
Assessment of Sleep-Related Problems in Children with Cerebral Palsy Using the SNAKE Sleep Questionnaire




Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. CP Screening
2.3. Patients’ Sleep Behavior
2.4. Data Analysis
3. Results
3.1. Patient Characteristics
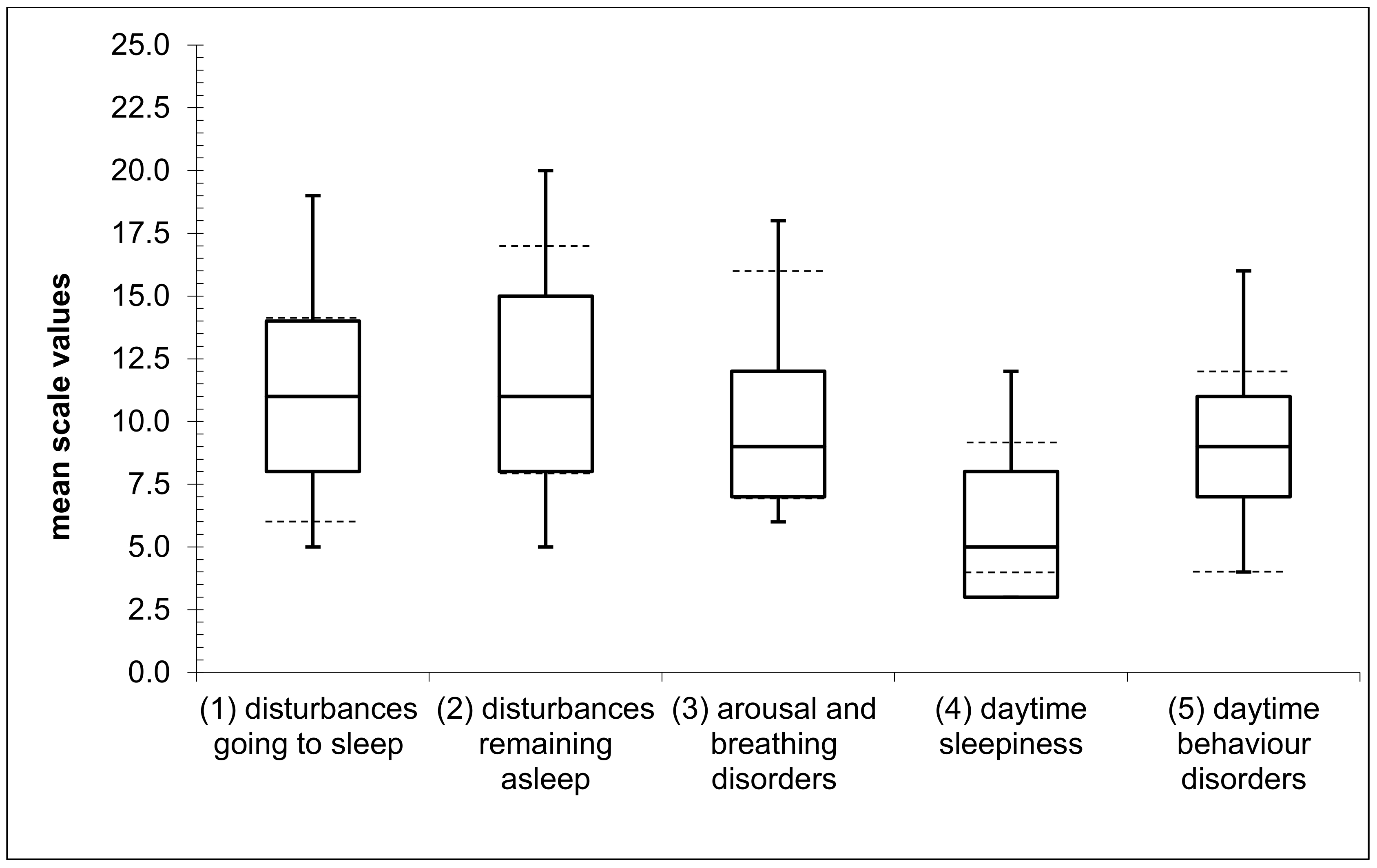
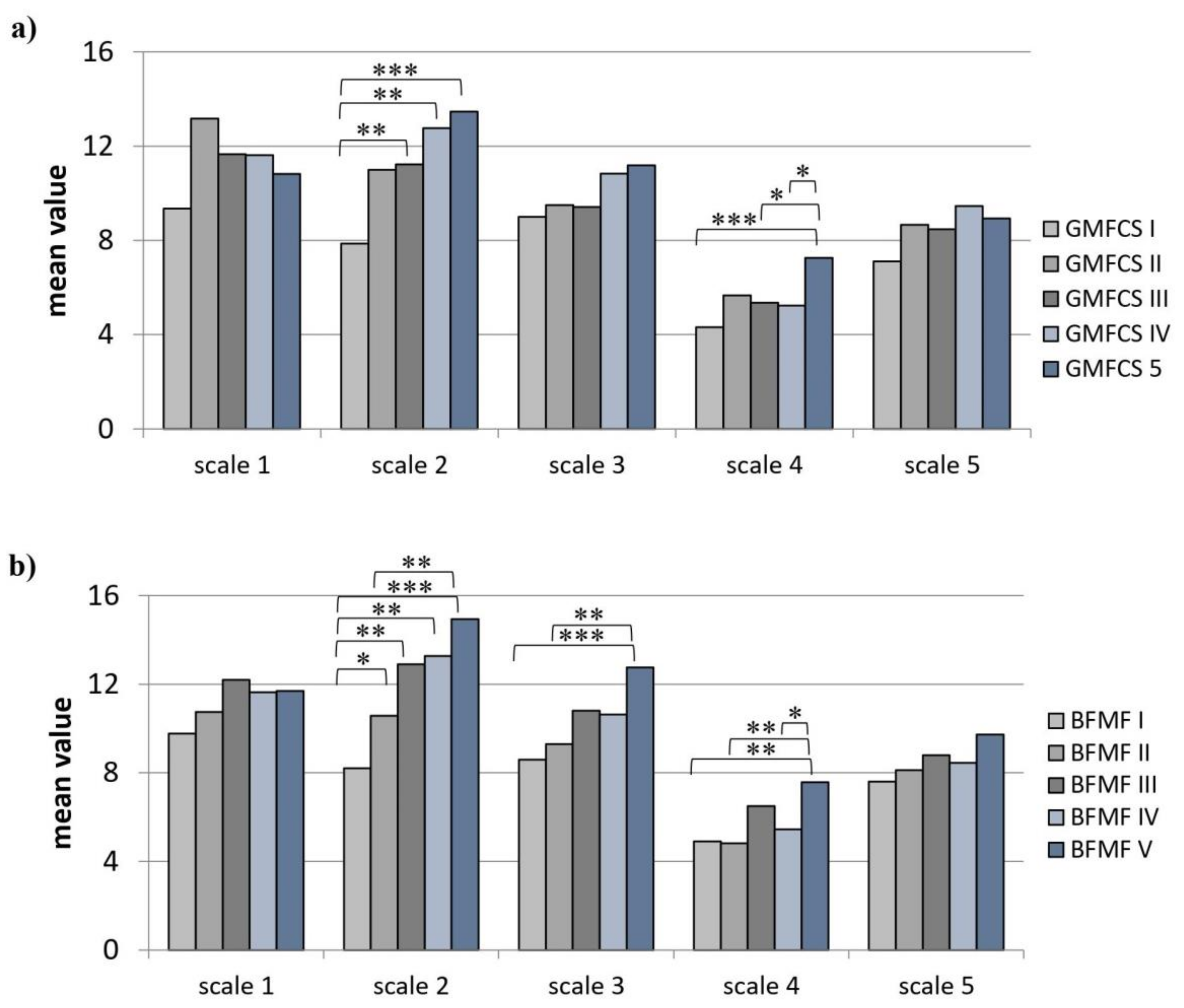
3.2. Patients’ Sleep Behavior
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Christine, C.; Dolk, H.; Platt, M.J.; Colver, A.; Prasauskiene, A.; Krägeloh-Mann, I. Recommendations from the scpe collaborative group for defining and classifying cerebral palsy. Dev. Med. Child Neurol. Suppl. 2007, 109, 35–38. [Google Scholar] [PubMed]
- Patel, D.R.; Neelakantan, M.; Pandher, K.; Merrick, J. Cerebral palsy in children: A clinical overview. Transl. Pediatrics 2020, 9, S125–S135. [Google Scholar] [CrossRef] [PubMed]
- Sadowska, M.; Sarecka-Hujar, B.; Kopyta, I. Cerebral palsy: Current opinions on definition, epidemiology, risk factors, classification and treatment options. Neuropsychiatr. Dis. Treat. 2020, 16, 1505–1518. [Google Scholar] [CrossRef] [PubMed]
- Palisano, R.; Rosenbaum, P.; Walter, S.; Russell, D.; Wood, E.; Galuppi, B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev. Med. Child Neurol. 1997, 39, 214–223. [Google Scholar] [CrossRef]
- Beckung, E.; Hagberg, G. Neuroimpairments, activity limitations, and participation restrictions in children with cerebral palsy. Dev. Med. Child Neurol. 2002, 44, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, D.A.; Follett, J.; Van Asperen, P.P. Assessing and managing lung disease and sleep disordered breathing in children with cerebral palsy. Paediatr. Respir. Rev. 2009, 10, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Tsubouchi, Y.; Tanabe, A.; Saito, Y.; Noma, H.; Maegaki, Y. Long-term prognosis of epilepsy in patients with cerebral palsy. Dev. Med. Child Neurol. 2019, 61, 1067–1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rauchenzauner, M.; Schiller, K.; Honold, M.; Baldissera, I.; Biedermann, R.; Tschiderer, B.; Albrecht, U.; Arnold, C.; Rostasy, K. Visual impairment and functional classification in children with cerebral palsy. Neuropediatrics 2021. [Google Scholar] [CrossRef]
- Stadskleiv, K. Cognitive functioning in children with cerebral palsy. Dev. Med. Child Neurol. 2020, 62, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Löwing, K.; Gyllensvärd, M.; Tedroff, K. Exploring sleep problems in young children with cerebral palsy—A population-based study. Eur. J. Paediatr. Neurol. 2020, 28, 186–192. [Google Scholar] [CrossRef]
