
How Do Children with Autism Spectrum Disorder and Children with Developmental Delays Differ on the Child Behavior Checklist 1.5–5 DSM-Oriented Scales?


Abstract
:1. Introduction
1.1. Factor Structure of CBCL DSM-Oriented Scales with ASD and DD
1.2. The Application of Differential Item Functioning with Screening
1.3. The Present Study
2. Materials and Methods
2.1. Participants
2.2. Procedure and Measures
2.3. Data Analysis
2.3.1. Measurement Invariance
2.3.2. Differential Item Functioning
3. Results
3.1. Descriptive Statistics
3.2. Reliability Estimates
3.3. Measurement Invariance
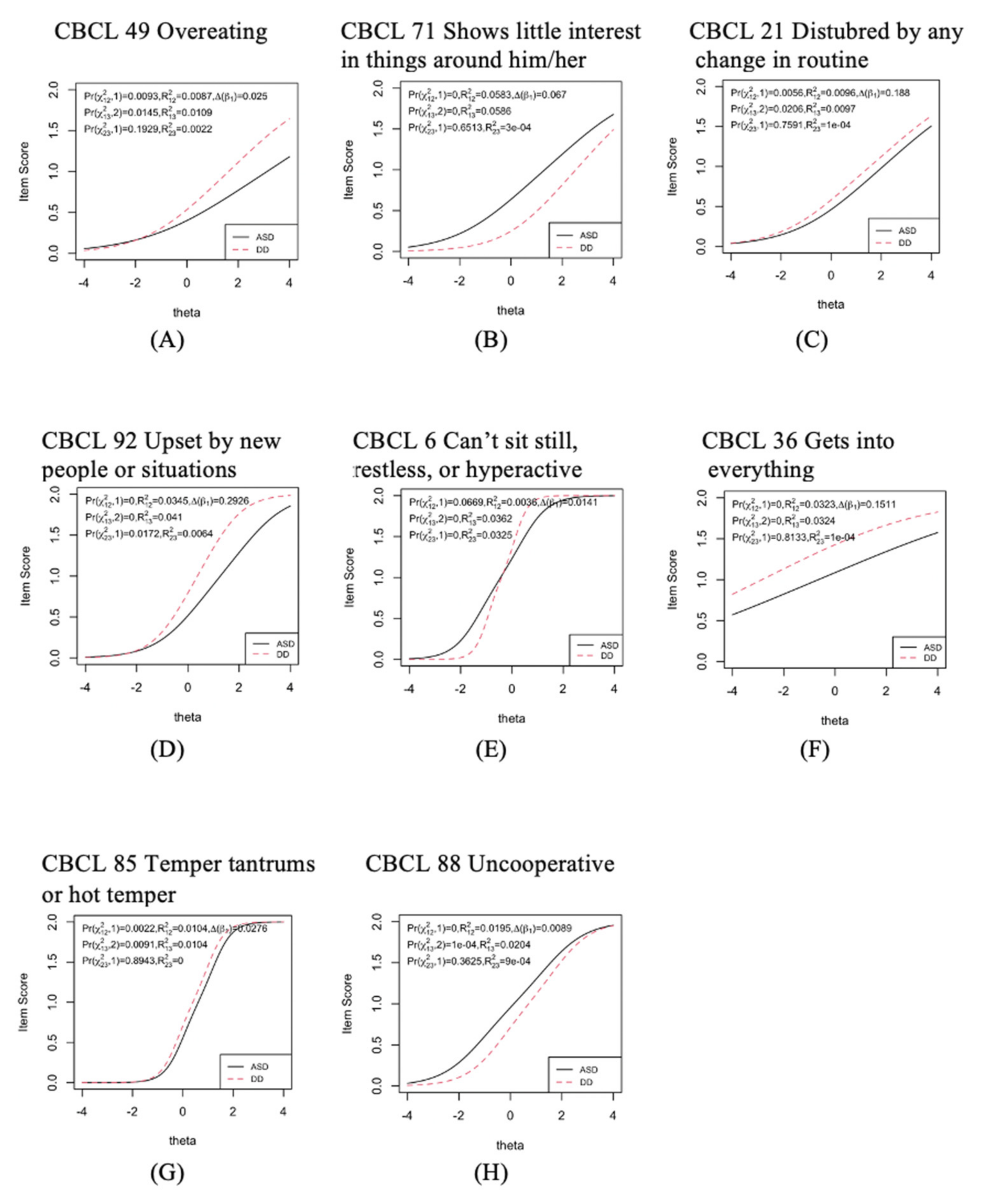
3.4. Differential Item Functioning
4. Discussion
Limitation and Implication
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Subscales Item Loadings | Affective Problems | Subscales Item Loadings | Anxiety Problems ASD DD | Subscales Item Loadings | Pervasive Developmental Problems |
|---|---|---|---|---|---|
| 13. cries a lot | 0.503 (0.053) | 10. clings to adults or too dependent | 0.490 (0.071) 0.552 (072) | 3. afraid to try new things | 0.465 (0.050) |
| 24. doesn’t eat well | 0.394 (0.057) | 22. doesn’t want to sleep alone | 0.276 (0.082) 0.386 (0.084) | 4. avoids looking others in the eye | 0.576 (0.048) |
| 38. has trouble getting to sleep | 0.698 (0.052) | 28. doesn’t want to go out of home | 0.460 (0.093) 0.423 (0.086) | 7. can’t stand having things out of place | 0.290 (0.055) |
| 43. looks unhappy without good reason | 0.665 (0.058) | 32. fears certain animals, situations, or places | 0.603 (0.059) 0.249 (0.086) | 21. disturbed by any change in routine | 0.418 (0.054) |
| 49. overeating | 0.381 (0.061) | 37. gets too upset when separated from parents | 0.478 (0.068) 0.544 | 23. doesn’t answer when people talk to him/her | 0.495 (0.052) |
| 50. overtired | 0.747 (0.053) | 47. nervous, highstrung, or tense | 0.829 (0.045) 0.776 (0.061) | 25. doesn’t get along with other children | 0.621 (0.049) |
| 71. shows little interest in things around him/her | 0.434 (0.058) | 48. nightmares | 0.426 (0.079) 0.591 (0.067) | 63. repeatedly rocks head or body | 0.326 (0.054) |
| 74. sleeps less than most kids during day and/or night | 0.722 (0.050) | 51. shows panic for no good reason | 0.788 (0.053) 0.695 (0.069) | 67. seems unresponsive to affection | 0.586 (0.047) |
| 89. underactive, slow moving, or lacks energy | 0.664 (0.056) | 87. too fearful or anxious | 0.816 (0.052) 0.790 (0.051) | 70. shows little affection toward people | 0.606 (0.045) |
| 90. unhappy, sad, or depressed | 0.857 (0.056) | 99. worries | 0.803 (0.068) 0.852 (0.073) | 76. speech problem | 0.282 (0.064) |
| 80. strange behavior | 0.490 (0.054) | ||||
| 92. upset by new people or situations | 0.564 (0.045) | ||||
| 98. withdrawn, doesn’t get involved with others | 0.717 (0.043) | ||||
