
Hypnosis and Sedation for Anxious Children Undergoing Dental Treatment: A Retrospective Practice-Based Longitudinal Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection of Participants
2.2. Medical History
2.3. Recording of Findings and Treatment Planning
2.4. Preparatory Measures
2.5. Treatment Goal and Treatment
2.6. Evaluation of the Videos
2.7. Statistics
3. Results
3.1. Behavior before and during Treatment
3.2. Self-Assessment of the Children
4. Discussion
4.1. Behavior of the Children during the Treatment
4.2. Self-Assessment of the Children
4.3. Accompanying Measures through Behavioral Guidance and Hypnotic Techniques
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cianetti, S.; Lombardo, G.; Lupatelli, E.; Pagano, S.; Abraha, I.; Montedori, A.; Caruso, S.; Gatto, R.; De Giorgio, S.; Salvato, R. Dental fear/anxiety among children and adolescents. A systematic review. Eur. J. Paediatr. Dent. 2017, 18, 121–130. [Google Scholar]
- Klaassen, M.; Veerkamp, J.; Hoogstraten, J. Changes in children’s dental fear: A longitudinal study. Eur. Arch. Paediatr. Dent. 2008, 9 (Suppl. S1), 29–35. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, A.; Broberg, L.; Bodin, U.; Berggren, K.; Arnrup, K. Dental behaviour management problems: The role of child personal characteristics. Int. J. Paediatr. Dent. 2010, 20, 242–253. [Google Scholar] [CrossRef] [PubMed]
- Klingberg, G.; Berggren, U.; Carlsson, S.G.; Norén, J.G. Child dental fear: Cause-related factors and clinical effects. Eur. J. Oral Sci. 1995, 103, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Ten Berge, M.; Veerkamp, J.S.; Hoogstraten, J.; Prins, P.J. Behavioural and emotional problems in children referred to a centre for special dental care. Community Dent. Oral Epidemiol. 1999, 27, 181–186. [Google Scholar] [CrossRef]
- Klaassen, M.; Veerkamp, J.; Hoogstraten, J. Predicting dental anxiety: The clinical value of anxiety questionnaires: An explorative study. Eur. J. Paediatr. Dent. 2003, 4, 171–176. [Google Scholar] [PubMed]
- Splieth, C.H.; Bünger, B.; Pine, C. Barriers for dental treatment of primary teeth in East and West Germany. Int. J. Paediatr. Dent. 2009, 19, 84–90. [Google Scholar] [CrossRef]
- Davis, D.M.; Fadavi, S.; Kaste, L.M.; Vergotine, R.; Rada, R. Acceptance and use of protective stabilization devices by pediatric dentistry diplomates in the United States. J. Dent. Child. (Chic.) 2016, 83, 60–66. [Google Scholar]
- Hallonsten, A.-L.; Jensen, B.; Raadal, M.; Veerkamp, J.S.J.; Hosey, M.T.; Poulsen, S. EAPD Guidelines on Sedation in Paediatric Dentistry. 2003, pp. 1–11. Available online: https://www.eapd.eu/uploads/5CF03741_file.pdf (accessed on 11 March 2022).