- Lelis, A.L.; Cardoso, M.V.; Hall, W.A. Sleep disorders in children with cerebral palsy: An integrative review. Sleep Med. Rev. 2016, 30, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Owens, J. Classification and epidemiology of childhood sleep disorders. Prim. Care 2008, 35, 533–546.vii. [Google Scholar] [CrossRef] [PubMed]
- Newman, C.J.; O’Regan, M.; Hensey, O. Sleep disorders in children with cerebral palsy. Dev. Med. Child Neurol. 2006, 48, 564–568. [Google Scholar] [CrossRef]
- Sandella, D.E.; O’Brien, L.M.; Shank, L.K.; Warschausky, S.A. Sleep and quality of life in children with cerebral palsy. Sleep Med. 2011, 12, 252–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obrecht, A.; de Almeida, M.F.; Maltauro, L.; da Silva, W.D.L.; Bueno Zonta, M.; de Souza Crippa, A.C. The relationship between gross motor function impairment in cerebral palsy and sleeping issues of children and caregivers. Sleep Med. 2021, 81, 261–267. [Google Scholar] [CrossRef]
- Galland, B.C.; Elder, D.E.; Taylor, B.J. Interventions with a sleep outcome for children with cerebral palsy or a post-traumatic brain injury: A systematic review. Sleep Med. Rev. 2012, 16, 561–573. [Google Scholar] [CrossRef]
- Horwood, L.; Mok, E.; Li, P.; Oskoui, M.; Shevell, M.; Constantin, E. Prevalence of sleep problems and sleep-related characteristics in preschool- and school-aged children with cerebral palsy. Sleep Med. 2018, 50, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Atmawidjaja, R.W.; Wong, S.W.; Yang, W.W.; Ong, L.C. Sleep disturbances in malaysian children with cerebral palsy. Dev. Med. Child Neurol. 2014, 56, 681–685. [Google Scholar] [CrossRef] [Green Version]
- Griffiths, N.; Spence, K.; Loughran-Fowlds, A.; Westrup, B. Individualised developmental care for babies and parents in the nicu: Evidence-based best practice guideline recommendations. Early Hum. Dev. 2019, 139, 104840. [Google Scholar] [CrossRef]
- McCabe, S.M.; Blackmore, A.M.; Abbiss, C.R.; Langdon, K.; Elliott, C. Sleep concerns in children and young people with cerebral palsy in their home setting. J. Paediatr. Child Health 2015, 51, 1188–1194. [Google Scholar] [CrossRef]
- Cohen, R.; Halevy, A.; Shuper, A. Children’s sleep disturbance scale in differentiating neurological disorders. Pediatric Neurol. 2013, 49, 465–468. [Google Scholar] [CrossRef]