| Subscales Item Loadings | Attention-Deficit/Hyperactive Problems | Subscales Item Loadings | Anxiety Problems | ||
| 5. can’t concentrate, can’t pay attention for long | 0.780 (0.033) | 15. defiant | 0.426 (0.035) | ||
| 6. can’t sit still, restless, or hyperactive | 0.776 (0.034) | 20. disobedient | 0.730 (0.036) | ||
| 8. can’t stand waiting; wants everything now | 0.812 (0.036) | 44. angry moods | 0.739 (0.039) | ||
| 16. demands must be met immediately | 0.778 (0.038) | 81. stubborn, sullen, or irritable | 0.812 (0.035) | ||
| 36. gets into everything | 0.209 (0.054) | 85. temper tantrums or hot temper | 0.870 (0.030) | ||
| 59. quickly shifts from one activity to another | 0.376 (0.049) | 88. uncooperative | 0.599 (0.042) |
References
- Werner, E.; Dawson, G.; Munson, J.; Osterling, J. Variation in early developmental course in autism and its relation with behavioral outcome at 3–4 years of age. J. Autism Dev. Disord. 2005, 35, 337–350. [Google Scholar] [CrossRef]
- Achenbach, T.M.; Dumenci, L.; Rescorla, L.A. DSM-oriented and empirically based approaches to constructing scales from the same item pools. J. Clin. Child Adolesc. Psychol. 2003, 32, 328–340. [Google Scholar] [CrossRef] [PubMed]
- Chericoni, N.; Balboni, G.; Costanzo, V.; Mancini, A.; Prosperi, M.; Lasala, R.; Tancredi, R.; Scattoni, M.L.; NIDA Network; Muratori, F.; et al. A combined study on the use of the Child Behavior Checklist 1½–5 for identifying autism spectrum disorders at 18 months. J. Autism Dev. Disord. 2021, 51, 3829–3842. [Google Scholar] [CrossRef]
- Rescorla, L.A.; Adams, A.; Ivanova, M.Y.; International ASEBA Consortium. The CBCL/1½–5′s DSM-ASD scale: Confirmatory factor analyses across 24 societies. J. Autism Dev. Disord. 2020, 50, 3326–3340. [Google Scholar] [CrossRef] [PubMed]
- Dovgan, K.; Mazurek, M.O.; Hansen, J. Measurement invariance of the Child Behavior Checklist in children with autism spectrum disorder with and without intellectual disability: Follow-up study. Res. Autism Spectr. Disord. 2019, 58, 19–29. [Google Scholar] [CrossRef]
- Murray, A.L.; Booth, T.; McKenzie, K.; Kuenssberg, R.; O’Donnell, M. Are autistic traits measured equivalently in individuals with and without an autism spectrum disorder? An invariance analysis of the Autism Spectrum Quotient Short Form. J. Autism Dev. Disord. 2014, 44, 55–64. [Google Scholar] [CrossRef] [Green Version]
- Rescorla, L.A.; Ghassabian, A.; Ivanova, M.Y.; Jaddoe, V.W.; Verhulst, F.C.; Tiemeier, H. Structure, longitudinal invariance, and stability of the Child Behavior Checklist 1½–5′s Diagnostic and Statistical Manual of Mental Disorders–Autism Spectrum Disorder scale: Findings from Generation R (Rotterdam). Autism 2019, 23, 223–235. [Google Scholar] [CrossRef]
