COVID-19: Neurological Considerations in Neonates and Children

Abstract
:1. Introduction
2. COVID-19 in Neonates and Children
3. Neurological Involvement in COVID-19
3.1. Cerebrovascular Disease
3.2. Encephalitis
3.3. Seizures and Other CNS Symptoms
3.4. Hypogeusia, Hyposmia
3.5. Demyelinating Disorders
3.6. Examples of Children with Neurological Involvement
4. Neurological Signs and Symptoms in Multi-System Inflammatory Syndrome (MIS-C)
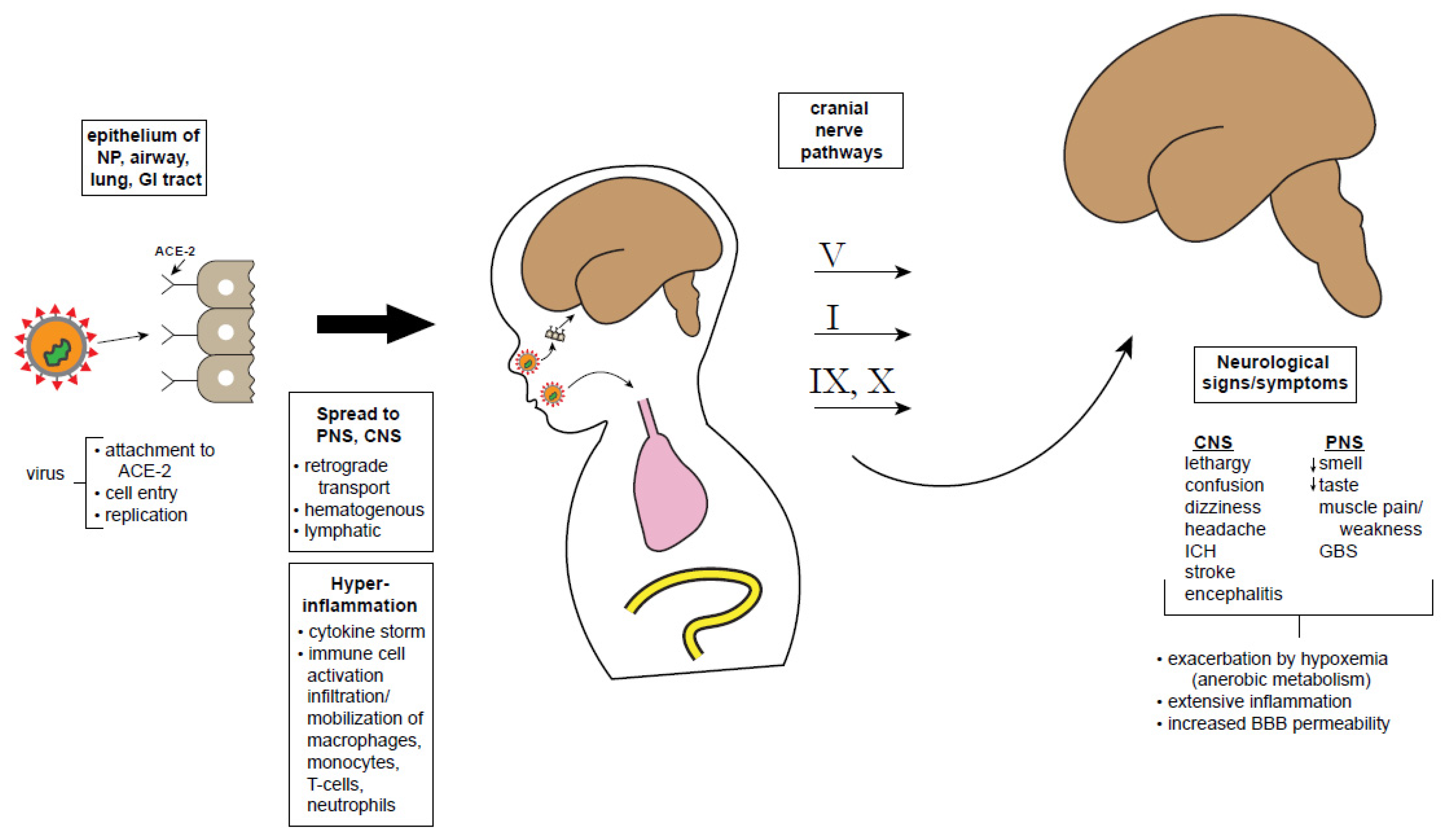
5. Coronavirus Infectivity
6. SARS-CoV-2 Neurologic Mechanisms
7. Conclusions—A Cautionary Tale
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baig, A.M.; Khaleeq, A.; Ali, U.; Syeda, H. Evidence of the COVID-19 Virus Targeting the CNS: Tissue Distribution, Host–Virus Interaction, and Proposed Neurotropic Mechanisms. ACS Chem. Neurosci. 2020, 11, 995–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.; Xu, X.; Chen, Z.; Duan, J.; Hashimoto, K.; Yang, L.; Liu, C.; Yang, C. Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain Behav. Immun. 2020, 87, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Paterson, R.W.; Brown, R.L.; Benjamin, L.; Nortley, R.; Wiethoff, S.; Bharucha, T.; Jayaseelan, D.L.; Kumar, G.; Raftopoulos, R.E.; Zambreanu, L.; et al. The emerging spectrum of COVID-19 neurology: Clinical, radiological and laboratory findings. Brain 2020, 8, awaa240. [Google Scholar] [CrossRef]
- Koralnik, I.J.; Tyler, K.L. COVID -19: A Global Threat to the Nervous System. Ann. Neurol. 2020, 88, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Bohmwald, K.; Gálvez, N.M.S.; Ríos, M.; Kalergis, A.M. Neurologic Alterations Due to Respiratory Virus Infections. Front. Cell. Neurosci. 2018, 12, 386. [Google Scholar] [CrossRef] [PubMed]
- Montalvan, V.; Lee, J.; Bueso, T.; De Toledo, J.; Rivas, K. Neurological manifestations of COVID-19 and other coronavirus infections: A systematic review. Clin. Neurol. Neurosurg. 2020, 194, 105921. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Liu, T.; Yang, N.; Han, D.; Mi, X.; Li, Y.; Liu, K.; Vuylsteke, A.; Xiang, H.; Guo, X. Neurological manifestations of patients with COVID-19: Potential routes of SARS-CoV-2 neuroinvasion from the periphery to the brain. Front. Med. 2020, 1–9. [Google Scholar] [CrossRef]
- Atluri, V.S.R.; Hidalgo, M.; Samikkannu, T.; Kurapati, K.R.V.; Nair, M.P.N. Synaptic Plasticity and Neurological Disorders in Neurotropic Viral Infections. Neural Plast. 2015, 2015, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Dong, Y.; Mo, X.; Hu, Y.; Qi, X.; Jiang, F.; Jiang, Z.; Tong, S. Epidemiology of COVID-19 among Children in China. Pediatrics 2020, 145, e20200702. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China. JAMA 2020, 323, 1239. [Google Scholar] [CrossRef] [PubMed]
