
The Assessment of Brain Volume Differences in Idiopathic Central Precocious Puberty Girls; Comparison of Age-Matched Girls and Normal Puberty Girls


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Data Acquisition
2.3. Postprocessing and Statistical Analysis
3. Results
3.1. Clinical Characteristics
3.2. Total Intracranial Volume (TICV)
3.3. Regional Volume Difference
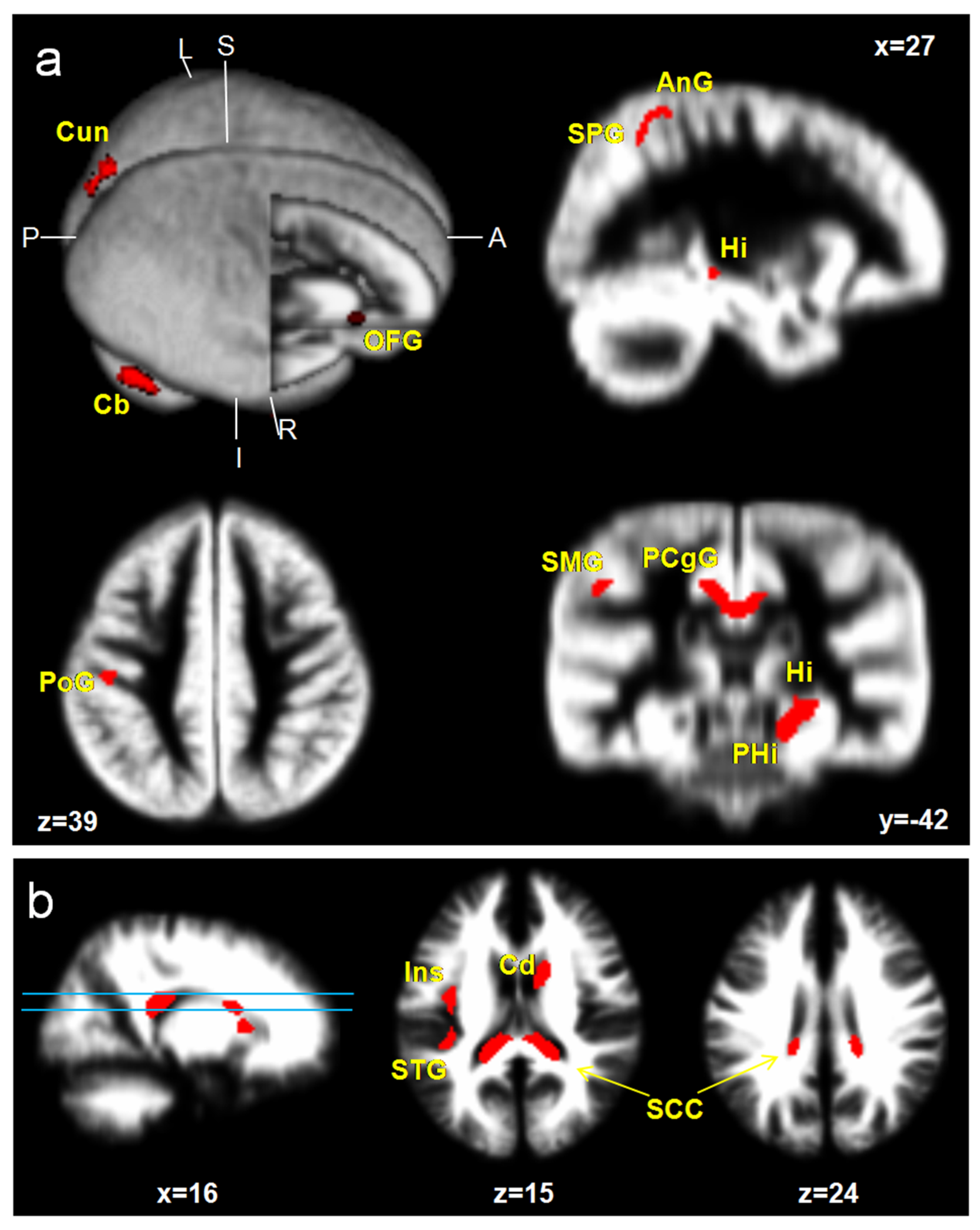
3.3.1. ICPP vs. Age-Matched Control
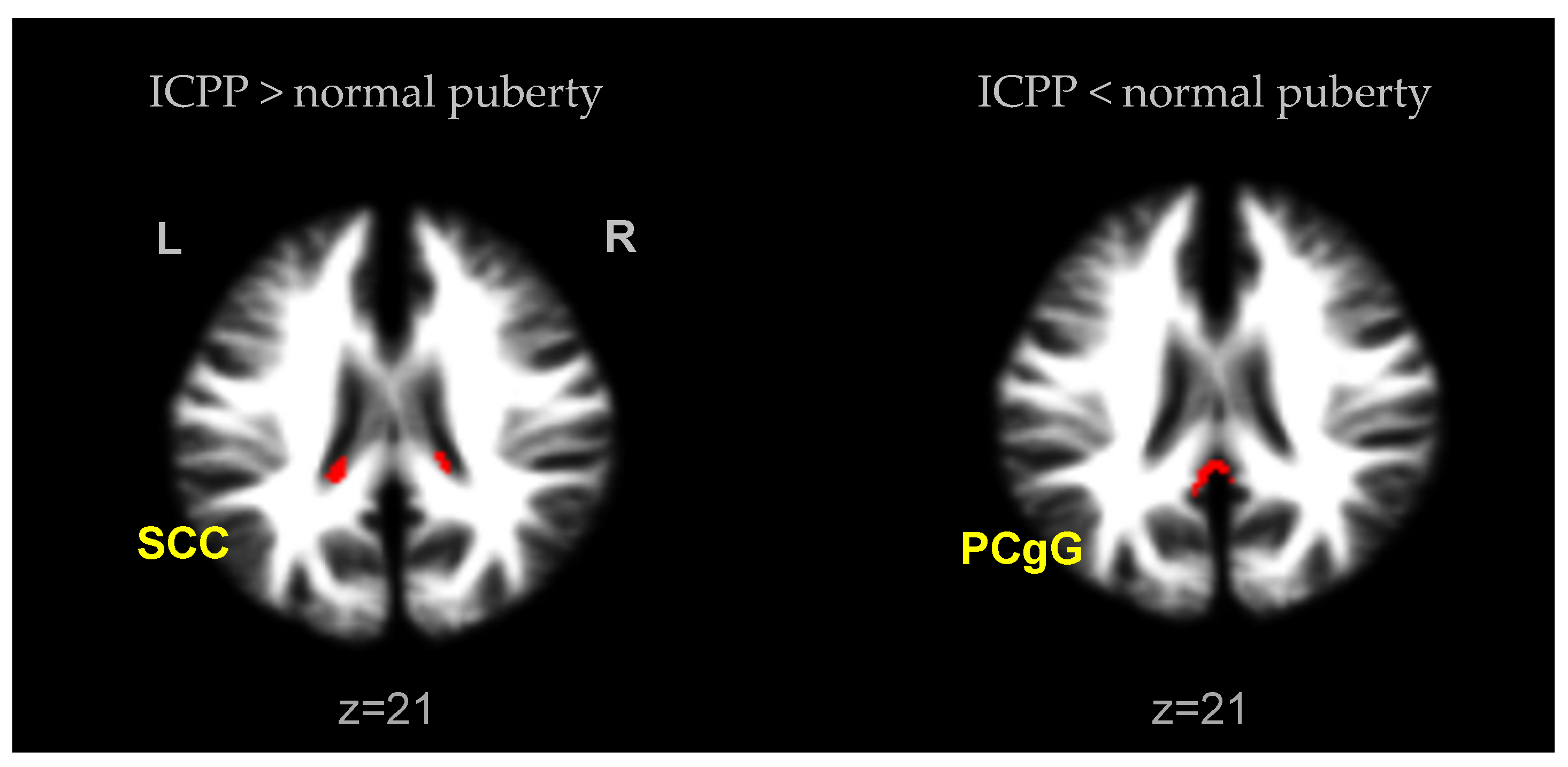
3.3.2. ICPP vs. Normal Puberty Control
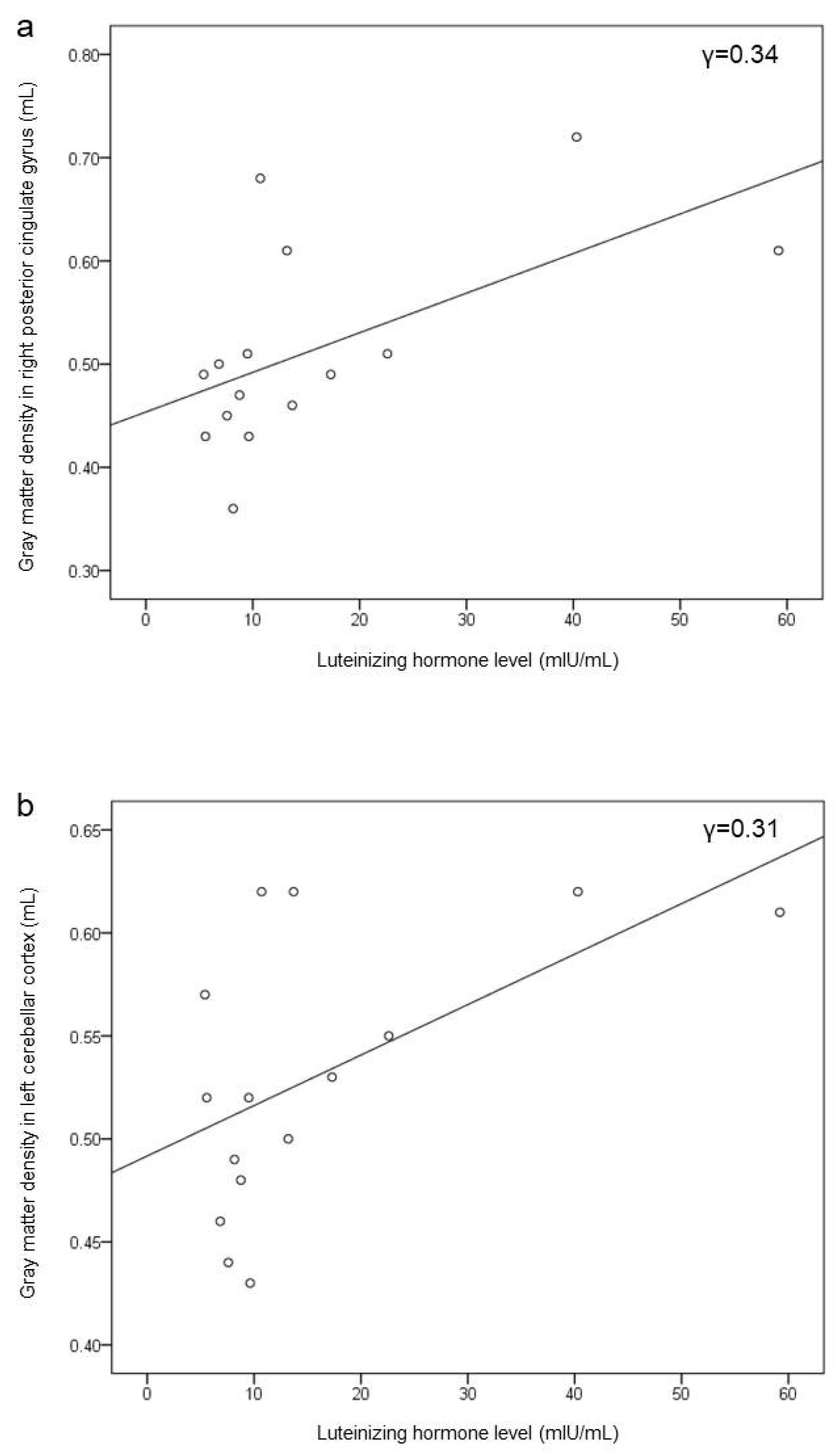
3.4. Correlation of Brain Volume with LH Level
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Berberoglu, M. Precocious Puberty and Normal Variant Puberty: Definition, etiology, diagnosis and current management–Review. J. Clin. Res. Pediatr. Endocrinol. 2009, 1, 164–174. [Google Scholar] [CrossRef] [PubMed]
- Kaplowitz, P.B.; Oberfield, S.E. Reexamination of the age limit for defining when puberty is precocious in girls in the United States: Implications for evaluation and treatment. Drug and Therapeutics and Executive Committees of the Lawson Wilkins Pediatric Endocrine Society. Pediatrics 1999, 104, 936–941. [Google Scholar] [CrossRef] [PubMed]
- Herman-Giddens, M.E.; Slora, E.J.; Wasserman, R.C.; Bourdony, C.J.; Bhapkar, M.V.; Koch, G.G.; Hasemeier, C.M. Secondary sexual characteristics and menses in young girls seen in office practice: A study from the Pediatric Research in Office Settings network. Pediatrics 1997, 99, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Brooks-Gunn, J.; Petersen, A.C.; Eichorn, D. The study of maturational timing effects in adolescence. J. Youth Adolesc. 1985, 14, 149–161. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.S.; Kim, E.Y. Body image and depression in girls with idiopathic precocious puberty treated with gonadotropin-releasing hormone analogue. Ann. Pediatr. Endocrinol. Metab. 