
The Effect of Antibiotic Treatment of Early Childhood Shigellosis on Long-Term Prevalence of Attention Deficit/Hyperactivity Disorder

Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
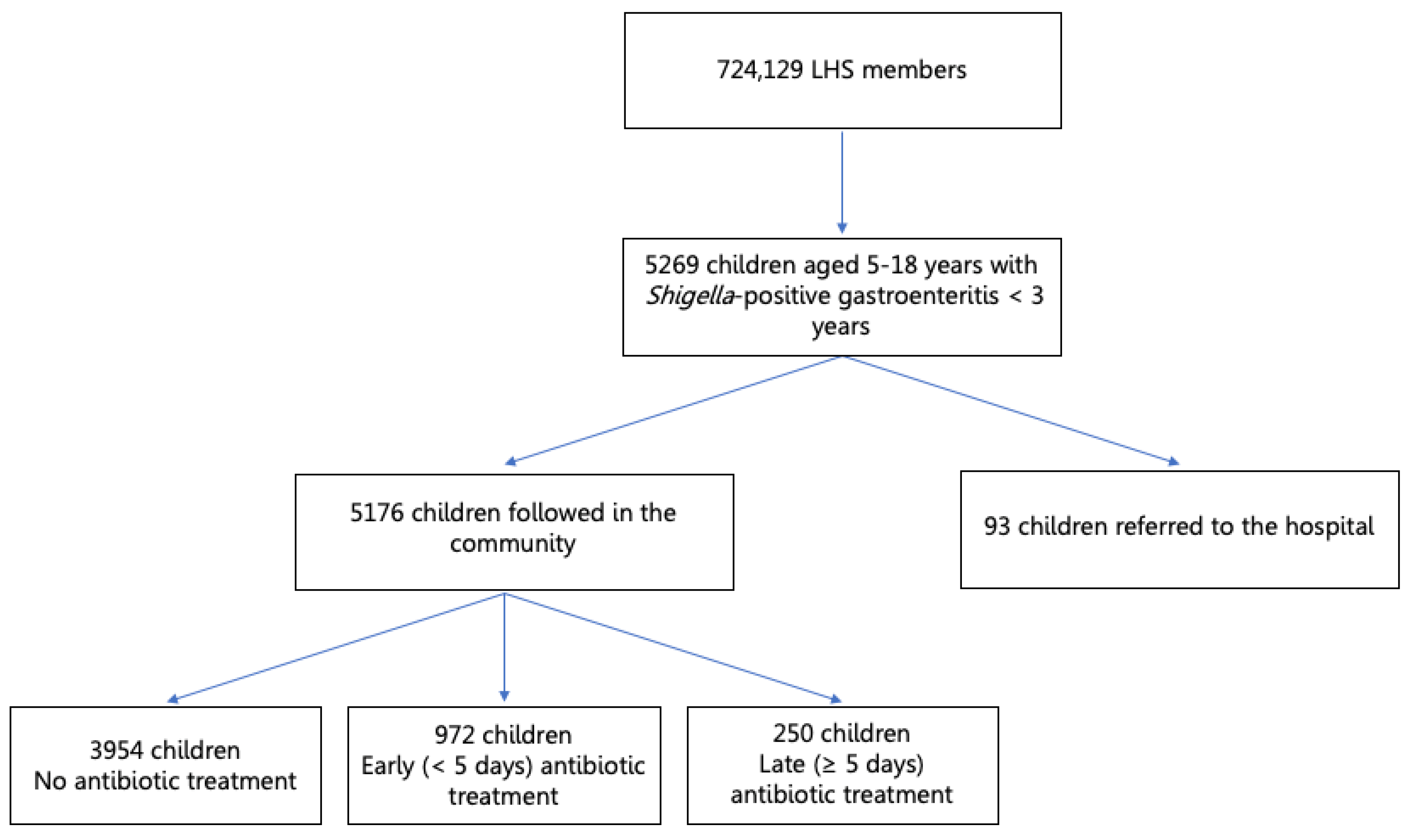
3.1. Study Population
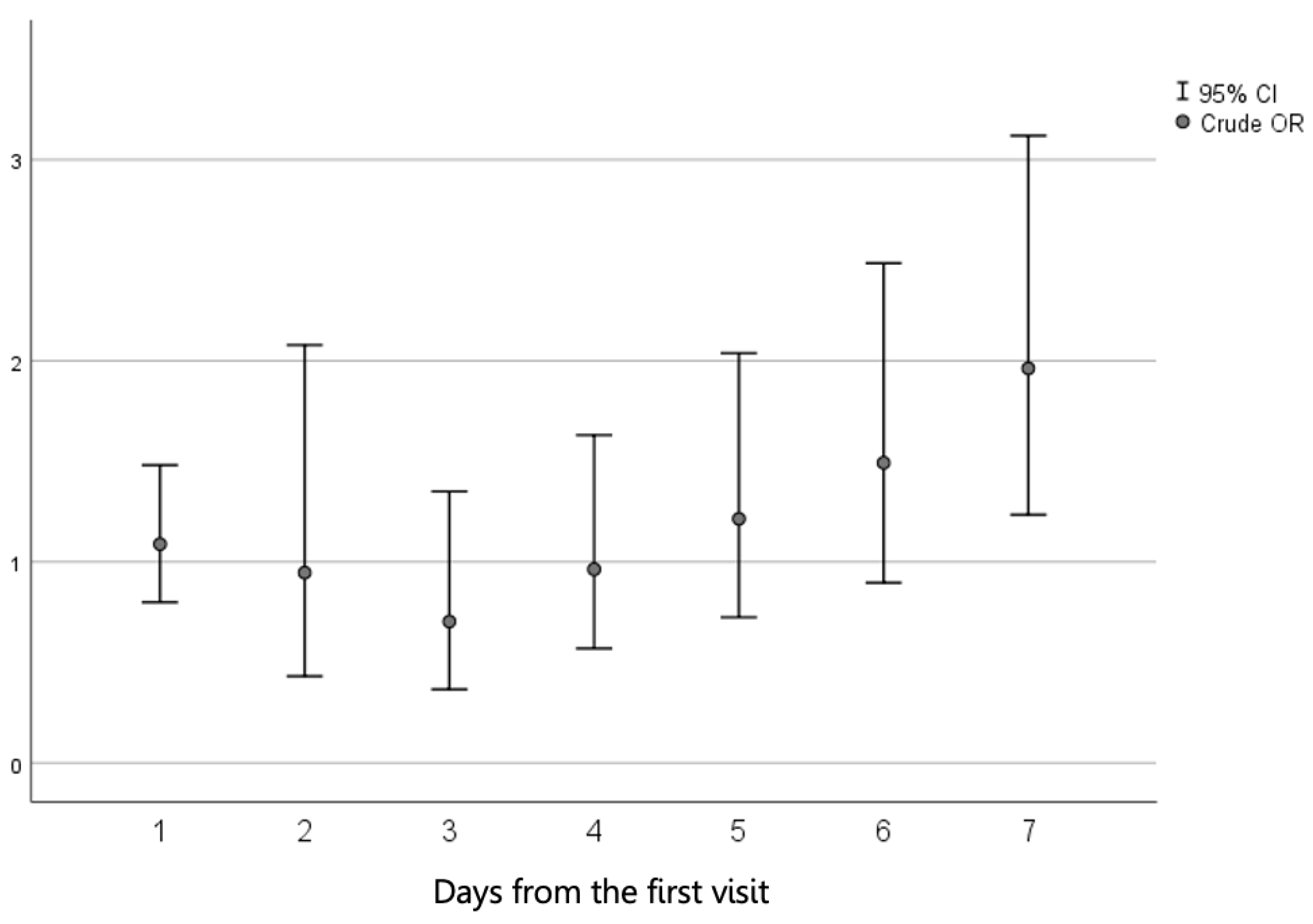
3.2. Univariable Analysis
3.3. Multivariable Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kotloff, K.L.; Riddle, M.S.; Platts-Mills, J.A.; Pavlinac, P.; Zaidi, A.K.M. Shigellosis. Lancet 2018, 391, 801–812. [Google Scholar] [CrossRef]
- Kotloff, K.L.; Nataro, J.P.; Blackwelder, W.C.; Nasrin, D.; Farag, T.H.; Panchalingam, S.; Wu, Y.; Sow, S.O.; Sur, D.; Breiman, R.F.; et al. Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the Global Enteric Multicenter Study, GEMS): A prospective, case-control study. Lancet 2013, 382, 209–222. [Google Scholar] [CrossRef]
- Mattock, E.; Blocker, A.J. How Do the Virulence Factors of Shigella Work Together to Cause Disease? Front. Cell. Infect. Microbiol. 2017, 7, 64. [Google Scholar] [CrossRef]
- Baker, S.; The, H.C. Recent insights into Shigella: A major contributor to the global diarrhoeal disease burden. Curr. Opin. Infect. Dis. 2018, 31, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Tickell, K.D.; Brander, R.L.; E Atlas, E.H.; Pernica, J.M.; Walson, J.L.; Pavlinac, P.B. Identification and management of Shigella infection in children with diarrhoea: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e1235–e1248. [Google Scholar] [CrossRef] [Green Version]
- Khan, W.A.; Dhar, U.; Salam, M.A.; Griffiths, J.K.; Bennish, M.L. Central Nervous System Manifestations of Childhood Shigellosis: Prevalence, Risk Factors, and Outcome. Pediatrics 1999, 103, e18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merzon, E.; Gutbir, Y.; Vinker, S.; Cohen, A.G.; Horwitz, D.; Ashkenazi, S.; Sadaka, Y. Early Childhood Shigellosis and Attention Deficit Hyperactivity Disorder: A Population-Based Cohort Study with a Prolonged Follow-up. J. Atten. Disord. 2021, 25, 1791–1800. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, C.J. Neurodevelopmental Abnormalities in ADHD. Behav. Neurobiol. Psychedelic Drugs 2011, 9, 49–66. [Google Scholar] [CrossRef] [Green Version]