- Tezer, H.; Demirdağ, T.B. Novel coronavirus disease (COVID-19) in children. Turk. J. Med Sci. 2020, 50, 592–603. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, P.; Curtis, N. Coronavirus Infections in Children Including COVID-19. Pediatr. Infect. Dis. J. 2020, 39, 355–368. [Google Scholar] [CrossRef] [PubMed]
- Brodin, P. Why is COVID-19 so mild in children. Acta Paediatr. 2020, 109, 1082–1083. [Google Scholar] [CrossRef] [PubMed]
- Baig, A.M. Neurological manifestations in COVID-19 caused by SARS-CoV-2. CNS Neurosci. Ther. 2020, 26, 499–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simon, A.K.; Holländer, G.A.; McMichael, A.J. Evolution of the immune system in humans from infancy to old age. Proc. R. Soc. B Biol. Sci. 2015, 282, 20143085. [Google Scholar] [CrossRef]
- Sposato, B.; Scalese, M. Why do children seem to be more protected against COVID-19? A hypothesis. Med. Hypotheses 2020, 143, 110151. [Google Scholar] [CrossRef]
- Zhu, L.Q.; Lu, X.; Chen, L. Possible causes for decreased susceptibility of children to coronavirus. Pediatr. Res. 2020, 1–3. [Google Scholar] [CrossRef]
- Zimmermann, P.; Curtis, N. COVID-19 in Children, Pregnancy and Neonates. Pediatr. Infect. Dis. J. 2020, 39, 469–477. [Google Scholar] [CrossRef]
- Verdoni, L.; Mazza, A.; Gervasoni, A.; Martelli, L.; Ruggeri, M.; Ciuffreda, M.; Bonanomi, E.; D’Antiga, L. An outbreak of severe Kawasaki-like disease at the Italian epicentre of the SARS-CoV-2 epidemic: An observational cohort study. Lancet 2020, 395, 1771–1778. [Google Scholar] [CrossRef]
- Riphagen, S.; Gomez, X.; Gonzalez-Martinez, C.; Wilkinson, N.; Theocharis, P. Hyperinflammatory shock in children during COVID-19 pandemic. Lancet 2020, 395, 1607–1608. [Google Scholar] [CrossRef]
- Sisman, J.; Jaleel, M.A.; Moreno, W.; Rajaram, V.; Collins, R.R.; Savani, R.C.; Rakheja, D.; Evans, A.S. Intrauterine transmission of sars-cov-2 infection in a preterm infant. Pediatr. Infect. Dis. J. 2020, 39, 2265–2267. [Google Scholar] [CrossRef] [PubMed]
- Kirtsman, M.; Diambomba, Y.; Poutanen, S.M.; Malinowski, A.K.; Vlachodimitropoulou, E.; Parks, W.T.; Erdman, L.; Morris, S.K.; Shah, P.S. Probable congenital SARS-CoV-2 infection in a neonate born to a woman with active SARS-CoV-2 infection. Can. Med. Assoc. J. 2020, 192, E647–E650. [Google Scholar] [CrossRef] [PubMed]
