
Correlation between Pacifier Use in Preterm Neonates and Breastfeeding in Infancy: A Systematic Review

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Exposure/Intervention: Pacifier Use by Preterm Neonates
2.3. Outcomes: Interruption of Exclusive Breastfeeding
2.4. Search Strategy
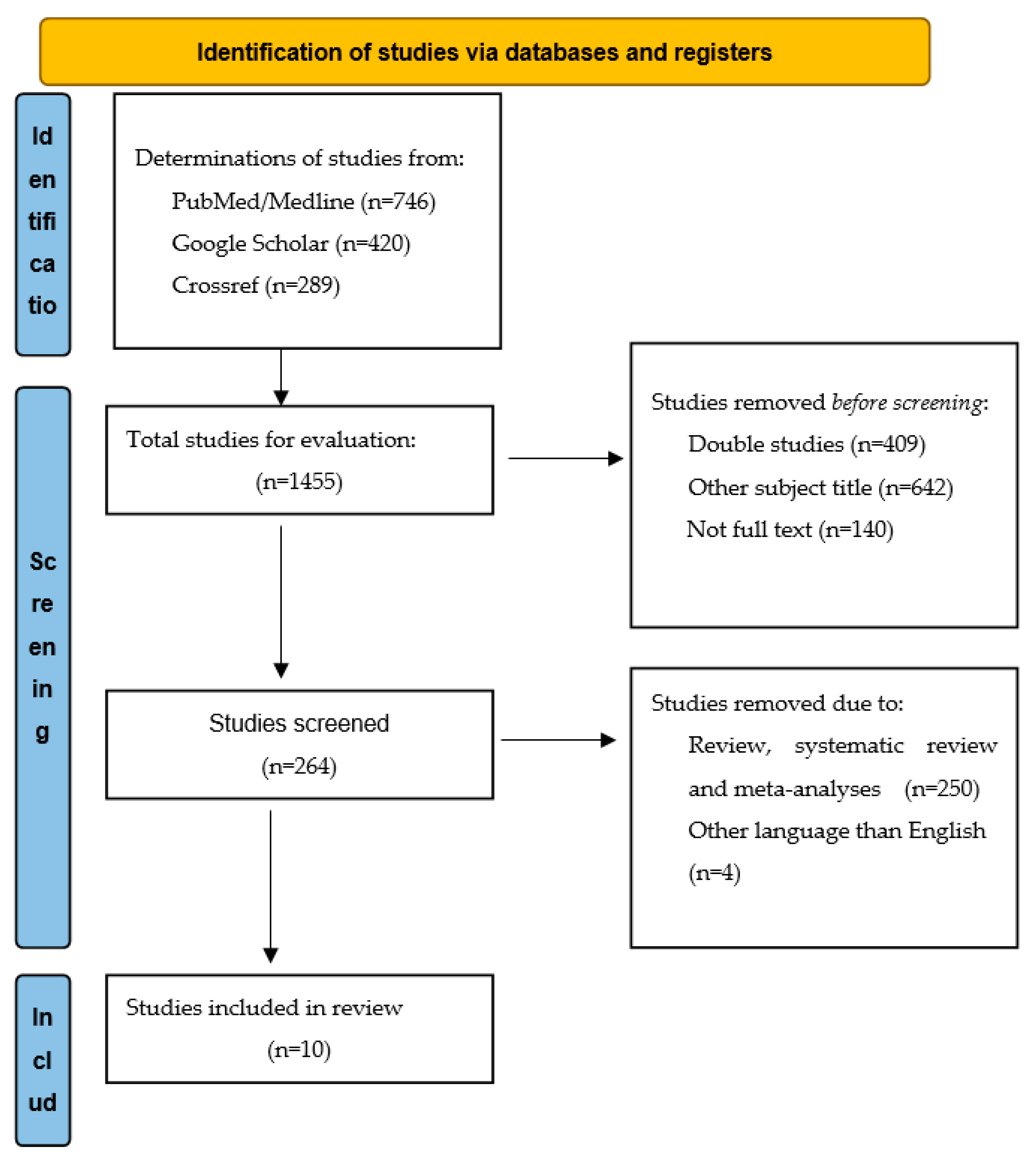
2.5. Study Selection
2.6. Quality Assessment of the Articles
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ponti, M.; Canadian Paediatric Society; Community Paediatrics Committee. Recommendations for the Use of Pacifiers. Paediatr. Child Health 2003, 8, 515–519. [Google Scholar] [CrossRef] [Green Version]
- Binns, C.W.; Lee, M.K. Exclusive Breastfeeding for Six Months: The WHO Six Months Recommendation in the Asia Pacific Region. Asia Pac. J. Clin. Nutr. 2014, 23, 344–350. [Google Scholar] [CrossRef]
- WHO European Region Has Lowest Global Breastfeeding Rates. Available online: https://www.euro.who.int/en/health-topics/Life-stages/maternal-and-newborn-health/news/news/2015/08/who-european-region-has-lowest-global-breastfeeding-rates (accessed on 21 May 2022).
