
Use of Paclitaxel to Successfully Treat Children, Adolescents, and Young Adults with Kaposi Sarcoma in Southwestern Tanzania


 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. KS Diagnosis
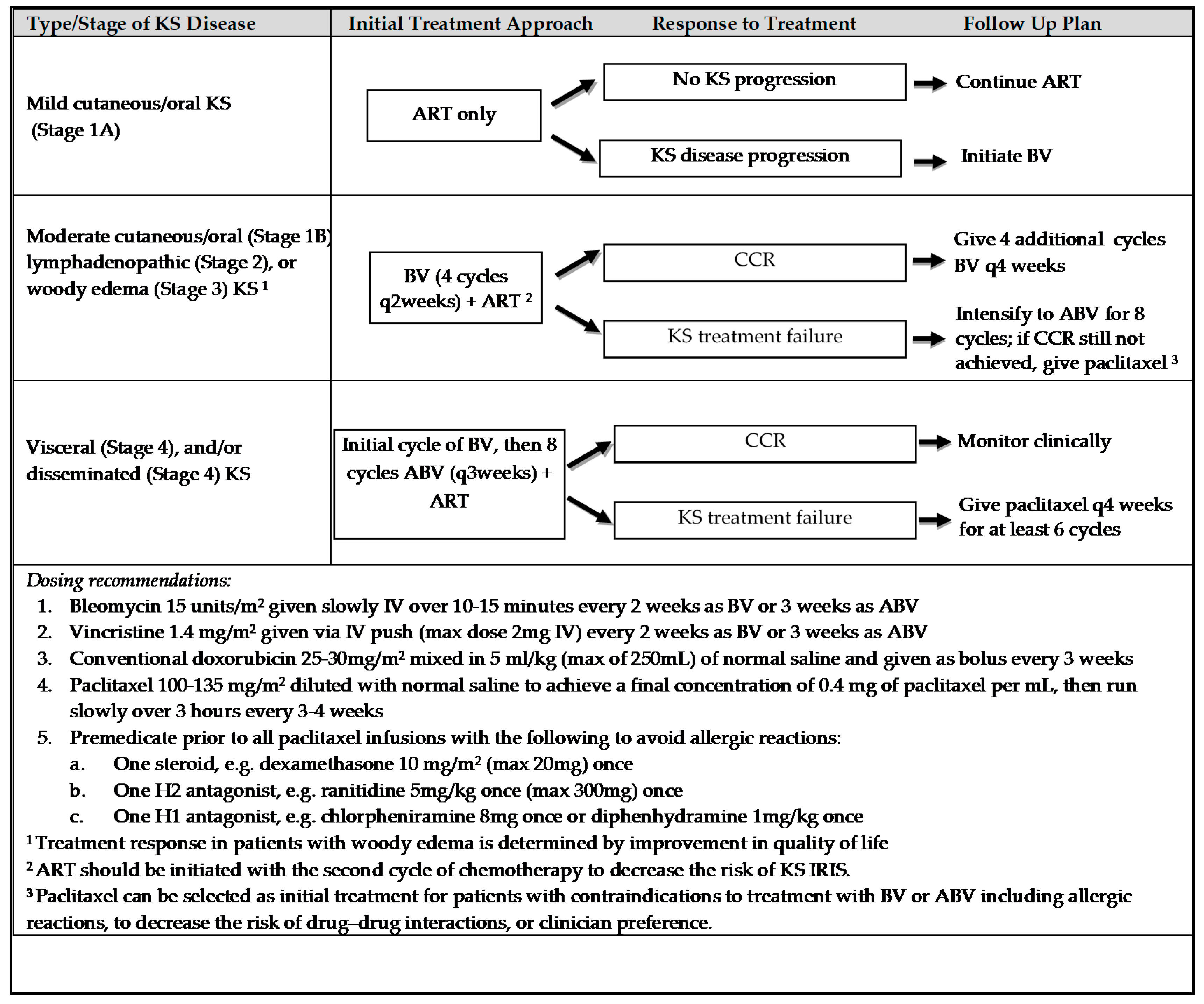
2.2. Approach to Chemotherapy
2.3. HIV Care
2.4. Nutritional Assessment and Support
2.5. Palliative Care
2.6. Statistical Analysis
2.7. Ethical Clearance
3. Results
3.1. Clinical Characteristics
3.2. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef]
- Cesarman, E.; Damania, B.; Krown, S.E.; Martin, J.; Bower, M.; Whitby, D. Kaposi sarcoma. Nat. Rev. Dis. Primers 2019, 5. [Google Scholar] [CrossRef]
- Irira, M.; Ngocho, J.S.; Youze, J.; Shayo, I.; Komba, V.; Minja, L.; Karia, F.P.; Bartlett, J.; Mmbaga, B.T. Prevalence and Outcome of HIV-associated Malignancies Among HIV-infected Children Enrolled into Care at Kilimanjaro Christian Medical Center 2006 to 2014: A Hospital-based Retrospective Analytical Study. J. Pediatr. Hematol. Oncol. 2020, 42, 69–73. [Google Scholar] [CrossRef]
- Mutalima, N.; Molyneux, E.M.; Johnston, W.T.; Jaffe, H.W.; Kamiza, S.; Borgstein, E.; Mkandawire, N.; Liomba, G.N.; Batumba, M.; Carpenter, L.M.; et al. Impact of infection with human immunodeficiency virus-1 (HIV) on the risk of cancer among children in Malawi—Preliminary findings. Infect. Agents Cancer 2010, 5, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Stefan, D.C.; Stones, D.K. Children with cancer and HIV infection: What is different about them? J. Pediatr. Hematol. Oncol. 2013, 35, 590–596. [Google Scholar] [CrossRef]
- Idele, P.; Gillespie, A.; Porth, T.; Suzuki, C.; Mahy, M.; Kasedde, S.; Luo, C. Epidemiology of HIV and AIDS among adolescents: Current status, inequities, and data gaps. J. Acquir. Immune Defic. Syndr. 2014, 66, 144–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Semango, G.P.; Charles, R.M.; Swai, C.I.; Mremi, A.; Amsi, P.; Sonda, T.; Shao, E.R.; Mavura, D.R.; Joosten, L.A.B.; Sauli, E.; et al. Prevalence and associated risk factors for Kaposi’s sarcoma among HIV-positive patients in a referral hospital in Northern Tanzania: A retrospective hospital-based study. BMC Cancer 2018, 18, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Borges, Á.H.; Neuhaus, J.; Babiker, A.G.; Henry, K.; Jain, M.K.; Palfreeman, A.; Mugyenyi, P.; Domingo, P.; Hoffmann, C.; Read, T.R.H.; et al. Immediate Antiretroviral Therapy Reduces Risk of Infection-Related Cancer During Early HIV Infection. Clin. Infect. Dis. 2016, 63, 1668–1676. [Google Scholar] [CrossRef] [PubMed]
