
The Impact of the COVID-19 Pandemic on Youth with Chronic Pain and Their Parents: A Longitudinal Examination of Who Are Most at Risk


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Procedure
2.3. Measures
2.3.1. Pain Interference
2.3.2. Depressive and Anxiety Symptoms
2.3.3. Personality Traits
2.4. Data Analyses
3. Results
3.1. Participants
3.2. Descriptive Statistics
3.2.1. Changes in Pain and Mental Health from pre- to during the COVID-19 Pandemic
3.2.2. Pain Interference
3.2.3. Depression
3.2.4. Anxiety
3.2.5. Depression
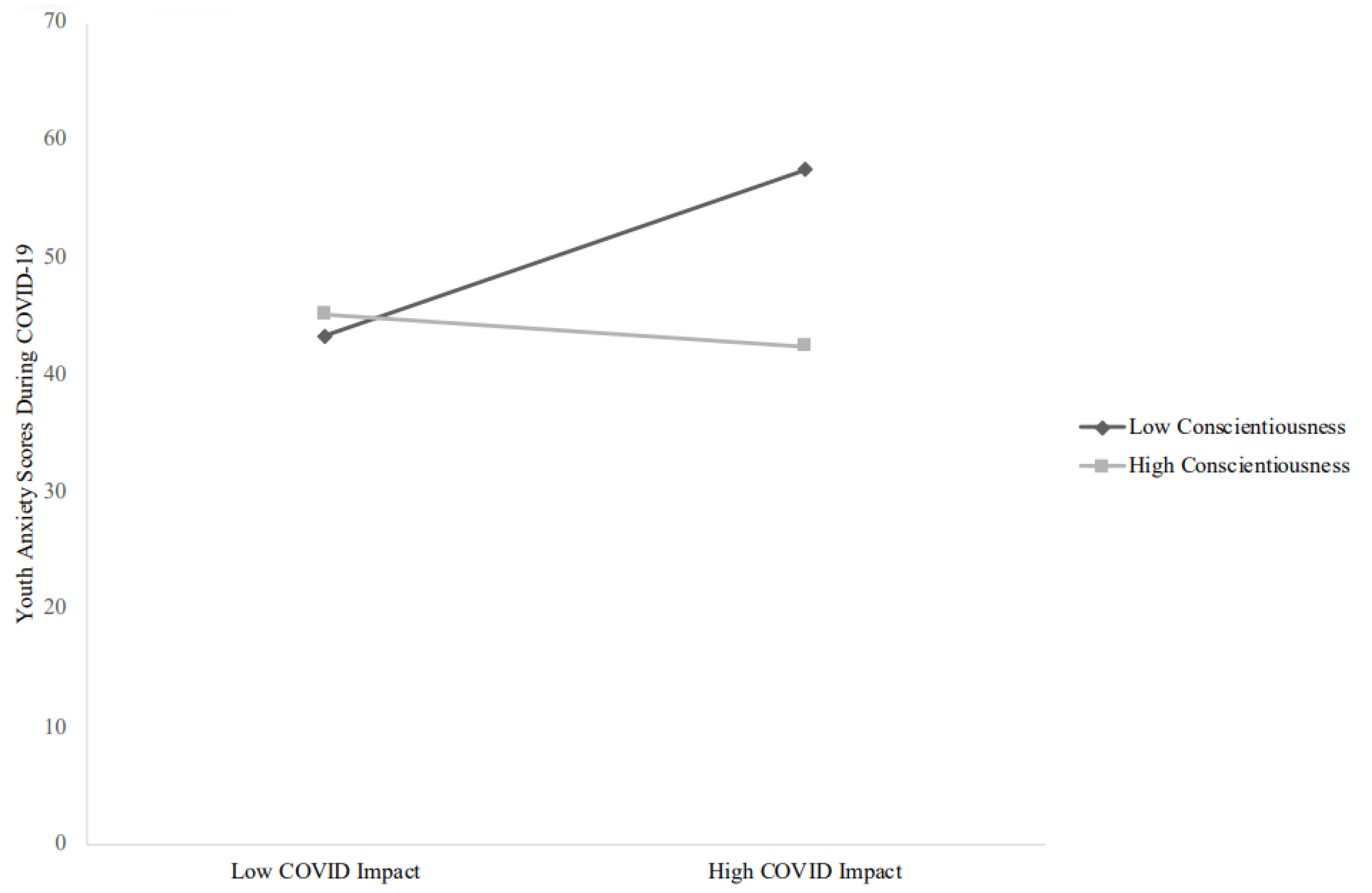
3.2.6. Anxiety
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Birnie, K.A.; Heathcote, L.C.; Bhandari, R.P.; Feinstein, A.; Yoon, I.A.; Simons, L.E. Parent physical and mental health contributions to interpersonal fear avoidance processes in pediatric chronic pain. Pain 2020, 161, 1202–1211. [Google Scholar] [CrossRef] [PubMed]
- Cordts, K.P.; Stone, A.L.; Beveridge, J.K.; Wilson, A.C.; Noel, M. The (Parental) Whole Is Greater Than the Sum of Its Parts: A Multifactorial Model of Parent Factors in Pediatric Chronic Pain. J. Pain 2019, 20, 786–795. [Google Scholar] [CrossRef] [PubMed]
- King, S.; Chambers, C.T.; Huguet, A.; MacNevin, R.C.; McGrath, P.J.; Parker, L.; Macdonald, A.J. The epidemiology of chronic pain in children and adolescents revisited: A systematic review. Pain 2011, 152, 2729–2738. [Google Scholar] [CrossRef] [PubMed]
- Weissman, M.M. Recent advances in depression across the generations. Epidemiol. Psichiatr. Soc. 2006, 15, 16–19. [Google Scholar] [CrossRef]
- Golberstein, E.; Wen, H.; Miller, B.F. Coronavirus Disease 2019 (COVID-19) and Mental Health for Children and Adolescents. JAMA Pediatr. 2020, 174, 819. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, E.K.; McAuliffe, C.; Hirani, S.; Richardson, C.; Thomson, K.C.; McGuinness, L.; Morris, J.; Kousoulis, A.; Gadermann, A. A portrait of the early and differential mental health impacts of the COVID-19 pandemic in Canada: Findings from the first wave of a nationally representative cross-sectional survey. Prev. Med. 2021, 145, 106333. [Google Scholar] [CrossRef]
- Nochaiwong, S.; Ruengorn, C.; Thavorn, K.; Hutton, B.; Awiphan, R.; Phosuya, C.; Ruanta, Y.; Wongpakaran, N.; Wongpakaran, T. Global prevalence of mental health issues among the general population during the coronavirus disease-2019 pandemic: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 10173. [Google Scholar] [CrossRef]
- Santomauro, D.F.; Herrera, A.M.M.; Shadid, J.; Zheng, P.; Ashbaugh, C.; Pigott, D.M.; Abbafati, C.; Adolph, C.; Amlag, J.O.; Aravkin, A.Y.; et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef]
- Racine, N.; McArthur, B.A.; Cooke, J.E.; Eirich, R.; Zhu, J.; Madigan, S. Global Prevalence of Depressive and Anxiety Symptoms in Children and Adolescents during COVID-19: A Meta-analysis. JAMA Pediatr. 2021, 175, 1142. [Google Scholar] [CrossRef]
- Craig, S.G.; Ames, M.E.; Bondi, B.C.; Pepler, D.J. Canadian adolescents’ mental health and substance use during the COVID-19 pandemic: Associations with COVID-19 stressors. Can. J. Behav. Sci. Rev. Can. Sci. Comport. 2022. [Google Scholar] [CrossRef]
- Clauw, D.J.; Häuser, W.; Cohen, S.P.; Fitzcharles, M.-A. Considering the potential for an increase in chronic pain after the COVID-19 pandemic. Pain 2020, 161, 1694–1697. [Google Scholar] [CrossRef] [PubMed]
- Lacasse, A.; Pagé, M.G.; Dassieu, L.; Sourial, N.; Janelle-Montcalm, A.; Dorais, M.; Nguefack, H.L.N.; Godbout-Parent, M.; Hudspith, M.; Moor, G.; et al. Impact of the COVID-19 pandemic on the pharmacological, physical, and psychological treatments of pain: Findings from the Chronic Pain & COVID-19 Pan-Canadian Study. Pain Rep. 2021, 6, e891. [Google Scholar] [CrossRef] [PubMed]