- Vivanti, A.J.; Vauloup-Fellous, C.; Prevot, S.; Zupan, V.; Suffee, C.; Cao, J.D.; Benachi, A.; De Luca, D. Transplacental transmission of SARS-CoV-2 infection. Nat. Commun. 2020, 11, 3572. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Guo, J.; Wang, C.; Luo, F.; Yu, X.; Zhang, W.; Li, J.; Zhao, D.; Xu, D.; Gong, Q.; et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: A retrospective review of medical records. Lancet 2020, 395, 809–815. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Dong, L.; Ming, L.; Wei, M.; Li, J.; Hu, R.; Yang, J. Severe acute respiratory syndrome coronavirus 2(SARS-CoV-2) infection during late pregnancy: A report of 18 patients from Wuhan, China. BMC Pregnancy Childbirth 2020, 20, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Zeng, L.; Xia, S.; Yuan, W.; Yan, K.; Xiao, F.; Shao, J.; Zhou, W. Neonatal Early-Onset Infection With SARS-CoV-2 in 33 Neonates Born to Mothers With COVID-19 in Wuhan, China. JAMA Pediatr. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, W.; Wang, J.; Li, W.; Zhou, Z.; Liu, S.; Rong, Z. Clinical characteristics of 19 neonates born to mothers with COVID-19. Front. Med. 2020, 14, 193–198. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, D.A. An Analysis of 38 Pregnant Women with COVID-19, Their Newborn Infants, and Maternal-Fetal Transmission of SARS-CoV-2: Maternal Coronavirus Infections and Pregnancy Outcomes. Arch. Pathol. Lab. Med. 2020, 144, 799–805. [Google Scholar] [CrossRef] [Green Version]
- Lu, Q.; Shi, Y. Coronavirus disease (COVID-19) and neonate: What neonatologist need to know. J. Med. Virol. 2020, 92, 564–567. [Google Scholar] [CrossRef] [Green Version]
- Salvatore, C.M.; Han, J.-Y.; Acker, K.P.; Tiwari, P.; Jin, J.; Brandler, M.; Cangemi, C.; Gordon, L.; Parow, A.; DiPace, J.; et al. Neonatal management and outcomes during the COVID-19 pandemic: An observation cohort study. Lancet Child Adolesc. Health 2020, 2352. [Google Scholar] [CrossRef]
- Wei, M.; Yuan, J.; Liu, Y.; Fu, T.; Yu, X.; Zhang, Z.-J. Novel Coronavirus Infection in Hospitalized Infants Under 1 Year of Age in China. JAMA 2020, 323, 1313. [Google Scholar] [CrossRef] [PubMed]
- Piersigilli, F.; Carkeek, K.; Hocq, C.; Van Grambezen, B.; Hubinont, C.; Chatzis, O.; Van Der Linden, D.; Danhaive, O. COVID-19 in a 26-week preterm neonate. Lancet Child Adolesc. Heal. 2020, 4, 476–478. [Google Scholar] [CrossRef]
- Mehan, A.; Venkatesh, A.; Girish, M. COVID-19 in pregnancy: Risk of adverse neonatal outcomes. J. Med. Virol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Abdoli, A.; Falahi, S.; Kenarkoohi, A.; Shams, M.; Mir, H.; Jahromi, M.A.M. The COVID-19 pandemic, psychological stress during pregnancy, and risk of neurodevelopmental disorders in offspring: A neglected consequence. J. Psychosom. Obstet. Gynecol. 2020, 1–2. [Google Scholar] [CrossRef]
- Li, Q. Psychosocial and coping responses towards 2019 coronavirus diseases (COVID-19): A cross-sectional study within the Chinese general population. QJM 2020, 17, hcaa226. [Google Scholar] [CrossRef]