2016, 21, 155–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Natsuaki, M.N.; Klimes-Dougan, B.; Ge, X.; Shirtcliff, E.A.; Hastings, P.D.; Zahn-Waxler, C. Early pubertal maturation and internalizing problems in adolescence: Sex differences in the role of cortisol reactivity to interpersonal stress. J. Clin. Child Adolesc Psychol. 2009, 38, 513–524. [Google Scholar] [CrossRef] [Green Version]
- latronico, A.C.; Brto, V.N.; Carel, J.C. Causes, diagnosis, and treatment of central precious puberty. Lancent Diabetes Endocrnol. 2016, 4, 265–274. [Google Scholar] [CrossRef]
- Carel, J.C.; Leger, J. Clinical practice. Precocious puberty. N. Engl. J. Med. 2008, 358, 2366–2377. [Google Scholar] [CrossRef] [PubMed]
- Shin, Y.-L. An update on the genetic causes of central precocious puberty. Ann. Pediatr. Endocrinol. Metab. 2016, 21, 66–69. [Google Scholar] [CrossRef] [Green Version]
- Willemsen, R.; Elleri, D.; Williams, R.M.; Ong, K.K.; Dunger, P.D. Pros and cons of GnRHa treatment for early puberty in girls. Nat. Rev. Endocrinol. 2014, 10, 352–363. [Google Scholar] [CrossRef] [PubMed]
- Parent, A.-S.; Teilmann, G.; Juul, A.; Skakkebaek, N.E.; Toppari, J.; Bourguignon, J.-P. The Timing of Normal Puberty and the Age Limits of Sexual Precocity: Variations around the World, Secular Trends, and Changes after Migration. Endocr. Rev. 2003, 24, 668–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carel, J.-C.; Eugster, E.A.; Rogol, A.; Ghizzoni, L.; Palmert, M.R.; on behalf of the members of the ESPE-LWPES GnRH Analogs Consensus Conference Group. Consensus Statement on the Use of Gonadotropin-Releasing Hormone Analogs in Children. Pediatrics 2009, 123, e752–e762. [Google Scholar] [CrossRef] [PubMed]