- de Lima, C.T.; de Araújo, P.S.R.; de Teixeira, H.M.; dos Santos, J.B.; da Silveira, V.M. Clinical and laboratory characteristics, staging, and outcomes of individuals with AIDS-associated Kaposi’s sarcoma at an university hospital. An. Bras. Dermatol. 2017, 92, 172–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, M.C.G.; Frobisher, C.; Hawkins, M.M.; Jenney, M.; Lancashire, E.R.; Reulen, R.C.; Taylor, A.J.; Winter, D.L. The British Childhood Cancer Survivor Study: Objectives, methods, population structure, response rates and initial descriptive information. Pediatr. Blood Cancer 2008, 50, 1018–1025. [Google Scholar] [CrossRef]
- El-Mallawany, N.K.; Kamiyango, W.; Villiera, J.; Slone, J.S.; Kovarik, C.L.; Campbell, L.R.; Agrawal, A.K.; Dittmer, D.P.; Eason, A.B.; Ahmed, S.; et al. Proposal of a risk-stratification platform to address distinct clinical features of pediatric Kaposi sarcoma in Lilongwe, Malawi. J. Glob. Oncol. 2018, 2018. [Google Scholar] [CrossRef]
- Herce, M.E.; Kalanga, N.; Wroe, E.B.; Keck, J.W.; Chingoli, F.; Tengatenga, L.; Gopal, S.; Phiri, A.; Mailosi, B.; Bazile, J.; et al. Excellent clinical outcomes and retention in care for adults with HIV-associated Kaposi sarcoma treated with systemic chemotherapy and integrated antiretroviral therapy in rural Malawi. J. Int. Aids Soc. 2015, 18, 19929. [Google Scholar] [CrossRef] [PubMed]
- Natarajan, P.; Miller, A. A case of relapsed visceral Kaposi’s sarcoma with bilateral chylothoraces successfully treated with paclitaxel. Int. J. STD AIDS 2015, 26, 605–609. [Google Scholar] [CrossRef] [PubMed]
- Brambilla, L.; Romanelli, A.; Bellinvia, M.; Ferrucci, S.; Vinci, M.; Boneschi, V.; Miedico, A.; Tedeschi, L. Weekly paclitaxel for advanced aggressive classic Kaposi sarcoma: Experience in 17 cases. Br. J. Dermatol. 2008, 158, 1339–1344. [Google Scholar] [CrossRef]
- Krown, S.E.; Moser, C.B.; MacPhail, P.; Matining, R.M.; Godfrey, C.; Caruso, S.R.; Hosseinipour, M.C.; Samaneka, W.; Nyirenda, M.; Busakhala, N.W.; et al. Treatment of advanced AIDS-associated Kaposi sarcoma in resource-limited settings: A three-arm, open-label, randomised, non-inferiority trial. Lancet 2020, 395, 1195–1207. [Google Scholar] [CrossRef]