- Munyumu, K.; Idro, R.; Abbo, C.; Kaddumukasa, M.; Katabira, E.; Mupere, E.; Kakooza-Mwesige, A. Prevalence and factors associated with sleep disorders among children with cerebral palsy in uganda; a cross-sectional study. BMC Pediatrics 2018, 18, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dutt, R.; Roduta-Roberts, M.; Brown, C.A. Sleep and children with cerebral palsy: A review of current evidence and environmental non-pharmacological interventions. Children 2015, 2, 78–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romeo, D.M.; Brogna, C.; Quintiliani, M.; Baranello, G.; Pagliano, E.; Casalino, T.; Sacco, A.; Ricci, D.; Mallardi, M.; Musto, E.; et al. Sleep disorders in children with cerebral palsy: Neurodevelopmental and behavioral correlates. Sleep Med. 2014, 15, 213–218. [Google Scholar] [CrossRef]
- Grychtol, R.; Chan, E.Y. Use of non-invasive ventilation in cerebral palsy. Arch. Dis. Child 2018, 103, 1170–1177. [Google Scholar] [CrossRef] [PubMed]
- Blankenburg, M.; Tietze, A.L.; Hechler, T.; Hirschfeld, G.; Michel, E.; Koh, M.; Zernikow, B. Snake: The development and validation of a questionnaire on sleep disturbances in children with severe psychomotor impairment. Sleep Med. 2013, 14, 339–351. [Google Scholar] [CrossRef]
- Bruni, O.; Ottaviano, S.; Guidetti, V.; Romoli, M.; Innocenzi, M.; Cortesi, F.; Giannotti, F. The sleep disturbance scale for children (sdsc). Construction and validation of an instrument to evaluate sleep disturbances in childhood and adolescence. J. Sleep Res. 1996, 5, 251–261. [Google Scholar] [CrossRef]
- Owens, J.A.; Spirito, A.; McGuinn, M. The children’s sleep habits questionnaire (cshq): Psychometric properties of a survey instrument for school-aged children. Sleep 2000, 23, 1043–1051. [Google Scholar] [CrossRef]
- Churchill, S.S.; Kieckhefer, G.M.; Bjornson, K.F.; Herting, J.R. Relationship between sleep disturbance and functional outcomes in daily life habits of children with down syndrome. Sleep 2015, 38, 61–71. [Google Scholar] [CrossRef] [Green Version]
- Larson, A.M.; Ryther, R.C.; Jennesson, M.; Geffrey, A.L.; Bruno, P.L.; Anagnos, C.J.; Shoeb, A.H.; Thibert, R.L.; Thiele, E.A. Impact of pediatric epilepsy on sleep patterns and behaviors in children and parents. Epilepsia 2012, 53, 1162–1169. [Google Scholar] [CrossRef]
- Breau, L.M.; Camfield, C.S. Pain disrupts sleep in children and youth with intellectual and developmental disabilities. Res. Dev. Disabil. 2011, 32, 2829–2840. [Google Scholar] [CrossRef]
- Wayte, S.; McCaughey, E.; Holley, S.; Annaz, D.; Hill, C.M. Sleep problems in children with cerebral palsy and their relationship with maternal sleep and depression. Acta Paediatr. 2012, 101, 618–623. [Google Scholar] [CrossRef]