- Glod, M.; Creswell, C.; Waite, P.; Jamieson, R.; McConachie, H.; Don South, M.; Rodgers, J. Comparisons of the factor structure and measurement invariance of the Spence Children’s Anxiety Scale—Parent version in children with autism spectrum disorder and typically developing anxious children. J. Autism Dev. Disord. 2017, 47, 3834–3846. [Google Scholar] [CrossRef] [Green Version]
- Bruckner, C.; Yoder, P.; Stone, W.; Saylor, M. Construct validity of the MCDI-I receptive vocabulary scale can be improved: Differential item funtioning between toddlers with autism specturm disorders and typically developing infants. J. Speech Lang. Hear. Res. 2007, 50, 1631–1638. [Google Scholar] [CrossRef]
- Conrad, K.J.; Dennis, M.L.; Bezruczko, N.; Funk, R.R.; Riley, B.B. Substance use disorder symptoms: Evidence of differential item funtioning by age. J. Appl. Meas. 2007, 8, 373–387. [Google Scholar]
- Geri, T.; Piscitelli, D.; Meroni, R.; Bonetti, F.; Giovannico, G.; Traversi, R.; Testa, M. Rasch analysis of the Neck Bournemouth Questionnaire to measure disability related to chronic neck pain. J. Rehabil. Med. 2015, 47, 836–843. [Google Scholar] [CrossRef] [Green Version]
- Pellicciari, L.; Piscitelli, D.; Basagni, B.; De Tanti, A.; Algeri, L.; Caselli, S.; Ciurli, M.P.; Conforti, J.; Estraneo, A.; Moretta, P.; et al. ‘Less is more’: Validation with Rasch analysis of five short-forms for the Brain Injury Rehabilition Trust Personality Questionnaires (BIRT-PQs). Brain Injury 2020, 34, 1741–1755. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.W.; Gibbons, L.E.; Crane, P.K. Lordif: An R package for detecting differential item functioning using iterative hybrid ordinal logistic regression/item response theory and Monte Carlo simulations. J. Stat. Softw. 2011, 39, 1–30. [Google Scholar] [CrossRef] [Green Version]
- Mazefsky, C.A.; Yu, L.; White, S.W.; Siegel, M.; Pilkonis, P.A. The Emotion Dysregulation Inventory: Psychometric properties and item response theory calibration in an autism spectrum disorder sample. Autism Res. 2018, 11, 928–941. [Google Scholar] [CrossRef] [PubMed]
- Agelink van Rentergem, J.A.; Lever, A.G.; Geurts, H.M. Negatively phrased items of the Autism Spectrum Quotient function differently for groups with and without autism. Autism 2019, 23, 1752–1764. [Google Scholar] [CrossRef] [Green Version]
- McClain, M.B.; Harris, B.; Schwartz, S.E.; Golson, M.E. Differential item and test functioning of the Autism Spectrum Rating Scales: A follow-up evaluation in a diverse, nonclinical sample. J. Psychoeduc. Assess. 2021, 39, 247–257. [Google Scholar] [CrossRef]
- Lazenby, D.C.; Sideridis, G.D.; Huntington, N.; Prante, M.; Dale, P.S.; Curtin, S.; Henkel, L.; Iverson, J.M.; Carver, L.; Dobkins, K.; et al. Language differences at 12 months in infants who develop autism spectrum disorder. J. Autism Dev. Disord. 2016, 46, 899–909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Visser, L.; Vlaskamp, C.; Emde, C.; Ruiter, S.A.J.; Timmerman, M.E. Difference or delay? A comparison of Bayley-III Cognition item scores of young children with and without developmental disabilities. Res. Dev. Disabil. 2017, 71, 109–119. [Google Scholar] [CrossRef] [Green Version]
