
COVID-19 Related Information on Pediatric Dental Care including the Use of Teledentistry: A Narrative Review
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Pediatric Oral and Dental Care and the COVID-19 Pandemic
3.1.1. Changes in Pediatric Oral and Dental Care during the First Peak of the COVID-19 Pandemic
3.1.2. Pediatric Oral and Dental Care Provision during the Further Waves of the COVID-19 Pandemic
3.1.3. Pediatric Dentistry Practice: Infection Control, Ergonomics, and Pedodontics Patient Management
In-Office Procedures
Home Care Prescriptions and Recommendations
3.2. Dental Caries in Pediatric Subjects during the COVID-19 Pandemic
3.2.1. Nutrition
3.2.2. Oral Hygiene
3.2.3. Fluoroprophylaxis
3.3. TMD Disorders and Oral Bad Habits
3.4. Pediatric Oral and Dental Care: Lessons Learned from COVID-19 and Future Applications in Pedodontics
3.4.1. Pediatric Dentistry Practice during and after the COVID-19 Era
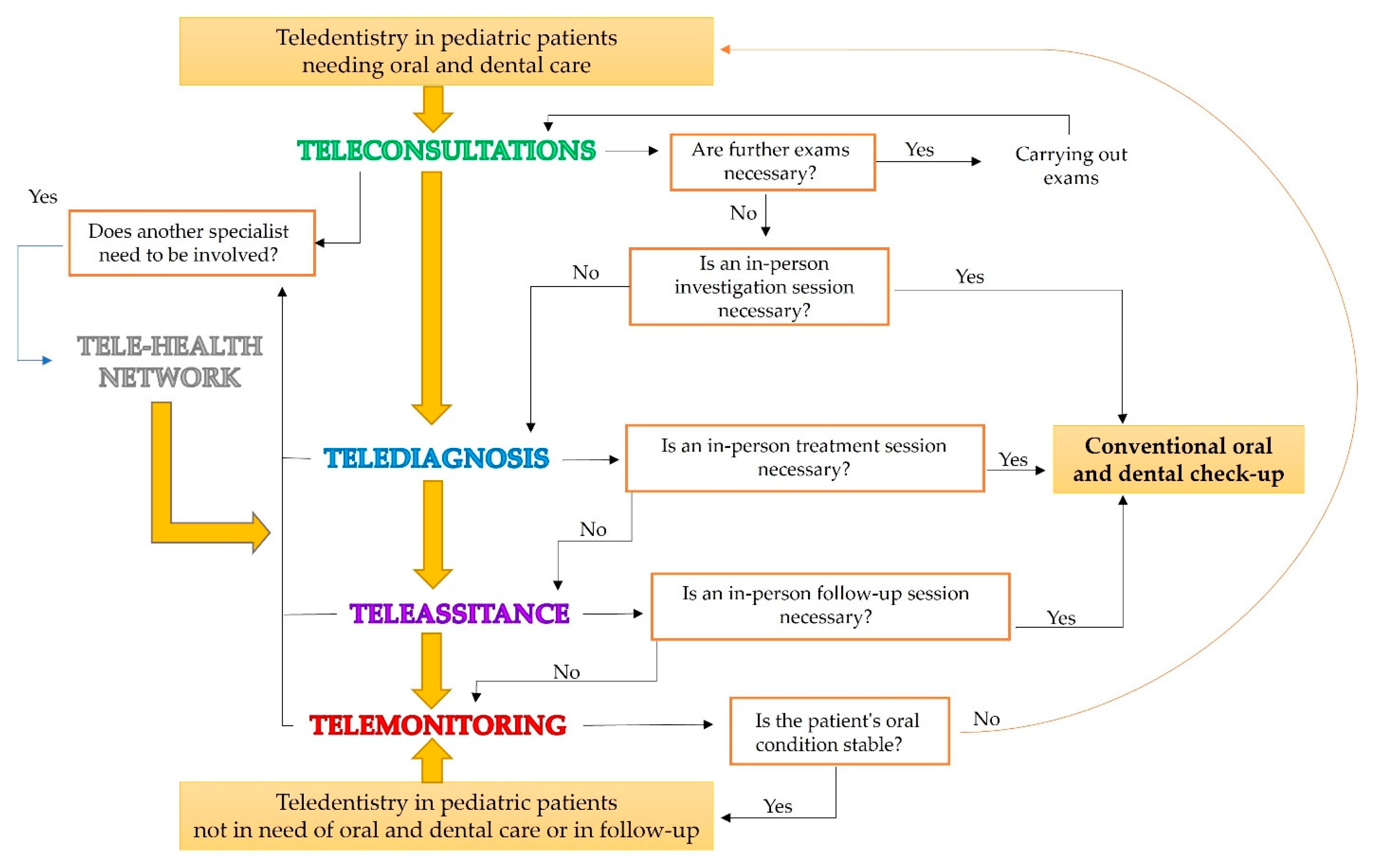
3.4.2. Teledentistry
Teleconsultations in Pediatric Dentistry
Telediagnosis in Pediatric Dentistry
Telescreening in Pediatric Dentistry
Teleassistance and Telemonitoring in Pediatric Dentistry
Telehealth Networks in Pediatric Dentistry
Tele-Education and Pediatric Dentistry
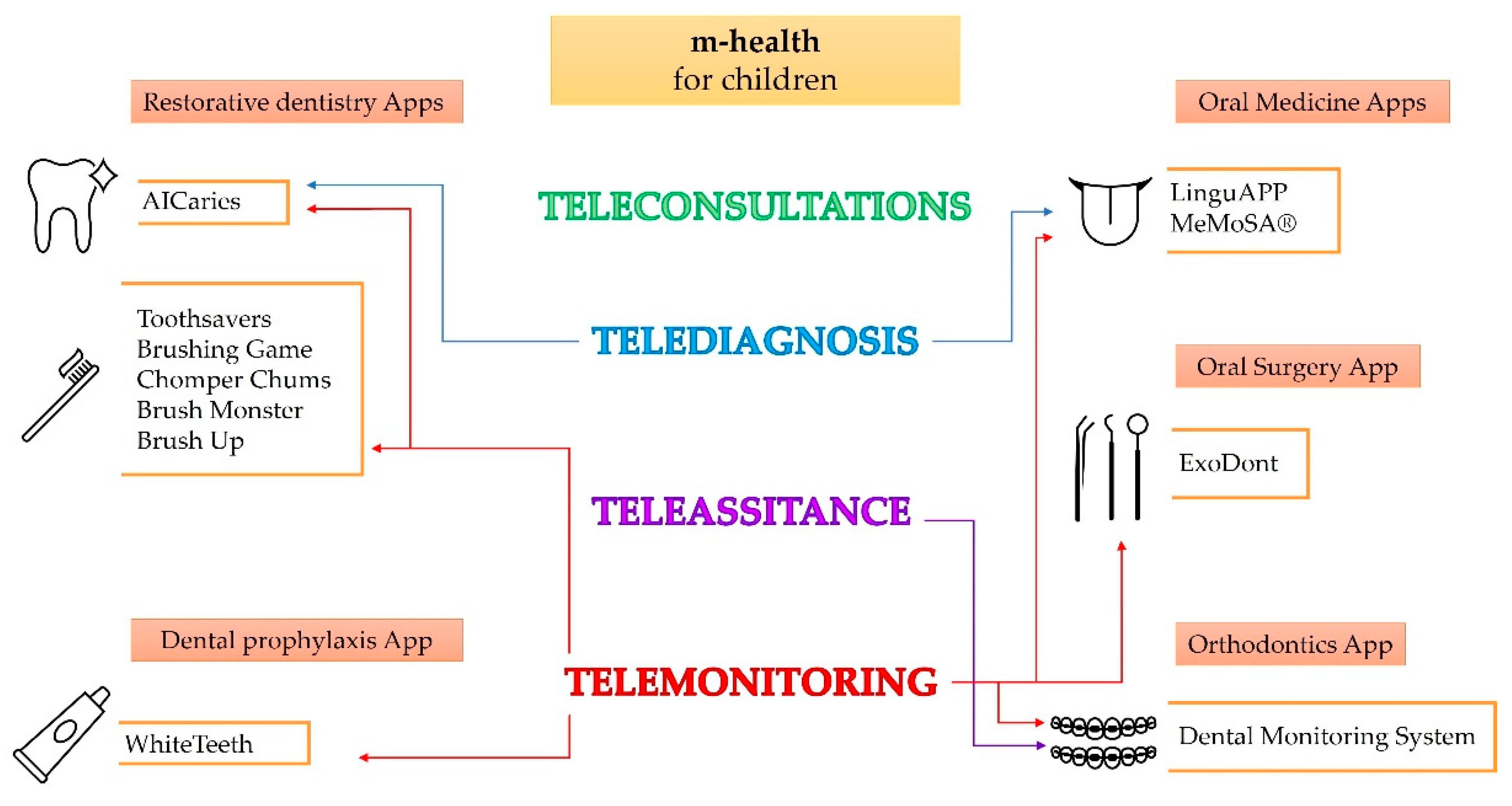
3.4.3. Mobile Health (m-Health)
Restorative Dentistry Apps
Dental Prophylaxis App
Oral Medicine Apps
Oral Surgery App
Orthodontics App
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Luzzi, V.; Ierardo, G.; Bossù, M.; Polimeni, A. Paediatric Oral Health during and after the COVID-19 Pandemic. Int. J. Paediatr. Dent. 2021, 31, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Fazio, M.; Lombardo, C.; Marino, G.; Marya, A.; Messina, P.; Scardina, G.A.; Tocco, A.; Torregrossa, F.; Valenti, C. Lingu APP: An m-Health Application for Teledentistry Diagnostics. Int. J. Environ. Res. Public Health 2022, 19, 822. [Google Scholar] [CrossRef] [PubMed]
- Amato, A.; Caggiano, M.; Amato, M.; Moccia, G.; Capunzo, M.; de Caro, F. Infection Control in Dental Practice during the Covid-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 4769. [Google Scholar] [CrossRef] [PubMed]
- Al-Halabi, M.; Salami, A.; Alnuaimi, E.; Kowash, M.; Hussein, I. Assessment of Paediatric Dental Guidelines and Caries Management Alternatives in the Post COVID-19 Period. A Critical Review and Clinical Recommendations. Eur. Arch. Paediatr. Dent. 2020, 21, 543–556. [Google Scholar] [CrossRef]
- American Dental Association. ADA Interim Guidance for Management of Emergency and Urgent Dental Care. Available online: Https://Www.Ada.Org (accessed on 30 April 2020).
- Pendyala, G.S.; Joshi, S.R.; Kale, P.; Phadnis, M.V.; Mopagar, V.P. Paediatric Dental Care in COVID-19 Pandemic—Time to Rethink—A Review. J. Evol. Med. Dent. Sci. 2021, 10, 546–549. [Google Scholar] [CrossRef]
- di Spirito, F.; Iacono, V.J.; Alfredo, I.; Alessandra, A.; Sbordone, L.; Lanza, A. Evidence-Based Recommendations on Periodontal Practice and the Management of Periodontal Patients during and after the COVID-19 Era: Challenging Infectious Diseases Spread by Airborne Transmission. Open Dent. J. 2021, 15, 325–336. [Google Scholar] [CrossRef]
- Nuvvula, S.; Mallineni, S. Remote Management of Dental Problems in Children during and Post the COVID-19 Pandemic Outbreak: A Teledentistry Approach. Dent. Med. Probl. 2021, 58, 237–241. [Google Scholar] [CrossRef]
- Fleagle, J.; Xiao, W.; Cottam, M.; Lorch, M. Oral Complaint Visits to the Pediatric Emergency Department during the COVID-19 Pandemic. Cureus 2022, 14, e28559. [Google Scholar] [CrossRef]
- Carmagnola, D.; Toma, M.; Henin, D.; Perrotta, M.; Gianolio, L.; Colombo, A.; Dellavia, C. Dental Emergencies in an Italian Pediatric Hospital during the COVID-19 Pandemic. Healthcare 2022, 10, 537. [Google Scholar] [CrossRef]
- Samuel, S.R.; Mathew, M.G.; Suresh, S.G.; Varma, S.R.; Elsubeihi, E.S.; Arshad, F.; Elkareimi, Y.; Elsahn, N.A.; Khalil, E. Pediatric Dental Emergency Management and Parental Treatment Preferences during COVID-19 Pandemic as Compared to 2019. Saudi J. Biol. Sci. 2021, 28, 2591–2597. [Google Scholar] [CrossRef]
- Olszewska, A.; Paszynska, E.; Roszak, M.; Czajka-Jakubowska, A. Management of the Oral Health of Children during the COVID-19 Pandemic in Poland. Front. Public Health 2021, 9, 1049. [Google Scholar] [CrossRef] [PubMed]
- Nikolopoulou, G.B.; Maltezou, H.C. COVID-19 in Children: Where Do We Stand? Arch. Med. Res. 2022, 53, 1–8. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Vaccine Tracker European Centre for Disease Prevention and Control (Europa.Eu). Available online: Https://Www.EcDc.Europa.Eu/En/Publications-Data/Covid-19-Vaccine-Tracker (accessed on 2 September 2022).
- Nakra, N.; Blumberg, D.; Herrera-Guerra, A.; Lakshminrusimha, S. Multi-System Inflammatory Syndrome in Children (MIS-C) following SARS-CoV-2 Infection: Review of Clinical Presentation, Hypothetical Pathogenesis, and Proposed Management. Children 2020, 7, 69. [Google Scholar] [CrossRef] [PubMed]
- di Spirito, F.; Pelella, S.; Argentino, S.; Sisalli, L.; Sbordone, L. Oral Manifestations and the Role of the Oral Healthcare Workers in COVID-19. Oral Dis. 2022, 28, 1003–1004. [Google Scholar] [CrossRef] [PubMed]
- Kalyoncu, I.; Özcan, G.; Kargül, B. Oral Health Practice and Health-Related Quality of Life of a Group of Children during the Early Stage of the COVID.19 Pandemic in Istanbul. J. Educ. Health Promot. 2021, 10, 313. [Google Scholar] [CrossRef] [PubMed]
- Martina, S.; Amato, A.; Rongo, R.; Caggiano, M.; Amato, M. The Perception of COVID-19 among Italian Dentists: An Orthodontic Point of View. Int. J. Environ. Res. Public Health 2020, 17, 4384. [Google Scholar] [CrossRef]
- Amato, A.; Ciacci, C.; Martina, S.; Caggiano, M.; Amato, M. COVID-19: The Dentists’ Perceived Impact on the Dental Practice. Eur. J. Dent. 2021, 15, 469–474. [Google Scholar] [CrossRef]
- Prati, C.; Pelliccioni, G.A.; Sambri, V.; Chersoni, S.; Gandolfi, M.G. COVID-19: Its Impact on Dental Schools in Italy, Clinical Problems in Endodontic Therapy and General Considerations. Int. Endod J. 2020, 53, 723–725. [Google Scholar] [CrossRef] [Green Version]
- Schulz-Weidner, N.; Schlenz, M.A.; Krämer, N.; Boukhobza, S.; Bekes, K. Impact and Perspectives of Pediatric Dental Care during the COVID-19 Pandemic Regarding Unvaccinated Children: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2021, 18, 12117. [Google Scholar] [CrossRef]
- di Spirito, F.; Caggiano, M.; di Palo, M.P.; Contaldo, M.; D’Ambrosio, F.; Martina, S.; Amato, A. Oral Lesions in Pediatric Subjects: SARS-CoV-2 Infection and COVID-19 Vaccination. Appl. Sci. 2022, 12, 8995. [Google Scholar] [CrossRef]
- Yang, J.; Yang, G.; Jin, R.; Song, G.; Yuan, G. Changes in Paediatric Dental Clinic after Reopening during COVID-19 Pandemic in Wuhan: A Retrospective Study. BMJ Open 2022, 12, e048430. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.; Nkenke, E. Approaches to the Management of Patients in Oral and Maxillofacial Surgery during COVID-19 Pandemic. J. Cranio-Maxillofac. Surg. 2020, 48, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Sales, S.C.; Meyfarth, S.; Scarparo, A. The Clinical Practice of Pediatric Dentistry Post-COVID-19: The Current Evidences. Pediatr. Dent. J. 2021, 31, 25–32. [Google Scholar] [CrossRef] [PubMed]
- BaniHani, A.; Gardener, C.; Raggio, D.P.; Santamaría, R.M.; Albadri, S. Could COVID-19 Change the Way We Manage Caries in Primary Teeth? Current Implications on Paediatric Dentistry. Int. J. Paediatr. Dent. 2020, 30, 523–525. [Google Scholar] [CrossRef]
- United States Department of Labor. Hazard Recognition, Control and Prevention. Dentistry. Occupational Safety and Health Administration. Available online: Https://Www.Osha.Gov/Dentistry (accessed on 30 August 2022).
- Cavalcante-Leão, B.L.; de Araujo, C.; Basso, I.; Schroder, A.; Guariza-Filho, O.; Ravazzi, G.; Gonçalves, F.; Zeigelboim, B.; Santos, R.; Stechman-Neto, J. Is There Scientific Evidence of the Mouthwashes Effectiveness in Reducing Viral Load in Covid-19? A Systematic Review. J. Clin. Exp. Dent. 2021, 13, e179–e189. [Google Scholar] [CrossRef]
- Paglia, L. COVID-19 and Paediatric Dentistry after the Lockdown. Eur. J. Paediatr. Dent. 2020, 21, 89. [Google Scholar] [CrossRef]
- Meng, L.; Hua, F.; Bian, Z. Coronavirus Disease 2019 (COVID-19): Emerging and Future Challenges for Dental and Oral Medicine. J. Dent. Res. 2020, 99, 481–487. [Google Scholar] [CrossRef] [Green Version]
- Goriuc, A.; Sandu, D.; Tatarciuc, M.; Luchian, I. The Impact of the COVID-19 Pandemic on Dentistry and Dental Education: A Narrative Review. Int. J. Environ. Res. Public Health 2022, 19, 2537. [Google Scholar] [CrossRef]
- Lyu, W.; Wehby, G.L. Effects of the COVID-19 Pandemic on Children’s Oral Health and Oral Health Care Use. J. Am. Dent. Assoc. 2022, 153, 787–796.e2. [Google Scholar] [CrossRef]
- Hotwani, K.; Lamba, G.; Nagpal, D.I.; Gunwal, M.K.; Chowdhari, P. Oral Healthcare Management of Children after COVID-19 Outbreak. Int. J. Clin. Pediatr. Dent. 2021, 14, 293–297. [Google Scholar] [CrossRef]
- al Makhmari, S.A.; Kaklamanos, E.G.; Athanasiou, A.E. Short-Term and Long-Term Effectiveness of Powered Toothbrushes in Promoting Periodontal Health during Orthodontic Treatment: A Systematic Review and Meta-Analysis. Am. J. Orthod. Dentofac. Orthop. 2017, 152, 753–766.e7. [Google Scholar] [CrossRef] [PubMed]
- Maru, V. The ‘New Normal’ in Post–COVID-19 Pediatric Dental Practice. Int. J. Paediatr. Dent. 2021, 31, 528–538. [Google Scholar] [CrossRef] [PubMed]
- ElShehaby, M.; Mofti, B.; Montasser, M.A.; Bearn, D. Powered vs. Manual Tooth Brushing in Patients with Fixed Orthodontic Appliances: A Systematic Review and Meta-Analysis. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 639–649. [Google Scholar] [CrossRef] [PubMed]
- Hussain, U.; Alam, S.; Rehman, K.; Antonoglou, G.N.; Papageorgiou, S.N. Effects of Chlorhexidine Use on Periodontal Health during Fixed Appliance Orthodontic Treatment: A Systematic Review and Meta-Analysis. Eur. J. Orthod. 2022. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulou, C.; Karamani, I.; Gkourtsogianni, S.; Seremidi, K.; Kloukos, D. A Systematic Review on the Effectiveness of Organic Unprocessed Products in Controlling Gingivitis in Patients Undergoing Orthodontic Treatment with Fixed Appliances. Clin. Exp. Dent. Res. 2021, 7, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Kommuri, K.; Michelogiannakis, D.; Barmak, B.A.; Rossouw, P.E.; Javed, F. Efficacy of Herbal- versus Chlorhexidine-based Mouthwashes towards Oral Hygiene Maintenance in Patients Undergoing Fixed Orthodontic Therapy: A Systematic Review and Meta-analysis. Int. J. Dent. Hyg. 2022, 20, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.; di Spirito, F.; D’Ambrosio, F.; Boccia, G.; Moccia, G.; de Caro, F. Probiotics in Periodontal and Peri-Implant Health Management: Biofilm Control, Dysbiosis Reversal, and Host Modulation. Microorganisms 2022, 10, 2289. [Google Scholar] [CrossRef]
- Lardani, L.; Derchi, G.; Marchio, V.; Carli, E. One-Year Clinical Performance of ActivaTM Bioactive-Restorative Composite in Primary Molars. Children 2022, 9, 433. [Google Scholar] [CrossRef]
- Maturo, P.; Costacurta, M.; Perugia, C.; Docimo, R. Fluoride Supplements in Pregnancy, Effectiveness in the Prevention of Dental Caries in a Group of Children. Oral Implantol. 2011, 4, 23–27. [Google Scholar]
- Scherrer, C.; Naavaal, S.; Lin, M.; Griffin, S.O. COVID-19 Pandemic Impact on US Childhood Caries and Potential Mitigation. J. Dent. Res. 2022, 101, 1147–1154. [Google Scholar] [CrossRef]
- Docimo, R.; Costacurta, M.; Gualtieri, P.; Pujia, A.; Leggeri, C.; Attinà, A.; Cinelli, G.; Giannattasio, S.; Rampello, T.; di Renzo, L. Cariogenic Risk and COVID-19 Lockdown in a Paediatric Population. Int. J. Environ. Res. Public Health 2021, 18, 7558. [Google Scholar] [CrossRef] [PubMed]
- Castañeda-Babarro, A.; Arbillaga-Etxarri, A.; Gutiérrez-Santamaría, B.; Coca, A. Physical Activity Change during COVID-19 Confinement. Int. J. Environ. Res. Public Health 2020, 17, 6878. [Google Scholar] [CrossRef] [PubMed]
- Jia, P.; Liu, L.; Xie, X.; Yuan, C.; Chen, H.; Guo, B.; Zhou, J.; Yang, S. Changes in Dietary Patterns among Youths in China during COVID-19 Epidemic: The COVID-19 Impact on Lifestyle Change Survey (COINLICS). Appetite 2021, 158, 105015. [Google Scholar] [CrossRef] [PubMed]
- Brondani, B.; Knorst, J.K.; Tomazoni, F.; Cósta, M.D.; Vargas, A.W.; Noronha, T.G.; Mendes, F.M.; Ardenghi, T.M. Effect of the COVID-19 Pandemic on Behavioural and Psychosocial Factors Related to Oral Health in Adolescents: A Cohort Study. Int. J. Paediatr. Dent. 2021, 31, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Ferrazzano, G.; Cantile, T.; Alcidi, B.; Coda, M.; Ingenito, A.; Zarrelli, A.; di Fabio, G.; Pollio, A. Is Stevia Rebaudiana Bertoni a Non Cariogenic Sweetener? A Review. Molecules 2015, 21, 38. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Oral Health. Available online: Https://Www.Who.Int/Health-Topics/Oral-Health (accessed on 4 November 2022).
- Iandolo, A.; Amato, A.; Martina, S.; Latif, D.A.; Pantaleo, G. Management of Severe Curvatures in Root Canal Treatment with the New Generation of Rotating Files Using a Safe and Predictable Protocol. Open Dent. J. 2020, 14, 421–425. [Google Scholar] [CrossRef]
- Campagnaro, R.; de Oliveira Collet, G.; de Andrade, M.P.; Salles, J.P.; Fracasso, M.D.; Scheffel, D.L.; Freitas, K.M.; Santin, G.C. COVID-19 Pandemic and Pediatric Dentistry: Fear, Eating Habits and Parent’s Oral Health Perceptions. Child. Youth Serv. Rev. 2020, 118, 105469. [Google Scholar] [CrossRef]
- Amato, A.; Iandolo, A.; Scelza, G.; Spirito, F.; Martina, S. COVID-19: The Patients’ Perceived Impact on Dental Care. Eur. J. Dent. 2022, 16, 333–338. [Google Scholar] [CrossRef]
- Gu, L.; Pathoulas, J.T.; Widge, A.S.; Idnani, A.; Lipner, S.R. Exacerbation of Onychophagia and Onychotillomania during the COVID-19 Pandemic: A Survey-based Study. Int. J. Dermatol. 2022, 61, e412–e414. [Google Scholar] [CrossRef]
- Kolcakoglu, K.; Yucel, G. Anxiety and Harmful Oral Habits in Preschool Children during the 2020 First-Wave COVID-19 Lockdown in Turkey. Dent. Med. Probl. 2021, 58, 433–439. [Google Scholar] [CrossRef]
- Kui, A.; Popescu, C.; Labuneț, A.; Almășan, O.; Petruțiu, A.; Păcurar, M.; Buduru, S. Is Teledentistry a Method for Optimizing Dental Practice, Even in the Post-Pandemic Period? An Integrative Review. Int. J. Environ. Res. Public Health 2022, 19, 7609. [Google Scholar] [CrossRef] [PubMed]
- de Cola, M.C.; Maresca, G.; D’Aleo, G.; Carnazza, L.; Giliberto, S.; Maggio, M.G.; Bramanti, A.; Calabrò, R.S. Teleassistance for Frail Elderly People: A Usability and Customer Satisfaction Study. Geriatr. Nurs. 2020, 41, 463–467. [Google Scholar] [CrossRef] [PubMed]
- Muniz, I.D.A.F.; Campos, D.E.S.; Shinkai, R.S.A.; Trindade, T.G.D.; Cosme-Trindade, D.C. Case Report of Oral Mucosa Garlic Burn during COVID-19 Pandemic Outbreak and Role of Teledentistry to Manage Oral Health in an Older Adult Woman. Spec. Care Dent. 2021, 41, 639–643. [Google Scholar] [CrossRef] [PubMed]
- Brecher, E.A.; Keels, M.A.; Carrico, C.K.; Hamilton, D.S. Teledentistry Implementation in a Private Pediatric Dental Practice During the COVID-19 Pandemic. Pediatr. Dent. 2021, 43, 463–467. [Google Scholar] [PubMed]
- Wallace, C.K.; Schofield, C.E.; Burbridge, L.A.L.; O’Donnell, K.L. Role of Teledentistry in Paediatric Dentistry. Br. Dent. J. 2021, 25, 1–6. [Google Scholar] [CrossRef]
- Lewandowska, M.; Partyka, M.; Romanowska, P.; Saczuk, K.; Lukomska-Szymanska, M.M. Impact of the COVID-19 pandemic on the dental service: A narrative review. Dent. Med. Probl. 2021, 58, 539–544. [Google Scholar] [CrossRef]
- Samaranayake, L.; Anil, S. The Monkeypox Outbreak and Implications for Dental Practice. Int. Dent. J. 2022, 72, 589–596. [Google Scholar] [CrossRef]
- Di Spirito, F.; Amato, A.; di Palo, M.P.; Contaldo, M.; D’Ambrosio, F.; lo Giudice, R.; Amato, M. Oral Lesions Following Anti-SARS-CoV-2 Vaccination: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 10228. [Google Scholar] [CrossRef]
- lo Giudice, R.; Famà, F. Health Care and Health Service Digital Revolution. Int. J. Environ. Res. Public Health 2020, 17, 4913. [Google Scholar] [CrossRef]
- Butera, A.; Maiorani, C.; Natoli, V.; Bruni, A.; Coscione, C.; Magliano, G.; Giacobbo, G.; Morelli, A.; Moressa, S.; Scribante, A. Bio-Inspired Systems in Nonsurgical Periodontal Therapy to Reduce Contaminated Aerosol during COVID-19: A Comprehensive and Bibliometric Review. J. Clin. Med. 2020, 9, 3914. [Google Scholar] [CrossRef]
- Estai, M.; Kanagasingam, Y.; Xiao, D.; Vignarajan, J.; Huang, B.; Kruger, E.; Tennant, M. A Proof-of-Concept Evaluation of a Cloud-Based Store-and-Forward Telemedicine App for Screening for Oral Diseases. J. Telemed. Telecare 2016, 22, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Sharma, H.; Suprabha, B.S.; Rao, A. Teledentistry and Its Applications in Paediatric Dentistry: A Literature Review. Pediatr. Dent. J. 2021, 31, 203–215. [Google Scholar] [CrossRef] [PubMed]
- Singhal, S.; Mohapatra, S.; Quiñonez, C. Reviewing Teledentistry Usage in Canada during COVID-19 to Determine Possible Future Opportunities. Int. J. Environ. Res. Public Health 2021, 19, 31. [Google Scholar] [CrossRef] [PubMed]
- Cook, J.; Austen, G.; Stephens, C. Videoconferencing: What Are the Benefits for Dental Practice? Br. Dent. J. 2000, 188, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.N.; Antonarakis, G.S. Factors Influencing the Adoption and Implementation of Teledentistry in the UK, with a Focus on Orthodontics. Community Dent. Oral Epidemiol. 2012, 41, 424–431. [Google Scholar] [CrossRef]
- Sanghvi, R.; Barrow, S.; Hullah, E.; de Souza, M.; Cook, R.; Siddik, D. Paediatric Dental-Oral Medicine Clinic: Management during COVID 19. J. Oral Med. Oral Surg. 2021, 27, 18. [Google Scholar] [CrossRef]
- McLaren, S.W.; Kopycka-Kedzierawski, D.T.; Nordfelt, J. Accuracy of Teledentistry Examinations at Predicting Actual Treatment Modality in a Pediatric Dentistry Clinic. J. Telemed. Telecare 2017, 23, 710–715. [Google Scholar] [CrossRef]
- Haron, N.; Zain, R.B.; Ramanathan, A.; Abraham, M.T.; Liew, C.S.; Ng, K.G.; Cheng, L.C.; Husin, R.B.; Chong, S.M.Y.; Thangavalu, L.A.; et al. M-Health for Early Detection of Oral Cancer in Low- and Middle-Income Countries. Telemed. e-Health 2020, 26, 278–285. [Google Scholar] [CrossRef]
- Viswanathan, A.; Patel, N.; Vaidyanathan, M.; Bhujel, N. Utilizing Teledentistry to Manage Cleft Lip and Palate Patients in an Outpatient Setting. Cleft Palate-Craniofacial J. 2022, 59, 675–679. [Google Scholar] [CrossRef]
- Bossù, M.; Valletta, A.; Fiore, R.; Riccitiello, F.; D’Amora, M.; Coppolino, F.; Simeone, M.; Polimeni, A. Deciduous Dentition: Anatomical Study by μ-CT|Dentizione Decidua: Studio Della Complessità Anatomica Mediante ΜtC. Recent. Prog. Med. 2013, 104, 425–429. [Google Scholar]
- Pace, M.; Cioffi, I.; D’antò, V.; Valletta, A.; Valletta, R.; Amato, M. Facial Attractiveness of Skeletal Class i and Class II Malocclusion as Perceived by Laypeople, Patients and Clinicians. Minerva Stomatol. 2018, 67, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Nutalapati, R.; Boyapati, R.; Jampani, N.; Dontula, B.S.K. Applications of Teledentistry: A Literature Review and Update. J. Int. Soc. Prev. Community Dent. 2011, 1, 37. [Google Scholar] [CrossRef] [PubMed]
- Maspero, C.; Abate, A.; Cavagnetto, D.; el Morsi, M.; Fama, A.; Farronato, M. Available Technologies, Applications and Benefits of Teleorthodontics. A Literature Review and Possible Applications during the COVID-19 Pandemic. J. Clin. Med. 2020, 9, 1891. [Google Scholar] [CrossRef]
- Sangalli, L.; Savoldi, F.; Dalessandri, D.; Bonetti, S.; Gu, M.; Signoroni, A.; Paganelli, C. Effects of Remote Digital Monitoring on Oral Hygiene of Orthodontic Patients: A Prospective Study. BMC Oral Health 2021, 21, 435. [Google Scholar] [CrossRef] [PubMed]
- Mandall, N.A.; O’Brien, K.D.; Brady, J.; Worthington, H.V.; Harvey, L. Teledentistry for Screening New Patient Orthodontic Referrals. Part 1: A Randomised Controlled Trial. Br. Dent. J. 2005, 199, 659–662. [Google Scholar] [CrossRef] [Green Version]
- Borujeni, E.S.; Sarshar, F.; Nasiri, M.; Sarshar, S.; Jazi, L. Effect of Teledentistry on the Oral Health Status of Patients Undergoing Fixed Orthodontic Treatment at the First Three Follow-up Visits. Dent. Med. Probl. 2021, 58, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Menachemi, N.; Burke, D.E.; Ayers, D.J. Factors Affecting the Adoption of Telemedicine—A Multiple Adopter Perspective. J. Med. Syst. 2004, 28, 617–632. [Google Scholar] [CrossRef]
- Byrne, E.; Watkinson, S. Patient and Clinician Satisfaction with Video Consultations during the COVID-19 Pandemic: An Opportunity for a New Way of Working. J. Orthod. 2021, 48, 64–73. [Google Scholar] [CrossRef]
- Giraudeau, N.; Bauer, M.; Tramini, P.; Inquimbert, C.; Toupenay, S. A National Teledentistry Study on the Knowledge, Attitudes, Training and Practices of Private Dentists. Digit. Health 2022, 8, 205520762210850. [Google Scholar] [CrossRef]
- Fijačko, N.; Gosak, L.; Cilar, L.; Novšak, A.; Creber, R.M.; Skok, P.; Štiglic, G. The Effects of Gamification and Oral Self-Care on Oral Hygiene in Children: Systematic Search in App Stores and Evaluation of Apps. JMIR Mhealth Uhealth 2020, 8, e16365. [Google Scholar] [CrossRef]
- Xiao, J.; Luo, J.; Ly-Mapes, O.; Wu, T.T.; Dye, T.; al Jallad, N.; Hao, P.; Ruan, J.; Bullock, S.; Fiscella, K. Assessing a Smartphone App (AICaries) That Uses Artificial Intelligence to Detect Dental Caries in Children and Provides Interactive Oral Health Education: Protocol for a Design and Usability Testing Study. JMIR Res. Protoc. 2021, 10, e32921. [Google Scholar] [CrossRef] [PubMed]
- Scheerman, J.F.M.; Meijel, B.; Empelen, P.; Verrips, G.H.W.; Loveren, C.; Twisk, J.W.R.; Pakpour, A.H.; Braak, M.C.T.; Kramer, G.J.C. The Effect of Using a Mobile Application (“WhiteTeeth”) on Improving Oral Hygiene: A Randomized Controlled Trial. Int. J. Dent. Hyg. 2020, 18, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Aghiorghiesei, O.; Zanoaga, O.; Nutu, A.; Braicu, C.; Campian, R.S.; Lucaciu, O.; Berindan Neagoe, I. The World of Oral Cancer and Its Risk Factors Viewed from the Aspect of MicroRNA Expression Patterns. Genes 2022, 13, 594. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.V.; Kang, E.T.B.; Senger, C.; Poh, C.F. Oral Cancer in a 5-Year-Old Boy: A Rare Case Report and Review of Literature. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 130, e10–e19. [Google Scholar] [CrossRef] [PubMed]
- Krishna, M.; Sybil, D.; Shrivastava, P.K.; Premchandani, S.; Kumar, H.; Kumar, P. An Innovative App (ExoDont) for Postoperative Care of Patients After Tooth Extraction: Prototype Development and Testing Study. JMIR Perioper. Med. 2021, 4, e31852. [Google Scholar] [CrossRef]
- D’Ambrosio, F.; di Spirito, F.; de Caro, F.; Lanza, A.; Passarella, D.; Sbordone, L. Adherence to Antibiotic Prescription of Dental Patients: The Other Side of the Antimicrobial Resistance. Healthcare 2022, 10, 1636. [Google Scholar] [CrossRef]
- D’Ambrosio, F.; di Spirito, F.; Amato, A.; Caggiano, M.; lo Giudice, R.; Martina, S. Attitudes towards Antibiotic Prescription and Antimicrobial Resistance Awareness among Italian Dentists: What Are the Milestones? Healthcare 2022, 10, 1585. [Google Scholar] [CrossRef]
- Caruso, S.; Caruso, S.; Pellegrino, M.; Skafi, R.; Nota, A.; Tecco, S. A Knowledge-Based Algorithm for Automatic Monitoring of Orthodontic Treatment: The Dental Monitoring System. Two Cases. Sensors 2021, 21, 1856. [Google Scholar] [CrossRef]
- Ramanarayanan, V.; Sanjeevan, V.; Janakiram, C. The Covid-19 Uncertainty and Ethical Dilemmas in Dental Practice. Indian J. Med. Ethics 2021, 6, 182–183. [Google Scholar] [CrossRef]
- Elster, N.; Parsi, K. Oral Health Matters: The Ethics of Providing Oral Health During COVID-19. HEC Forum 2021, 33, 157–164. [Google Scholar] [CrossRef]
- Opydo-Szymaczek, J.; Borysewicz-Lewicka, M.; Andrysiak, K.; Witkowska, Z.; Hoffmann-Przybylska, A.; Przybylski, P.; Walicka, E.; Gerreth, K. Clinical Consequences of Dental Caries, Parents’ Perception of Child’s Oral Health and Attitudes towards Dental Visits in a Population of 7-Year-Old Children. Int. J. Environ. Res. Public Health 2021, 18, 5844. [Google Scholar] [CrossRef] [PubMed]
- Malcangi, G.; Inchingolo, A.D.; Inchingolo, A.M.; Santacroce, L.; Marinelli, G.; Mancini, A.; Vimercati, L.; Maggiore, M.E.; D’Oria, M.T.; Hazballa, D.; et al. COVID-19 Infection in Children, Infants and Pregnant Subjects: An Overview of Recent Insights and Therapies. Microorganisms 2021, 9, 1964. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| US [9] | Italy [10] | Turkey [11] | Israel [12] | |||||
|---|---|---|---|---|---|---|---|---|
| 2019 | 2020 | 2019 | 2020 | 2019 | 2020 | 2019 | 2020 | |
| Dental traumas | 67.4% | 68.0% | Dislocation and Avulsion 41% Fractures 35.5% | 24.7% | ||||
| School-related | 21.8% | 1.9% | ||||||
| Cycling-related | 3.6% | 9.6% | ||||||
| Dog bites-related | 6.0% | 8.7% | ||||||
| Swelling/pain | 32.6% | |||||||
| Swelling due to abscess | 22.7% | 25.2% | 86.5% | |||||
| Pain due to dental pulp inflammation | 94.0% | |||||||
| Infections | 28.1% | 23.5% | 15% | 15% | 28.4% | |||
| Dental | 40.0% | 68.1% | ||||||
| Mucosal (“oral ulcers”) | 47.6% | 19.4% | ||||||
| Mucosal injuries | ||||||||
| Due to orthodontic appliances | 20.5% | |||||||
| Not due to orthodontic appliances (any) | 19.5% | |||||||
| India March–July 2020 [14] | Poland March–April 2019/2020 [15] | ||
|---|---|---|---|
| Non Emergency treatments | 2019 | 2020 | |
| Primary teeth | |||
| 6.4% | 19.3% | ||
| Teeth restorations | 42% | Permanent teeth | |
| 5.8% | 11.4% | ||
| Preventive procedures | 24.4% | ||
| Elective treatments | 12.6% | ||
| Emergency treatments | |||
| Endodontics | 3.2% | 12.8% | |
| Abscess incisions | 3.5% | 17.8% | |
| Oral mucosal lesions treatments | 2.3% | 4.3% | |
| Surgical dressing | 1.5% | 10.07% | |
| Turkey [20] | Germany [21] | Brazil [22] | Italy [23] (Orthodontics) | Italy [24] | ||||
|---|---|---|---|---|---|---|---|---|
| Dental routine visits | Before COVID-19 outbreak 60.4% | After COVID-19 Outbreak 5.2% | Before COVID-19 outbreak 24.4% | After COVID-19 outbreak 17.8% | ||||
| Missed dental routine visits | 64.2% | 16% | ||||||
| Dental treatment | −38% | |||||||
| Urgent treatments (only) | 66.6% | 72% | ||||||
| Non-urgent treatments | 15.1% | |||||||
| Missed appointment for urgent treatments | 86% | |||||||
| Parents’ anxiety or fear | 54.6% | 65.3% | ||||||
| Parents considering the dental setting as a source of infection | 79.6% | 2020 [24] 55.3% | 2022 [25] 43% | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Spirito, F.; Amato, A.; Di Palo, M.P.; Ferraro, G.A.; Baroni, A.; Serpico, R.; Contaldo, M. COVID-19 Related Information on Pediatric Dental Care including the Use of Teledentistry: A Narrative Review. Children 2022, 9, 1942. https://doi.org/10.3390/children9121942
Di Spirito F, Amato A, Di Palo MP, Ferraro GA, Baroni A, Serpico R, Contaldo M. COVID-19 Related Information on Pediatric Dental Care including the Use of Teledentistry: A Narrative Review. Children. 2022; 9(12):1942. https://doi.org/10.3390/children9121942
Chicago/Turabian StyleDi Spirito, Federica, Alessandra Amato, Maria Pia Di Palo, Giuseppe A. Ferraro, Adone Baroni, Rosario Serpico, and Maria Contaldo. 2022. "COVID-19 Related Information on Pediatric Dental Care including the Use of Teledentistry: A Narrative Review" Children 9, no. 12: 1942. https://doi.org/10.3390/children9121942