
Leveraging Grief: Involving Bereaved Parents in Pediatric Palliative Oncology Program Planning and Development

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Parental Recommendations to Improve the Quality of Pediatric Palliative and End-of-Life Care (“The Eight Priorities”)
- Recommendation #1: To ensure that children receive the best possible treatment of disease and have the best possible quality of life, always hoping for the best possible outcome.
- Recommendation #2: To provide effective symptom management throughout the illness trajectory.
- Recommendation #3: To provide relationship-based care.
- Recommendation #4: To empower families with useful and reliable information.
- Recommendation #5: To support children and families in the process of making difficult care decisions.
- Recommendation #6: To facilitate care coordination.
- Recommendation #7: To ensure that children with progressive, incurable illness experience a comfortable and peaceful death.
- Recommendation #8: To provide bereavement support for surviving family members and hospital staff.
3. Progress towards These Goals
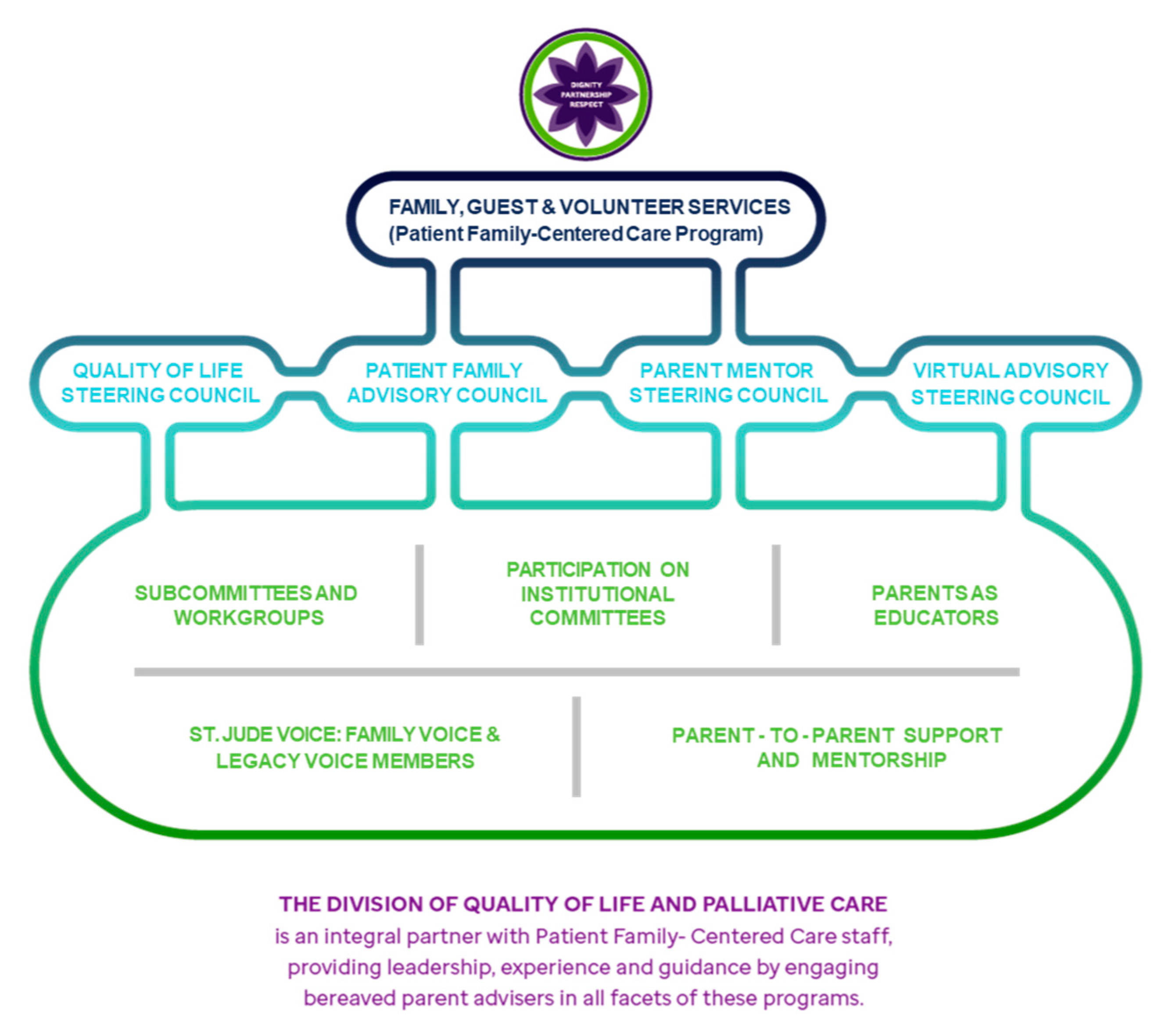
4. Quality of Life Steering Council (QoLSC)
5. Quality of Life for All (QoLA) Clinical Team
6. Bereaved Parent Educators
7. Bereavement Program
- Mailing Program: Each family receives four bereaved parent-created mailings during the first year following the death of their child. In addition, the QoLA clinical service and psychosocial teams sign and mail condolence cards to all families. Finally, for patients enrolled in the institutional School Program, a condolence card signed by their teacher(s) is sent and a book is donated in the child’s memory to their local school.