- Lord, C.; Rutter, M.; DiLavore, P.C.; Risi, S. Autism Diagnostic Observation Schedule (ADOS); Western Psychological Services: Los Angeles, CA, USA, 1999; ISBN 978-192-202-187-8. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Pub: Washington, DC, USA, 2013; ISBN 978-089-042-555-8. [Google Scholar]
- Mullen, E. Mullen Scales of Early Learning; American Guidance Service: Circle Pines, MN, USA, 1995. [Google Scholar]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA Preschool Forms and Profiles; University of Vermont, Research Center for Children, Youth, and Families: Burlington, VT, USA, 2000; ISBN 978-093-856-568-0. [Google Scholar]
- Leung, P.W.L.; Wong, M.M.T. Measures of child and adolescent psychopathology in Asia. Psychol. Assess. 2003, 15, 268–279. [Google Scholar] [CrossRef]
- Wu, Y.T.; Chen, W.J.; Hsieh, W.S.; Chen, P.C.; Liao, H.F.; Su, Y.N.; Jeng, S.F. Maternal-reported behavioral and emotional problems in Taiwanese preschool children. Res. Dev. Disabil. 2012, 33, 866–873. [Google Scholar] [CrossRef]
- American Educational Research Association; American Psychological Association; National Council on Measurement in Education. Standards for Educational and Psychological Testing; American Educational Research Association: Washington, DC, USA, 2014; ISBN 978-093-530-235-6. [Google Scholar]
- Jackson, P.H.; Agunwamba, C.C. Lower bounds for the reliability of the total score on a test composed of non-homogeneous items. I: Algebraic lower bounds. Psychometrika 1977, 42, 567–578. [Google Scholar] [CrossRef]
- Sijtsma, K. On the use, the misuse, and the very limited usefulness of Cronbach’s alpha. Psychometrika 2009, 74, 107–120. [Google Scholar] [CrossRef] [Green Version]
- Wagenmakers, E.J.; Marsman, M.; Jamil, T.; Ly, A.; Verhagen, J.; Love, J.; Selker, R.; Gronau, Q.F.; Šmíra, M.; Epskamp, S.; et al. Bayesian inference for psychology. Part I: Theoretical advantages and practical ramifications. Psychon. Bull. Rev. 2018, 25, 35–57. [Google Scholar] [CrossRef]
- Vandenberg, R.J.; Lance, C.E. A review and synthesis of the measurement invariance literature: Suggestions, practices, and recommendations for organizational research. Organ. Res. Methods 2000, 3, 4–70. [Google Scholar] [CrossRef]
- Sass, D.A. Testing measurement invariance and comparing latent factor means within a confirmatory factor analysis framework. J. Psychoeduc. Assess. 2011, 29, 347–363. [Google Scholar] [CrossRef]
- Cheung, G.W.; Rensvold, R.B. Evaluating goodness-of-fit indexes for testing measurement invariance. Struc. Equ. Modeling 2002, 9, 233–255. [Google Scholar] [CrossRef]
