

Social, Educational and Medical Aspects after Cataract Surgery of Bilaterally Blind Children in Kinshasa—Perception of Parents and Children
 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Site and Study Population
2.2. Study Instrument
2.3. Data Collection and Analysis
3. Results
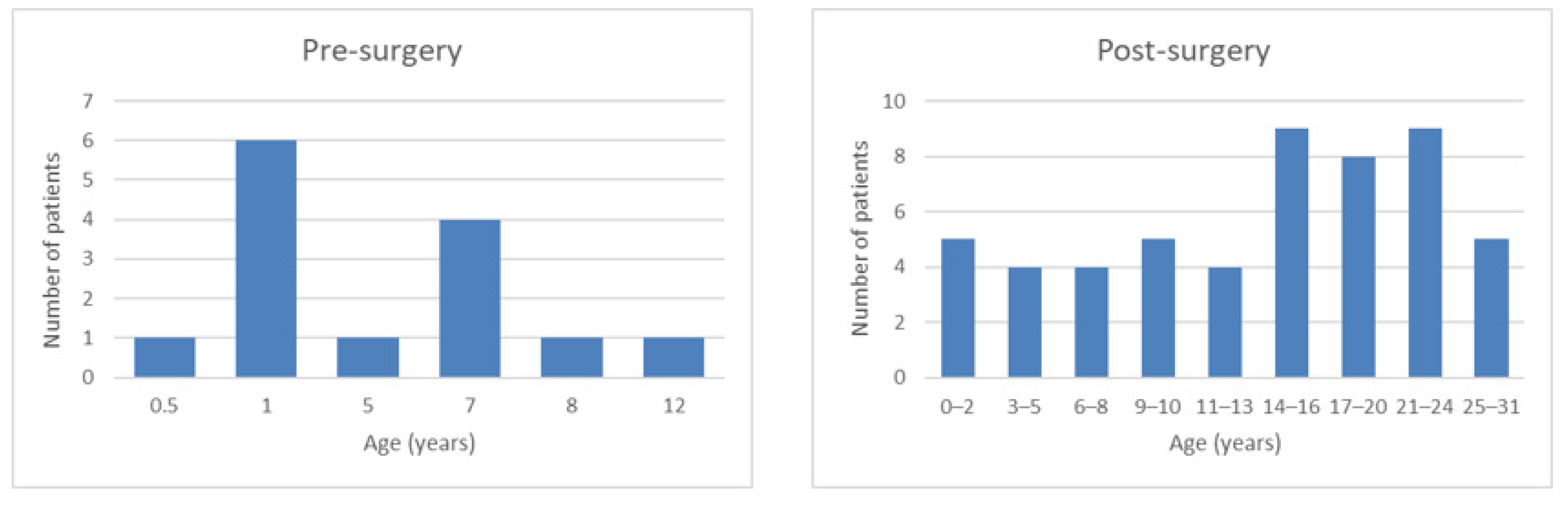
3.1. Characteristics of the Study Population
3.2. Pre-Surgery Group—Perception of Parents
3.2.1. Visit to the Hospital
3.2.2. Cataract Surgery
3.3. Post-Surgery Group—Perception of Parents
3.3.1. Visit to the Hospital
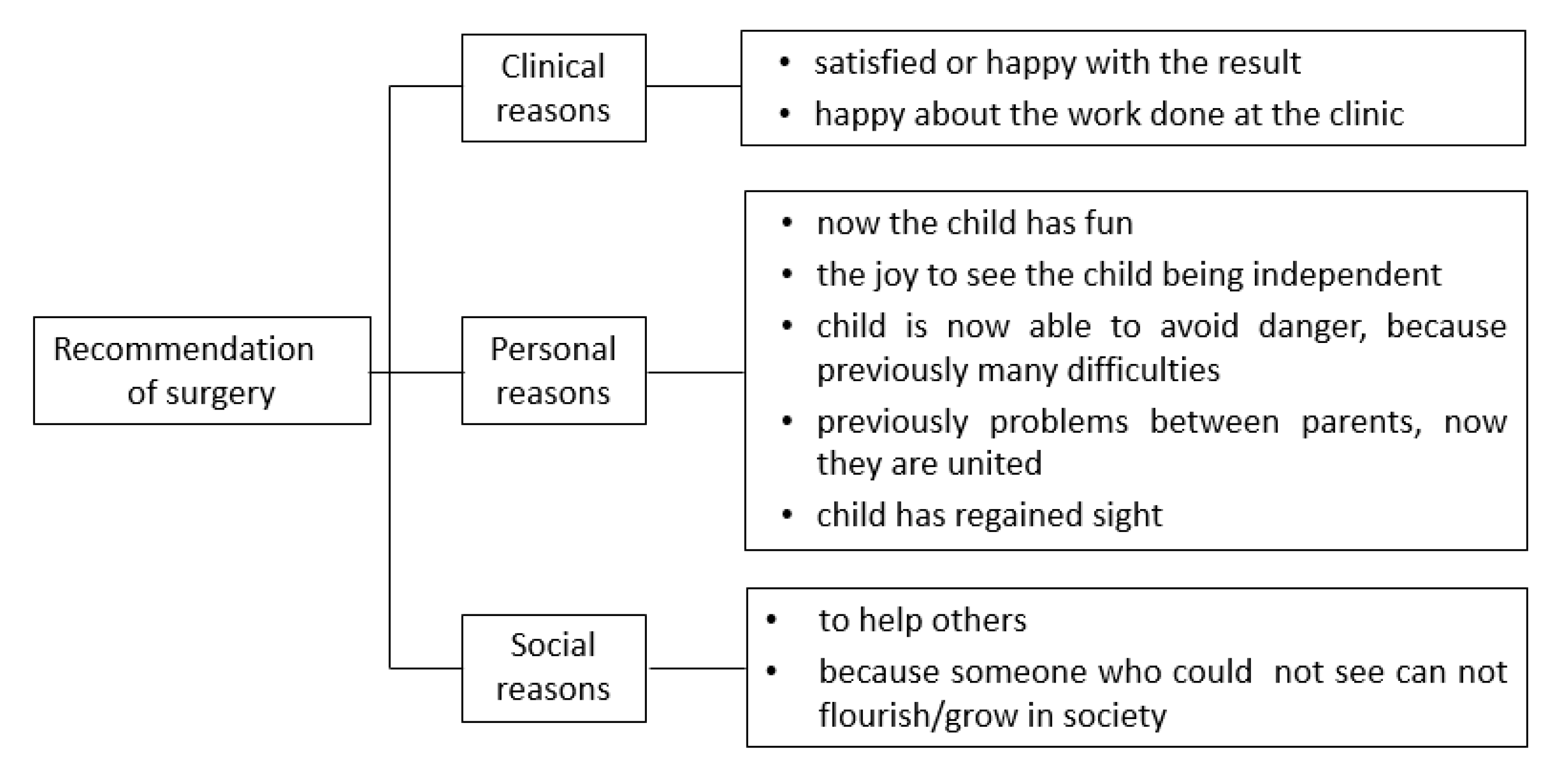
3.3.2. Recommendation of Surgery to Others
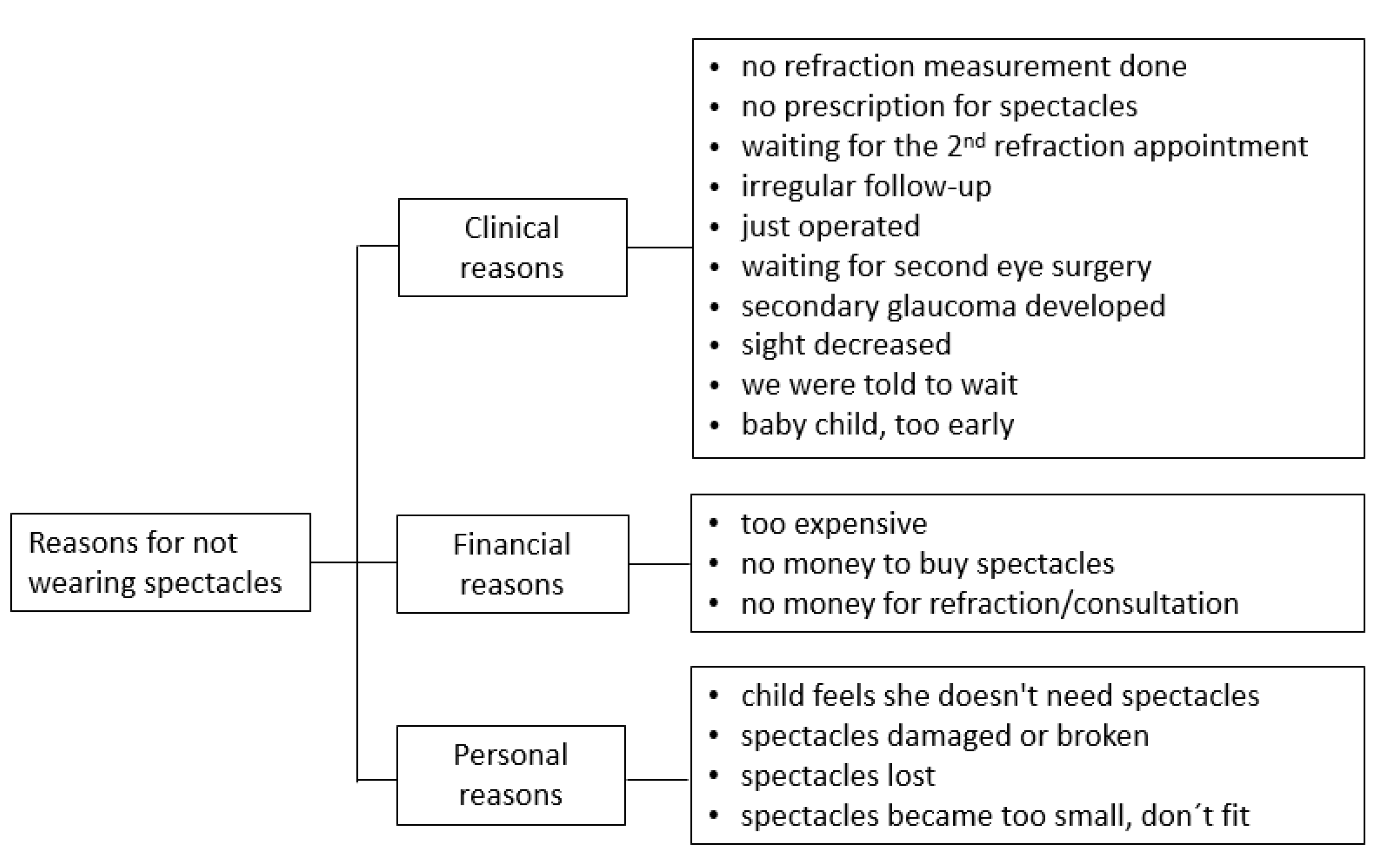
3.3.3. Eyeglasses
3.3.4. Follow-Up Examination
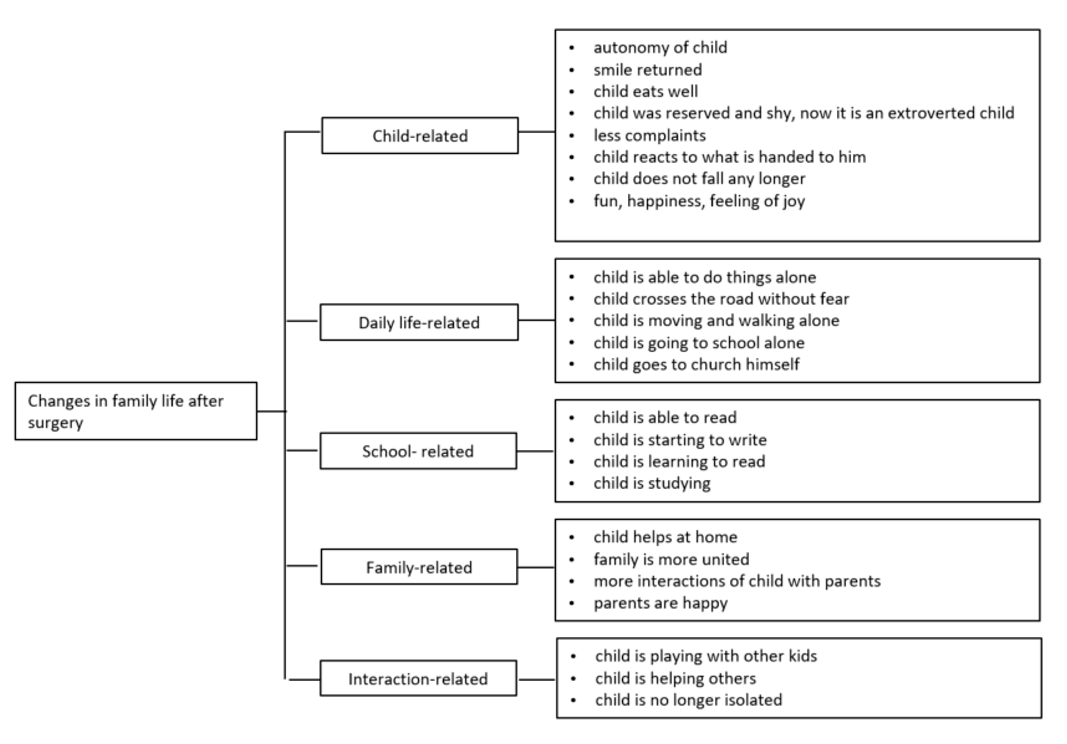
3.3.5. Family Life after Surgery
3.3.6. The Complete Treatment Process at a Glance
3.4. Post-Surgery Group—Perception of Children
3.4.1. After the Surgery
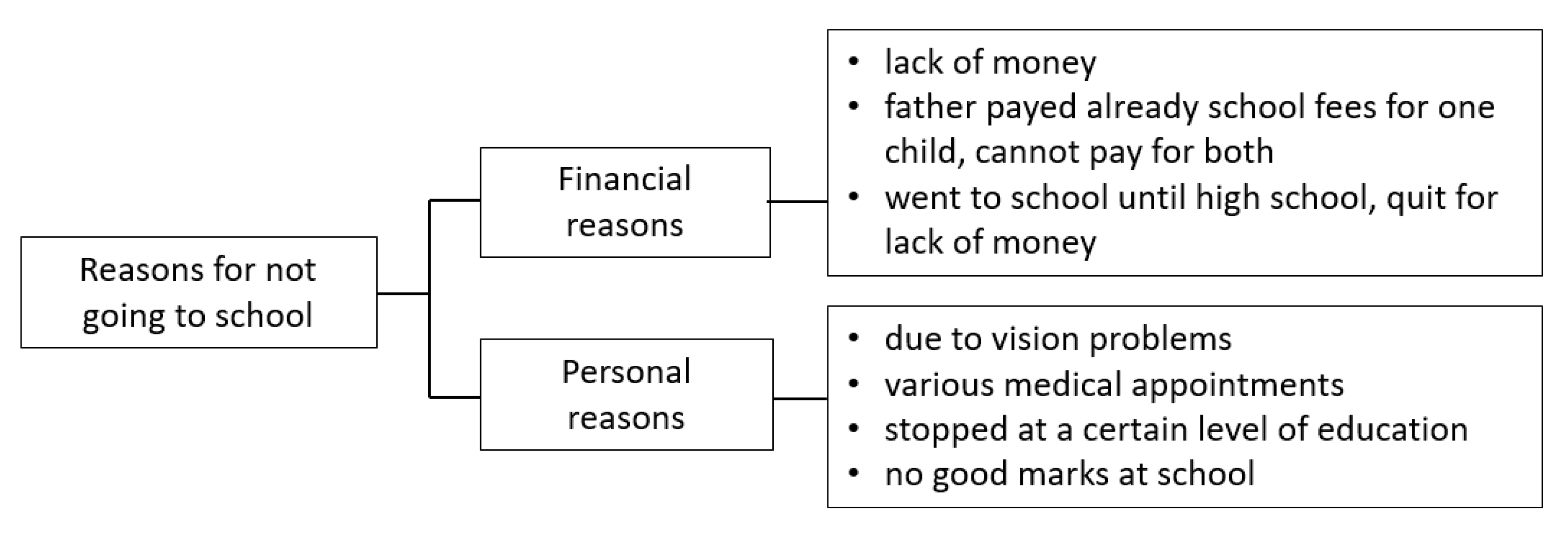
3.4.2. School and Education
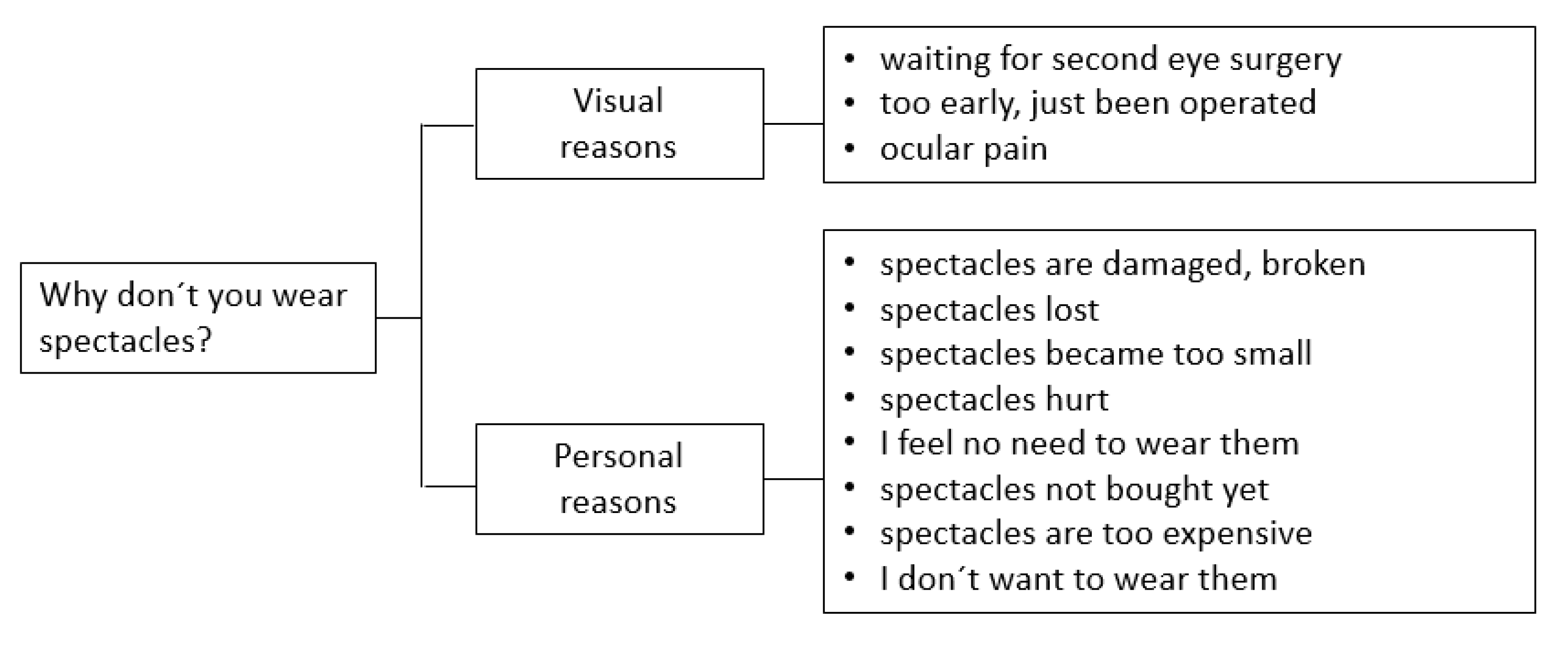
3.4.3. Eyeglasses
3.4.4. Personal Wishes for the Future
4. Discussion
4.1. Delay between Detection of Cataract and Start of Treatment
4.2. Barriers Influencing the Treatment Process
4.3. Parents’ Perceptions Concerning the Recommendation of Surgery to Others and Their Suggestions for Improvement of the Treatment Process
4.4. Wearing Eyeglasses