- Berthelot, N.; Lemieux, R.; Garon-Bissonnette, J.; Drouin-Maziade, C.; Martel, É.; Maziade, M. Uptrend in distress and psychiatric symptomatology in pregnant women during the coronavirus disease 2019 pandemic. Acta Obstet. Gynecol. Scand. 2020, 99, 848–855. [Google Scholar] [CrossRef] [PubMed]
- Jiao, W.Y.; Na Wang, L.; Liu, J.; Fang, S.F.; Jiao, F.Y.; Pettoello-Mantovani, M.; Somekh, E. Behavioral and Emotional Disorders in Children during the COVID-19 Epidemic. J. Pediatr. 2020, 221, 264. [Google Scholar] [CrossRef]
- Lackey, K.A.; Pace, R.M.; Williams, J.E.; Bode, L.; Donovan, S.M.; Järvinen, K.M.; Seppo, A.E.; Raiten, D.J.; Meehan, C.L.; McGuire, M.A.; et al. SARS-CoV-2 and human milk: What is the evidence. Matern. Child Nutr. 2020, e13032. [Google Scholar] [CrossRef]
- Mimouni, F.; Lakshminrusimha, S.; Pearlman, S.A.; Raju, T.; Gallagher, P.G.; Mendlovic, J. Perinatal aspects on the covid-19 pandemic: A practical resource for perinatal–neonatal specialists. J. Perinatol. 2020, 40, 820–826. [Google Scholar] [CrossRef]
- Puopolo, K.M.; Hudak, M.L.; Kimberlin, D.W.; Cummings, J. Initial Guidance: Management of Infants Born to Mothers with COVID-19; American Academy of Pediatrics Committee on Fetus and Newborn, Section on Neonatal Perinatal Medicine, and Commitee on Infectious Diseases: Washington, DC, USA, 2020. [Google Scholar]
- Chen, D.; Yang, H.; Cao, Y.; Cheng, W.; Duan, T.; Fan, C.; Fan, S.; Feng, L.; Gao, Y.; He, F.; et al. Expert consensus for managing pregnant women and neonates born to mothers with suspected or confirmed novel coronavirus ( COVID -19) infection. Int. J. Gynecol. Obstet. 2020, 149, 130–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asadi-Pooya, A.A.; Simani, L. Central nervous system manifestations of COVID-19: A systematic review. J. Neurol. Sci. 2020, 413, 116832. [Google Scholar] [CrossRef] [PubMed]
- Needham, E.J.; Chou, S.H.-Y.; Coles, A.J.; Menon, D.K. Neurological Implications of COVID-19 Infections. Neurocrit. Care 2020, 32, 667–671. [Google Scholar] [CrossRef] [PubMed]
- Paybast, S.; Emami, A.; Koosha, M.; Baghalha, F. Novel Coronavirus Disease (COVID-19) and Central Nervous System Complications: What Neurologist Need to Know. Acta Neurol. Taiwan 2020, 29, 24–31. [Google Scholar] [PubMed]
- Helms, J.; Kremer, S.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Kummerlen, C.; Collange, O.; Boulay, C.; Fafi-Kremer, S.; Ohana, M.; et al. Neurologic features in severe SARS-CoV-2 infection. N. Engl. J. Med. 2020, 382, 2268–2270. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Gomes, J. Neuropathogenesis of SARS-CoV-2 infection. Elife 2020, 9, 59136. [Google Scholar] [CrossRef] [PubMed]