- Hirschfeld, G.; von Brachel, R. Improving multiple-group confirmatory factor analysis in R–A tutorial in measurement invariance with continuous and ordinal indicators. Pract. Assess. Res. Evaluation 2014, 19, 7. [Google Scholar] [CrossRef]
- Rosseel, Y. Lavaan: An R package for structural equation modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 7th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2012; ISBN 978-098-299-830-4. [Google Scholar]
- Svetina, D.; Rutkowski, L.; Rutkowski, D. Multiple-group invariance with categorical outcomes using updated guidelines: An illustration using Mplus and the lavaan/semTools packages. Struc. Equ. Modeling 2020, 27, 111–130. [Google Scholar] [CrossRef]
- Li, C.H. Confirmatory factor analysis with ordinal data: Comparing robust maximum likelihood and diagonally weighted least squares. Behav. Res. 2016, 48, 936–949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sass, D.A.; Schmitt, T.A.; Marsh, H.W. Evaluating model fit with ordered categorical data within a measurement invariance framework: A comparison of estimators. Struc. Equ. Modeling 2014, 21, 167–180. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struc. Equ. Modeling 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Iacobucci, D. Structural equations modeling: Fit indices, sample size, and advanced topics. J. Consum. Psychol. 2010, 20, 90–98. [Google Scholar] [CrossRef]
- Chen, F.F. Sensitivity of goodness of fit indexes to lack of measurement invariance. Struc. Equ. Modeling 2007, 14, 464–504. [Google Scholar] [CrossRef]
- Meade, A.W.; Johnson, E.C.; Braddy, P.W. Power and sensitivity of alternative fit indices in tests of measurement invariance. J. Appl. Psychol. 2008, 93, 568–592. [Google Scholar] [CrossRef]
- Raykov, T.; Marcoulides, G.A. A First Course in Structural Equation Modeling, 2nd ed.; Routledge: New York, NY, USA, 2006; ISBN 978-080-585-588-3. [Google Scholar]
- Gregorich, S.E. Do self-report instruments allow meaningful comparisons across diverse population groups? Testing measurement invariance using the confirmatory factor analysis framework. Med. Care 2006, 44, S78–S94. [Google Scholar] [CrossRef] [PubMed]
- Millsap, R.E.; Kwok, O.M. Evaluating the impact of partial factorial invariance on selection in two populations. Psychol. Methods 2004, 9, 93–115. [Google Scholar] [CrossRef]
- Vasa, R.A.; Keefer, A.; McDonald, R.G.; Hunsche, M.C.; Kerns, C.M. A scoping review of anxiety in young children with autism spectrum disorder. Autism Res. 2020, 13, 2038–2057. [Google Scholar] [CrossRef]