- Cortesi, F.; Giannotti, F.; Ottaviano, S. Sleep problems and daytime behavior in childhood idiopathic epilepsy. Epilepsia 1999, 40, 1557–1565. [Google Scholar] [CrossRef]
- Byars, A.W.; Byars, K.C.; Johnson, C.S.; DeGrauw, T.J.; Fastenau, P.S.; Perkins, S.; Austin, J.K.; Dunn, D.W. The relationship between sleep problems and neuropsychological functioning in children with first recognized seizures. Epilepsy Behav. EB 2008, 13, 607–613. [Google Scholar] [CrossRef] [Green Version]
- Bloetzer, C.; Jeannet, P.Y.; Lynch, B.; Newman, C.J. Sleep disorders in boys with duchenne muscular dystrophy. Acta Paediatr. 2012, 101, 1265–1269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tietze, A.L.; Blankenburg, M.; Hechler, T.; Michel, E.; Koh, M.; Schluter, B.; Zernikow, B. Sleep disturbances in children with multiple disabilities. Sleep Med. Rev. 2012, 16, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Dreier, L.A.; Zernikow, B.; Blankenburg, M.; Wager, J. A sleep questionnaire for children with severe psychomotor impairment (snake)-concordance with a global rating of sleep quality. Children 2018, 5, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bautista, M.; Whittingham, K.; Edwards, P.; Boyd, R.N. Psychometric properties of parent and child reported sleep assessment tools in children with cerebral palsy. Dev. Med. Child Neurol. 2018, 60, 162–172. [Google Scholar] [CrossRef] [PubMed]
- Petruch, U.; Weber, P.M.; Krägeloh-Mann, I. The reference and training manual of the scpe (surveillance of cerebral palsy in europe). Neuropediatrics 2004, 35, 495–496. [Google Scholar] [CrossRef]
- McGraw, P.; Winn, B.; Whitaker, D. Reliability of the snellen chart. BMJ 1995, 310, 1481–1482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moutray, T.N.; Williams, M.A.; Jackson, A.J. Change of visual acuity recording methods in clinical studies across the years. Ophthalmologica 2008, 222, 173–177. [Google Scholar] [CrossRef]
- Eliasson, A.-C.; Krumlinde-Sundholm, L.; Rösblad, B.; Beckung, E.; Arner, M.; Öhrvall, A.-M.; Rosenbaum, P. The manual ability classification system (macs) for children with cerebral palsy: Scale development and evidence of validity and reliability. Dev. Med. Child Neurol. 2006, 48, 549–554. [Google Scholar] [CrossRef]