- Funerary assistance: Funerary assistance is provided to families (paid directly to the funeral home of choice) following the death of a patient to offset the cost of funeral and burial services.
- Bereavement website: www.stjude.org/bereavement [12] provides families with grief information and resources, specifically centering grief due to the death of a child.
- Stay in Touch Program: Trained bereaved parent volunteers contact newly bereaved parents once a month for 4 months following the death of their child to offer condolences from one bereaved parent to another and identify concerns or needs that may need to be addressed by the Bereavement Coordinator. This program was created by bereaved parents to serve other newly bereaved parents.
- Resource assistance: The Bereavement Coordinator (L.C.) is available to all bereaved families and locates local bereavement supports for families as needed.
- Day of Remembrance Event: We host an annual two-day event, traditionally held on the medical campus, for families whose child has died within the previous 5 years. Families honor their child, interact with faculty and staff, and meet other bereaved families. The 2020 Day of Remembrance was held as a virtual event because of the COVID-19 global pandemic and virtually hosted 155 families. Through pre-recorded videos, families heard from faculty and staff; a panel of bereaved parents and grandparents; and Child Life Specialists, who modeled a memory-making activity. Families interacted via virtual small-group discussions facilitated by 39 trained bereaved parent volunteers. Parents sent in photographs, which were arranged into a pre-recorded slideshow for the celebration of life. Finally, special notecards were crafted by staff close to children of attendees and were then mailed or emailed to families.
- Podcast Series: Members of the QoLSC are working to develop a podcast series. Here, bereaved parents share their experiences with a series of grief-related topics to expand the diversity of bereavement care offerings we provide to bereaved families who have fewer local supports available in their communities.
- Virtual Parent-Led Group Discussions: Parents may join in quarterly virtual small-group topical discussions with other bereaved parents (or grandparents or adult siblings, depending on the group) run by trained, bereaved parent facilitators.
- Virtual Adviser Community (Legacy Voice): Bereaved caregivers may join this interactive listserv following the death of their child to provide parental input to improve institutional care. Members of Legacy Voice respond to staff-created surveys and discussion forums to tailor quality-improvement efforts.
- Bereaved Parent Mentoring Program: A formalized, peer-to-peer support service for bereaved parents was established to support parents with children nearing the end-of-life and/or after the death of a child. A steering council of psychosocial staff and parent mentors oversees the program. A structured process was created to match referred parents with a bereaved parent mentor. Parent mentors, who must be 2 or more years from the death of their child, are carefully vetted and receive formal training in mentorship skills, logistics of the mentor role, understanding boundaries and limitations, and mentor self-care. The role of the parent mentor is to provide a level of support distinct from that provided by clinical staff, family, or friends due to insight into the lived experience of anticipatory grief and grief after the death of a child. The mentors regularly reach out to mentees for a designated 15-month period as an additional layer of support during early bereavement. For each contact that a parent mentor has with their mentee, an encounter summary is created; at regular intervals, these encounters are evaluated and discussed with the Bereavement Coordinator. The mentors are trained to “flag” encounters of concern to assure follow up is provided by the Bereavement Coordinator or another member of the clinical team.
8. Strategic Planning
9. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hendrickson, K.C. Morbidity, mortality, and parental grief: A review of the literature on the relationship between the death of a child and the subsequent health of parents. Palliat. Support Care 2009, 7, 109. [Google Scholar] [CrossRef] [PubMed]
- Snaman, J.M.; Kaye, E.C.; Torres, C.; Gibson, D.V.; Baker, J.N. Helping parents live with the hole in their heart: The role of health care providers and institutions in bereaved parents’ grief journey. Cancer 2016, 122, 2757–2765. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.; Weng, C.; Spraker-Perlman, H.L. A Provider-Based Survey to Assess Bereavement Care Knowledge, Attitudes, and Practices in Pediatric Oncologists. J. Palliat. Med. 2017, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiener, L.; Kazak, A.; Noll, R.B.; Patenaude, A.F.; Kupst, M. Standards for the Psychosocial Care of Children With Cancer and Their Famillies: An Introduction to the Special Issue. Pediatr. Blood Cancer 2015, 62, S419–S424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snaman, J.M.; Kaye, E.C.; Levine, D.R.; Cochran, B.; Wilcox, R.; Sparrow, C.K.; Noyes, N.; Clark, L.; Avery, W.; Baker, J.N. Empowering Bereaved Parents through the Development of a Comprehensive Bereavement Program. J. Pain Symptom Manag. 2017, 53, 767–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snaman, J.M.; Kaye, E.C.; Spraker-Perlman, H.; Levine, D.; Clark, L.; Wilcox, R.; Barnett, B.; Sykes, A.; Lu, Z.; Cunningham, M.J.; et al. Incorporating Bereaved Parents as Faculty Facilitators and Educators in Teaching Principles of Palliative and End-of-Life Care. Am. J. Hosp. Palliat. Med. 2018, 35, 1518–1525. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.N.; ASCO Post Evening News. St. Jude Children’s Research Hospital Committee Identifies Eight Palliative Care Priorities in Pediatric Oncology. Available online: https://ascopost.com/issues/march-15-2014/st-jude-children-s-research-hospital-committee-identifies-eight-palliative-care-priorities-in-pediatric-oncology/ (accessed on 31 May 2021).
- Meij, L.W.-D.; Stroebe, M.; Stroebe, W.; Schut, H.; Bout, J.V.D.; Van Der Heijden, P.G.M.; Dijkstra, I. The Impact of Circumstances Surrounding the Death of a Child on Parents’ Grief. Death Stud. 2008, 32, 237–252. [Google Scholar] [CrossRef] [PubMed]
- Schuelke, T.; Crawford, C.; Kentor, R.; Eppelheimer, H.; Chipriano, C.; Springmeyer, K.; Shukraft, A.; Hill, M. Current Grief Support in Pediatric Palliative Care. Children 2021, 8, 278. [Google Scholar] [CrossRef] [PubMed]
- Levine, D.; Johnson, L.M.; Wiser, R.K.; Gibson, D.; Kane, J.R.; Baker, J.N. Integrating Palliative Care in Pediatric Oncology: Evidence for an Evolving Paradigm of Comprehensive Cancer Care. J. Natl. Compr. Cancer Netw. 2016, 14, 741–748. [Google Scholar] [CrossRef] [PubMed]
- Snaman, J.M.; Kaye, E.C.; Cunningham, M.J.; Sykes, A.D.; Levine, D.R.; Mahoney, D.; Baker, J.N. Going straight to the source: A pilot study of bereaved parent-facilitated communication training for pediatric subspecialty fellows. Pediatr. Blood Cancer 2016, 64, 156–162. [Google Scholar] [CrossRef] [PubMed]
- St. Jude Bereavement Website. Available online: www.stjude.org/bereavement (accessed on 31 May 2021).
- Wiener, L.; Rosenberg, A.R.; Lichtenthal, W.G.; Tager, J.; Weaver, M.S. Personalized and yet standardized: An informed approach to the integration of bereavement care in pediatric oncology settings. Palliat. Support Care. 2018, 16, 706–711. [Google Scholar] [CrossRef] [PubMed]
- Kaye, E.C.; Kiefer, A.; Blazin, L.; Spraker-Perlman, H.; Clark, L.; Baker, J.N. Bereaved parents, hope, and realism. Pediatrics 2020, 145. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Eight Pivotal Parent Recommendations |
|---|
|
| Pediatric Subspecialty Fellow Communication Training |
|
| Institutional Clinical Staff Training (open to all healthcare providers) |
|
| Regional Hospice Nurse Conferences |
| Pediatric Palliative Oncology Symposium (PPOS) |
| Grand Rounds and institutional didactics |
| Consultation with other pediatric institutions for bereavement program development |
| Quality of Life Steering Council Goals |
|---|
|
|
|
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spraker-Perlman, H.L.; Aglio, T.; Kaye, E.C.; Levine, D.; Barnett, B.; Berry Carter, K.; McNeil, M.; Clark, L.; Baker, J.N.; the St. Jude Quality of Life Steering Council. Leveraging Grief: Involving Bereaved Parents in Pediatric Palliative Oncology Program Planning and Development. Children 2021, 8, 472. https://doi.org/10.3390/children8060472
Spraker-Perlman HL, Aglio T, Kaye EC, Levine D, Barnett B, Berry Carter K, McNeil M, Clark L, Baker JN, the St. Jude Quality of Life Steering Council. Leveraging Grief: Involving Bereaved Parents in Pediatric Palliative Oncology Program Planning and Development. Children. 2021; 8(6):472. https://doi.org/10.3390/children8060472
Chicago/Turabian StyleSpraker-Perlman, Holly L., Taylor Aglio, Erica C. Kaye, Deena Levine, Brittany Barnett, Kathryn Berry Carter, Michael McNeil, Lisa Clark, Justin N. Baker, and the St. Jude Quality of Life Steering Council. 2021. "Leveraging Grief: Involving Bereaved Parents in Pediatric Palliative Oncology Program Planning and Development" Children 8, no. 6: 472. https://doi.org/10.3390/children8060472