- Chen, X.; Jin, S.F.; Liu, H.B. Survey of parental acceptance rate to behavior management techniques used in pediatric dentistry. Shanghai Kou Qiang Yi Xue 2008, 17, 475–478. [Google Scholar]
- Armfield, J.M.; Heaton, L.J. Management of fear and anxiety in the dental clinic: A review. Aust. Dent. J. 2013, 58, 390–407. [Google Scholar] [CrossRef]
- Balian, A.; Cirio, S.; Salerno, C.; Wolf, T.G.; Campus, G.; Cagetti, M.G. Is visual pedagogy effective in improving cooperation towards oral hygiene and dental care in children with autism spectrum disorder? A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2021, 18, 789. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Cameron, E.; Forbes, G.; Humphris, G. Systematic review of dental staff behaviour on child dental patient anxiety and behavior. Patient Educ. Couns. 2011, 85, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Kuttner, L. Pediatric hypnosis: Treatment that adds and rarely subtracts. Int. J. Clin. Exp. Hypn. 2020, 68, 16–28. [Google Scholar] [CrossRef]
- Elkins, G.R.; Barabasz, A.F.; Council, J.R.; Spiegel, D. Advancing research and practice: The revised APA Division 30 definition of hypnosis. Int. J. Clin. Exp. Hypn. 2015, 63, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Huet, A.; Lucas-Polomeni, M.M.; Robert, J.C.; Sixou, J.L.; Wodey, E. Hypnosis and dental anesthesia in children: A prospective controlled study. Int. J. Clin. Exp. Hypn. 2011, 59, 424–440. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Carrasco, A.; Butrón-Téllez Girón, C.; Sanchez-Armass, O.; Pierdant-Pérez, M. Effectiveness of hypnosis in combination with conventional techniques of behavior management in anxiety/pain reduction during dental anesthetic infiltration. Pain Res. Manag. 2017, 2017, 1434015. [Google Scholar] [CrossRef]
- Wilson, S.; Alcaino, E.A. Survey on sedation in paediat.tric dentistry: A global perspective. Int. J. Paediatr. Dent. 2011, 21, 321–332. [Google Scholar] [CrossRef]
- Zanette, G.; Manani, G.; Favero, L.; Stellini, E.; Mazzoleni, S.; Cocilovo, F.; Modolo, O.; Ferrarese, N.; Facco, E. Conscious sedation with diazepam and midazolam for dental patient: Priority to diazepam. Minerva Stomatol. 2013, 62, 355–374. [Google Scholar]
- Huijboom-Tan, H.L.; Verkamp, J.S.J.; ten Berge, M. Prediction of dental behavior problems in preschool children. Ned. Tijdschr. Tandheelkd. 2003, 110, 195–199. [Google Scholar]