- Oxley, T.J.; Mocco, J.; Majidi, S.; Kellner, C.P.; Shoirah, H.; Singh, I.P.; De Leacy, R.A.; Shigematsu, T.; Ladner, T.R.; Yaeger, K.A.; et al. Large-Vessel Stroke as a Presenting Feature of Covid-19 in the Young. N. Engl. J. Med. 2020, 382, e60. [Google Scholar] [CrossRef]
- Beyrouti, R.E.; Adams, M.; Benjamin, L.; Cohen, H.; Farmer, S.F.; Goh, Y.Y.; Humphries, F.; Jäger, H.R.A.; Losseff, N.; Perry, R.J.; et al. Characteristics of ischaemic stroke associated with COVID-19. J. Neurol. Neurosurg. Psychiatry 2020, 91, 889–891. [Google Scholar] [CrossRef]
- Christy, A. COVID-19: A Review for the Pediatric Neurologist. J. Child Neurol. 2020. [Google Scholar] [CrossRef]
- Pilotto, A.; Odolini, S.; Masciocchi, S.S.; Comelli, A.; Volonghi, I.; Gazzina, S.; Nocivelli, S.; Pezzini, A.; Focà, E.; Caruso, A.; et al. Steroid-Responsive Encephalitis in Coronavirus Disease 2019. Ann. Neurol. 2020, 88, 423–427. [Google Scholar] [CrossRef]
- Von Weyhern, C.H.; Kaufmann, I.; Neff, F.; Kremer, M. Early evidence of pronounced brain involvement in fatal COVID-19 outcomes. Lancet 2020, 395, e109. [Google Scholar] [CrossRef]
- Solomon, I.H.; Normandin, E.; Bhattacharyya, S.; Mukerji, S.S.; Keller, K.; Ali, A.S.; Adams, G.; Hornick, J.L.; Padera, R.F.; Sabeti, P. Neuropathological Features of Covid-19. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Schaller, T.; Hirschbühl, K.; Burkhardt, K.; Braun, G.; Trepel, M.; Märkl, B.; Claus, R. Postmortem Examination of Patients With COVID-19. JAMA 2020, 323, 2518. [Google Scholar] [CrossRef] [PubMed]
- Sohal, S.; Mansur, M.; Mossammat, M. COVID-19 Presenting with Seizures. IDCases 2020, 20, e00782. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, N. Epilepsy and COVID-19: Associations and important considerations. Epilepsy Behav. 2020, 108, 107122. [Google Scholar] [CrossRef] [PubMed]
- Galanopoulou, A.S.; Ferastraoaru, V.; Correa, D.J.; Cherian, K.; Duberstein, S.; Gursky, J.; Hanumanthu, R.; Hung, C.; Molinero, I.; Khodakivska, O.; et al. EEG findings in acutely ill patients investigated for SARS-CoV-2/COVID-19: A small case series preliminary report. Epilepsia Open 2020, 5, 314–324. [Google Scholar] [CrossRef] [PubMed]
- Petrescu, A.-M.; Taussig, D.; Bouilleret, V. Electroencephalogram (EEG) in COVID-19: A systematic retrospective study. Neurophysiol. Clin. Neurophysiol. 2020, 50, 155–165. [Google Scholar] [CrossRef]
- Poncet-Megemont, L.; Paris, P.; Tronchere, A.; Salazard, J.; Pereira, B.; Dallel, R.; Aumeran, C.; Beytout, J.; Jacomet, C.; Laurichesse, H.; et al. High Prevalence of Headaches During Covid-19 Infection: A Retrospective Cohort Study. Headache J. Head Face Pain 2020. [Google Scholar] [CrossRef]