- Gotham, K.; Brunwasser, S.M.; Lord, C. Depressive and anxiety symptom trajectories from school age through young adulthood in samples with autism spectrum disorder and developmental delay. J. Am. Acad. Child Adolesc. Psychiatry 2015, 54, 369–376.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rescorla, L.A.; Kim, Y.A.; Oh, K.J. Screening for ASD with the Korean CBCL/1½–5. J. Autism Dev. Disord. 2015, 45, 4039–4050. [Google Scholar] [CrossRef] [PubMed]
- Predescu, E.; Sipos, R.; Dobrean, A.; Miclutia, I. The discriminative power of the CBCL 1½–5 between autism spectrum disorders and other psychiatric disorders. J. Cogn. Behav. Psychother. Res. 2013, 13, 71–83. [Google Scholar]
- Prosperi, M.; Santocchi, E.; Balboni, G.; Narzisi, A.; Bozza, M.; Fulceri, F.; Apicella, F.; Igliozzi, R.; Cosenza, A.; Tancredi, R.; et al. Behavioral phenotype of ASD preschoolers with gastrointestinal symptoms or food selectivity. J. Autism Dev. Disord. 2017, 47, 3574–3588. [Google Scholar] [CrossRef]
- Nadeau, M.V.; Richard, E.; Wallace, G.L. The combination of food approach and food avoidant behaviors in children with autism spectrum disorder: “Selective overeating”. J. Autism Dev. Disord. 2021. [Google Scholar] [CrossRef] [PubMed]
- McDonald, J.L.; Milne, S.; Knight, J.; Webster, V. Developmental and behavioural characteristics of children enrolled in a child protection pre-school. J. Paediatr. Child Health 2013, 49, E142–E146. [Google Scholar] [CrossRef] [PubMed]
- Regier, D.A.; Kuhl, E.A.; Kupfer, D.J. The DSM-5: Classification and criteria changes. World Psychiatry. 2013, 12, 92–98. [Google Scholar] [CrossRef] [Green Version]
- McClain, M.B.; Harris, B.; Schwartz, S.E.; Golson, M.E. Evaluation of the Autism Spectrum Rating Scales in a diverse, nonclinical sample. J. Psychoeduc. Assess. 2020, 38, 740–752. [Google Scholar] [CrossRef]
- Ekermans, G.; Saklofske, D.H.; Austin, E.; Stough, C. Measurement invariance and differential item functioning of the Bar-On EQ-i: S measure over Canadian, Scottish, South African and Australian samples. Pers. Individ. Dif. 2011, 50, 286–290. [Google Scholar] [CrossRef]
- Randall, J.; Cheong, Y.F.; Engelhard, G., Jr. Using explanatory item response theory modeling to investigate context effects of differential item functioning for students with disabilities. Educ. Psychol. Meas. 2011, 71, 129–147. [Google Scholar] [CrossRef]

| ASD (n = 228) | DD (n = 215) | p | |
|---|---|---|---|
| CA (months) | |||
| Mean (SD) | 32.28 (9.16) | 30.75 (10.10) | 0.097 |
| MA (months) | |||
| Mean (SD) | 21.02 (10.03) | 23.94 (9.21) | 0.002 |
| Reporter | |||
| Mother: Father | 211:17 | 199:16 | 0.995 |
| Parents’ years of education | |||
| Mean (SD): mother | 14.52 (2.39) | 14.03 (2.55) | 0.037 |
| Mean (SD): father | 14.56 (2.51) | 13.65 (2.73) | <0.001 |
| ADOS total scores a | |||
| Mean (SD): Module 1 | 17.19 (3.13) | 3.38 (2.33) | <0.001 |
| Mean (SD): Module 2 | 15.77 (3.09) | 3.00 (1.86) | <0.001 |
| Gender | |||
| Male: female | 203:25 | 148:67 | <0.001 |