- Jing, Q.; Wan, K.; Ma, L.; Chen, X.; Tong, Y.L. Evaluation of oral midazolam conscious sedation in different age groups in pediatric dentistry. Zhonghua Kou Qiang Yi Xue Za Zhi 2010, 45, 770–772. [Google Scholar]
- Somri, M.; Parisinos, C.A.; Kharouba, J.; Cherni, N.; Smidt, A.; Abu Ras, Z.; Darawshi, G.; Gaitini, L.A. Optimising the dose of oral midazolam sedation for dental procedures in children: A prospective, randomised and controlled study. Int. J. Paediatr. Dent. 2012, 22, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Ashley, P.F.; Chaudhary, M.; Lourenço-Matharu, L. Sedation of children undergoing dental treatment. Cochrane Database Syst. Rev. 2018, 12, CD003877. [Google Scholar] [CrossRef] [Green Version]
- Day, P.F.; Power, A.M.; Hibbert, S.A.; Paterson, S.A. Effectiveness of oral midazolam for paediatric dental care: A retrospective study in two specialist centres. Eur. Arch. Paediatr. Dent. 2006, 7, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Venham, L.L.; Bengston, D.; Cipes, M. Children’s response to sequential dental visists. J. Dent. Res. 1977, 56, 545–559. [Google Scholar] [CrossRef] [PubMed]
- Cravero, J.P.; Fanciullo, G.J.; McHugo, G.J.; Baird, J.C. The validity of the Computer Face Scale for measuring pediatric pain and mood. Paediatr. Anaesth. 2013, 23, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Veerkamp, J.S.; Gruythuysen, R.J.; van Amerongen, W.E.; Hoogstraten, J. Dental treatment of fearful children using nitrous oxide. Part 3: Anxiety during sequential visits. ASDC J. Dent. Child. 1993, 60, 175–182. [Google Scholar] [PubMed]
- Santamaria, R.M.; Innes, N.P.T.; Machiulskiene, V.; Evans, D.J.P.; Alkilzy, M.; Splieth, C.H. Acceptability of different caries management methods for primary molars in a RCT. Int. J. Paediatr. Dent. 2015, 25, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Schwendicke, F.; Krois, J.; Splieth, C.H.; Innes, N.; Robertson, M.; Schmoeckel, J.; Santamaria, R.M. Cost-effectiveness of managing cavitated primary molar caries lesions: A randomized trial in Germany. J. Dent. 2018, 78, 40–45. [Google Scholar] [CrossRef] [Green Version]
- Kossak, H.C.; Zehner, G. Hypnose beim Kinder-Zahnarzt. Verhaltensführung und Kommunikation; Springer: Berlin, Germany, 2011. [Google Scholar]
- Schmierer, A.; Lee Butz, C.; Schoderböck, R. Kinderhypnose in der Zahnmedizin; Hypnos Verlag: Stuttgart, Germany, 2002. [Google Scholar]