- Gane, S.B.; Kelly, C.; Hopkins, C. Isolated sudden onset anosmia in COVID-19 infection. A novel syndrome. Rhinology 2020, 58, 299–301. [Google Scholar] [CrossRef]
- Sedaghat, A.R.; Gengler, I.; Speth, M.M. Olfactory Dysfunction: A Highly Prevalent Symptom of COVID-19 with Public Health Significance. Otolaryngol. Neck Surg. 2020, 163, 12–15. [Google Scholar] [CrossRef]
- Cooper, K.W.; Brann, D.H.; Farruggia, M.C.; Bhutani, S.; Pellegrino, R.; Tsukahara, T.; Weinreb, C.; Joseph, P.V.; Larson, E.D.; Parma, V.; et al. COVID-19 and the Chemical Senses: Supporting Players Take Center Stage. Neuron 2020, 107, 219–233. [Google Scholar] [CrossRef]
- Mak, P.Q.; Chung, K.-S.; Wong, J.S.-C.; Shek, C.-C.; Kwan, M.Y.-W. Anosmia and Ageusia: Not an Uncommon Presentation of COVID-19 Infection in Children and Adolescents. Pediatr. Infect. Dis. J. 2020, 39, e199–e200. [Google Scholar] [CrossRef] [PubMed]
- Alberti, P.; Beretta, S.; Piatti, M.; Karantzoulis, A.; Piatti, M.L.; Santoro, P.; Viganò, M.; Giovannelli, G.; Pirro, F.; Montisano, D.A.; et al. Guillain-Barré syndrome related to COVID-19 infection. Neurol. Neuroimmunol. Neuroinflamm. 2020, 7, e741. [Google Scholar] [CrossRef] [PubMed]
- Dalakas, M.C. Guillain-Barré syndrome: The first documented COVID-19–triggered autoimmune neurologic disease. Neurol. Neuroimmunol. Neuroinflamm. 2020, 7, e781. [Google Scholar] [CrossRef] [PubMed]
- Khalifa, M.; Zakaria, F.; Ragab, Y.; Saad, A.; Bamaga, A.; Emad, Y.; Rasker, J.J. Guillain-Barré syndrome associated with severe accute respiratory syndrome coronoavirus 2 detection and coronavirus disease 2019 in a child. J. Pediatr. Infect. Dis. Soc. 2020, 11, piaa086. [Google Scholar] [CrossRef]
- Frank, C.H.M.; Almeida, T.V.R.; Marques, E.A.; de Sousa Monteiro, Q.; Feitoza, P.V.S.; Borba, M.G.S.; Vasconcelos, H.L.; de Souza Bastos, M.; Lacerda, M.V.G. Guillain-Barré syndrome associated with SARS-CoV-2 infection in a pediatric patient. J. Trop. Pediatr. 2020, 12, fmaa044. [Google Scholar] [CrossRef]
- Boziki, M.K.; Mentis, A.-F.A.; Shumilina, M.; Makshakov, G.; Evdoshenko, E.; Grigoriadis, N. COVID-19 Immunopathology and the Central Nervous System: Implication for Multiple Sclerosis and Other Autoimmune Diseases with Associated Demyelination. Brain Sci. 2020, 10, 345. [Google Scholar] [CrossRef]
- Berger, J.R.; Brandstadter, R.; Bar-Or, A. COVID-19 and MS disease-modifying therapies. Neurol. Neuroimmunol. Neuroinflamm. 2020, 7, e761. [Google Scholar] [CrossRef]
- De Rose, D.; Piersigilli, F.; Ronchetti, M.P.; Santisi, A.; Bersani, I.; Dotta, A.; Danhaive, O.; Auriti, C. The Study Group of Neonatal Infectious Diseases of The Italian Society of Neonatology (SIN); Novel Coronavirus disease (COVID-19) in newborns and infants: What we know so far. Ital. J. Pediatr. 2020, 46, 1–8. [Google Scholar] [CrossRef]