- Margolies, S.O.; Patidar, S.M.; Chidgey, B.A.; Goetzinger, A.; Sanford, J.B.; Short, N.A. Growth in crisis: A mixed methods study of lessons from our patients with chronic pain during the COVID-19 pandemic. J. Context. Behav. Sci. 2020, 19, 12–16. [Google Scholar] [CrossRef]
- Zambelli, Z.; Fidalgo, A.R.; Halstead, E.J.; Dimitriou, D. Acute impact of a national lockdown during the COVID-19 pandemic on wellbeing outcomes among individuals with chronic pain. J. Health Psychol. 2021, 27, 1099–1110. [Google Scholar] [CrossRef] [PubMed]
- Chatkoff, D.K.; Leonard, M.T.; Najdi, R.R.; Cruga, B.; Forsythe, A.; Bourgeau, C.; Easton, H. A Brief Survey of the COVID-19 Pandemic’s Impact on the Chronic Pain Experience. Pain Manag. Nurs. 2021, 23, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Pagé, M.G.; Lacasse, A.; Dassieu, L.; Hudspith, M.; Moor, G.; Sutton, K.; Thompson, J.M.; Dorais, M.; Montcalm, A.J.; Sourial, N.; et al. A cross-sectional study of pain status and psychological distress among individuals living with chronic pain: The Chronic Pain & COVID-19 Pan-Canadian Study. Health Promot. Chronic Dis. Prev. Can. 2021, 41, 141–152. [Google Scholar] [CrossRef]
- Ali, O.M.; Debono, V.B.; Anthonypillai, J.; Hapidou, E.G. A Qualitative Study of the Impact of the COVID-19 Pandemic on a Sample of Patients with Chronic Pain. J. Patient Exp. 2022, 9, 237437352210896. [Google Scholar] [CrossRef]
- Vinall, J.; Pavlova, M.; Asmundson, G.J.G.; Rasic, N.; Noel, M. Mental Health Comorbidities in Pediatric Chronic Pain: A Narrative Review of Epidemiology, Models, Neurobiological Mechanisms and Treatment. Children 2016, 3, 40. [Google Scholar] [CrossRef] [Green Version]
- Palermo, T.M.; Valrie, C.; Karlson, C.W. Family and parent influences on pediatric chronic pain: A developmental perspective. Am. Psychol. 2014, 69, 142–152. [Google Scholar] [CrossRef]
- Soltani, S.; Kopala-Sibley, D.; Noel, M. The Co-occurrence of Pediatric Chronic Pain and Depression: A Narrative Review and Conceptualization of Mutual Maintenance. Clin. J. Pain 2019, 35, 633–643. [Google Scholar] [CrossRef]
- Law, E.F.; Zhou, C.; Seung, F.; Perry, F.; Palermo, T.M. Longitudinal study of early adaptation to the coronavirus disease pandemic among youth with chronic pain and their parents: Effects of direct exposures and economic stress. Pain 2021, 162, 2132–2144. [Google Scholar] [CrossRef] [PubMed]
- Tham, S.W.; Murray, C.B.; Law, E.F.; Slack, K.E.; Palermo, T.M. The impact of the coronavirus disease 2019 pandemic on pain and psychological functioning in young adults with chronic pain. Pain 2022, 10–1097. [Google Scholar] [CrossRef] [PubMed]
- Coyne, J.C.; Downey, G. Social Factors and Psychopathology: Stress, Social Support, and Coping Processes. Annu. Rev. Psychol. 1991, 42, 401–425. [Google Scholar] [CrossRef] [PubMed]
- Hammen, C. Stress and Depression. Annu. Rev. Clin. Psychol. 2005, 1, 293–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monroe, S.M.; Bromet, E.J.; Connell, M.M.; Steiner, S.C. Social support, life events, and depressive symptoms: A 1-year prospective study. J. Consult. Clin. Psychol. 1986, 54, 424–431. [Google Scholar] [CrossRef]
- Norris, F.H.; Friedman, M.J.; Watson, P.J.; Byrne, C.M.; Diaz, E.; Kaniasty, K. 60,000 Disaster Victims Speak: Part I. An Empirical Review of the Empirical Literature, 1981–2001. Psychiatry 2002, 65, 207–239. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, M.E.; Weber, K.; Courvoisier, D.S.; Genevay, S. Big Five Personality Traits and Disabling Chronic Low Back Pain: Association with Fear-Avoidance, Anxious and Depressive Moods. J. Pain Res. 2020, 13, 745–754. [Google Scholar] [CrossRef] [Green Version]