- Thapar, A.; Cooper, M. Attention deficit hyperactivity disorder. Lancet 2016, 387, 1240–1250. [Google Scholar] [CrossRef]
- Bennish, M.L.; Khan, W.A.; Begum, M.; Bridges, E.A.; Ahmed, S.; Saha, D.; Salam, M.A.; Acheson, D.; Ryan, E.T. Low Risk of Hemolytic Uremic Syndrome after Early Effective Antimicrobial Therapy for Shigella dysenteriae Type 1 Infection in Bangladesh. Clin. Infect. Dis. 2006, 42, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Ashkenazi, S. Shigella infections in children: New insights. Semin. Pediatr. Infect. Dis. 2004, 15, 246–252. [Google Scholar] [CrossRef] [Green Version]
- Sharon, G.; Sampson, T.; Geschwind, D.H.; Mazmanian, S.K. The Central Nervous System and the Gut Microbiome. Cell 2016, 167, 915–932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ihekweazu, F.D.; Versalovic, J. Development of the Pediatric Gut Microbiome: Impact on Health and Disease. Am. J. Med Sci. 2018, 356, 413–423. [Google Scholar] [CrossRef] [Green Version]
- Pfefferbaum, A.; Mathalon, D.H.; Sullivan, E.V.; Rawles, J.M.; Zipursky, R.B.; Lim, K.O. A Quantitative Magnetic Resonance Imaging Study of Changes in Brain Morphology from Infancy to Late Adulthood. Arch. Neurol. 1994, 51, 874–887. [Google Scholar] [CrossRef] [PubMed]
- Benakis, C.; Martin-Gallausiaux, C.; Trezzi, J.-P.; Melton, P.; Liesz, A.; Wilmes, P. The microbiome-gut-brain axis in acute and chronic brain diseases. Curr. Opin. Neurobiol. 2020, 61, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Dinan, T.; Cryan, J.F. Gut instincts: Microbiota as a key regulator of brain development, ageing and neurodegeneration. J. Physiol. 2016, 595, 489–503. [Google Scholar] [CrossRef]
- Borre, Y.E.; O’Keeffe, G.; Clarke, G.; Stanton, C.; Dinan, T.; Cryan, J.F. Microbiota and neurodevelopmental windows: Implications for brain disorders. Trends Mol. Med. 2014, 20, 509–518. [Google Scholar] [CrossRef] [PubMed]