- Nathan, N.; Prevost, B.; Corvol, H. Atypical presentation of COVID-19 in young infants. Lancet 2020, 395, 1481. [Google Scholar] [CrossRef]
- Chacón-Aguilar, R.; Osorio-Cámara, J.M.; Sanjurjo-Jimenez, I.; González-González, C.; López-Carnero, J.; Pérez-Moneo-Agapito, B. COVID-19: Fever syndrome and neurological symptoms in a neonate. An. Pediatr (English Edition) 2020, 92, 373–374. [Google Scholar] [CrossRef]
- Lorenz, N.; Treptow, A.; Schmidt, S.; Hofmann, R.; Raumer-Engler, M.; Heubner, G.; Gröber, K. Neonatal Early-Onset Infection With SARS-CoV-2 in a Newborn Presenting With Encephalitic Symptoms. Pediatr. Infect. Dis. J. 2020. [Google Scholar] [CrossRef] [PubMed]
- Dugue, R.; Cay-Martínez, K.C.; Thakur, K.T.; Garcia, J.A.; Chauhan, L.V.; Williams, S.H.; Briese, T.; Jain, K.; Foca, M.; McBrian, D.K.; et al. Neurologic manifestations in an infant with COVID-19. Neurology 2020, 94, 1100–1102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatta, S.; Sayed, A.; Ranabhat, B.; Bhatta, R.K.; Acharya, Y. New-Onset Seizure as the Only Presentation in a Child With COVID-19. Cureus 2020. [Google Scholar] [CrossRef]
- Nakra, N.A.; Blumberg, D.A.; Herrera-Guerra, A.; Lakshminrusimha, S. Multi-System Inflammatory Syndrome in Children (MIS-C) Following SARS-CoV-2 Infection: Review of Clinical Presentation, Hypothetical Pathogenesis, and Proposed Management. Children 2020, 7, 69. [Google Scholar] [CrossRef]
- Chiotos, K.; Bassiri, K.C.H.; Behrens, E.M.; Blatz, A.M.; Chang, J.; Diorio, C.; Fitzgerald, J.C.; Topjian, A.; Odom John, A.R. Multisystem inflammatory syndrome in children during the COVID-19 pandemic: A case series. J. Pediatr. Infect. Dis. Soc. 2020, 13, 393–398. [Google Scholar] [CrossRef]
- Whittaker, E.; Bamford, A.; Kenny, J.; Kaforou, M.; Jones, C.E.; Shah, P.; Ramnarayan, P.; Fraisse, A.; Miller, O.; Davies, P.; et al. Clinical Characteristics of 58 Children With a Pediatric Inflammatory Multisystem Syndrome Temporally Associated With SARS-CoV-2. JAMA 2020. [Google Scholar] [CrossRef]
- Toubiana, J.; Poirault, C.; Corsia, A.; Bajolle, F.; Fourgeaud, J.; Angoulvant, F.; Debray, A.; Basmaci, R.; Salvador, E.; Biscardi, S.; et al. Kawasaki-like multisystem inflammatory syndrome in children during the covid-19 pandemic in Paris, France: Prospective observational study. BMJ 2020, 369, m2094. [Google Scholar] [CrossRef]
- Feldstein, L.R.; Rose, E.B.; Horwitz, S.M.; Collins, J.P.; Newhams, M.M.; Son, M.B.F.; Newburger, J.W.; Kleinman, L.C.; Heidemann, S.M.; Martin, A.A.; et al. Multisystem Inflammatory Syndrome in U.S. