.00 [10] | 3.00 [10] | 2.25 [10] | 3.75 [11] | 2.25 [8] | 0.00 [6] | 0.00 [7] | <0.001 | ||||||||
| (prism diopters) | 5.14 ± 10.21 | 5.14 ± 10.21 | 3.89 ± 8.40 | 4.00 ± 10.13 | 2.18 ± 7.49 | 1.29 ± 7.09 | 2.64 ± 4.92 | |||||||||
| (−17–25) | (−17–25) | (−17–16) | (−25–16) | (−20–10) | (−20–10) | (−8–10) | ||||||||||
| Near Cover Test | 7.75 [10] | 7.75 [11] | 7.50 [11] | 6.50 [8] | 4.75 [9] | 4.25 [9] | 6.75 [10] | 0.45 | ||||||||
| (prism diopters) | 7.50 ± 11.47 | 8.50 ± 11.67 | 6.32 ± 10.27 | 5.75 ± 9.94 | 3.99 ± 7.88 | 4.07 ± 8.46 | 6.89 ± 6.82 | |||||||||
| (−25–25) | (−25–25) | (−25–16) | (−25–16) | (−19–15) | (−19–19) | (−8–18) | ||||||||||
| BF | 4.00 [2.47] | 4.00 [2.73] | 4.00 [2.50] | 2.60 [1.70] | 2.60 [0.68] | 2.30 [0.75] | 2.30 [0.33] | 0.002 | ||||||||
| 3.79 ± 1.30 | 3.76 ± 1.33 | 3.62 ± 1.29 | 2.96 ± 1.09 | 2.29 ± 1.08 | 2.54 ± 0.75 | 2.52 ± 0.77 | ||||||||||
| (1.60–5.00) | (1.60–5.00) | (1.60–5.00) | (1.60–5.00) | (1.51–5.00) | (1.80–5.00) | (1.70–5.00) | ||||||||||
| Median [IQ] | Previous | 15 Days | 1 Month | 2 Months | 3 Months | 1 Year Post Avt | 2 Years Post Avt | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | ||||||||||||||||
| (Range) | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | p (0) | p (1) |
| Distance BCVA | 0.00 [0.02] | 0.22 [0.32] | 0.00 [0.00] | 0.07 [0.13] | 0.00 [0.00] | 0.02 [0.05] | 0.00 [0.00] | 0.02 [0.01] | 0.00 [0.00] | 0.01 [0.02] | 0.00 [0.00] | 0.01 [0.02] | 0.00 [0.04] | 0.00 [0.01] | 0.2 | <0.001 |
| (logMAR) | 0.01 ± 0.06 | 0.26 ± 0.17 | 0.01 ± 0.03 | 0.12 ± 0.10 | −0.00 ± 0.02 | 0.04 ± 0.03 | −0.01 ± 0.02 | 0.05 ± 0.08 | −0.01 ± 0.02 | 0.03 ± 0.06 | 0.00 ± 0.01 | 0.02 ± 0.02 | −0.02 ± 0.04 | −0.00 ± 0.02 | ||
| (−0.08–0.15) | (0.10–0.60) | (0.00–0.10) | (0.00–0.35) | (−0.08–0.02) | (0.02–0.10) | (−0.08–0.00) | (0.00–0.30) | (−0.08–0.00) | (0.00–0.22) | (0.00–0.02) | (0.00–0.07) | (−0.08–0.02) | (−0.08–0.02) | |||
| Near BCVA | 0.00 [0.10] | 0.20 [0.20] | 0.00 [0.05] | 0.10 [0.25] | 0.00 [0.00] | 0.00 [0.10] | 0.00 [0.05] | 0.00 [0.15] | −0.10 [0.10] | 0.00 [0.10] | 0.00 [0.10] | 0.00 [0.10] | −0.10 [0.10] | 0.00 [0.10] | 0.01 | <0.001 |
| (logMAR) | −0.01 ± 0.08 | 0.16 ± 0.18 | −0.01 ± 0.05 | 0.06 ± 0.12 | 0.00 ± 0.00 | 0.04 ± 0.06 | −0.02 ± 0.04 | 0.01 ± 0.09 | −0.05 ± 0.05 | −0.04 ± 0.06 | −0.04 ± 0.05 | −0.03 ± 0.05 | −0.05 ± 0.05 | −0.05 ± 0.05 | ||
| (−0.10–0.20) | (−0.10–0.60) | (−0.10–0.10) | (−0.10–0.20) | (0.00–0.00) | (0.00–0.20) | (−0.10–0.00) | (−0.10–0.20) | (−0.10–0.00) | (−0.10–0.10) | (−0.10–0.00) | (−0.10–0.00) | (−0.10–0.00) | (−0.10–0.00) | |||
| Cyploplegic refraction | 1.88 [1.56] | 4.38 [7.00] | 2.00 [1.56] | 4.38 [6.81] | 1.88 [1.56] | 4.38 [6.81] | 1.88 [1.94] | 4.38 [7.00] | 2.00 [2.13] | 3.25 [6.75] | 2.00 [2.31] | 3.63 [7.75] | 2.00 [2.75] | 3.38 [8.88] | 0.59 | 0.31 |