4.5. Strength and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Solebo, A.L.; Teoh, L.; Rahi, J. Epidemiology of blindness in children. Arch. Dis. Child. 2017, 102, 853–857. [Google Scholar] [CrossRef] [Green Version]
- Kong, L.; Fry, M.; Al-Samarraie, M.; Gilbert, C.; Steinkuller, P.G. An update on progress and the changing epidemiology of causes of childhood blindness worldwide. J. AAPOS 2012, 16, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Pascolini, D.; Mariotti, S.P. Global estimates of visual impairment: 2010. Br. J. Ophthalmol. 2012, 96, 614–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Courtright, P. Childhood cataract in sub-Saharan Africa. Saudi J. Ophthalmol. 2012, 26, 3–6. [Google Scholar] [CrossRef] [Green Version]
- Sheeladevi, S.; Lawrenson, J.G.; Fielder, A.R.; Suttle, C.M. Global prevalence of childhood cataract: A systematic review. Eye 2016, 30, 1160–1169. [Google Scholar] [CrossRef] [Green Version]
- Geneau, R.; Lewallen, S.; Bronsard, A.; Paul, I.; Courtright, P. The social and family dynamics behind the uptake of cataract surgery: Findings from Kilimanjaro region, Tanzania. Br. J. Ophthalmol. 2005, 89, 1399–1402. [Google Scholar] [CrossRef] [Green Version]
- Yorston, D.; Gichuhi, S.; Wood, M.; Foster, A. Does prospective monitoring improve cataract surgery outcomes in Africa? Br. J. Ophthalmol. 2002, 86, 543–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stasse, S.; Vita, D.; Kimfuta, J.; Da Silveira, V.C.; Bossyns, P.; Criel, B. Improving financial access to health care in the Kisantu district in the Democratic Republic of Congo: Acting upon complexity. Glob. Health Action 2015, 8, 25480. [Google Scholar] [CrossRef] [Green Version]
- Kinshasa Population 2022 (Demographics, Maps, Graphs). Available online: https://worldpopulationreview.com/world-cities/kinshasa-population (accessed on 13 October 2022).
- Kilangalanga, N.J.; Nsiangani, L.N.; Dilu, A.A.; Moanda, K.A.; Ilunga, M.J.; Makwanga, M.E.; Stahnke, T.; Guthoff, R. Epidemiology of Childhood Blindness and Low Vision in Kinshasa-democratic Republic of the Congo. Ophthalmic Epidemiol. 2020, 27, 45–51. [Google Scholar] [CrossRef]
- Steinmetz, J.D.; Bourne, R.R.A.; Briant, P.S.; Flaxman, S.R.; Taylor, H.R.B.; Jonas, J.B.; Abdoli, A.A.; Abrha, W.A.; Abualhasan, A.; Abu-Gharbieh, E.G.; et al. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: The Right to Sight: An analysis for the Global Burden of Disease Study. Lancet Glob. Health 2021, 9, e144–e160. [Google Scholar] [CrossRef]
- Amiebenomo, O.M.; Achugwo, D.C.; Abah, I. Parental knowledge and attitude to children’s eye care services. Nig. J. Paed. 2016, 43, 215. [Google Scholar] [CrossRef] [Green Version]
- Dean, S.; Mathers, J.M.; Calvert, M.; Kyte, D.G.; Conroy, D.; Folkard, A.; Southworth, S.; Murray, P.I.; Denniston, A.K. “The patient is speaking”: Discovering the patient voice in ophthalmology. Br. J. Ophthalmol. 2017, 101, 700–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilangalanga, J.N.; Stahnke, T.; Moanda, A.; Makwanga, E.; Hopkins, A.; Guthoff, R.F. Role of a Community-based Program for Identification and Referral of Pediatric Cataract Patients in Kinshasa, Democratic Republic of the Congo. Middle East Afr. J. Ophthalmol. 2019, 26, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Gogate, P.; Kalua, K.; Courtright, P. Blindness in childhood in developing countries: Time for a reassessment? PLoS Med. 2009, 6, e1000177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Courtright, P. Meeting the needs of children with congenital and developmental cataract in Africa. Community Eye Health J. 2008, 2008, 18–19. [Google Scholar]
- Ebeigbe, J.A.; Emedike, C.M. Parents’ awareness and perception of children’s eye diseases in Nigeria. J. Optom. 2017, 10, 104–110. [Google Scholar] [CrossRef]
- Bronsard, A.; Geneau, R.; Shirima, S.; Courtright, P.; Mwende, J. Why are children brought late for cataract surgery? Qualitative findings from Tanzania. Ophthalmic Epidemiol. 2008, 15, 383–388. [Google Scholar] [CrossRef]
- Mbonye, A.K. Prevalence of childhood illnesses and care-seeking practices in rural Uganda. Sci. World J. 2003, 3, 721–730. [Google Scholar] [CrossRef] [Green Version]
- Mwende, J.; Bronsard, A.; Mosha, M.; Bowman, R.; Geneau, R.; Courtright, P. Delay in presentation to hospital for surgery for congenital and developmental cataract in Tanzania. Br. J. Ophthalmol. 2005, 89, 1478–1482. [Google Scholar] [CrossRef] [Green Version]
- Sen, P.; Gupta, N.; Mohan, A.; Shah, C.; Sen, A.; Jain, E. Causes of delayed presentation of pediatric cataract: A questionnaire-based prospective study at a tertiary eye care center in central rural India. Indian J. Ophthalmol. 2020, 68, 603–607. [Google Scholar] [CrossRef]
- Bowman, R.J.C. How should blindness in children be managed? Eye 2005, 19, 1037–1043. [Google Scholar] [CrossRef] [PubMed]
- Rotchford, A.P.; Rotchford, K.M.; Mthethwa, L.P.; Johnson, G.J. Reasons for poor cataract surgery uptake—A qualitative study in rural South Africa. Trop. Med. Int. Health 2002, 7, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Lohfeld, L.; Graham, C.; Ebri, A.E.; Congdon, N.; Chan, V.F. Parents’ reasons for nonadherence to referral to follow-up eye care for schoolchildren who failed school-based vision screening in Cross River State, Nigeria-A descriptive qualitative study. PLoS ONE 2021, 16, e0259309. [Google Scholar] [CrossRef]
- Johnson, J.G.; Goode Sen, V.; Faal, H. Barriers to the uptake of cataract surgery. Trop. Doct. 1998, 28, 218–220. [Google Scholar] [CrossRef] [PubMed]
- Courtright, P.; Kanjaloti, S.; Lewallen, S. Barriers to acceptance of cataract surgery among patients presenting to district hospitals in rural Malawi. Trop. Geogr. Med. 1995, 47, 15–18. [Google Scholar] [PubMed]
- Ebeigbe, J.A. Factors influencing eye-care seeking behaviour of parents for their children in Nigeria. Clin. Exp. Optom. 2016, 101, 560–564. [Google Scholar] [CrossRef] [Green Version]
- Muhit Mohammad, A. Childhood Cataract: Home to Hospital. Community Eye Health J. 2004, 17, 19–22. [Google Scholar]
- Kitema, G.F.; Morjaria, P.; Mathenge, W.; Ramke, J. The Appointment System Influences Uptake of Cataract Surgical Services in Rwanda. Int. J. Environ. Res. Public Health 2021, 18, 743. [Google Scholar] [CrossRef]
- Wakefield, M.A.; Loken, B.; Hornik, R.C. Use of mass media campaigns to change health behaviour. Lancet 2010, 376, 1261–1271. [Google Scholar] [CrossRef] [Green Version]
- Ntsoane, M.D.; Oduntan, O.A. A review of factors influencing the utilization of eye care services. Afr. Vis. Eye Health 2010, 69, 182–192. [Google Scholar] [CrossRef] [Green Version]
- Burn, H.; Puri, L.; Roshan, A.; Singh, S.K.; Burton, M.J. Primary Eye Care in Eastern Nepal. Ophthalmic Epidemiol. 2020, 27, 165–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalua, K.; Gichangi, M.; Barassa, E.; Eliah, E.; Lewallen, S.; Courtright, P. Skills of general health workers in primary eye care in Kenya, Malawi and Tanzania. Hum. Resour. Health 2014, 12 (Suppl. 1), S2. [Google Scholar] [CrossRef] [PubMed]
- Kishiki, E.; Hogeweg, M.; Dieleman, M.; Lewallen, S.; Courtright, P. Is the existing knowledge and skills of health workers regarding eye care in children sufficient to meet needs? Int. Health 2012, 4, 303–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eriksen, J.R.; Bronsard, A.; Mosha, M.; Carmichael, D.; Hall, A.; Courtright, P. Predictors of poor follow-up in children that had cataract surgery. Ophthalmic Epidemiol. 2006, 13, 237–243. [Google Scholar] [CrossRef]
- Kishiki, E.; Shirima, S.; Lewallen, S.; Courtright, P. Improving postoperative follow-up of children receiving surgery for congenital or developmental cataracts in Africa. J. AAPOS 2009, 13, 280–282. [Google Scholar] [CrossRef]
- Kishiki, E.; van Dijk, K.; Courtright, P. Strategies to improve follow-up of children after surgery for cataract: Findings from Child Eye Health Tertiary Facilities in sub-Saharan Africa and South Asia. Eye 2016, 30, 1234–1241. [Google Scholar] [CrossRef] [Green Version]
- Odedra, N.; Wedner, S.H.; Shigongo, Z.S.; Nyalali, K.; Gilbert, C. Barriers to spectacle use in Tanzanian secondary school students. Ophthalmic Epidemiol. 2008, 15, 410–417. [Google Scholar] [CrossRef]
- Megbelayin Emmanuel, O. Barriers to Uptake of Prescribed Refractive Spectacles Amongst Nigerian Students 2013, pp. 71–77. Available online: https://www.researchgate.net/publication/249341532_Barriers_to_uptake_of_prescribed_refractive_spectacles_amongst_Nigerian_students (accessed on 10 August 2022).
- Chan, V.F.; Yong, A.C.; O’Neill, C.; Graham, C.; Congdon, N.; Lohfeld, L.; Stephan, T.; Ebri, A.E. Factors affecting guardians’ decision making on clinic-based purchase of children’s spectacles in Nigeria. PLoS ONE 2021, 16, e0254517. [Google Scholar] [CrossRef]
- Burnett, A.M.; Yashadhana, A.; Lee, L.; Serova, N.; Brain, D.; Naidoo, K. Interventions to improve school-based eye-care services in low- and middle-income countries: A systematic review. Bull. World Health Organ. 2018, 96, 682–694D. [Google Scholar] [CrossRef]
- Murthy, G.V.S.; John, N.; Shamanna, B.R.; Pant, H.B. Elimination of avoidable blindness due to cataract: Where do we prioritize and how should we monitor this decade? Indian J. Ophthalmol. 2012, 60, 438–445. [Google Scholar] [CrossRef]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frech, S.; Hopkins, A.; Moanda, A.; Kilangalanga, J.; Guthoff, R.F. Social, Educational and Medical Aspects after Cataract Surgery of Bilaterally Blind Children in Kinshasa—Perception of Parents and Children. Children 2022, 9, 1683. https://doi.org/10.3390/children9111683
Frech S, Hopkins A, Moanda A, Kilangalanga J, Guthoff RF. Social, Educational and Medical Aspects after Cataract Surgery of Bilaterally Blind Children in Kinshasa—Perception of Parents and Children. Children. 2022; 9(11):1683. https://doi.org/10.3390/children9111683
Chicago/Turabian StyleFrech, Stefanie, Adrian Hopkins, Astrid Moanda, Janvier Kilangalanga, and Rudolf F. Guthoff. 2022. "Social, Educational and Medical Aspects after Cataract Surgery of Bilaterally Blind Children in Kinshasa—Perception of Parents and Children" Children 9, no. 11: 1683. https://doi.org/10.3390/children9111683