- Bürger, B.; Schindler, K.; Tripolt, T.; Griesbacher, A.; Stüger, H.P.; Wagner, K.-H.; Weber, A.; Wolf-Spitzer, A. Factors Associated with (Exclusive) Breastfeeding Duration—Results of the SUKIE-Study. Nutrients 2022, 14, 1704. [Google Scholar] [CrossRef]
- Shaki, F.; Aziznejadroshan, P.; Rad, Z.A.; Chehrazi, M.; Arzani, A. Comparison of the Effect of Two Methods of Sucking on Pacifier and Mother’s Finger on Oral Feeding Behavior in Preterm Infants: A Randomized Clinical Trial. BMC Pediatr. 2022, 22, 292. [Google Scholar] [CrossRef]
- Popescu, E.A.; Popescu, M.; Wang, J.; Barlow, S.M.; Gustafson, K.M. Non-nutritive sucking recorded in utero via fetal magnetography. Physiol. Meas. 2008, 29, 127–139. [Google Scholar] [CrossRef] [PubMed]
- Harding, C.; Law, J.; Pring, T. The Use of Non-Nutritive Sucking to Promote Functional Sucking Skills in Premature Infants: An Exploratory Trial. Infant 2006, 2, 238–243. [Google Scholar]
- Grassi, A.; Cecchi, F.; Sgherri, G.; Guzzetta, A.; Gagliardi, L.; Laschi, C. Sensorized Pacifier to Evaluate Non-Nutritive Sucking in Newborns. Med. Eng. Phys. 2016, 38, 398–402. [Google Scholar] [CrossRef]
- Nijhuis, J.G. Fetal Behavior. Neurobiol. Aging 2003, 24, S41–S46; discussion S47–S49, S51–S52. [Google Scholar] [CrossRef]
- Weber, F.; Woolridge, M.W.; Baum, J.D. An Ultrasonographic Study of the Organisation of Sucking and Swallowing by Newborn Infants. Dev. Med. Child Neurol. 1986, 28, 19–24. [Google Scholar] [CrossRef]
- Lubbe, W.; ten Ham-Baloyi, W. When Is the Use of Pacifiers Justifiable in the Baby-Friendly Hospital Initiative Context? A Clinician’s Guide. BMC Pregnancy Childbirth 2017, 17, 130. [Google Scholar] [CrossRef] [Green Version]
- Kair, L.R.; Colaizy, T.T. Association Between In-Hospital Pacifier Use and Breastfeeding Continuation and Exclusivity: Neonatal Intensive Care Unit Admission as a Possible Effect Modifier. Breastfeed. Med. 2017, 12, 12–19. [Google Scholar] [CrossRef]
- Kamhawy, H.; Holditch-Davis, D.; Alsharkawy, S.; Alrafay, S.; Corazzini, K. Non-Nutritive Sucking for Preterm Infants in Egypt. J. Obs. Gynecol. Neonatal Nurs. 2014, 43, 330–340. [Google Scholar] [CrossRef]
- Office of the Surgeon General (US); Centers for Disease Control and Prevention (US); Office on Women’s Health (US). The Importance of Breastfeeding; Office of the Surgeon General (US): Washington, DC, USA, 2011.