- Giedd, J.N.; Clasen, L.S.; Lenroot, R.; Greenstein, D.; Wallace, G.L.; Ordaz, S.; Molloy, E.A.; Blumenthal, J.D.; Tossell, J.W.; Stayer, C.; et al. Puberty-related influences on brain development. Mol. Cell. Endocrinol. 2006, 254-255, 154–162. [Google Scholar] [CrossRef]
- Chen, T.; Lu, Y.; Wang, Y.; Guo, A.; Xie, X.; Fu, Y.; Shen, B.; Lin, W.; Yang, D.; Zhou, L.; et al. Altered Brain Structure and Functional Connectivity Associated with Pubertal Hormones in Girls with Precocious Puberty. Neural Plast. 2019, 2019, 1–10. [Google Scholar] [CrossRef]
- Cho, A.Y.; Ko, S.Y.; Lee, J.H.; Kim, E.Y. Relationship between final adult height and birth weight after gonadotropin-releasing hormone agonist treatment in girls with central precocious puberty. Ann. Pediatr. Endocrinol. Metab. 2020, 25, 24–30. [Google Scholar] [CrossRef]
- Giedd, J.N.; Blumenthal, J.; Jeffries, N.O.; Castellanos, F.; Liu, H.; Zijdenbos, A.; Paus, T.; Evans, A.C.; Rapoport, J.L. Brain development during childhood and adolescence: A longitudinal MRI study. Nat. Neurosci. 1999, 2, 861–863. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Raine, A. Prefrontal structural and functional brain imaging findings in antisocial, violent, and psychopathic individuals: A meta-analysis. Psychiatry Res. Neuroimaging 2009, 174, 81–88. [Google Scholar] [CrossRef] [Green Version]
- Helmeke, C.; Ovtscharoff, W.; Poeggel, G.; Braun, K. Imbalance of immunohistochemically characterized interneuron populations in the adolescent and adult rodent medial prefrontal cortex after repeated exposure to neonatal separation stress. Neuroscience 2008, 152, 18–28. [Google Scholar] [CrossRef]
- Mrug, S.; Elliott, M.N.; Davies, S.; Tortolero, S.R.; Cuccaro, P.; Schuster, M.A. Early Puberty, Negative Peer Influence, and Problem Behaviors in Adolescent Girls. Pediatrics 2013, 133, 7–14. [Google Scholar] [CrossRef] [Green Version]
- Parsons, L.M. Superior parietal cortices and varieties of mental rotation. Trends Cogn. Sci. 2003, 7, 515–517. [Google Scholar] [CrossRef]
