
Medical Comorbidities in MECP2 Duplication Syndrome: Results from the International MECP2 Duplication Database

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
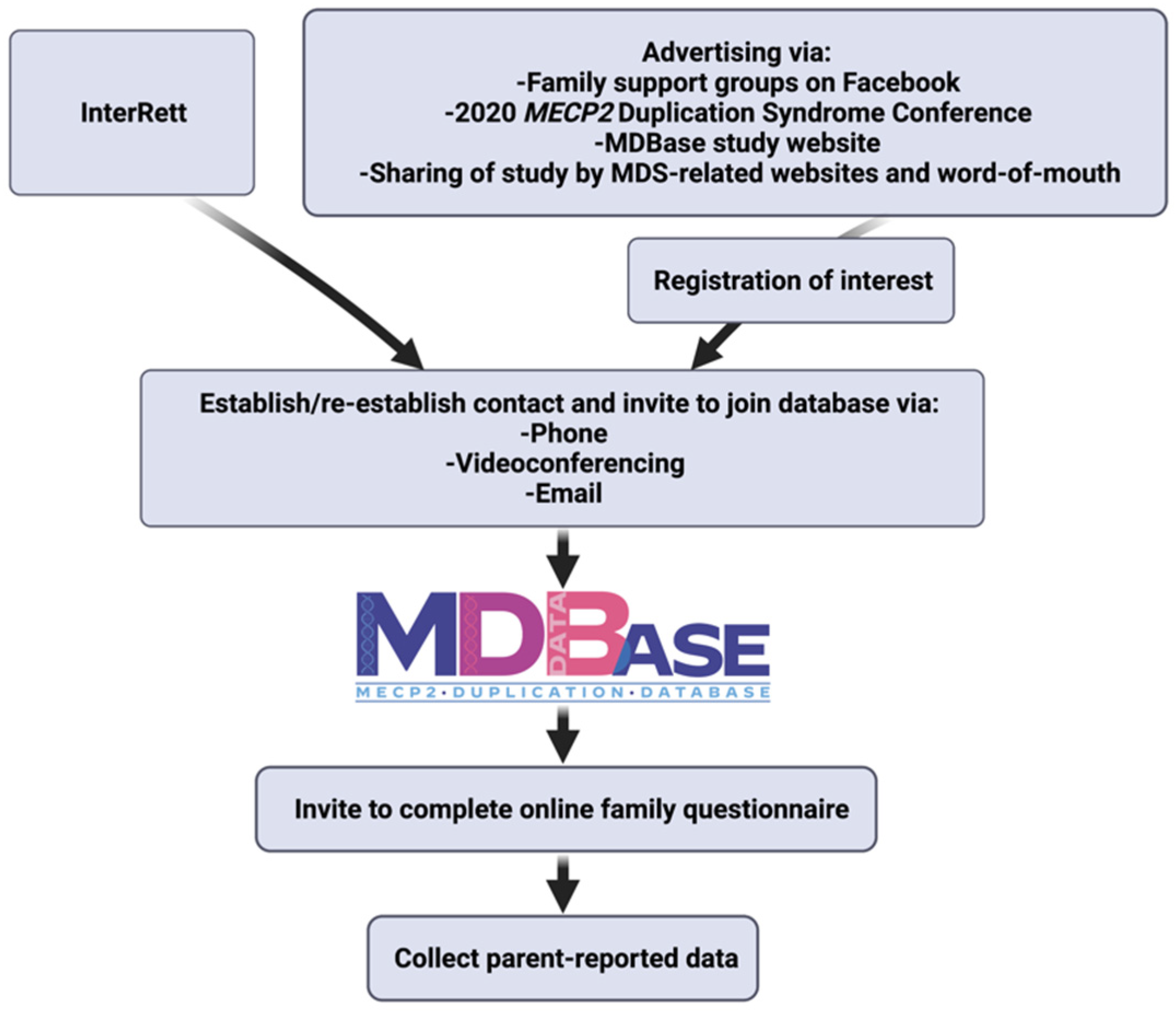
2.1. Data Source
2.2. Data Analysis
3. Results
3.1. Study Population
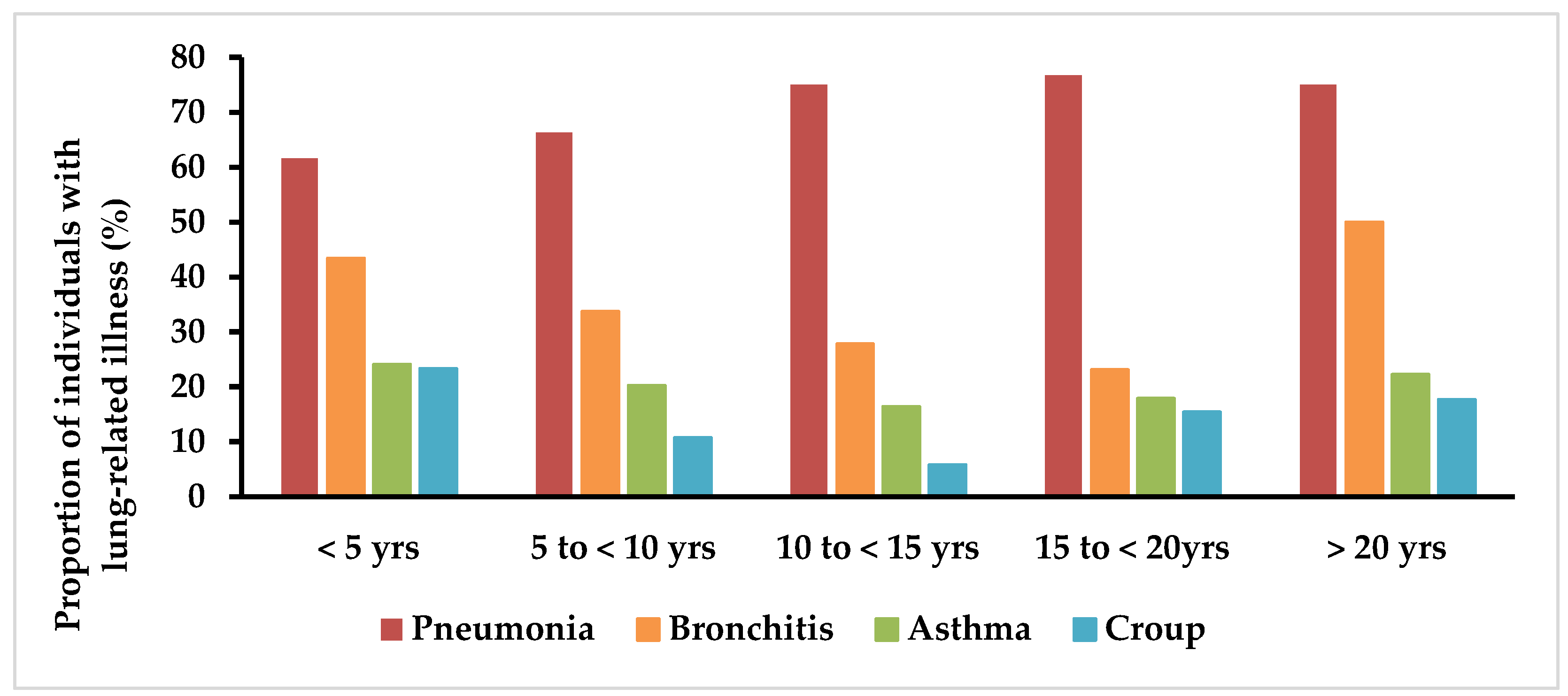
3.2. Cardiopulmonary Health
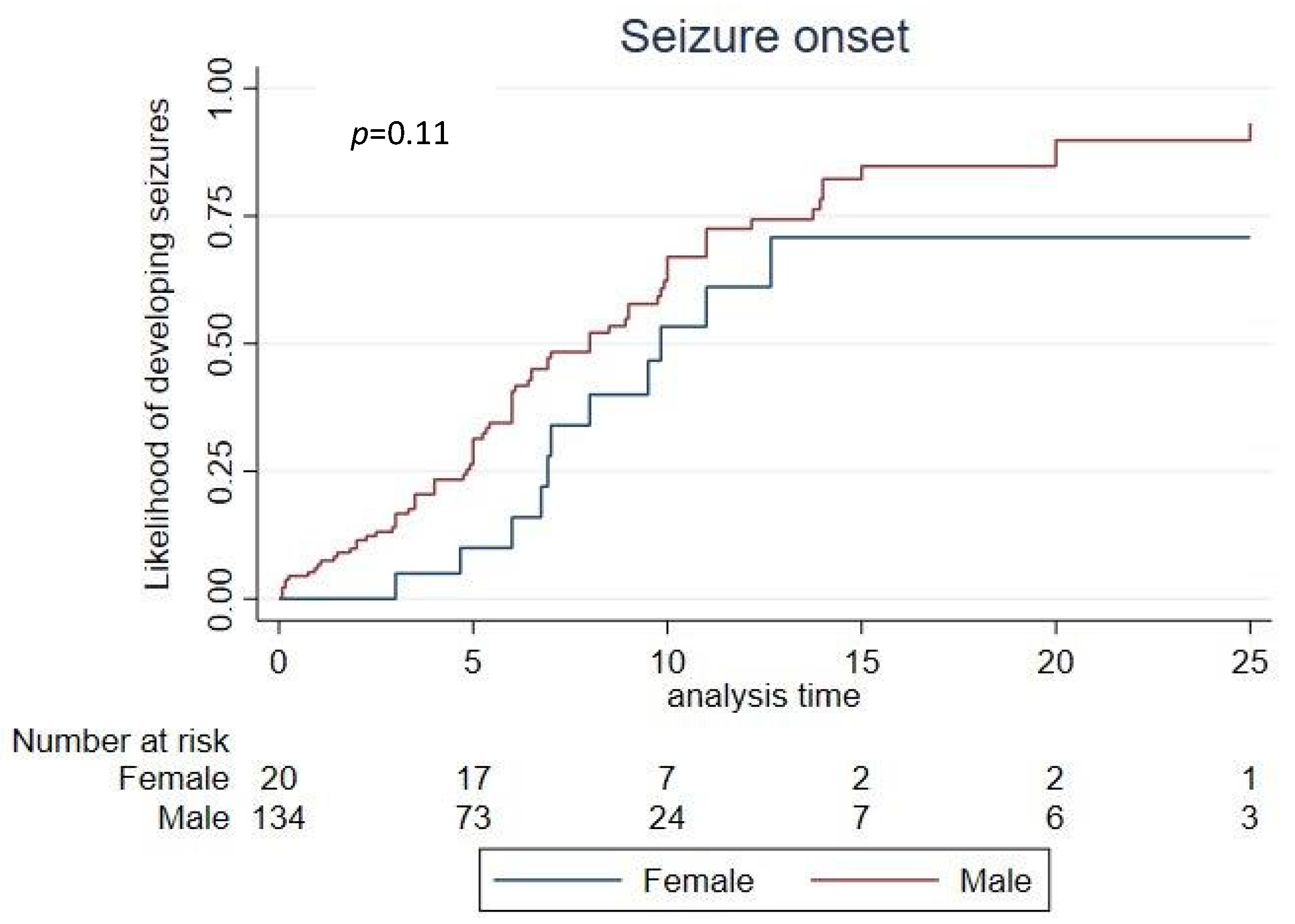
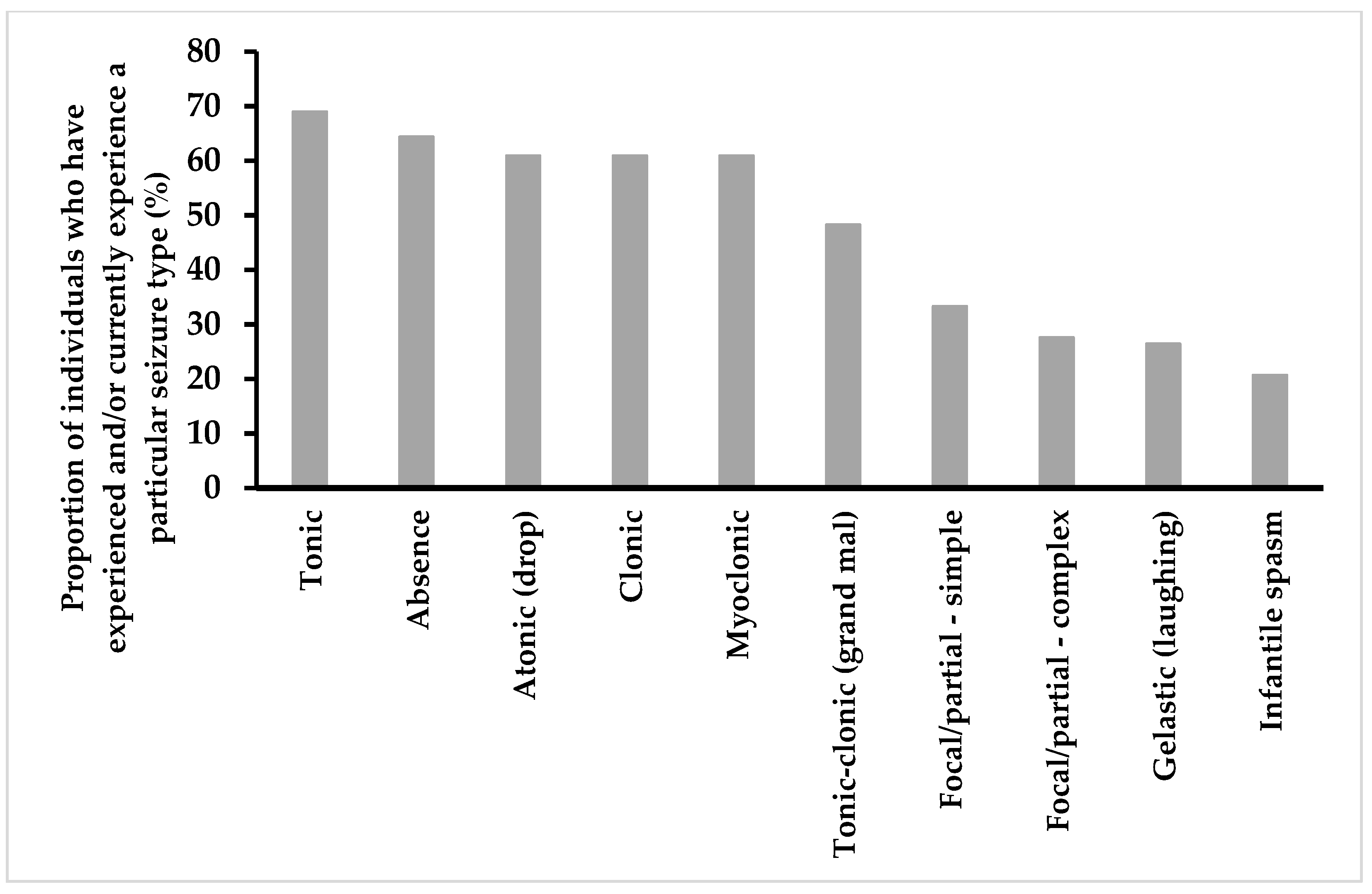
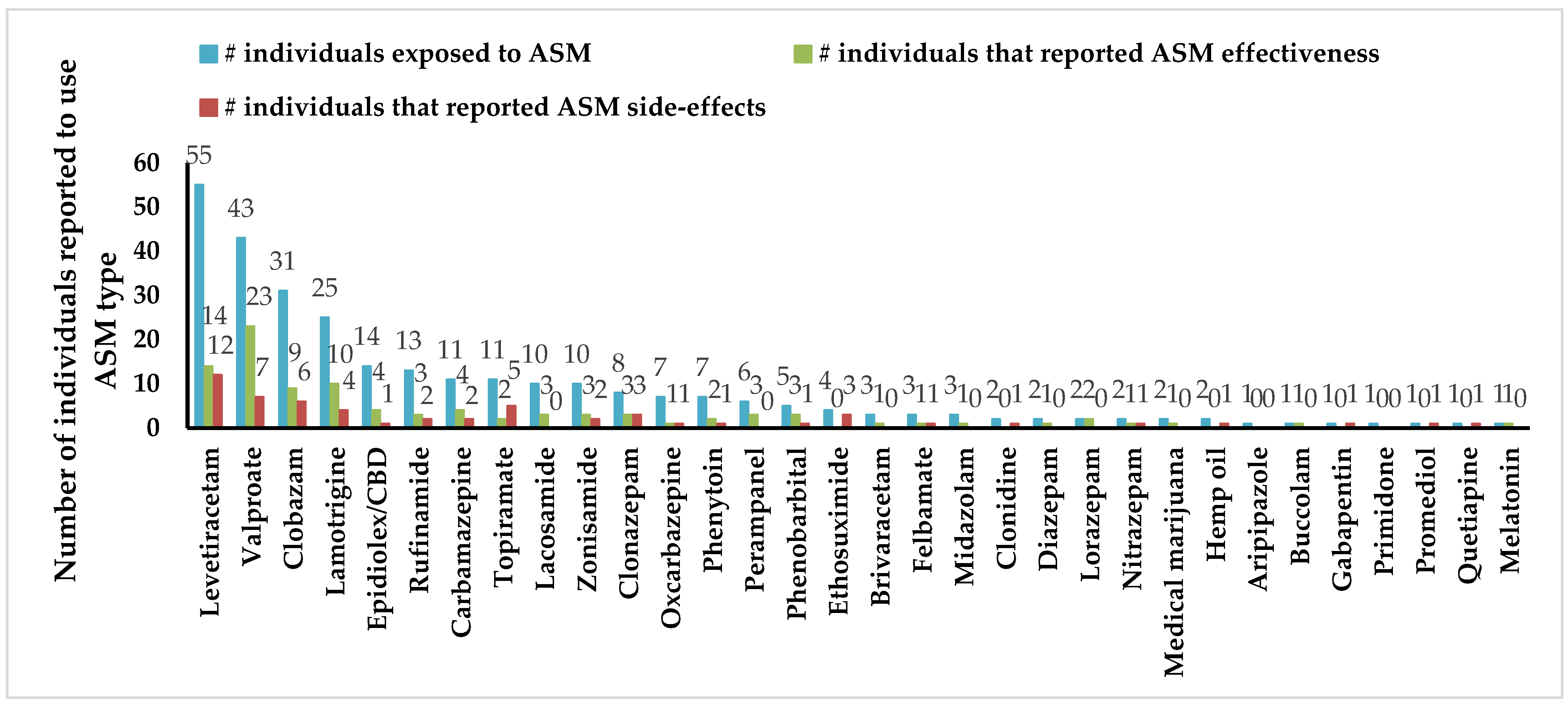
3.3. Epilepsy
3.4. Gastrointestinal Health
3.5. Ear, Nose and Throat (ENT) Health
3.6. Urogenital Problems
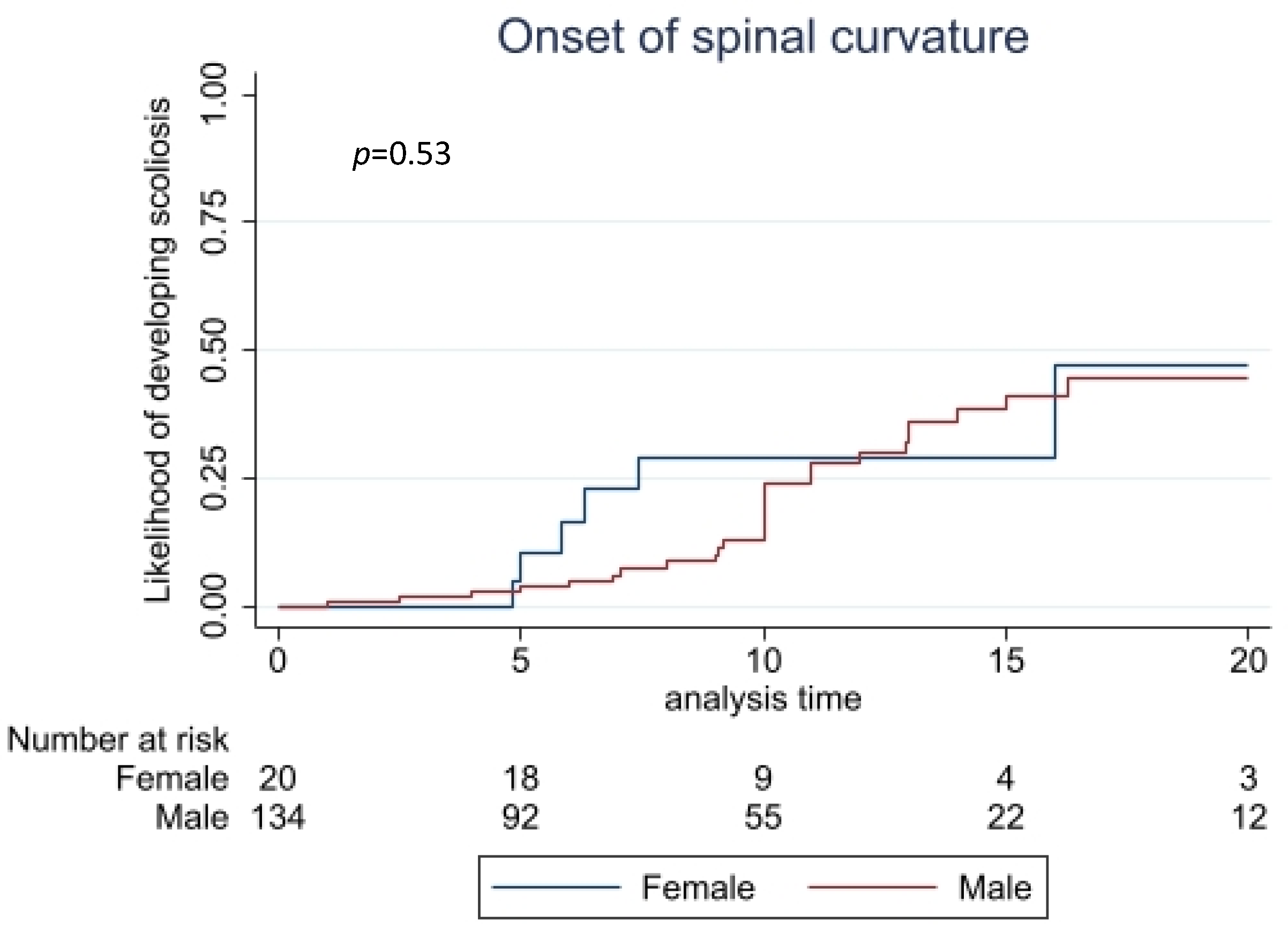
3.7. Musculoskeletal Problems
3.8. Abnormal Pain Sensation
3.9. Sleep
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Giudice-Nairn, P.; Downs, J.; Wong, K.; Wilson, D.; Ta, D.; Gattas, M.; Amor, D.; Thompson, E.; Kirrali-Borri, C.; Ellaway, C.; et al. The incidence, prevalence and clinical features of MECP2 duplication syndrome in Australian children. J. Paediatr. Child Health 2019, 55, 1315–1322. [Google Scholar] [CrossRef] [PubMed]