- Brown, T.A.; Rosellini, A.J. The direct and interactive effects of neuroticism and life stress on the severity and longitudinal course of depressive symptoms. J. Abnorm. Psychol. 2011, 120, 844–856. [Google Scholar] [CrossRef] [Green Version]
- Hutchinson, J.G.; Williams, P.G. Neuroticism, daily hassles, and depressive symptoms: An examination of moderating and mediating effects. Pers. Individ. Differ. 2007, 42, 1367–1378. [Google Scholar] [CrossRef]
- Kendler, K.S.; Kuhn, J.; Prescott, C.A. The Interrelationship of Neuroticism, Sex, and Stressful Life Events in the Prediction of Episodes of Major Depression. Am. J. Psychiatry 2004, 161, 631–636. [Google Scholar] [CrossRef]
- Klein, D.N.; Kotov, R.; Bufferd, S.J. Personality and Depression: Explanatory Models and Review of the Evidence. Annu. Rev. Clin. Psychol. 2011, 7, 269–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kopala-Sibley, D.C.; Klein, D.N.; Perlman, G.; Kotov, R. Self-criticism and dependency in female adolescents: Prediction of first onsets and disentangling the relationships between personality, stressful life events, and internalizing psychopathology. J. Abnorm. Psychol. 2017, 126, 1029–1043. [Google Scholar] [CrossRef] [PubMed]
- Kopala-Sibley, D.C.; Danzig, A.P.; Kotov, R.; Bromet, E.J.; Carlson, G.A.; Olino, T.M.; Bhatia, V.; Black, S.R.; Klein, D.N. Negative emotionality and its facets moderate the effects of exposure to Hurricane Sandy on children’s postdisaster depression and anxiety symptoms. J. Abnorm. Psychol. 2016, 125, 471–481. [Google Scholar] [CrossRef] [PubMed]
- Kopala-Sibley, D.C.; Kotov, R.; Bromet, E.J.; Carlson, G.A.; Danzig, A.P.; Black, S.R.; Klein, D.N. Personality diatheses and Hurricane Sandy: Effects on post-disaster depression. Psychol. Med. 2015, 46, 865–875. [Google Scholar] [CrossRef] [Green Version]
- Anderson, K.W.; McLean, P.D. Conscientiousness in Depression: Tendencies, Predictive Utility, and Longitudinal Stability. Cogn. Ther. Res. 1997, 21, 223–238. [Google Scholar] [CrossRef]
- Compas, B.E.; Connor-Smith, J.; Jaser, S.S. Temperament, Stress Reactivity, and Coping: Implications for Depression in Childhood and Adolescence. J. Clin. Child Adolesc. Psychol. 2004, 33, 21–31. [Google Scholar] [CrossRef]
- Kotov, R.; Gamez, W.; Schmidt, F.; Watson, D. Linking “big” personality traits to anxiety, depressive, and substance use disorders: A meta-analysis. Psychol. Bull. 2010, 136, 768–821. [Google Scholar] [CrossRef]
- Roberts, B.W.; Kuncel, N.R.; Shiner, R.; Caspi, A.; Goldberg, L.R. The Power of Personality: The Comparative Validity of Personality Traits, Socioeconomic Status, and Cognitive Ability for Predicting Important Life Outcomes. Perspect. Psychol. Sci. 2007, 2, 313–345. [Google Scholar] [CrossRef] [Green Version]
- Beveridge, J.K.; Dobson, K.S.; Madigan, S.; Yeates, K.O.; Stone, A.L.; Wilson, A.C.; Salberg, S.; Mychasiuk, R.; Noel, M. Adverse childhood experiences in parents of youth with chronic pain: Prevalence and comparison with a community-based sample. Pain Rep. 2020, 5, e866. [Google Scholar] [CrossRef]
- Neville, A.; Griep, Y.; Palermo, T.M.; Vervoort, T.; Schulte, F.; Yeates, K.O.; Sumpton, J.E.; Mychasiuk, R.; Noel, M. A “dyadic dance”: Pain catastrophizing moderates the daily relationships between parent mood and protective responses and child chronic pain. Pain 2020, 161, 1072–1082. [Google Scholar] [CrossRef]
- Neville, A.; Jordan, A.; Beveridge, J.K.; Pincus, T.; Noel, M. Diagnostic Uncertainty in Youth with Chronic Pain and Their Parents. J. Pain 2019, 20, 1080–1090. [Google Scholar] [CrossRef]