- Ehrhardt, A.A.; Meyer-Bahlburg, H.F. Idiopathic precocious puberty in girls: Long-term effects on adolescent behavior. Eur. J. Endocrinol. 1986, 113, S247–S253. [Google Scholar] [CrossRef]
- Waber, D.P. Sex differences in cognition: A function of maturation rate? Science 1976, 192, 572–574. [Google Scholar] [CrossRef] [PubMed]
- Neukel, C.; Herpertz, S.C.; Hinid-Attar, C.; Zietlow, A.-L.; Fuchs, A.; Moehler, E.; Bermpohl, F.; Bertsch, K. Neural processing of the own child’s facial emotions in mothers with a history of early life maltreatment. Eur. Arch. Psychiatry Clin. Neurosci. 2018, 269, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Waylen, A.; Wolke, D. Sex ‘n’ drugs ‘n’ rock ‘n’ roll: The meaning and social consequences of pubertal timing. Eur. J. Endocrinol. 2004, 151 (Suppl. 3), U151–U159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.H.; Shin, C.H. Observed trends for an earlier onset of puberty: When is the need of treatment indicated? J. Korean Med. Assoc. 2009, 52, 1189–1200. [Google Scholar] [CrossRef] [Green Version]
- Ehrhardt, A.; Meyer-Bahlburg, H. Psychosocial Aspects of Precocious Puberty. Horm. Res. 1994, 41, 30–35. [Google Scholar] [CrossRef]
- Shenhav, A.; Greene, J.D. Integrative moral judgment: Dissociating the roles of the amygdala and ventromedial prefrontal cortex. J. Neurosci. 2014, 34, 4741–4749. [Google Scholar] [CrossRef] [Green Version]
- Amadi, U.; Lim, S.H.; Liu, E.; Baratta, M.V.; Goosens, K.A. Hippocampal Processing of Ambiguity Enhances Fear Memory. Psychol. Sci. 2016, 28, 143–161. [Google Scholar] [CrossRef] [Green Version]
- Udwin, O. Annotation: Children’s Reactions to Traumatic Events. J. Child Psychol. Psychiatry 1993, 34, 115–127. [Google Scholar] [CrossRef]