- Fleiss, J.L. The Design and Analysis of Clinical Experiments; John Wiley & Sons: New York, NY, USA, 1986; p. 62. [Google Scholar]
- Afshar, H.; Baradaran Nakhjavani, Y.; Mahmoudi-Gharaei, J.; Paryab, M.; Zadhoosh, S. The effect of parental presence on the 5 year-old children’s anxiety and cooperative behavior in the first and second dental visit. Iran. J. Pediatr 2011, 21, 193–200. [Google Scholar]
- Kapur, A.; Chawla, H.S.; Gauba, K.; Goyal, A.; Bhardwaj, N. Effect of oral-transmucosal midazolam sedation on anxiety levels of 3–4 years old children during a Class II restorative procedure. Contemp. Clin. Dent. 2014, 5, 334–339. [Google Scholar] [CrossRef]
- Kain, Z.N.; Hofstadter, M.B.; Mayes, L.C.; Krivutza, D.M.; Alexander, G.; Wang, S.M.; Reznick, J.S. Midazolam: Effects on amnesia and anxiety in children. Anesthesiology 2000, 93, 676–684. [Google Scholar] [CrossRef]
- Millar, K.; Asbury, A.J.; Bowman, A.W.; Hosey, M.T.; Martin, K.; Musiello, T.; Welbury, R.R. A randomised placebo-controlled trial of the effects of midazolam premedication on children’s postoperative cognition. Anaesthesia 2007, 62, 923–930. [Google Scholar] [CrossRef]
- Hembrecht, E.J.; Nieuwenhuizen, J.; Aartman, I.H.; Krikken, J.K.; Veerkamp, J.S.J. Pain-related behaviour in children: A randomised study during two sequential dental visits. Eur. Arch. Paediatr. Dent. 2013, 14, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Nainar, S.M.; Crall, J.J. Child patient behavior: A new perspective. ASDC J. Dent. Child. 1991, 58, 303–305. [Google Scholar] [PubMed]
- Anand, K.J.; Clark, A.E.; Willson, D.F.; Berger, J.; Meert, K.L.; Zimmerman, J.J.; Harrison, R.; Carcillo, J.A.; Newth, C.J.; Bisping, S.; et al. Opioid analgesia in mechanically ventilated children: Results from the multicenter Measuring Opioid Tolerance Induced by Fentanyl study. Pediatr. Crit. Care Med. 2013, 14, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Touitou, Y. Sleep disorders and hypnotic agents: Medical, social and economical impact. Ann. Pharm. Fr. 2007, 65, 230–238. [Google Scholar] [CrossRef]
- Ratson, T.; Peretz, B. Ranking of dental and somatic pain sensations among paediatric dental patients. Int. J. Paediatr. Dent. 2013, 23, 259. [Google Scholar] [CrossRef]