- Van Esch, H. MECP2 duplication syndrome. Mol. Syndromol. 2011, 2, 128–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miguet, M.; Faivre, L.; Amiel, J.; Nizon, M.; Touraine, R.; Prieur, F.; Pasquier, L.; Lefebvre, M.; Thevenon, J.; Dubourg, C.; et al. Further delineation of the MECP2 duplication syndrome phenotype in 59 French male patients, with a particular focus on morphological and neurological features. J. Med. Genet. 2018, 55, 359–371. [Google Scholar] [CrossRef] [Green Version]
- Peters, S.U.; Fu, C.; Marsh, E.D.; Benke, T.A.; Suter, B.; Skinner, S.A.; Lieberman, D.N.; Standridge, S.; Jones, M.; Beisang, A.; et al. Phenotypic features in MECP2 duplication syndrome: Effects of age. Am. J. Med. Genet. Part A 2020, 185, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Lubs, H.; Abidi, F.; Bier, J.-A.B.; Abuelo, D.; Ouzts, L.; Voeller, K.; Fennell, E.; Stevenson, R.E.; Schwartz, C.E.; Arena, F. XLMR syndrome characterized by multiple respiratory infections, hypertelorism, severe CNS deterioration and early death localizes to distal Xq28. Am. J. Med. Genet. 1999, 85, 243–248. [Google Scholar] [CrossRef]