- Tyborowska, A.; Volman, I.; Niermann, H.C.M.; Pouwels, J.L.; Smeekens, S.; Cillessen, A.H.N.; Toni, I.; Roelofs, K. Early-life and pubertal stress differentially modulate grey matter devel-opment in human adolescents. Sci. Rep. 2018, 8, 1–11. [Google Scholar]
- Menk, T.A.; Inácio, M.; Macedo, D.B.; Bessa, D.S.; Latronico, A.C.; Mendonca, B.; Brito, V.N. Assessment of stress levels in girls with central precocious puberty before and during long-acting gonadotropin-releasing hormone agonist treatment: A pilot study. J. Pediatr. Endocrinol. Metab. 2017, 30, 657–662. [Google Scholar] [CrossRef]
- Middleton, F.; Strick, P.L. Cerebellar Projections to the Prefrontal Cortex of the Primate. J. Neurosci. 2001, 21, 700–712. [Google Scholar] [CrossRef]
- Ramnani, N. The primate cortico-cerebellar system: Anatomy and function. Nat. Rev. Neurosci. 2006, 7, 511–522. [Google Scholar] [CrossRef]
- Riva, D.; Giorgi, C. The cerebellum contributes to higher functions during development: Evidence from a series of children surgically treated for posterior fossa tumors. Brain 2000, 123 Pt 5, 1051–1061. [Google Scholar] [CrossRef]
- Schmahmann, J.D. Disorders of the cerebellum: Ataxia, dysmetria of thought, and the cerebellar cognitive affective syndrome. J. Neuropsychiatry Clin. Neurosci. 2004, 16, 367–378. [Google Scholar] [CrossRef] [PubMed]
- Tiemeier, H.; Lenroot, R.K.; Greenstein, D.K.; Tran, L.; Pierson, R.; Giedd, J.N. Cerebellum development during childhood and adolescence: A longitudinal morphometric MRI study. NeuroImage 2010, 49, 63–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leech, R.; Braga, R.; Sharp, D.J. Echoes of the Brain within the Posterior Cingulate Cortex. J. Neurosci. 2012, 32, 215–222. [Google Scholar] [CrossRef] [Green Version]