- Vaz, P.; Macassa, E.; Jani, I.; Thome, B.; Mahagaja, E.; Madede, T.; Muando, V.; Biberfeld, G.; Anderson, S.; Blanche, S. Treatment of Kaposi sarcoma in human immunodeficiency virus-1-infected Mozambican children with antiretroviral drugs and chemotherapy. Pediatr. Infect. Dis. J. 2011, 30, 891–893. [Google Scholar] [CrossRef] [PubMed]
- Reddy-Holdcraft, S.; Mehta, P.S.; Agrawal, A.K. Paclitaxel for relapsed or recurrent HIV-associated pediatric Kaposi’s sarcoma. Aids 2014, 28, 800–802. [Google Scholar] [CrossRef] [PubMed]
- El-Mallawany, N.K.; McAtee, C.L.; Campbell, L.R.; Kazembe, P.N. Pediatric Kaposi sarcoma in context of the HIV epidemic in sub-Saharan Africa: Current perspectives. Pediatr. Healthmed. Ther. 2018, 9, 35–46. [Google Scholar] [CrossRef] [Green Version]
- Krown, S.E.; Testa, M.A.; Huang, J. AIDS-related Kaposi’s sarcoma: Prospective validation of the AIDS Clinical Trials Group staging classification. AIDS Clinical Trials Group Oncology Committee. J. Clin. Oncol. 1997, 15, 3085–3092. [Google Scholar] [CrossRef]
- El-Mallawany, N.K.; Kamiyango, W.; Slone, J.S.; Villiera, J.; Kovarik, C.L.; Cox, C.M.; Dittmer, D.P.; Ahmed, S.; Schutze, G.E.; Scheurer, M.E.; et al. Clinical Factors Associated with Long-Term Complete Remission versus Poor Response to Chemotherapy in HIV-Infected Children and Adolescents with Kaposi Sarcoma Receiving Bleomycin and Vincristine: A Retrospective Observational Study. PLoS ONE 2016, 11, e0153335. [Google Scholar] [CrossRef]
- Bacha, J.M.; El-Mallawany, N.K.; Slone, J.S.; Wilkinson, J.P.; Mehta, P.S.; Campbell, L.R. Recommendations for treating life-threatening Kaposi sarcoma during pregnancy in HIV-positive women in low income countries. Int. J. STD AIDS 2020, 31, 724–734. [Google Scholar] [CrossRef] [PubMed]
- Krown, S.E.; Metroka, C.; Wernz, J.C. Kaposi’s sarcoma in the acquired immune deficiency syndrome: A proposal for uniform evaluation, response, and staging criteria. AIDS Clinical Trials Group Oncology Committee. J. Clin. Oncol. 1989, 7, 1201–1207. [Google Scholar] [CrossRef] [PubMed]
- MoHcdec, N. National Guidelines for the Management of HIV and AIDS, 6th ed.; National AIDS Control Programme: Dar es Salaam, Tanzania, 2017; p. 344.