- Louise, S.; Fyfe, S.; Bebbington, A.; Bahi-Buisson, N.; Anderson, A.; Pineda, M.; Percy, A.; Ben Zeev, B.; Wu, X.R.; Bao, X.; et al. InterRett, a model for international data collection in a rare genetic disorder. Res. Autism Spectr. Disord. 2009, 3, 639–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, S.U.; Fu, C.; Suter, B.; Marsh, E.; Benke, T.A.; Skinner, S.A.; Lieberman, D.N.; Standridge, S.; Jones, M.; Beisang, A.; et al. Characterizing the phenotypic effect of Xq28 duplication size inMECP2duplication syndrome. Clin. Genet. 2019, 95, 575–581. [Google Scholar] [CrossRef]
- San Antonio-Arce, V.; Fenollar-Cortés, M.; Oancea Ionescu, R.; DeSantos-Moreno, T.; Gallego-Merlo, J.; Illana Cámara, F.J.; Cotarelo Pérez, M.C. MECP2 duplications in symptomatic females: Report on 3 patients showing the broad phenotypic spectrum. Child Neurol. Open 2016, 3, 2329048x16630673. [Google Scholar] [CrossRef] [Green Version]
- Lim, Z.; Downs, J.; Wong, K.; Ellaway, C.; Leonard, H. Expanding the clinical picture of theMECP2Duplication syndrome. Clin. Genet. 2016, 91, 557–563. [Google Scholar] [CrossRef]
- Wu, W.; He, J.; Shao, X. Incidence and mortality trend of congenital heart disease at the global, regional, and national level, 1990–2017. Medicine 2020, 99, e20593. [Google Scholar] [CrossRef]
- Nembhard, W.N.; Bourke, J.; Leonard, H.; Eckersley, L.; Li, J.; Bower, C. Twenty-five-year survival for aboriginal and caucasian children with congenital heart defects in Western Australia, 1980 to 2010. Birth Defects Res. Part A Clin. Mol. Teratol. 2016, 106, 1016–1031. [Google Scholar] [CrossRef] [PubMed]
- Ko, J.M. Genetic Syndromes associated with Congenital Heart Disease. Korean Circ. J. 2015, 45, 357–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Chehadeh, S.; Faivre, L.; Mosca-Boidron, A.L.; Malan, V.; Amiel, J.; Nizon, M.; Touraine, R.; Prieur, F.; Pasquier, L.; Callier, P.; et al. Large national series of patients with Xq28 duplication involving MECP2: Delineation of brain MRI abnormalities in 30 affected patients. Am. J. Med. Genet. A 2015, 170, 116–129. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.; Kölsch, U.; Krüger, R.; Unterwalder, N.; Hameister, K.; Kaiser, F.M.; Vignoli, A.; Rossi, R.; Botella, M.P.; Budisteanu, M.; et al. Infectious and Immunologic Phenotype of MECP2 Duplication Syndrome. J. Clin. Immunol. 2015, 35, 168–181. [Google Scholar] [CrossRef]
- Weinberg, G.A.; Hall, C.B.; Iwane, M.K.; Poehling, K.A.; Edwards, K.M.; Griffin, M.R.; Staat, M.A.; Curns, A.T.; Erdman, D.D.; Szilagyi, P.G. Parainfluenza Virus Infection of Young Children: Estimates of the Population-Based Burden of Hospitalization. J. Pediatr. 2009, 154, 694–699. [Google Scholar] [CrossRef]
- Dharmage, S.C.; Perret, J.L.; Custovic, A. Epidemiology of Asthma in Children and Adults. Front. Pediatr. 2019, 7, 246. [Google Scholar] [CrossRef]
- Statistics ABo. National Health Survey: First Results 2017-18 Financial Year 2018. Available online: https://www.abs.gov.au/statistics/health/health-conditions-and-risks/national-health-survey-first-results/2017-18#data-download (accessed on 21 February 2022).