- Neiva, F.C.B.; Leone, C.R. Sucking in preterm newborns and the sucking stimulation. Pró-Fono R. Atual. Cient. 2006, 18, 141–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonkin, S.L.; Lui, D.; McIntosh, C.G.; Rowley, S.; Knight, D.B.; Gunn, A.J. Effect of Pacifier Use on Mandibular Position in Preterm Infants. Acta Paediatr. 2007, 96, 1433–1436. [Google Scholar] [CrossRef]
- Yilmaz, F.; Arikan, D. The Effects of Various Interventions to Newborns on Pain and Duration of Crying. J. Clin. Nurs. 2011, 20, 1008–1017. [Google Scholar] [CrossRef]
- Altimier, L.; Phillips, R. The Neonatal Integrative Developmental Care Model: Advanced Clinical Applications of the Seven Core Measures for Neuroprotective Family-Centered Developmental Care. Newborn Infant Nurs. Rev. 2016, 16, 230–244. [Google Scholar] [CrossRef]
- Dadalto, E.C.V.; Rosa, E.M. Cultural Aspects for Offering Pacifiers to Children. J. Hum. Growth Dev. 2013, 23, 231–237. [Google Scholar] [CrossRef] [Green Version]
- Buccini, G.D.S.; Pérez-Escamilla, R.; Venancio, S.I. Pacifier Use and Exclusive Breastfeeding in Brazil. J. Hum. Lact. 2016, 32, NP52–NP60. [Google Scholar] [CrossRef]
- Section on Breastfeeding. Breastfeeding and the Use of Human Milk. Pediatrics 2012, 129, e827–e841. [Google Scholar] [CrossRef] [Green Version]
- Zimmerman, E. Pacifier and Bottle Nipples: The Targets for Poor Breastfeeding Outcomes. J. Pediatr. 2018, 94, 571–573. [Google Scholar] [CrossRef]
- Oral Health Policies and Recommendations. Available online: https://www.aapd.org/research/oral-health-policies--recommendations/ (accessed on 10 August 2022).
- North Stone, K.; Fleming, P.; Golding, J. Socio-Demographic Associations with Digit and Pacifier Sucking at 15 Months of Age and Possible Associations with Infant Infection. The ALSPAC Study Team. Avon Longitudinal Study of Pregnancy and Childhood. Early Hum. Dev. 2000, 60, 137–148. [Google Scholar] [CrossRef]
- Salah, M.; Abdel-Aziz, M.; Al-Farok, A.; Jebrini, A. Recurrent Acute Otitis Media in Infants: Analysis of Risk Factors. Int. J. Pediatr. Otorhinolaryngol. 2013, 77, 1665–1669. [Google Scholar] [CrossRef]
- Clark, M.; Krol, D. Protecting All Children’s Teeth: Caries. MedEdPORTAL 2013, 9, 9534. [Google Scholar] [CrossRef]
- Breastfeeding|UNICEF. Available online: https://www.unicef.org/topics/breastfeeding (accessed on 16 May 2022).
- Ten Steps to Successful Breastfeeding. Available online: https://www.who.int/teams/nutrition-and-food-safety/food-and-nutrition-actions-in-health-systems/ten-steps-to-successful-breastfeeding (accessed on 16 May 2022).
- Baby-Friendly Hospital Initiative. Available online: https://www.unicef.org/documents/baby-friendly-hospital-initiative (accessed on 10 August 2022).
- Howard, C.R.; Howard, F.M.; Lanphear, B.; Eberly, S.; deBlieck, E.A.; Oakes, D.; Lawrence, R.A. Randomized Clinical Trial of Pacifier Use and Bottle-Feeding or Cupfeeding and Their Effect on Breastfeeding. Pediatrics 2003, 111, 511–518. [Google Scholar] [CrossRef]
- Kronborg, H.; Vaeth, M. How Are Effective Breastfeeding Technique and Pacifier Use Related to Breastfeeding Problems and Breastfeeding Duration? Birth 2009, 36, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Kair, L.R.; Kenron, D.; Etheredge, K.; Jaffe, A.C.; Phillipi, C.A. Pacifier Restriction and Exclusive Breastfeeding. Pediatrics 2013, 131, e1101–e1107. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, N.R.; Tanabe, K.O.; Siadaty, M.S.; Hauck, F.R. Pacifiers and Breastfeeding: A Systematic Review. Arch. Pediatr. Adolesc. Med. 2009, 163, 378–382. [Google Scholar] [CrossRef] [Green Version]
- Jaafar, S.H.; Ho, J.J.; Jahanfar, S.; Angolkar, M. Effect of Restricted Pacifier Use in Breastfeeding Term Infants for Increasing Duration of Breastfeeding. Cochrane Database Syst. Rev. 2016, 8, CD007202. [Google Scholar] [CrossRef] [PubMed]
- Karabulut, E.; Yalçın, S.; Ozdemir-Geyik, P.; Karaagaoglu, E. Effect of Pacifier Use on Exclusive and Any Breastfeeding: A Meta-Analysis. Turk. J. Pediatr. 2009, 51, 35–43. [Google Scholar] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 Explanation and Elaboration: Updated Guidance and Exemplars for Reporting Systematic Reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Indicators for Assessing Infant and Young Child Feeding Practices. Available online: http://webcache.googleusercontent.com/search?q=cache:F7HQw7Kazg8J:whqlibdoc.who.int/publications/2008/9789241596664_eng.pdf+&cd=1&hl=el&ct=clnk&gl=gr (accessed on 16 June 2022).