- Pavlova, M.; Kopala-Sibley, D.C.; Nania, C.; Mychasiuk, R.; Christensen, J.; McPeak, A.; Tomfohr-Madsen, L.; Katz, J.; Palermo, T.M.; Noel, M. Sleep disturbance underlies the co-occurrence of trauma and pediatric chronic pain: A longitudinal examination. Pain 2020, 161, 821–830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soltani, S.; Van Ryckeghem, D.M.; Vervoort, T.; Heathcote, L.C.; Yeates, K.; Sears, C.; Noel, M. Attentional biases in pediatric chronic pain: An eye-tracking study assessing the nature of the bias and its relation to attentional control. Pain 2020, 161, 2263–2273. [Google Scholar] [CrossRef] [PubMed]
- IASP Task Force on Taxonomy. Classification of Chronic Pain, 2nd ed.; IASP Press: Malaga, Spain, 1994. [Google Scholar]
- Neville, A.; Lund, T.; Soltani, S.; Jordan, A.; Stinson, J.; Killackey, T.; Birnie, K.A.; Noel, M. Pediatric Chronic Pain in the Midst of the COVID-19 Pandemic: Lived Experiences of Youth and Parents. J. Pain 2021, 23, 841–851. [Google Scholar] [CrossRef] [PubMed]
- REDCap. Vanderbuilt University. 2018. Available online: https://news.vanderbilt.edu/tag/redcap/ (accessed on 23 April 2020).
- Kashikar-Zuck, S.; Carle, A.; Barnett, K.; Goldschneider, K.R.; Sherry, D.D.; Mara, C.A.; Cunningham, N.; Farrell, J.; Tress, J.; DeWitt, E.M. Longitudinal evaluation of patient-reported outcomes measurement information systems measures in pediatric chronic pain. Pain 2016, 157, 339–347. [Google Scholar] [CrossRef] [Green Version]
- Palermo, T.M.; Harrison, D.; Koh, J.L. Effect of Disease-related Pain on the Health-related Quality of Life of Children and Adolescents with Cystic Fibrosis. Clin. J. Pain 2006, 22, 532–537. [Google Scholar] [CrossRef]
- Chorpita, B.F.; Yim, L.; Moffitt, C.; Umemoto, L.A.; Francis, S.E. Assessment of symptoms of DSM-IV anxiety and depression in children: A revised child anxiety and depression scale. Behav. Res. Ther. 2000, 38, 835–855. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Chorpita, B.F.; Moffitt, C.E.; Gray, J. Psychometric properties of the Revised Child Anxiety and Depression Scale in a clinical sample. Behav. Res. Ther. 2005, 43, 309–322. [Google Scholar] [CrossRef]
- Snaith, R.P. The Hospital Anxiety and Depression Scale. Health Qual. Life Outcomes 2003, 1, 29. [Google Scholar] [CrossRef] [Green Version]
- John, O.P.; Donahue, E.M.; Kentle, R.L. The Big Five Inventory—Versions 4a and 54; Institute of Personality and Social Research, University of California: Berkeley, CA, USA, 1991. [Google Scholar]
- John, O.P.; Naumann, L.P.; Soto, C.J. Paradigm Shift to the Integrative Big Five Trait Taxonomy: History, Measurement, and Con-Ceptual Issues. In Handbook of Personality: Theory and Research; John, O.P., Robins, R.W., Pervin, L.A., Eds.; Guilford Press: New York, NY, USA, 2008; pp. 114–158. [Google Scholar]
- Borghuis, J.; Denissen, J.J.A.; Oberski, D.; Sijtsma, K.; Meeus, W.H.J.; Branje, S.; Koot, H.M.; Bleidorn, W. Big Five personality stability, change, and codevelopment across adolescence and early adulthood. J. Pers. Soc. Psychol. 2017, 113, 641–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fossati, A.; Borroni, S.; Marchione, D.; Maffei, C. The Big Five Inventory (BFI): Reliability and Validity of its Italian Translation in Three Independent Nonclinical Samples. Eur. J. Psychol. Assess. 2011, 27, 50–58. [Google Scholar] [CrossRef]
- Rammstedt, B.; John, O.P. Measuring personality in one minute or less: A 10-item short version of the Big Five Inventory in English and German. J. Res. Pers. 2007, 41, 203–212. [Google Scholar] [CrossRef]
- Speed, B.C.; Nelson, B.D.; Perlman, G.; Klein, D.N.; Kotov, R.; Hajcak, G. Personality and emotional processing: A relationship between extraversion and the late positive potential in adolescence: Personality and the late positive potential. Psychophysiology 2015, 52, 1039–1047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis; The Guilford Press: New York, NY, USA, 2017. [Google Scholar]
- Canadian Pain Task Force. An Action Plan for Pain in Canada; Health Canada: Ottawa, ON, Canada, 2021.