- Surveillance of Cerebral Palsy in Europe. Surveillance of cerebral palsy in Europe: A collaboration of cerebral palsy surveys and registers. Surveillance of cerebral palsy in europe (scpe). Dev. Med. Child Neurol. 2000, 42, 816–824. [Google Scholar]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders. Diagnostic and Coding Manual, 2nd ed.; American Academy of Sleep Medicine: Westchester, IL, USA, 2005. [Google Scholar]
- Dreier, L.A.; Wager, J.; Blankenburg, M.; Zernikow, B. The unfavorable alliance of pain and poor sleep in children with life-limiting conditions and severe psychomotor impairment. Children 2018, 5, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Himmelmann, K.; Beckung, E.; Hagberg, G.; Uvebrant, P. Gross and fine motor function and accompanying impairments in cerebral palsy. Dev. Med. Child Neurol. 2006, 48, 417–423. [Google Scholar] [CrossRef] [Green Version]
- Himmelmann, K.; Horber, V.; Sellier, E.; De la Cruz, J.; Papavasiliou, A.; Krägeloh-Mann, I. Neuroimaging patterns and function in cerebral palsy-application of an mri classification. Front. Neurol. 2020, 11, 617740. [Google Scholar] [CrossRef] [PubMed]
- Shevell, M.I.; Dagenais, L.; Hall, N. Comorbidities in cerebral palsy and their relationship to neurologic subtype and GMFCS level. Neurology 2009, 72, 2090–2096. [Google Scholar] [CrossRef]
- Ballester-Plané, J.; Laporta-Hoyos, O.; Macaya, A.; Póo, P.; Meléndez-Plumed, M.; Toro-Tamargo, E.; Gimeno, F.; Narberhaus, A.; Segarra, D.; Pueyo, R. Cognitive functioning in dyskinetic cerebral palsy: Its relation to motor function, communication and epilepsy. Eur. J. Paediatr. Neurol. 2018, 22, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Philip, S.S.; Guzzetta, A.; Chorna, O.; Gole, G.; Boyd, R.N. Relationship between brain structure and cerebral visual impairment in children with cerebral palsy: A systematic review. Res. Dev. Disabil. 2020, 99, 103580. [Google Scholar] [CrossRef]
- Hutson, J.A.; Snow, L. Sleep assessments for children with severe cerebral palsy: A scoping review. Arch. Rehabil. Res. Clin. Transl. 2020, 2, 100087. [Google Scholar]
- Shellhaas, R.A.; Burns, J.W.; Barks, J.D.E.; Hassan, F.; Chervin, R.D. Maternal voice and infant sleep in the neonatal intensive care unit. Pediatrics 2019, 144, e20190288. [Google Scholar] [CrossRef] [PubMed]
- Horwood, L.; Li, P.; Mok, E.; Shevell, M.; Constantin, E. A systematic review and meta-analysis of the prevalence of sleep problems in children with cerebral palsy: How do children with cerebral palsy differ from each other and from typically developing children? Sleep Health 2019, 5, 555–571. [Google Scholar] [CrossRef]