- Quality Assessment Tool for Quantitative Studies. Effective Public Healthcare Panacea Project. Available online: https://www.ephpp.ca/quality-assessment-tool-for-quantitative-studies/ (accessed on 17 June 2022).
- Maastrup, R.; Hansen, B.M.; Kronborg, H.; Bojesen, S.N.; Hallum, K.; Frandsen, A.; Kyhnaeb, A.; Svarer, I.; Hallström, I. Breastfeeding Progression in Preterm Infants Is Influenced by Factors in Infants, Mothers and Clinical Practice: The Results of a National Cohort Study with High Breastfeeding Initiation Rates. PLoS ONE 2014, 9, e108208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maastrup, R.; Hansen, B.M.; Kronborg, H.; Bojesen, S.N.; Hallum, K.; Frandsen, A.; Kyhnaeb, A.; Svarer, I.; Hallström, I. Factors Associated with Exclusive Breastfeeding of Preterm Infants. Results from a Prospective National Cohort Study. PLoS ONE 2014, 9, e89077. [Google Scholar] [CrossRef] [PubMed]
- Dadalto, E.C.V.; Rosa, E.M. Factors Associated to Pacifier Use in Preterm Infants. Rev. CEFAC 2016, 18, 601–612. [Google Scholar] [CrossRef]
- Carcavalli, L.; Martins, C.C.; Rocha, I.A.; Parlato, E.M.; Serra-Negra, J.M. Preterm Birth, Pacifier Use and Breastfeeding: Is There a Relationship? Braz. Dent. J. 2018, 29, 388–394. [Google Scholar] [CrossRef]
- Say, B.; Simsek, G.K.; Canpolat, F.E.; Oguz, S.S. Effects of Pacifier Use on Transition Time from Gavage to Breastfeeding in Preterm Infants: A Randomized Controlled Trial. Breastfeed. Med. 2018, 13, 433–437. [Google Scholar] [CrossRef]
- Fucile, S.; Wener, E.; Dow, K. Enhancing Breastfeeding Establishment in Preterm Infants: A Randomized Clinical Trial of Two Non-Nutritive Sucking Approaches. Early Hum. Dev. 2021, 156, 105347. [Google Scholar] [CrossRef]
- Maastrup, R.; Rom, A.L.; Walloee, S.; Sandfeld, H.B.; Kronborg, H. Improved exclusive breastfeeding rates in preterm infants after a neonatal nurse training program focusing on six breastfeeding-supportive clinical practices. PLoS ONE 2021, 16, e0245273. [Google Scholar] [CrossRef]
- Kaya, V.; Aytekin, A. Effects of Pacifier Use on Transition to Full Breastfeeding and Sucking Skills in Preterm Infants: A Randomised Controlled Trial. J. Clin. Nurs. 2017, 26, 2055–2063. [Google Scholar] [CrossRef] [PubMed]
- Tolppola, O.; Renko, M.; Sankilampi, U.; Kiviranta, P.; Hintikka, L.; Kuitunen, I. Pacifier Use and Breastfeeding in Term and Preterm Newborns—A Systematic Review and Meta-Analysis. Eur. J. Pediatr. 2022, 181, 3421–3428. [Google Scholar] [CrossRef]
- Task Force on Sudden Infant Death Syndrome. The Changing Concept of Sudden Infant Death Syndrome: Diagnostic Coding Shifts, Controversies Regarding the Sleeping Environment, and New Variables to Consider in Reducing Risk. Pediatrics 2005, 116, 1245–1255. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author/Year | Selection Bias | Study Design | Confounders | Blinding | Data Collection Methods | Withdrawals and Drops Out | Final Score |
|---|---|---|---|---|---|---|---|
| 1. Maastrup (2014) [40] | Strong | Moderate | Moderate | Weak | Strong | Strong | Moderate |
| 2. Maastrup (2014) [41] | Strong | Moderate | Moderate | Weak | Strong | Strong | Moderate |
| 3. Dadalto (2016) [42] | Moderate | Moderate | Strong | Strong | Strong | Strong | Strong |
| 4. Carcavalli (2018) [43] | Moderate | Strong | Strong | Moderate | Strong | Strong | Strong |
| 5. Kamhawy (2014) [13] | Moderate | Strong | Strong | Strong | Strong | Strong | Strong |
| 7. Say (2018) [44] | Moderate | Strong | Moderate | Strong | Strong | Strong | Strong |
| 8. Fucile (2021) [45] | Moderate | Strong | Strong | Strong | Strong | Strong | Strong |
| 9. Maastrup (2021) [46] | Strong | Strong | Strong | Strong | Strong | Strong | Strong |
| 10. Shaki (2022) [5] | Moderate | Strong | Strong | Moderate | Strong | Strong | Strong |