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Silver, R.C.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Chioqueta, A.P.; Stiles, T.C. Personality traits and the development of depression, hopelessness, and suicide ideation. Pers. Individ. Differ. 2005, 38, 1283–1291. [Google Scholar] [CrossRef]
- Gomez, R.; Holmberg, K.; Bounds, J.; Fullarton, C.; Gomez, A. Neuroticism and extraversion as predictors of coping styles during early adolescence. Pers. Individ. Differ. 1999, 27, 3–17. [Google Scholar] [CrossRef]
- Borja, S.E.; Callahan, J.L.; Rambo, P.L. Understanding negative outcomes following traumatic exposure: The roles of neuroticism and social support. Psychol. Trauma Theory Res. Pract. Policy 2009, 1, 118–129. [Google Scholar] [CrossRef] [Green Version]
- Duberstein, P.R.; Laurent, J.; Conner, K.R.; Conwell, Y.; Cox, C. Personality Correlates of Hopelessness in Depressed Inpatients 50 Years of Age and Older. J. Pers. Assess. 2001, 77, 380–390. [Google Scholar] [CrossRef]
- Fredrickson, B.L. The Role of Positive Emotions in Positive Psychology. Am. Psychol. 2001, 56, 218–226. [Google Scholar] [CrossRef]
- Mun, C.J.; Campbell, C.M.; McGill, L.S.; Aaron, R.V. The Early Impact of COVID-19 on Chronic Pain: A Cross-Sectional Investigation of a Large Online Sample of Individuals with Chronic Pain in the United States, April to May, 2020. Pain Med. 2021, 22, 470–480. [Google Scholar] [CrossRef] [PubMed]
- Neville, A.; Soltani, S.; Pavlova, M.; Noel, M. Unravelling the Relationship Between Parent and Child PTSD and Pediatric Chronic Pain: The Mediating Role of Pain Catastrophizing. J. Pain 2018, 19, 196–206. [Google Scholar] [CrossRef] [PubMed]
- Killackey, T.; Noel, M.; Birnie, K.A.; Choinière, M.; Pagé, M.G.; Dassieu, L.; Lacasse, A.; Lalloo, C.; Brennenstuhl, S.; Poulin, P.; et al. COVID-19 Pandemic Impact and Response in Canadian Pediatric Chronic Pain Care: A National Survey of Medical Directors and Pain Professionals. Can. J. Pain 2021, 5, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Birnie, K.A.; Killackey, T.; Stinson, J.; Noel, M.; Lorenzetti, D.L.; Marianayagam, J.; Jordan, I.; Jordan, E.; Neville, A.; Pavlova, M.; et al. Best practices for virtual care to support youth with chronic pain and their families: A rapid systematic review to inform health care and policy during COVID-19 and beyond. Pain Rep. 2021, 6, e935. [Google Scholar] [CrossRef] [PubMed]
- Birnie, K.A.; Pavlova, M.; Neville, A.; Noel, M.; Jordan, I.; Jordan, E.; Marianayagam, J.; Stinson, J.; Lorenzetti, D.L.; Faulkner, V.; et al. Rapid evidence and gap map of virtual care solutions across a stepped care continuum for youth with chronic pain and their families in response to the COVID-19 pandemic. Pain 2021, 162, 2658–2668. [Google Scholar] [CrossRef]
- Partnering for Pain—Identifying the Top 10 Research Priorities in Childhood Chronic Pain in Canada. 2019. Available online: http://bit.ly/2NSYY7p (accessed on 18 April 2022).
- Bell, L.; Cornish, P.; Gauthier, R.; Kargus, C.; Rash, J.; Robbins, R.; Ward, S.; Poulin, P.A. Implementation of the Ottawa Hospital Pain Clinic stepped care program: A preliminary report. Can. J. Pain 2020, 4, 168–178. [Google Scholar] [CrossRef]
- Galea, S.; Merchant, R.M.; Lurie, N. The Mental Health Consequences of COVID-19 and Physical Distancing: The need for prevention and early intervention. JAMA Intern. Med. 2020, 180, 817–818. [Google Scholar] [CrossRef] [Green Version]
- Cornish, P. Stepped Care 2.0: A Paradigm Shift in Mental Health; Springer: Berlin/Heidelberg, Germany, 2020; Available online: https://www.springer.com/gp/book/9783030480547 (accessed on 26 May 2021).