- Warner, B.B. The contribution of the gut microbiome to neurodevelopment and neuropsychiatric disorders. Pediatr. Res. 2019, 85, 216–224. [Google Scholar] [CrossRef] [Green Version]
- Angelucci, F.; Cechova, K.; Amlerova, J.; Hort, J. Antibiotics, gut microbiota, and Alzheimer’s disease. J. Neuroinflammation 2019, 16, 1–10. [Google Scholar] [CrossRef]
- Caputi, V.; Giron, M.C. Microbiome-Gut-Brain Axis and Toll-Like Receptors in Parkinson’s Disease. Int. J. Mol. Sci. 2018, 19, 1689. [Google Scholar] [CrossRef] [Green Version]
- Bull-Larsen, S.; Mohajeri, M.H. The Potential Influence of the Bacterial Microbiome on the Development and Progression of ADHD. Nutrients 2019, 11, 2805. [Google Scholar] [CrossRef] [Green Version]
- Mathee, K.; Cickovski, T.; Deoraj, A.; Stollstorff, M.; Narasimhan, G. The gut microbiome and neuropsychiatric disorders: Implications for attention deficit hyperactivity disorder (ADHD). J. Med Microbiol. 2020, 69, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Grill, M.F.; Maganti, R.K. Neurotoxic effects associated with antibiotic use: Management considerations. Br. J. Clin. Pharmacol. 2011, 72, 381–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grill, M.F.; Maganti, R. Cephalosporin-Induced Neurotoxicity: Clinical Manifestations, Potential Pathogenic Mechanisms, and the Role of Electroencephalographic Monitoring. Ann. Pharmacother. 2008, 42, 1843–1850. [Google Scholar] [CrossRef]
- Neuman, H.; Forsythe, P.; Uzan, A.; Avni, O.; Koren, O. Antibiotics in early life: Dysbiosis and the damage done. FEMS Microbiol. Rev. 2018, 42, 489–499. [Google Scholar] [CrossRef] [Green Version]
- Slykerman, R.F.; Thompson, J.; Waldie, K.; Murphy, R.; Wall, C.; Mitchell, E.A. Antibiotics in the first year of life and subsequent neurocognitive outcomes. Acta Paediatr. 2017, 106, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Ornoy, A.; Ovadia, M.; Rivkin, D.; Milshtein, E.; Barlev, L. Prevalence of ADHD among 7-9-Year-Old Children in Israel. A Comparison between Jewish and Arab Populations. Isr. J. Psychiatry Relat. Sci. 2016, 53, 3–8. [Google Scholar]