- Tomlinson, D.; von Baeyer, C.L.; Stinson, J.N.; Sung, L. A systematic review of faces scales for the self-report of pain intensity in children. Pediatrics 2010, 126, e1168–e1198. [Google Scholar] [CrossRef] [Green Version]
- Garra, G.; Singer, A.J.; Domingo, A.; Thode, H.C. The Wong-Baker pain FACES scale measures pain, not fear. Pediatr. Emerg. Care 2013, 29, 17–20. [Google Scholar] [CrossRef]
- Virdee, P.K.; Rodd, H.D. Who accompanies children to a dental hospital appointment? Eur. Arch. Paediatr. Dent. 2007, 8, 95–98. [Google Scholar] [CrossRef]
- Roberts, J.F.; Curzon, M.E.; Koch, G.; Martens, L.C. Review: Behaviour management techniques in paediatric dentistry. Eur. Arch. Paediatr. Dent. 2010, 11, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Peretz, B.; Glaicher, H.; Ram, D. Child-management techniques. Are there differences in the way female and male pediatric dentists in Israel practice? Braz. Dent. J. 2003, 14, 82–86. [Google Scholar] [CrossRef] [Green Version]
- Strøm, K.; Rønneberg, A.; Skaare, A.B.; Espelid, I.; Willumsen, T. Dentists’ use of behavioural management techniques and their attitudes towards treating paediatric patients with dental anxiety. Eur. Arch. Paediatr. Dent. 2015, 16, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Kebriaee, F.; Sarraf Shirazi, A.; Fani, K.; Moharreri, F.; Soltanifar, A.; Khaksar, Y.; Mazhari, F. Comparison of the effects of cognitive behavioural therapy and inhalation sedation on child dental anxiety. Eur. Arch. Paediatr. Dent. 2015, 16, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Luis de León, J.; Guinot Jimeno, F.; Bellet Dalmau, L.J. Acceptance by Spanish parents of behaviour-management techniques used in paediatric dentistry. Eur. Arch. Paediatr. Dent. 2010, 11, 175–178. [Google Scholar] [CrossRef]
- Crossley, M.L.; Joshi, G. An investigation of paediatric dentists’ attitudes towards parental accompaniment and behavioural management techniques in the UK. Br. Dent. J. 2002, 192, 517–521. [Google Scholar] [CrossRef]
- Abushal, M.S.; Adenubi, J.O. Attitudes of Saudi parents toward behavior management techniques in pediatric dentistry. J. Dent. Child. (Chic.) 2003, 70, 104–110. [Google Scholar]
- Davies, E.B.; Buchanan, H. An exploratory study investigating children’s perceptions of dental behavioural management techniques. Int. J. Paediatr. Dent. 2013, 23, 297–309. [Google Scholar] [CrossRef]
- Al-Harasi, S.; Ashley, P.F.; Moles, D.R.; Parekh, S.; Walters, V. Hypnosis for children undergoing dental treatment. Cochrane Database Syst. Rev. 2010, 4, CD007154. [Google Scholar]
- Peretz, B.; Bercovich, R.; Blumer, S. Using elements of hypnosis prior to or during pediatric dental treatment. Pediatr. Dent. 2013, 35, 33–36. [Google Scholar]
- Peretz, B.; Bimstein, E. The use of imagery suggestions during administration of local anesthetic in pediatric dental patients. ASDC J. Dent. Child. 2000, 67, 263–267. [Google Scholar] [PubMed]
- Gokli, M.A.; Wood, A.J.; Mourino, A.P.; Farrington, F.H.; Best, A.M. Hypnosis as an adjunct to the administration of local anesthetic in pediatric patients. ASDC J. Dent. Child. 1994, 61, 272–275. [Google Scholar] [PubMed]
- Peretz, B. Confusion as a technique to induce hypnosis in a severely anxious pediatric dental patient. J. Clin. Pediatr. Dent. 1996, 21, 27–30. [Google Scholar] [PubMed]
- Bell, S.M.; Ainsworth, M.D. Infant crying and maternal responsiveness. Child. Dev. 1972, 43, 1171–1190. [Google Scholar] [CrossRef] [PubMed]
- Guéguen, N.; Meineri, S.; Charles-Sire, V. Improving medication adherence by using practitioner nonverbal techniques: A field experiment on the effect of touch. J. Behav. Med. 2010, 33, 466–473. [Google Scholar] [CrossRef] [PubMed]
- Schoderböck, R. Wie kann man das Bewusstsein von Kindern ohne Medikamente beeinflussen? Dent. Trib. Austria 2006, 7, 3–11. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Code | Treatment | 1st Session | 2nd Session | 3rd Session |
|---|---|---|---|---|
| n Children (%) | n Children (%) | n Children (%) | ||
| 0 | No treatment | 17 (5.5) | 4 (3.9) | 0 (0.0) |
| 1 | Restoration/strip crown without anesthesia | 38 (12.2) | 6 (5.8) | 0 (0.0) |
| 2 | Restoration and/or strip crown with anesthesia | 36 (11.6) | 20 (19.4) | 5 (20.0) |
| 3 | Extraction | 62 (19.8) | 14 (13.6) | 4 (16.0) |
| 4 | Extraction and restoration | 38 (12.2) | 10 (9.7) | 3 (12.0) |
| 5 | Steel crown with pulpotomy or root treatment | 81 (26.0) | 40 (38.8) | 8 (32.0) |
| 6 | Pulpotomy or root canal treatment without steel crown | 13 (4.2) | 1 (1.0) | 2 (8.0) |
| 7 | Extraction and steel crown with pulpotomy | 9 (2.9) | 2 (1.9) | 0 (0.0) |
| 8 | Miscellaneous | 4 (1.3) | 0 (0.0) | 0 (0.0) |
| 9 | Steel crown | 13 (4.2) | 6 (5.8) | 3 (12.0) |
| Total treatments | 311 (100.0) | 103 (100.0) | 25 (100.0) |
| Session | Mother | Father | Both Parents | Others |