{kind=link}
{kind=link}
| (n = 84 Youth; n = 90 Parents) | |
|---|---|
| Youth age (M years, SD) | 14.39 (2.21) |
| Youth gender (% female) | 67.8 |
| Parent gender (% female) | 86.7 |
| Ethnicity | |
| White | 83.5 |
| Two or more ethnicities | 8.8 |
| Other | 7.7 |
| Aboriginal | 4.4 |
| Latin American | 2.2 |
| Black | 2.2 |
| Chinese | 2.2 |
| South-East Asian | 2.2 |
| Filipino | 1.1 |
| Arab/West Asian | 1.1 |
| Did not want to answer | 2.2 |
| Annual household income (%) | |
| <$10,000–$29,999 | 3.3 |
| $30,000–$59,999 | 6.7 |
| $60,000–$89,999 | 15.6 |
| >$90,000 | 62.2 |
| Did not want to answer | 12.2 |
| Parent education level (%) | |
| High school or less | 7.8 |
| Vocational school/some college | 20.0 |
| College, bachelors degree | 52.2 |
| Graduate/professional school | 20.0 |
| Pre-COVID | During COVID | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | M | n | M | Mean Difference | SD | 95% CI | t | df | p | |
| Parents | ||||||||||
| Depression | 88 | 3.28 | 88 | 4.22 | −0.93 | 2.79 | −1.52 to −0.34 | −3.13 | 87 | <0.01 ** |
| Anxiety | 88 | 6.42 | 88 | 6.65 | −0.23 | 3.05 | −0.87 to 0.42 | −0.70 | 87 | 0.486 |
| COVID-19 impact | 90 | 50.49 | 13.57 | |||||||
| Neuroticism | 89 | 21.30 | 6.27 | |||||||
| Extroversion | 89 | 31.53 | 6.38 | |||||||
| Conscientiousness | 89 | 35.48 | 5.30 | |||||||
| Youth | ||||||||||
| Pain interference | 81 | 55.27 | 81 | 52.10 | 3.17 | 9.37 | 1.10 to 5.24 | 3.05 | 80 | <0.01 ** |
| Depression | 80 | 55.26 | 80 | 54.92 | 0.34 | 14.54 | −2.89 to 3.58 | 0.21 | 80 | 0.833 |
| Anxiety | 72 | 51.17 | 72 | 47.54 | 3.63 | 14.21 | 0.29 to 6.97 | 2.17 | 71 | 0.034 * |
| COVID-19 impact | 84 | 51.90 | 13.49 | |||||||
| Neuroticism | 84 | 25.25 | 6.76 | |||||||
| Extroversion | 84 | 27.78 | 6.72 | |||||||
| Conscientiousness | 84 | 30.08 | 6.42 | |||||||
| β | B | SE | T | R2 | 95% CI | p | |
|---|---|---|---|---|---|---|---|
| Model 1: Youth depression and Neuroticism | |||||||
| Block 1 | 0.45 | <0.01 | |||||
| Gender | 0.03 | 1.14 | 3.52 | 0.32 | −5.88 to 8.15 | 0.75 | |
| Age | 0.15 | 1.24 | 0.76 | 1.64 | −0.27 to 2.76 | 0.11 | |
| Pre-COVID depression | 0.62 ** | 0.72 | 0.10 | 6.64 | 0.51 to 0.92 | <0.01 | |
| Block 2 | 0.54 | <0.01 | |||||
| COVID impact | 0.13 | 0.18 | 0.12 | 1.48 | −0.06 to 0.42 | 0.14 | |
| Neuroticism | 0.31 ** | 0.85 | 0.25 | 3.43 | 0.36 to 1.34 | <0.01 | |
| Block 3 | 0.55 | <0.01 | |||||
| COVID impact * Neuroticism | 0.10 | 0.02 | 0.02 | 1.22 | −0.01 to 0.06 | 0.23 | |
| Model 2: Youth depression and Extroversion | |||||||
| Block 2 | 0.52 | ||||||
| COVID impact | 0.16 | 0.21 | 0.12 | 1.71 | −0.04 to 0.46 | 0.09 | |
| Extroversion | −0.24 ** | −0.65 | 0.24 | −2.74 | −1.13 to −0.18 | <0.01 | |
| Block 3 | 0.54 | ||||||
| COVID impact * Extroversion | −0.14 | −0.03 | 0.02 | −1.75 | −0.05 to 0.004 | 0.09 | |
| Model 3: Youth depression and Conscientiousness | |||||||
| Block 2 | 0.54 | ||||||
| COVID impact | 0.09 | 0.13 | 0.12 | 1.04 | −0.12 to 0.37 | 0.30 | |
| Conscientiousness | −0.28 ** | −0.83 | 0.25 | −3.35 | −1.32 to −0.34 | <0.01 | |
| Block 3 | 0.54 | ||||||
| COVID impact * Conscientiousness | −0.02 | −0.01 | 0.02 | −0.20 | −0.05 to 0.04 | 0.85 | |
| β | B | SE | T | R2 | 95% CI | p | |
| Model 4: Youth anxiety and Neuroticism | |||||||
| Block 1 | 0.40 | <0.01 | |||||
| Gender | 0.08 | 2.77 | 3.33 | 0.83 | −3.87 to 9.41 | 0.41 | |
| Age | 0.18 | 1.27 | 0.68 | 1.86 | −0.09 to 2.64 | 0.08 | |
| Pre-COVID anxiety | 0.56 ** | 0.38 | 0.07 | 5.72 | 0.25 to 0.51 | <0.01 | |
| Block 2 | 0.64 | <0.01 | |||||
| COVID impact | 0.20 * | 0.22 | 0.09 | 2.42 | 0.04 to 0.40 | 0.019 | |
| Neuroticism | 0.52 ** | 1.19 | 0.20 | 6.08 | 0.80 to 1.58 | <0.01 | |
| Block 3 | 0.65 | <0.01 | |||||
| COVID impact * Neuroticism | 0.12 | 0.02 | 0.01 | 1.53 | −0.01 to 0.05 | 0.13 | |
| Model 5: Youth anxiety and Extroversion | |||||||
| Block 2 | 0.52 | <0.01 | |||||
| COVID impact | 0.24 * | 0.26 | 0.10 | 2.53 | 0.06 to 0.47 | 0.014 | |
| Extroversion | −0.28 ** | −0.62 | 0.20 | −3.15 | −1.01 to −0.23 | <0.01 | |
| Block 3 | 0.54 | <0.01 | |||||
| COVID impact * Extroversion | −0.14 | −0.02 | 0.02 | −1.69 | −0.04 to 0.004 | 0.10 | |
| Model 6: Youth anxiety and Conscientiousness | |||||||
| Block 2 | 0.49 | <0.01 | |||||
| COVID impact | 0.17 | 0.18 | 0.11 | 1.70 | −0.03 to 0.40 | 0.09 | |
| Conscientiousness | −0.22 * | −0.51 | 0.22 | −2.29 | −0.95 to −0.07 | 0.03 | |
| Block 3 | 0.53 | <0.01 | |||||
| COVID impact * Conscientiousness | −0.19 * | −0.05 | 0.02 | −2.17 | −0.09 to −0.003 | 0.034 | |
| β | B | SE | T | R2 | 95% CI | p | |
| Model 7: Youth Pain Interference and Neuroticism | |||||||
| Block 1 | 0.25 | <0.01 | |||||
| Gender | −0.003 | −0.06 | 1.99 | −0.03 | −4.02 to 3.89 | 0.97 | |
| Age | 0.08 | 0.35 | 0.43 | 0.82 | −0.50 to 1.20 | 0.41 | |
| Pre-COVID pain interference | 0.48 ** | 0.49 | 0.11 | 4.60 | 0.28 to 0.70 | <0.01 | |
| Block 2 | 0.33 | <0.01 | |||||
| COVID impact | 0.27 * | 0.19 | 0.07 | 2.59 | 0.04 to 0.33 | 0.01 | |
| Neuroticism | 0.19 | 0.26 | 0.14 | 1.80 | −0.03 to 0.55 | 0.08 | |
| Block 3 | 0.34 | <0.01 | |||||
| COVID impact * Neuroticism | −0.10 | −0.01 | 0.01 | −0.97 | −0.03 to 0.01 | 0.34 | |
| Model 8: Youth Pain Interference and Extroversion | |||||||
| Block 2 | 0.35 | <0.01 | |||||
| COVID impact | 0.30 ** | 0.20 | 0.07 | 2.82 | 0.06 to 0.35 | <0.01 | |
| Extroversion | −0.21 * | −0.29 | 0.14 | −2.15 | −0.57 to −0.02 | 0.04 | |
| Block 3 | 0.35 | <0.01 | |||||
| COVID impact * Extroversion | 0.10 | 0.01 | 0.01 | 1.00 | −0.01 to 0.03 | 0.32 | |
| Model 9: Youth Pain Interference and Conscientiousness | |||||||
| Block 2 | 0.34 | <0.01 | |||||
| COVID impact | 0.24 * | 0.17 | 0.07 | 2.28 | 0.02 to 0.31 | 0.03 | |
| Conscientiousness | −0.19 | −0.28 | 0.15 | −1.93 | −0.57 to 0.01 | 0.06 | |
| Block 3 | 0.35 | <0.01 | |||||
| COVID impact * Conscientiousness | 0.06 | 0.52 |
| β | B | SE | T | R2 | 95% CI | p | |
|---|---|---|---|---|---|---|---|
| Model 1: Parent depression and Neuroticism | |||||||
| Block 1 | 0.59 | <0.01 | |||||
| Gender | −0.12 | −1.30 | 0.77 | −1.68 | −2.83 to 0.23 | 0.10 | |
| Pre-COVID depression | 0.77 ** | 0.98 | 0.09 | 10.95 | 0.80 to 1.16 | <0.01 | |
| Block 2 | 0.61 | <0.01 | |||||
| COVID impact | 0.06 | 0.02 | 0.02 | 0.89 | −0.03 to 0.07 | 0.37 | |