- Bluhm, R.; Williamson, P.; Lanius, R.; Tjeberge, J.; Densmore, M.; Bartha, R.; Neufeld, R.; Osuch, E. Resting state default-mode network connectivity in early depression using a seed region-of-interest analysis: Decreased connectivity with caudate nucleus. Psychiatry Clin. Neurosci. 2009, 63, 754–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chavarria, M.C.; Sánchez, F.J.; Chou, Y.-Y.; Thompson, P.M.; Luders, E. Puberty in the corpus callosum. Neuroscience 2014, 265, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genc, S.; Seal, M.L.; Dhollander, T.; Malpas, C.B.; Hazell, P.; Silk, T.J. White matter alterations at pubertal onset. NeuroImage 2017, 156, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Taki, Y.; Hashizume, H.; Sassa, Y.; Takeuchi, H.; Asano, M.; Asano, K.; Kotozaki, Y.; Nouchi, R.; Wu, K.; Fukuda, H.; et al. Correlation among body height, intelligence, and brain gray matter volume in healthy children. NeuroImage 2012, 59, 1023–1027. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Girls with ICPP (N = 15) | Normal Puberty Girls (N = 15) | Age-Matched Girls (N = 15) | Statistical Analysis (p-Value) | ||||
|---|---|---|---|---|---|---|---|
| ANOVA | ICPP vs. Puberty | ICPP vs. Age-Matched | Puberty vs. Age-Matched | ||||
| Gray matter | 708.15 ± 61.14 | 666.16 ± 33.65 | 670.24 ± 59.64 | p = 0.364 | p = 0.331 | p = 0.727 | p = 0.780 |
| White matter | 486.47 ± 107.97 | 507.77 ± 64.19 | 468.75 ± 49.61 | p = 0.508 | p = 0.726 | p = 0.921 | p = 0.487 |
| Total | 1194.63 ± 122.39 | 1173.93 ± 68.93 | 1138.99 ± 75.49 | p = 0.754 | p = 0.984 | p = 0.752 | p = 0.847 |
| Brain Area | Abbr. | Side | BA* | MNI Coordinate | t-Value | Cluster Size (Voxels) | ||
|---|---|---|---|---|---|---|---|---|
| x | y | z | ||||||
| Gray matter | ||||||||
| Medial prefrontal cortex | mPFC | R | 11 | 21 | 24 | −12 | 4.48 | 143 |
| Superior parietal gyrus | SPG | R | 40 | 29 | −46 | 49 | 5.21 | 129 |
| Supramarginal gyrus | SMG | L | 48 | −47 | −30 | 34 | 4.98 | 179 |
| Angular gyrus | AnG | R | 7 | 27 | −54 | 46 | 4.79 | 129 |