{kind=link}
{kind=link}
| Demographic Variables | Antibiotic Treatment for Shigella Gastroenteritis | p | ||
|---|---|---|---|---|
| No Antibiotic Treatment Number (%) (n = 3954) | Early Antibiotic Treatment Number (%) (n = 972) | Late Antibiotic Treatment Number (%) (n = 250) | ||
| Gender | ||||
| Male | 2191 (55.4) | 521 (53.6) | 136 (54.4) | 0.584 |
| Female | 1763 (44.6) | 451 (46.4) | 114 (45.6) | |
| Ethnicity | ||||
| Secular Jewish | 2347 (59.4) | 548 (56.4) | 142 (56.8) | 0.353 |
| Orthodox Jewish | 1269 (32.1) | 344 (35.4) | 84 (33.6) | |
| Israeli Arab | 338 (8.5) | 80 (8.2) | 24 (9.6) | |
| SES | ||||
| High | 323 (9.0) | 79 (9.0) | 21 (9.5) | 0.084 |
| Middle | 1653 (46.1) | 370 (42.0) | 88 (39.6) | |
| Low | 1607 (44.9) | 432 (49.0) | 113 (50.9) | |
| Age at positive stool culture examination | ||||
| 0–3 months | 659 (16.7) | 148 (15.2) | 41 (16.4) | 0.626 |
| 4–12 months | 1562 (39.5) | 380 (39.1) | 90 (36.0) | |
| 13–24 months | 1039 (26.3) | 263 (27.1) | 65 (26.0) | |
| 25–36 months | 694 (17.6) | 181 (18.6) | 54 (21.6) | |
| Patient Variable | ADHD | p | Crude OR (95% CI) p | ||
|---|---|---|---|---|---|
| No Number (%) (n = 4630) | Yes Number (%) (n = 546) | ||||
| Antibiotic treatment for Shigella infection | Treatment within 5 days of the clinic visit | 871 (18.8) | 101 (18.5) | 0.008 | 1.01 (0.80–1.28) 0.873 |
| Treatment ≥ 5 days of the clinic visit | 209 (4.5) | 41 (7.5) | 1.72 (1.21–2.44) 0.002 | ||
| No antibiotic treatment | 3550 (76.7) | 404 (74.0) | Reference group | ||
| Gender | Male | 2467 (53.3) | 381 (69.8) | <0.001 | 2.01 (1.67–2.45) <0.001 |
| Female | 2163 (46.7) | 165 (30.2) | |||
| SES | High | 367 (8.8) | 56 (11.3) | 0.002 | 1.55 (1.13–2.14) 0.006 |
| Middle | 1864 (44.5) | 247 (49.9) | 1.35 (1.10–1.65) 0.003 | ||
| Low | 1960 (46.8) | 192 (38.8) | Reference group | ||