- Hadden, K.L.; von Baeyer, C.L. Pain in children with cerebral palsy: Common triggers and expressive behaviors. Pain 2002, 99, 281–288. [Google Scholar] [CrossRef]
- Sato, H.; Iwasaki, T.; Yokoyama, M.; Inoue, T. Monitoring of body position and motion in children with severe cerebral palsy for 24 h. Disabil. Rehabil. 2014, 36, 1156–1160. [Google Scholar] [CrossRef] [PubMed]
- Angriman, M.; Caravale, B.; Novelli, L.; Ferri, R.; Bruni, O. Sleep in children with neurodevelopmental disabilities. Neuropediatrics 2015, 46, 199–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghorbanpour, Z.; Hosseini, S.A.; Akbarfahimi, N.; Rahgozar, M. Correlation between sleep disorders and function in children with spastic cerebral palsy. Iran. J. Child Neurol. 2019, 13, 35–44. [Google Scholar] [PubMed]
- Beecham, E.; Hudson, B.F.; Oostendorp, L.; Candy, B.; Jones, L.; Vickerstaff, V.; Lakhanpaul, M.; Stone, P.; Chambers, L.; Hall, D.; et al. A call for increased paediatric palliative care research: Identifying barriers. Palliat. Med. 2016, 30, 979–980. [Google Scholar] [CrossRef] [Green Version]
- Kaleyias, J.; Manley, P.; Kothare, S.V. Sleep disorders in children with cancer. Semin. Pediatric Neurol. 2012, 19, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Simard-Tremblay, E.; Constantin, E.; Gruber, R.; Brouillette, R.T.; Shevell, M. Sleep in children with cerebral palsy: A review. J. Child Neurol. 2011, 26, 1303–1310. [Google Scholar] [CrossRef]
- Smith, M.T.; McCrae, C.S.; Cheung, J.; Martin, J.L.; Harrod, C.G.; Heald, J.L.; Carden, K.A. Use of actigraphy for the evaluation of sleep disorders and circadian rhythm sleep-wake disorders: An american academy of sleep medicine clinical practice guideline. J. Clin. Sleep Med. 2018, 14, 1231–1237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwantes, S.; O’Brien, H.W. Pediatric palliative care for children with complex chronic medical conditions. Pediatric Clin. N. Am. 2014, 61, 797–821. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | n (%) * |
|---|---|
| Type of CP | |
| BSCP | 57 (57) |
| USCP | 29 (29) |
| dyskinetic | 14 (14) |
| dystonic | 13 |
| choreoathethoid | 1 |
| cause of CP | |
| periventricular leukomalacia | 25 (25) |
| ischemic stroke | 13 (13) |
| hypoxic brain injury | 13 (13) |
| brain malformations | 13 (13) |
| infections | 10 (10) |
| unknown | 10 (10) |
| intracranial bleeding | 8 (8) |
| genetic factors | 7 (7) |
| traumatic brain injury | 1 (1) |
| CP comorbidities | |
| epilepsy | 58 (58) |
| use of anticonvulsants | 47 (81) |
| visual impairment | 65 (65.7) |
| severe | 15 (23.8) |
| cognitive impairment | 56 (71.8) |
| hearing impairment | 23 (23.2) |
| severe | 6 (26.1) |
| birth weight | |
| >2500 g | 51 (53.1) |
| 1500–2500 g | 18 (18.8) |
| 1000–1499.99 g | 16 (16.7) |
| <1000 g | 11 (11.5) |
| gestational age | |
| term born (37–41 weeks) | 51 (51.5) |
| extreme preterm (<32 weeks) | 32 (32.3) |
| preterm (32–36 weeks) | 15 (15.2) |
| postterm (>41 weeks) | 1 (1) |
| type of delivery | |
| C-section, emergency | 41 (41) |
| vaginal | 34 (34) |
| C-section, planned | 25 (25) |
| GMFCS | |
| I | 29 (29) |
| II | 6 (6) |
| III | 21 (21) |
| IV | 13 (13) |
| V | 31 (31) |
| BFMF | |
| I | 35 (35) |
| II | 24 (24) |
| III | 10 (10) |
| IV | 11 (11) |
| V | 20 (20) |
| SNAKE Scales | CP Characteristics | |||||||
|---|---|---|---|---|---|---|---|---|
| Subtype | Comorbidities | |||||||
| VI severe | HI severe | CI | Epilepsy | Anticonvulsants | GMFCS | BFMF | ||
| 1 | 0.09 | 0.00 | 0.03 | 0.07 | 0.02 | −0.11 | 0.13 | 0.20 * |
| 0.06 | 0.00 | |||||||
| 2 | 0.02 | 0.21 * | 0.17 | 0.32 * | 0.27 * | 0.07 | 0.49 ** | 0.57 ** |
| 0.30 * | 0.03 | |||||||
| 3 | −0.12 | 0.12 | 0.27 * | 0.15 | 0.24 * | −0.05 | 0.24 * | 0.41 ** |
| 0.14 | −0.00 | |||||||
| 4 | 0.06 | 0.15 | −0.05 | 0.16 | 0.22 * | 0.04 | 0.39 * | 0.34 ** |
| 0.27 * | −0.13 | |||||||
| 5 | 0.02 | 0.15 | 0.05 | 0.23 * | 0.23 * | 0.11 | 0.21 * | 0.21 * |
| 0.15 | −0.09 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dreier, L.A.; Kapanci, T.; Lonnemann, K.; Koch-Hogrebe, M.; Wiethoff-Ubrig, L.; Rauchenzauner, M.; Blankenburg, M.; Zernikow, B.; Wager, J.; Rostasy, K. Assessment of Sleep-Related Problems in Children with Cerebral Palsy Using the SNAKE Sleep Questionnaire. Children 2021, 8, 772. https://doi.org/10.3390/children8090772
Dreier LA, Kapanci T, Lonnemann K, Koch-Hogrebe M, Wiethoff-Ubrig L, Rauchenzauner M, Blankenburg M, Zernikow B, Wager J, Rostasy K. Assessment of Sleep-Related Problems in Children with Cerebral Palsy Using the SNAKE Sleep Questionnaire. Children. 2021; 8(9):772. https://doi.org/10.3390/children8090772
Chicago/Turabian StyleDreier, Larissa Alice, Tugba Kapanci, Katharina Lonnemann, Margarete Koch-Hogrebe, Lucia Wiethoff-Ubrig, Markus Rauchenzauner, Markus Blankenburg, Boris Zernikow, Julia Wager, and Kevin Rostasy. 2021. "Assessment of Sleep-Related Problems in Children with Cerebral Palsy Using the SNAKE Sleep Questionnaire" Children 8, no. 9: 772. https://doi.org/10.3390/children8090772