|---|---|---|---|---|
| Treatments | n Children (%) | n Children (%) | n Children (%) | n Children (%) |
| 1st session | 209 (69.0) | 50 (76.9) | 47 (73.4) | 3 (60.0) |
| 2nd session | 75 (24.7) | 14 (21.5) | 12 (18.8) | 2 (40.0) |
| 3rd session | 19 (6.3) | 1 (1.6) | 5 (7.8) | 0 (0.0) |
| Total treatments | 303 (100.0) | 65 (100.0) | 64 (100.0) | 5 (100.0) |
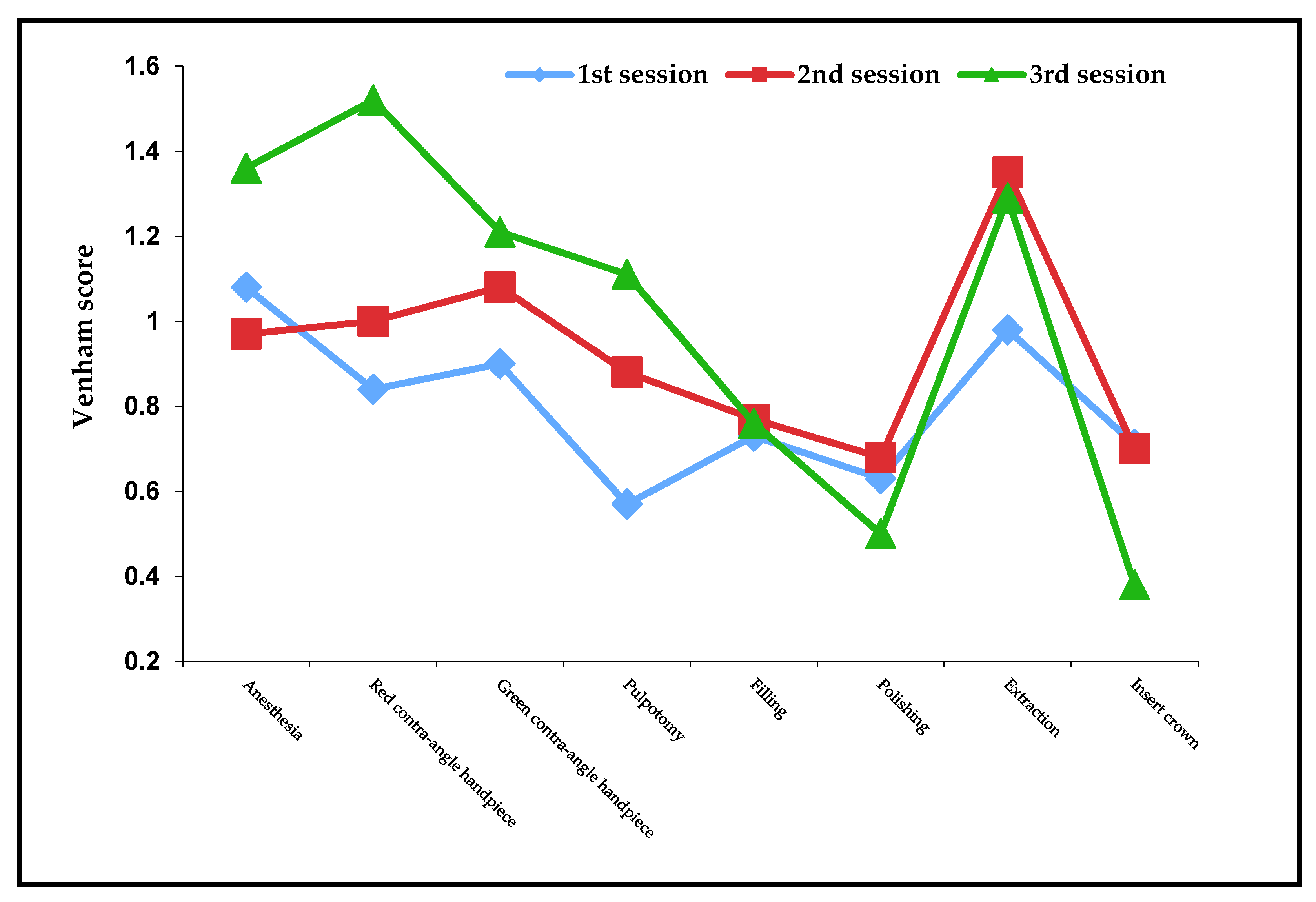
| (Mean/±SD) | 1st Session | 2nd Session | 3rd Session | p-Value * |
|---|---|---|---|---|
| Juice | 0.49 ± 1.18 | 0.47 ± 1.23 | 0.05 ± 0.35 | NS/0.02 |
| Before treatment | 0.23 ± 0.89 | 0.35 ± 0.91 | 0.24 ± 0.66 | 0.03/0.03 |
| Anesthesia | 1.08 ± 1.44 | 0.96 ± 1.34 | 1.36 ± 1.38 | NS/0.04 |
| Treatment | 0.99 ± 1.41 | 1.17 ± 1.39 | 1.27 ± 1.20 | NS/NS |
| End of treatment | 0.44 ± 1.10 | 0.44 ± 0.91 | 0.01 ± 0.14 | NS/<0.01 |
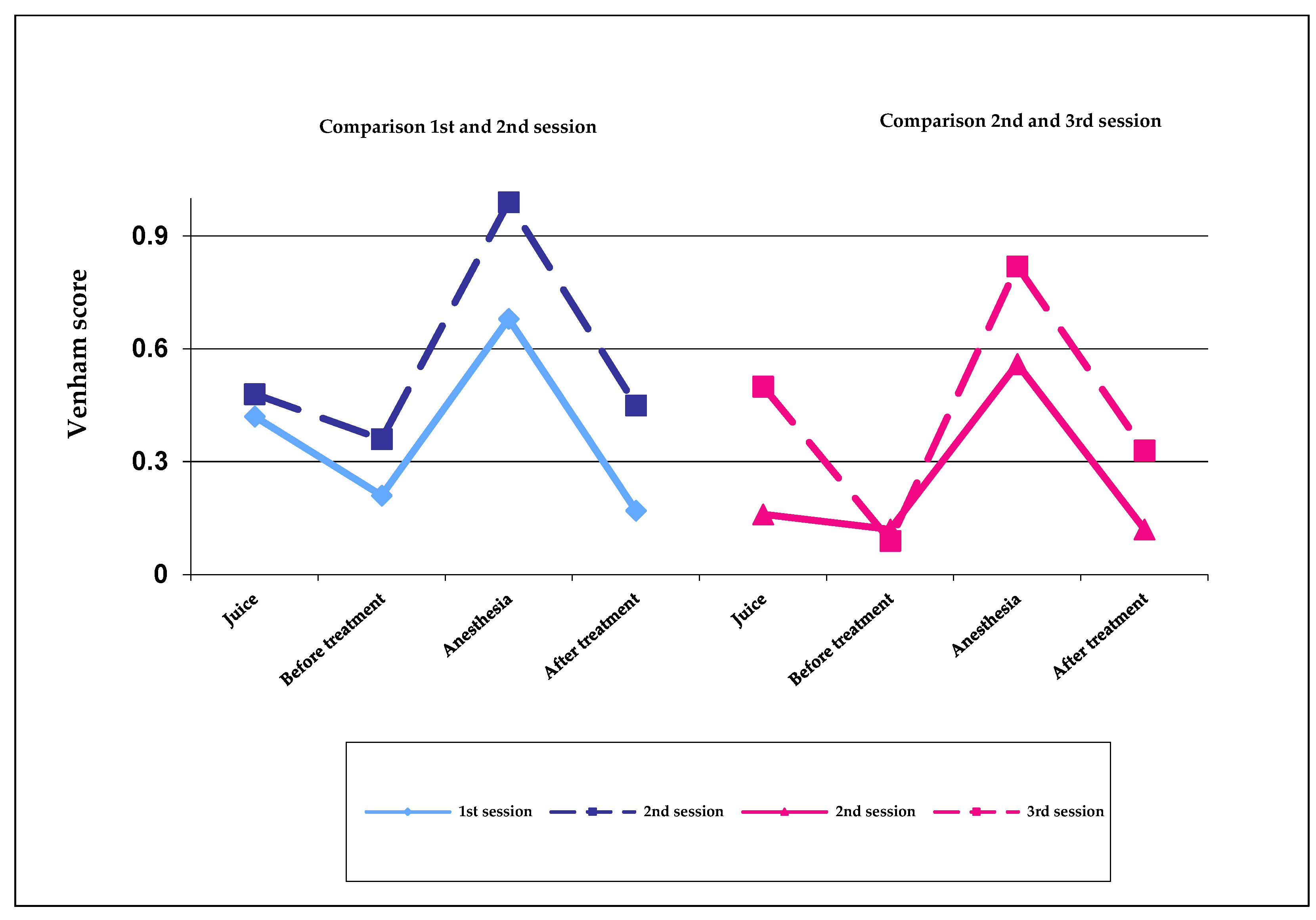
| 1st Session | 2nd Session | p-Value | |
|---|---|---|---|
| Juice | 0.42 ± 1.12 | 0.48 ± 1.25 | NS |
| Before treatment | 0.21 ± 0.89 | 0.36 ± 0.93 | NS |
| Anesthesia | 0.68 ± 1.17 | 0.99 ± 1.37 | 0.04 |
| After treatment | 1.17 ± 0.59 | 0.45 ± 0.92 | <0.01 |
| 2nd Session | 3rd Session | p-Value | |
|---|---|---|---|
| Juice | 0.16 ± 0.47 | 0.50 ± 1.41 | 0.01 |
| Before treatment | 0.12 ± 0.60 | 0.09 ± 0.29 | NS |
| Anesthesia | 0.56 ± 0.92 | 0.82 ± 1.26 | NS |
| After treatment | 0.12 ± 0.44 | 0.33 ± 0.76 | 0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rienhoff, S.; Splieth, C.H.; Veerkamp, J.S.J.; Rienhoff, J.; Krikken, J.B.; Campus, G.; Wolf, T.G. Hypnosis and Sedation for Anxious Children Undergoing Dental Treatment: A Retrospective Practice-Based Longitudinal Study. Children 2022, 9, 611. https://doi.org/10.3390/children9050611
Rienhoff S, Splieth CH, Veerkamp JSJ, Rienhoff J, Krikken JB, Campus G, Wolf TG. Hypnosis and Sedation for Anxious Children Undergoing Dental Treatment: A Retrospective Practice-Based Longitudinal Study. Children. 2022; 9(5):611. https://doi.org/10.3390/children9050611
Chicago/Turabian StyleRienhoff, Sabine, Christian H. Splieth, Jacobus S. J. Veerkamp, Jan Rienhoff, Janneke B. Krikken, Guglielmo Campus, and Thomas Gerhard Wolf. 2022. "Hypnosis and Sedation for Anxious Children Undergoing Dental Treatment: A Retrospective Practice-Based Longitudinal Study" Children 9, no. 5: 611. https://doi.org/10.3390/children9050611