- World Health Organization. Interim WHO Clinical Staging of HIV/AIDS and HIV/AIDS Case Definitions for Surveillance: African Region; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- World Health Organization. Pocket Book of Hospital Care for Children: Guidelines for the Management of Common Illnesses with Limited Resources; WHO Press: Geneva, Switzerland, 2013. [Google Scholar]
- World Health Organization. WHO Growth Reference 5–19 Years. Available online: http://www.who.int/growthref/who2007_bmi_for_age/en/ (accessed on 13 March 2021).
- World Health Organization. Guidelines for an Integrated Approach to Nutritional Care of HIV-Infected Children (6 Months–14 Years); World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Cox, C.M.; El-Mallawany, N.K.; Kabue, M.; Kovarik, C.; Schutze, G.E.; Kazembe, P.N.; Mehta, P.S. Clinical characteristics and outcomes of HIV-infected children diagnosed with Kaposi sarcoma in Malawi and Botswana. Pediatr. Blood Cancer 2013, 60, 1274–1280. [Google Scholar] [CrossRef] [PubMed]
- El-Mallawany, N.K.; Villiera, J.; Kamiyango, W.; Peckham-Gregory, E.C.; Scheurer, M.E.; Allen, C.E.; McAtee, C.L.; Legarreta, A.; Dittmer, D.P.; Kovarik, C.L.; et al. Endemic Kaposi sarcoma in HIV-negative children and adolescents: An evaluation of overlapping and distinct clinical features in comparison with HIV-related disease. Infect. Agents Cancer 2018, 13, 1–7. [Google Scholar] [CrossRef]
- Şen, H.S.; Ateş, B.T.; Yılmazbaş, P.; Ocak, S.; Kırımlıoğlu, H.; Gökçe, S.; Acarlı, K. Successful treatment of pediatric post-liver transplant Kaposi‘s sarcoma with paclitaxel. Turk. J. Pediatr. 2020, 62, 858–862. [Google Scholar] [CrossRef]
- Ocwieja, K.E.; Vargas, S.O.; Elisofon, S.A.; Shulman, D.S.; Lee, C.K.; Fawaz, R.; Collins, N.; Vakili, K.; Sharma, T.S. Pediatric post-transplant hepatic kaposi sarcoma due to donor-derived human herpesvirus 8. Pediatr. Transplant. 2019, 23, e13384. [Google Scholar] [CrossRef]
- Pashankar, F.; Frazier, A.L.; Krailo, M.; Xia, C.; Pappo, A.S.; Malogolowkin, M.; Olson, T.A.; Rodriguez-Galindo, C. Treatment of refractory germ cell tumors in children with paclitaxel, ifosfamide, and carboplatin: A report from the Children’s Oncology Group AGCT0521 study. Pediatr. Blood Cancer 2018, 65, e27111. [Google Scholar] [CrossRef]
- Funato, M.; Fukao, T.; Sasai, H.; Hori, T.; Terazawa, D.; Kanda, K.; Ozeki, M.; Mizuta, K.; Hirose, Y.; Kaneko, H.; et al. Paclitaxel-based chemotherapy for aggressive kaposiform hemangioendothelioma of the temporomastoid region: Case report and review of the literature. Head Neck 2013, 35, E258–E261. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic at Time of KS Diagnosis | Result |
|---|---|
| Age in Years (Median, IQR) | 13.0 (9.3–15.8) |
| Children (0–10 years) | 5 (29.4%) |
| Adolescents (10–19 years) | 11 (64.7%) |
| Young adults (20–25 years) | 1 (5.9%) |
| Male sex | 10 (58.8%) |
| Diagnosis supported by histopathology | 3 (17.6%) |
| KS Clinical Features | |
| Hyperpigmented Skin Lesions | 14 (82.4%) |
| Lymphadenopathy | 13 (76.5%) |
| Subcutaneous Nodules | 10 (58.8%) |
| Woody Edema | 9 (52.9%) |
| Oral lesions | 10 (58.8%) |
| Clinical GI involvement | 3 (17.6%) |
| Clinical Pulmonary involvement | 5 (29.4%) |
| Disseminated disease (>20 skin lesions) | 7 (41.2%) |
| Lilongwe Stage | |
| Stage 1 (Mild/Moderate KS limited to skin/oral involvement) | 0 (0%) |
| Stage 2 (Lymphadenopathic KS) | 5 (29.4%) |
| Stage 3 (Woody Edema KS) | 4 (23.5%) |
| Stage 4 (Visceral and/or Disseminated skin/oral KS) | 8 (47.1%) |
| TIS Stage 1 | |
| T0 | 5 (29.4%) |
| T1 | 12 (70.6%) |
| I0 2 | 6 (37.5%) |
| I1 | 10 (62.5%) |
| S0 | 5 (29.4%) |
| S1 | 12 (70.6%) |
| Cytopenias | |
| Severe anemia (Hemoglobin < 8 g/dL) | 2 (11.8%) |
| Severe thrombocytopenia (Platelets < 50,000/mm3) | 2 (11.8%) |
| Severe Acute Malnutrition | 6 (35.3%) |
| Moderate Acute Malnutrition | 4 (23.5%) |
| HIV+ | 16 (94.1%) |
| WHO severe immunosuppression | 10 (62.5%) |
| WHO advanced immunosuppression | 2 (12.5%) |
| WHO mild immunosuppression | 1 (6.2%) |
| No immunosuppression | 3 (18.8%) |
| On ART at diagnosis | 14 (87.5%) |
| Median time on ART prior to KS diagnosis | 5.3 months (IQR 1.5–93.8) |
| On ART < 6 months | 7 (50%) |
| On ART > 6 months | 7 (50%) |
| On NNRTI based regimen prior to diagnosis | 12 (85.7%) |
| On PI based regimen prior to diagnosis | 2 (14.2%) |
| VL obtained (for those on ART > 6 months at diagnosis) | 7 (n = 7) |
| VL < 1000 cp/mL | 2 (37.5%) |
| VL > 1000 cp/mL | 5 (62.5%) |
| IRIS | 4 (25%) |
| Clinical Characteristic | Upfront Paclitaxel (n = 5) | Relapse KS (n = 4) | Treatment Failure (n = 8) | No Paclitaxel (n = 54) | p-Value |
|---|---|---|---|---|---|
| Alive | 100% (5/5) | 75% (3/4) | 75% (6/8) | 70% (38/54) | 0.64 |
| Died | 0% (0/5) | 25% (1/4) | 25% (2/8) | 30% (16/54) | 0.64 |
| CCR | 100% (5/5) | 75% (3/4) | 38% (3/8) ‡ | 54% (29/54) | 0.08 |
| PR | 0% (0/5) | 0% (0/4) | 38% (3/8) | 17% (9/54) | 0.35 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adinani, H.; Campbell, L.; El-Mallawany, N.K.; Slone, J.; Mehta, P.; Bacha, J. Use of Paclitaxel to Successfully Treat Children, Adolescents, and Young Adults with Kaposi Sarcoma in Southwestern Tanzania. Children 2021, 8, 275. https://doi.org/10.3390/children8040275
Adinani H, Campbell L, El-Mallawany NK, Slone J, Mehta P, Bacha J. Use of Paclitaxel to Successfully Treat Children, Adolescents, and Young Adults with Kaposi Sarcoma in Southwestern Tanzania. Children. 2021; 8(4):275. https://doi.org/10.3390/children8040275
Chicago/Turabian StyleAdinani, Hamidu, Liane Campbell, Nader Kim El-Mallawany, Jeremy Slone, Parth Mehta, and Jason Bacha. 2021. "Use of Paclitaxel to Successfully Treat Children, Adolescents, and Young Adults with Kaposi Sarcoma in Southwestern Tanzania" Children 8, no. 4: 275. https://doi.org/10.3390/children8040275