- Blackmore, A.M.; Bear, N.; Blair, E.; Gibson, N.; Jalla, C.; Langdon, K.; Moshovis, L.; Steer, K.; Wilson, A.C. Factors Associated with Respiratory Illness in Children and Young Adults with Cerebral Palsy. J. Pediatr. 2015, 168, 151–157.e1. [Google Scholar] [CrossRef]
- Auber, B.; Burfeind, P.; Thiels, C.; Alsat, E.; Shoukier, M.; Liehr, T.; Nelle, H.; Bartels, I.; Salinas-Riester, G.; Laccone, F. An unbalanced translocation resulting in a duplication of Xq28 causes a Rett syndrome-like phenotype in a female patient. Clin. Genet. 2010, 77, 593–597. [Google Scholar] [CrossRef]
- Lund, C.; Brodtkorb, E.; Røsby, O.; Rødningen, O.K.; Selmer, K.K. Copy number variants in adult patients with Lennox–Gastaut syndrome features. Epilepsy Res. 2013, 105, 110–117. [Google Scholar] [CrossRef]
- Belligni, E.F.; Palmer, R.W.; Hennekam, R.C.M. MECP2 duplication in a patient with congenital central hypoventilation. Am. J. Med Genet. Part A 2010, 152, 1591–1593. [Google Scholar] [CrossRef]
- van Baelen, A.; Verhoustraeten, L.; Kenis, S.; Meuwissen, M.; Boudewyns, A.; van Hoorenbeeck, K.; Verhulst, S. Sleep-disordered breathing and nocturnal hypoventilation in children with the MECP2 duplication syndrome: A case series and review of the literature. Am. J. Med. Genet. A 2020, 182, 2437–2441. [Google Scholar] [CrossRef] [PubMed]
- Takeguchi, R.; Takahashi, S.; Akaba, Y.; Tanaka, R.; Nabatame, S.; Kurosawa, K.; Matsuishi, T.; Itoh, M. Early diagnosis of MECP2 duplication syndrome: Insights from a nationwide survey in Japan. J. Neurol. Sci. 2021, 422, 117321. [Google Scholar] [CrossRef] [PubMed]
- DiMario, F.J.; Burleson, J.A. Autonomic nervous system function in severe breath-holding spells. Pediatr. Neurol. 1993, 9, 268–274. [Google Scholar] [CrossRef]
- Anil, B.G.; Nedunchezian, K.; Jayanthini, V.; Pathmanabhan, M. Breath holding spells: Evaluation of autonomic nervous system function. Indian Pediatr. 2005, 42, 923–927. [Google Scholar]
- Lugtenberg, D.; Kleefstra, T.; Oudakker, A.R.; Nillesen, W.M.; Yntema, H.G.; Tzschach, A.; Raynaud, M.; Rating, D.; Journel, H.; Chelly, J.; et al. Structural variation in Xq28: MECP2 duplications in 1% of patients with unexplained XLMR and in 2% of male patients with severe encephalopathy. Eur. J. Hum. Genet. 2009, 17, 444–453. [Google Scholar] [CrossRef] [Green Version]
- Mackay, J.; Downs, J.; Wong, K.; Heyworth, J.; Epstein, A.; Leonard, H. Autonomic breathing abnormalities in Rett syndrome: Caregiver perspectives in an international database study. J. Neurodev. Disord. 2017, 9, 15. [Google Scholar] [CrossRef]
- Hosmer, D.W., Jr.; Lemeshow, S.; May, S. Applied Survival Analysis: Regression Modeling of Time-to-Event Data, 2nd ed.; Wiley: Hoboken, NJ, USA, 2008. [Google Scholar]
- Marafi, D.; Suter, B.; Schultz, R.; Glaze, D.; Pavlik, V.N.; Goldman, A.M. Spectrum and time course of epilepsy and the associated cognitive decline in MECP2 duplication syndrome. Neurology 2018, 92, e108–e114. [Google Scholar] [CrossRef]
- Cutri-French, C.; Armstrong, D.; Saby, J.; Gorman, C.; Lane, J.; Fu, C.; Peters, S.U.; Percy, A.; Neul, J.L.; Marsh, E.D. Comparison of Core Features in Four Developmental Encephalopathies in the Rett Natural History Study. Ann. Neurol. 2020, 88, 396–406. [Google Scholar] [CrossRef]
- Rajaprakash, M.; Richer, J.; Sell, E. Valproic acid as a monotherapy in drug-resistant methyl-CpG-binding protein 2 gene (MECP2) duplication-related epilepsy. Epilepsy Behav. Case Rep. 2018, 10, 133–136. [Google Scholar] [CrossRef]
- Hmouda, H.; Ben Salem, C.; Grira, M.; Slim, R.; Bouraoui, K. Carbamazepine-induced urinary retention. Br. J. Clin. Pharmacol. 2007, 64, 833–834. [Google Scholar]
- Schattner, A.; Al-Bewerat, A. Levetiracetam (Keppra), urinary retention and literature search. Neth. J. Med. 2016, 74, 371. [Google Scholar] [PubMed]
- Cilio, M.R.; Kartashov, A.I.; Vigevano, F. The long-term use of felbamate in children with severe refractory epilepsy. Epilepsy Res. 2001, 47, 1–7. [Google Scholar] [CrossRef]
- Geffrey, A.L.; Pollack, S.F.; Bruno, P.L.; Thiele, E.A. Drug-drug interaction between clobazam and cannabidiol in children with refractory epilepsy. Epilepsia 2015, 56, 1246–1251. [Google Scholar] [CrossRef] [PubMed]
- Nussinovitch, M.; Soen, G.; Volovitz, B.; Varsano, I.; Luttwak, P.Z. Urinary Retention Related to Phenytoin Therapy. Clin. Pediatr. 1995, 34, 382–383. [Google Scholar] [CrossRef] [PubMed]
- Leonard, H.; Downs, J.; Jian, L.; Bebbington, A.; Jacoby, P.; Nagarajan, L.; Ravine, D.; Woodhead, H. Valproate and risk of fracture in Rett syndrome. Arch. Dis. Child. 2010, 95, 444–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramocki, M.B.; Peters, S.U.; Tavyev, Y.J.; Zhang, F.; Carvalho, C.M.; Schaaf, C.P.; Richman, R.; Fang, P.; Glaze, D.G.; Lupski, J.R.; et al. Autism and other neuropsychiatric symptoms are prevalent in individuals with MeCP2 duplication syndrome. Ann. Neurol. 2009, 66, 771–782. [Google Scholar] [CrossRef] [Green Version]
- Breman, A.M.; Ramocki, M.B.; Kang, S.H.; Williams, M.; Freedenberg, D.; Patel, A.; Bader, P.I.; Cheung, S.W. MECP2 duplications in six patients with complex sex chromosome rearrangements. Eur. J. Hum. Genet. 2011, 19, 409–415. [Google Scholar] [CrossRef] [Green Version]
- Pascual-Alonso, A.; Blasco, L.; Vidal, S.; Gean, E.; Rubio, P.; O’Callaghan, M.; Martinez-Monseny, A.; Castells, A.A.; Xiol, C.; Català, V.; et al. Molecular characterization of Spanish patients with MECP2 duplication syndrome. Clin. Genet. 2020, 97, 610–620. [Google Scholar] [CrossRef]
- Downs, J.; Géranton, S.M.; Bebbington, A.; Jacoby, P.; Bahi-Buisson, N.; Ravine, D.; Leonard, H. Linking MECP2 and pain sensitivity: The example of Rett syndrome. Am. J. Med Genet. Part A 2010, 152, 1197–1205. [Google Scholar] [CrossRef] [Green Version]
- Zhang, R.; Huang, M.; Cao, Z.; Qi, J.; Qiu, Z.; Chiang, L.-Y. MeCP2 plays an analgesic role in pain transmission through regulating CREB / miR-132 pathway. Mol. Pain 2015, 11, 19. [Google Scholar] [CrossRef] [Green Version]
- Leonard, H.; Cobb, S.; Downs, J. Clinical and biological progress over 50 years in Rett syndrome. Nat. Rev. Neurol. 2016, 13, 37–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Males | Females | Total | |
|---|---|---|---|
| Median age (range) | 8.76 years (0.94–51.59 years) | 10.76 years (4.88–31.36 years) | 9.16 years (0.94–51.59 years) |
| N | N | N | |
| 0–<5 years | 40 | 1 | 12 |
| 5–<10 years | 34 | 8 | 42 |
| 10–<15 years | 27 | 7 | 34 |
| 15–<20 years | 13 | 1 | 14 |
| 20+ years | 20 | 3 | 23 |
| All age groups (%) | 134 (87%) | 20 (13%) | 154 (100%) |
| Continent | N (%) | ||
| North America 1 | 76 (49%) | ||
| Europe 2 | 51 (33%) | ||
| Oceania 3 | 21 (14%) | ||
| Asia 4 | 5 (3%) | ||
| South America 5 | 1 (1%) | ||
| Feature | Males | Females | Total | p-Value * |
|---|---|---|---|---|
| n/N (%) | n/N (%) | n/N (%) | ||
| Respiratory problems | ||||
| Pneumonia | 89/122 (73%) | 8/18 (44%) | 97/140 (70%) | 0.017 |
| Bronchitis | 60/118 (51%) | 4/19 (21%) | 64/137 (47%) | 0.013 |
| Bronchiolitis | 76/120 (63%) | 7/18 (39%) | 83/138 (60%) | 0.044 |
| Asthma | 31/119 (26%) | 3/18 (17%) | 34/137 (25%) | 0.295 |
| Croup | 29/116 (25%) | 2/17 (12%) | 31/133 (23%) | 0.187 |
| Aspiration | 72/127 (57%) | 9/20 (45%) | 81/147 (55%) | 0.231 |
| Seizures/epilepsy | 78/128 (61%) | 12/20 (60%) | 90/148 (61%) | 0.561 |
| Treatment-refractory seizures | 51/75 (68%) | 9/12 (75%) | 60/87 (69%) | 0.453 |