| (D) | 2.21 ± 1.60 | 2.71 ± 4.10 | 2.22 ± 1.60 | 2.74 ± 4.06 | 2.19 ± 1.56 | 2.70 ± 4.00 | 2.31 ± 1.71 | 2.75 ± 4.02 | 2.27 ± 1.73 | 2.50 ± 3.92 | 2.11 ± 1.70 | 2.32 ± 4.53 | 1.89 ± 1.88 | 2.13 ± 4.58 | ||
| (−0.50–6.25) | (−4.25–8.00) | (−0.50–6.25) | (−4.25–8.00) | (0.00–6.25 | (−4.25–7.88) | (0.00–6.25) | (−4.25–7.88) | (0.00–6.25) | (−4.25–7.88) | (−0.50–5.50) | (−5.75–7.63) | (5.50–6.50) | (−6.00–7.13) | |||
| Subjective refraction | 1.25 [1.13] | 3.50 [6.25] | 1.00 [1.00] | 2.50 [6.38] | 1.13 [1.00] | 4.00 [6.38] | 1.13 [1.25] | 3.00 [6.25] | 1.25 [1.50] | 3.75 [6.19] | 1.50 [2.00] | 2.63 [6.81] | 1.38 [2.00] | 2.38 [7.31] | 0.9 | <0.001 |
| (D) | 1.44 ± 1.48 | 2.29 ± 3.86 | 1.45 ± 1.47 | 2.13 ± 3.89 | 1.45 ± 1.44 | 2.22 ± 3.94 | 1.55 ± 1.49 | 2.06 ± 3.94 | 1.54 ± 1.51 | 2.11 ± 3.99 | 1.62 ± 1.49 | 1.90 ± 4.11 | 1.51 ± 1.61 | 1.49 ± 4.17 | ||
| (−0.25–5.50) | (−4.38–7.50) | (−0.25–5.50) | (−4.50–7.50) | (−0.25–5.50) | (−4.50–7.38) | (−0.25–5.50) | (−5.00–7.38) | (−0.25–5.50) | (−5.13–7.38) | (−0.25–5.25) | (−5.38–7.25) | (−1.00–5.00) | (−5.50–7.00) | |||
| Distance Cover Test | 0.00 [0] | 0.00 [0] | 0.00 [0] | 0.00 [0] | 0.00 [0] | 0.00 [0] | 0.00 [0] | 0.04 | ||||||||
| (prism diopters) | −0.69 ± 1.80 | −0.62 ± 1.56 | −0.86 ± 0.83 | 0.23 ± 0.83 | −0.38 ± 1.39 | −0.38 ± 1.39 | 0.00 ± 0.00 | |||||||||
| (−6–0) | (−5–0) | (0–3) | (0–3) | (−5–0) | (−5–0) | (0–0) | ||||||||||
| Near Cover Test | 0.00 [2.8] | 0.00 [3.3] | 0.00 [0] | 0.00 [0] | 0.00 [5] | −4.00 [4] | 0.00 [2] | 0.04 | ||||||||
| (prism diopters) | 0.15 ± 3.78 | 0.23 ± 3.85 | −0.62 ± 3.50 | −0.62 ± 3.50 | −1.69 ± 3.64 | −2.62 ± 2.76 | −1.23 ± 2.52 | |||||||||
| (−10–4.5) | (−10–4.5) | (−10–6) | (−10–6) | (−8–4) | (−8–0) | (−8–0) | ||||||||||
| BF | 2.30 [0.50] | 2.10 [0.66] | 2.00 [0.69] | 2.00 [0.44] | 2.08 [0.59] | 1.80 [0.14] | 1.80 [0.00] | <0.001 | ||||||||
| 2.52 ± 0.69 | 2.43 ± 0.75 | 2.19 ± 0.64 | 2.01 ± 0.34 | 2.06 ± 0.33 | 1.89 ± 0.33 | 1.85 ± 0.26 | ||||||||||
| (1.80–4.00) | (1.70–4.00) | (1.60–4.00) | (1.40–2.70) | (1.60–2.70) | (1.51–2.70) | (1.70–2.70) | ||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milla, M.; Molina-Martín, A.; Piñero, D.P. Long-Term Efficacy of the Combination of Active Vision Therapy and Occlusion in Children with Strabismic and Anisometropic Amblyopia. Children 2022, 9, 1012. https://doi.org/10.3390/children9071012
Milla M, Molina-Martín A, Piñero DP. Long-Term Efficacy of the Combination of Active Vision Therapy and Occlusion in Children with Strabismic and Anisometropic Amblyopia. Children. 2022; 9(7):1012. https://doi.org/10.3390/children9071012
Chicago/Turabian StyleMilla, Myriam, Ainhoa Molina-Martín, and David P. Piñero. 2022. "Long-Term Efficacy of the Combination of Active Vision Therapy and Occlusion in Children with Strabismic and Anisometropic Amblyopia" Children 9, no. 7: 1012. https://doi.org/10.3390/children9071012