| Age at positive culture (months) | 0–3 months | 762 (16.5) | 86 (15.8) | 0.383 | 0.895 (0.662–1.21) 0.473 |
| 4–12 months | 1833 (39.6) | 199 (36.4) | 0.861 (0.67–1.10) 0.243 | ||
| 13–24 months | 1210 (26.1) | 157 (28.8) | 1.029 (0.79–1.33) 0.830 | ||
| 25–36 months | 825 (17.8) | 104 (19) | Reference group | ||
| Variable | Adj. OR | 95% CI | p |
|---|---|---|---|
| Antibiotic treatment (<5 days vs. no treatment) | 1.02 | 0.80–1.31 | 0.817 |
| Antibiotic treatment (≥5 days vs. no treatment) | 1.61 | 1.10–2.37 | 0.015 |
| Gender (male vs. female) | 2.08 | 1.70–2.55 | < 0.001 |
| SES (middle vs. low) | 1.40 | 1.15–1.72 | 0.001 |
| SES (high vs. low) | 1.60 | 1.16–2.20 | 0.004 |
| Age at positive Shigella culture (0–3 months vs. 25–36 months) | 0.829 | 0.59–1.14 | 0.258 |
| Age at positive Shigella culture (4–12 months vs. 25–36 months) | 0.879 | 0.67–1.15 | 0.348 |
| Age at positive Shigella culture (13–24 months vs. 25–36 months) | 1.02 | 0.77–1.35 | 0.869 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sadaka, Y.; Freedman, J.; Ashkenazi, S.; Vinker, S.; Golan-Cohen, A.; Green, I.; Israel, A.; Eran, A.; Merzon, E. The Effect of Antibiotic Treatment of Early Childhood Shigellosis on Long-Term Prevalence of Attention Deficit/Hyperactivity Disorder. Children 2021, 8, 880. https://doi.org/10.3390/children8100880
Sadaka Y, Freedman J, Ashkenazi S, Vinker S, Golan-Cohen A, Green I, Israel A, Eran A, Merzon E. The Effect of Antibiotic Treatment of Early Childhood Shigellosis on Long-Term Prevalence of Attention Deficit/Hyperactivity Disorder. Children. 2021; 8(10):880. https://doi.org/10.3390/children8100880
Chicago/Turabian StyleSadaka, Yair, Judah Freedman, Shai Ashkenazi, Shlomo Vinker, Avivit Golan-Cohen, Ilan Green, Ariel Israel, Alal Eran, and Eugene Merzon. 2021. "The Effect of Antibiotic Treatment of Early Childhood Shigellosis on Long-Term Prevalence of Attention Deficit/Hyperactivity Disorder" Children 8, no. 10: 880. https://doi.org/10.3390/children8100880