| Author/ Country | Design | N | Data | Exposure | Outcome | Outcome Age | Effect of Pacifier Use | Additional Factors |
|---|---|---|---|---|---|---|---|---|
| 1. Maastrup (2014) [40] Denmark | Prospective | 1221 mothers and their 1.488 preterm infants | A national Danish cohort of preterm infants | Pacifier use during breastfeeding transition from neonates 24–36 gestational weeks who were admitted to a NICU | Minimizing the use of a pacifier during breastfeeding transition were associated with earlier establishment of exclusive breastfeeding | 1, 4, 6 and 12 months of chronological and corrected age. | Negative | Low gestational age, multiple birth, mechanically ventilated infant, primiparity, initiating breast milk expression later than 24 h after delivery |
| 2. Maastrup(2014) [41] Denmark | Prospective | 1205 preterm infants | A national Danish cohort of preterm infants | Pacifier use during breastfeeding transition from preterm neonates with a gestational age of 24–36 weeks | Pacifier use was associated with failure of exclusive breastfeeding | 1, 4, 6 and 12 months of chronological and corrected age | Negative | Nipple shields, Delayed initiation of breast milk expression |
| 4. Carcavalli (2018) Brazil [43] | Retrospective comparative Cross-sectional | 250 children into two groups | Public hospital and public day-care centre in Belo Horizonte, southwest Brazil | Pacifier use in preterm and full-term infants | Pacifier use was more prevalent among preterm infants and was associated with less than six months of breastfeeding and use of bottle | 3 to 5 years | Negative | Low monthly family income |
| 7. Say (2018) [44] Turkey | Prospective, randomized controlled trial | 90 Infants in 2 groups (pacifier and control) < 32 weeks | NICU University of Health Sciences Zekai Tahir Burak | Pacifier use in preterm infants up to switching to full breastfeeding | The time for transition to full breastfeeding was shorter in pacifier group infants | Hospital discharge | Positive | |
| 8. Fucile (2021) [45] Canada | Randomized | 33 preterm infants < 34 weeks | NICU at Kingston Health Science Centre | Pacifier use or emptied breast from mothers in NICU | Infants in the group of emptied breast sucking acquired exclusive breastfeeds at hospital discharge as compared with those in the pacifier group | Hospital discharge | Negative | |
| 9. Maastrup(2021) [46] Denmark | Intervention study | 420 and 494 preterm mother-infant dyads in training program | 17 Danish NICUs and one children’s department | Minimizing use of pacifiers | Exclusive breastfeeding rates at discharge from the NICU to home | Hospital discharge | Negative | |
| 10. Shaki (2022) [5] Iran | Single-blind randomized controlled clinical trial | 150 preterm infants with the gestational age of 31 to 33 weeks | NICU in Babol Rouhani Hospital, Iran | Finger use or pacifier use or nothing | Breastfeeding Behavior Scale score | Day 10 of interventions | Positive |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orovou, E.; Tzitiridou-Chatzopoulou, M.; Dagla, M.; Eskitzis, P.; Palaska, E.; Iliadou, M.; Iatrakis, G.; Antoniou, E. Correlation between Pacifier Use in Preterm Neonates and Breastfeeding in Infancy: A Systematic Review. Children 2022, 9, 1585. https://doi.org/10.3390/children9101585
Orovou E, Tzitiridou-Chatzopoulou M, Dagla M, Eskitzis P, Palaska E, Iliadou M, Iatrakis G, Antoniou E. Correlation between Pacifier Use in Preterm Neonates and Breastfeeding in Infancy: A Systematic Review. Children. 2022; 9(10):1585. https://doi.org/10.3390/children9101585
Chicago/Turabian StyleOrovou, Eirini, Maria Tzitiridou-Chatzopoulou, Maria Dagla, Panagiotis Eskitzis, Ermioni Palaska, Maria Iliadou, Georgios Iatrakis, and Evangelia Antoniou. 2022. "Correlation between Pacifier Use in Preterm Neonates and Breastfeeding in Infancy: A Systematic Review" Children 9, no. 10: 1585. https://doi.org/10.3390/children9101585