| Lennox–Gastaut syndrome | 20/77 (26%) | 2/12 (17%) | 22/89 (25%) | 0.386 |
| Gastrointestinal problems | 115/124 (93%) | 15/18 (83%) | 130/142 (92%) | 0.180 |
| Constipation | 111/117 (95%) | 15/18 (83%) | 126/135 (93%) | 0.100 |
| Intestinal pseudo-obstruction | 21/106 (20%) | 2/16 (13%) | 23/122 (19%) | 0.381 |
| Reflux | 97/115 (84%) | 10/17 (59%) | 107/132 (81%) | 0.020 |
| Air swallowing | 32/111 (29%) | 3/17 (18%) | 35/128 (27%) | 0.258 |
| Slow gut motility | 54/106 (51%) | 4/17 (24%) | 58/123 (47%) | 0.031 |
| Gallbladder problems | 6/103 (6%) | 1/17 (6%) | 7/120 (6%) | 0.667 |
| Ear, nose and throat (ENT) infections | ||||
| Otitis | 76/126 (60%) | 12/19 (63%) | 88/145 (61%) | 0.512 |
| Sinusitis | 45/122 (37%) | 5/18 (28%) | 50/140 (36%) | 0.318 |
| Pharyngitis/tonsillitis | 72/122 (59%) | 16/18 (89%) | 88/140 (63%) | 0.011 |
| Urogenital problems | ||||
| Urinary tract infection | 44/124 (35%) | 11/19 (58%) | 55/143 (38%) | 0.055 |
| Urinary retention | 37/123 (30%) | 4/19 (21%) | 41/142 (29%) | 0.304 |
| Episodes lasting more than a day | 13/36 (36%) | 1/4 (25%) | 14/40 (35%) | 0.562 |
| Scoliosis | 27/124 (22%) | 6/19 (32%) | 33/143 (23%) | 0.250 |
| Congenital heart disease (CHD) | 21/127 (17%) | 6/20 (30%) | 27/147 (18%) | 0.130 |
| Autonomic problems | ||||
| Cold peripheries | 90/125 (72%) | 11/20 (55%) | 101/145 (70%) | 0.103 |
| Episodes of hyperventilation | 16/124 (13%) | 2/20 (10%) | 18/144 (13%) | 0.528 |
| Episodes of breath holding | 48/125 (38%) | 7/19 (37%) | 55/144 (38%) | 0.555 |
| Problems regulating body temperature | 75/126 (60%) | 8/20 (40%) | 83/146 (57%) | 0.082 |
| Abnormal pain sensation | 71/124 (57%) | 14/19 (74%) | 85/143 (59%) | 0.133 |
| Decreased pain sensitivity | 67/124 (54%) | 11/19 (58%) | 78/143 (55%) | 0.475 |
| Increased pain sensitivity | 5/124 (4%) | 3/19 (16%) | 8/143 (6%) | 0.073 |
| Sleep apnoea | 54/123 (44%) | 6/19 (32%) | 60/142 (42%) | 0.225 |
| Age Range | Males | Females | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n/N (%) | Med Times (Range) | n/N (%) | Med Times (Range) | n/N (%) | Med Times (Range) | ||||
| Birth to 12 months | 56/78 (72%) | N = 56 | 2 (1–20) | 5/11 (45%) | N = 5 | 2 (1–6.5) | 61/89 (69%) | N = 61 | 2 (1–20) |
| 12 to 24 months | 65/75 (87%) | N = 65 | 2 (1–50) | 10/12 (83%) | N = 10 | 2.5 (1–6.5) | 75/87 (86%) | N = 75 | 2 (1–50) |
| 2 to 5 years | 55/64 (86%) | N = 55 | 3 (1–20) | 9/11 (82%) | N = 9 | 4 (1–18) | 64/75 (85%) | N = 64 | 3 (1–20) |
| 5 to 10 years | 44/51 (86%) | N = 44 | 2 (1–30) | 5/10 (50%) | N = 5 | 4 (2–15) | 49/61 (80%) | N = 49 | 3 (1–30) |
| 10 to 15 years | 32/35 (91%) | N = 32 | 2.25 (1–40) | 3/4 (75%) | N = 3 | 6 (1–7) | 35/39 (90%) | N = 35 | 2.5 (1–40) |
| 15 to 20 years | 15/20 (75%) | N = 15 | 5 (1–20) | 2/2 (100%) | N = 2 | 8 (1–15) | 17/22 (77%) | N = 17 | 5 (1–20) |
| Over 20 years | 12/13 (92%) | N = 12 | 6.5 (1–28) | 0/1 (0%) | N/A | 12/14 (86%) | N = 12 | 6.5 (1–28) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ta, D.; Downs, J.; Baynam, G.; Wilson, A.; Richmond, P.; Leonard, H. Medical Comorbidities in MECP2 Duplication Syndrome: Results from the International MECP2 Duplication Database. Children 2022, 9, 633. https://doi.org/10.3390/children9050633
Ta D, Downs J, Baynam G, Wilson A, Richmond P, Leonard H. Medical Comorbidities in MECP2 Duplication Syndrome: Results from the International MECP2 Duplication Database. Children. 2022; 9(5):633. https://doi.org/10.3390/children9050633
Chicago/Turabian StyleTa, Daniel, Jenny Downs, Gareth Baynam, Andrew Wilson, Peter Richmond, and Helen Leonard. 2022. "Medical Comorbidities in MECP2 Duplication Syndrome: Results from the International MECP2 Duplication Database" Children 9, no. 5: 633. https://doi.org/10.3390/children9050633