| Postcentral gyrus | PoG | L | 3 | −44 | −22 | 37 | 5.45 | 179 |
| Superior occipital gyrus | SOG | L | 19 | −6 | −82 | 43 | 3.96 | 116 |
| Cuneus | Cun | L | 19 | −5 | −85 | 34 | 3.75 | 116 |
| Hippocampus | Hi | R | 37 | 26 | −30 | −5 | 4.12 | 497 |
| Parahippocampal gyrus | PHG | L | 30 | −21 | −18 | −27 | 3.91 | 180 |
| Posterior cingulate gyrus | PCgG | L | 23 | −9 | −39 | 30 | 5.44 | 1485 |
| Cerebellar cortex | Cb | L | - | −50 | −67 | −29 | 5.69 | 888 |
| White matter | ||||||||
| Insular | Ins | L | 48 | −33 | 2 | 9 | 4.58 | 750 |
| Caudate | Cd | R | - | 12 | 2 | 18 | 4.35 | 419 |
| Splenium of corpus callosum | SCC | R | - | 5 | −28 | 13 | 4.88 | 533 |
| Brain Area | Abbr. | Side | BA* | MNI Coordinate | t-Value | Cluster Size (Voxels) | ||
|---|---|---|---|---|---|---|---|---|
| x | y | z | ||||||
| ICPP | ||||||||
| Splenium of corpus callosum | SCC | R | - | 15 | −30 | 19 | 4.20 | 160 |
| Splenium of corpus callosum | SCC | L | - | −15 | −34 | 18 | 4.65 | 194 |
| Normal puberty | ||||||||
| Posterior cingulate gyrus | PCgG | L | 26 | −3 | −43 | 21 | 4.60 | 172 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.-E.; Ahn, J.-Y.; Kim, E.-Y. The Assessment of Brain Volume Differences in Idiopathic Central Precocious Puberty Girls; Comparison of Age-Matched Girls and Normal Puberty Girls. Children 2021, 8, 797. https://doi.org/10.3390/children8090797
Park S-E, Ahn J-Y, Kim E-Y. The Assessment of Brain Volume Differences in Idiopathic Central Precocious Puberty Girls; Comparison of Age-Matched Girls and Normal Puberty Girls. Children. 2021; 8(9):797. https://doi.org/10.3390/children8090797
Chicago/Turabian StylePark, Shin-Eui, Ji-Ye Ahn, and Eun-Young Kim. 2021. "The Assessment of Brain Volume Differences in Idiopathic Central Precocious Puberty Girls; Comparison of Age-Matched Girls and Normal Puberty Girls" Children 8, no. 9: 797. https://doi.org/10.3390/children8090797