| Neuroticism | 0.15 * | 0.10 | 0.05 | 2.14 | 0.01 to 0.20 | 0.04 | |
| Block 3 | 0.62 | <0.01 | |||||
| COVID impact * Neuroticism | 0.11 | 0.01 | 0.003 | 1.61 | −0.001 to 0.01 | 0.11 | |
| Model 2: Parent depression and Extroversion | |||||||
| Block 2 | 0.63 | ||||||
| COVID impact | 0.06 | 0.02 | 0.02 | 0.88 | −0.03 to 0.06 | 0.38 | |
| Extroversion | −0.20 ** | −0.13 | 0.05 | −2.88 | −0.22 to −0.04 | <0.01 | |
| Block 3 | 0.64 | ||||||
| COVID impact * Extroversion | −0.12 | −0.01 | 0.004 | −1.83 | −0.01 to 0.001 | 0.07 | |
| Model 3: Parent depression and Conscientiousness | |||||||
| Block 2 | 0.59 | ||||||
| COVID impact | 0.06 | 0.02 | 0.02 | 0.77 | −0.03 to 0.07 | 0.44 | |
| Conscientiousness | −0.03 | −0.03 | 0.06 | −0.43 | −0.14 to 0.09 | 0.67 | |
| Block 3 | 0.60 | ||||||
| COVID impact * Conscientiousness | −0.11 | −0.01 | 0.004 | −1.56 | −0.02 to 0.002 | 0.12 | |
| Model 4: Parent anxiety and Neuroticism | |||||||
| Block 1 | 0.53 | ||||||
| Gender | −0.11 | −1.20 | 0.81 | −1.48 | −2.80 to 0.41 | 0.14 | |
| Pre-COVID anxiety | 0.73 ** | 0.78 | 0.08 | 9.73 | 0.62 to 0.94 | <0.01 | |
| Block 2 | 0.63 | ||||||
| COVID impact | 0.18 * | 0.06 | 0.02 | 2.60 | 0.01 to 0.10 | 0.01 | |
| Neuroticism | 0.29 ** | 0.19 | 0.05 | 3.97 | 0.10 to 0.29 | <0.01 | |
| Block 3 | 0.65 | ||||||
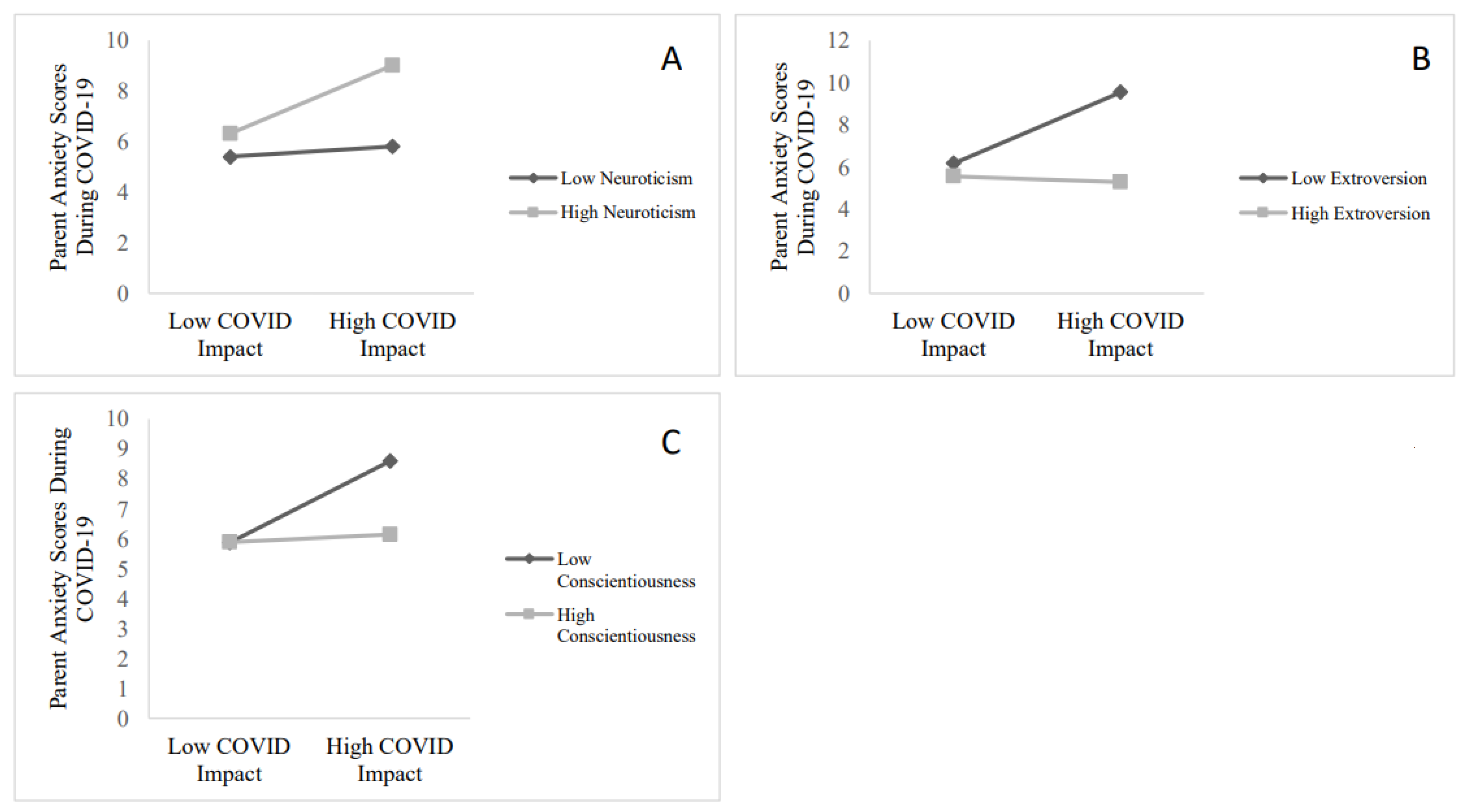
| COVID impact * Neuroticism | 0.16 * | 0.01 | 0.003 | 2.34 | 0.001 to 0.01 | 0.02 | |
| Model 5: Parent anxiety and Extroversion | |||||||
| Block 2 | 0.64 | ||||||
| COVID impact | 0.16 * | 0.05 | 0.02 | 2.45 | 0.01 to 0.09 | 0.02 | |
| Extroversion | −0.30 ** | −0.20 | 0.04 | −4.60 | −0.28 to −0.11 | <0.01 | |
| Block 3 | 0.68 | ||||||
| COVID impact * Extroversion | −0.20 ** | −0.01 | 0.003 | −3.23 | −0.02 to −0.004 | <0.01 | |
| Model 6: Parent anxiety and Conscientiousness | |||||||
| Block 2 | 0.58 | ||||||
| COVID impact | 0.16 * | 0.05 | 0.02 | 2.16 | 0.004 to 0.10 | 0.03 | |
| Conscientiousness | −0.16 * | −0.13 | 0.06 | −2.25 | −0.24 to −0.12 | 0.03 | |
| Block 3 | 0.60 | ||||||
| COVID impact * Conscientiousness | −0.15 * | −0.01 | 0.004 | −2.10 | −0.02 to 0 | 0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Birnie, K.A.; Kopala-Sibley, D.C.; Pavlova, M.; Nania, C.G.; Bernier, E.; Stinson, J.N.; Noel, M. The Impact of the COVID-19 Pandemic on Youth with Chronic Pain and Their Parents: A Longitudinal Examination of Who Are Most at Risk. Children 2022, 9, 745. https://doi.org/10.3390/children9050745
Birnie KA, Kopala-Sibley DC, Pavlova M, Nania CG, Bernier E, Stinson JN, Noel M. The Impact of the COVID-19 Pandemic on Youth with Chronic Pain and Their Parents: A Longitudinal Examination of Who Are Most at Risk. Children. 2022; 9(5):745. https://doi.org/10.3390/children9050745
Chicago/Turabian StyleBirnie, Kathryn A., Daniel C. Kopala-Sibley, Maria Pavlova, Cara G. Nania, Emily Bernier, Jennifer N. Stinson, and Melanie Noel. 2022. "The Impact of the COVID-19 Pandemic on Youth with Chronic Pain and Their Parents: A Longitudinal Examination of Who Are Most at Risk" Children 9, no. 5: 745. https://doi.org/10.3390/children9050745