| df | Test | RMSEA (Δ RMSEA) | SRMR (Δ SRMR) | CFI (Δ CFI) | ||
|---|---|---|---|---|---|---|
| Aff | ||||||
| Configural | 145.691 | 70 | 0.070 | 0.094 | 0.920 | |
| Configural vs. Metric * | 147.711 (2.02) | 79(9) | 0.358 | 0.063 (−0.007) | 0.099 (0.005) | 0.927 (0.007) |
| Metric vs. Scalar | 193.702 (45.991) | 88(9) | <0.001 | 0.074 (0.011) | 0.099 (0) | 0.888 (0.039) |
| Anx | ||||||
| Configural * | 134.905 | 70 | 0.065 | 0.089 | 0.944 | |
| Configural vs. Metric | 157.449 (22.544) | 79(9) | 0.019 | 0.067 (0.002) | 0.101 (0.012) | 0.932 (−0.012) |
| Metric vs. Scalar | NA | NA | NA | NA | NA | NA |
| PDP | ||||||
| Configural | 334.265 | 130 | 0.084 | 0.104 | 0.830 | |
| Configural vs. Metric * | 320.441 (−13.824) | 142(12) | 0.48 | 0.075 (−0.009) | 0.108 (0.004) | 0.852 (0.022) |
| Metric vs. Scalar | 368.433 (47.992) | 154(12) | <0.001 | 0.079 (0.004) | 0.108(0) | 0.822 (−0.030) |
| ADHP | ||||||
| Configural | 190.997 | 18 | 0.209 | 0.129 | 0.871 | |
| Configural vs. Metric * | 186.431 (−4.236) | 23(5) | 0.13 | 0.180 (−0.029) | 0.132 (0.003) | 0.878 (0.007) |
| Metric vs. Scalar | 233.757 (47.326) | 28(5) | <0.0001 | 0.183 (0.03) | 0.130 (−0.002) | 0.847 (−0.031) |
| ODP | ||||||
| Configural | 64.899 | 18 | 0.109 | 0.059 | 0.966 | |
| Configural vs. Metric * | 59.243 (−5.656) | 23(5) | 0.38 | 0.085 (−0.024) | 0.064 (0.005) | 0.973 (0.007) |
| Metric vs. Scalar | 98.809 (39.566) | 28(5) | 0.0001 | 0.107 (0.022) | 0.062 (−0.002) | 0.948 (−0.025) |
| It is non invariant if… | ≥0.015 | ≥0.030 | ≥−0.010 |
| Subscale | Items |
|---|---|
| Affective Problems | CBCL 49 Overeating |
| CBCL 71 Shows little interest in things around him/her | |
| Pervasive Developmental Problems | CBCL 21 Disturbed by any change in routine |
| CBCL 92 Upset by new people or situations | |
| Attention Deficit/Hyperactive Problems | CBCL 6 Can’t sit still, restless, or hyperactive |
| CBCL 36 Gets into everything | |
| Oppositional Defiant Problems | CBCL 85 Temper tantrums or hot temper |
| CBCL 88 Uncooperative |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, Y.-L.; Chu, C.-L.; Wu, C.-C. How Do Children with Autism Spectrum Disorder and Children with Developmental Delays Differ on the Child Behavior Checklist 1.5–5 DSM-Oriented Scales? Children 2022, 9, 111. https://doi.org/10.3390/children9010111
Cheng Y-L, Chu C-L, Wu C-C. How Do Children with Autism Spectrum Disorder and Children with Developmental Delays Differ on the Child Behavior Checklist 1.5–5 DSM-Oriented Scales? Children. 2022; 9(1):111. https://doi.org/10.3390/children9010111
Chicago/Turabian StyleCheng, Yi-Ling, Ching-Lin Chu, and Chin-Chin Wu. 2022. "How Do Children with Autism Spectrum Disorder and Children with Developmental Delays Differ on the Child Behavior Checklist 1.5–5 DSM-Oriented Scales?" Children 9, no. 1: 111. https://doi.org/10.3390/children9010111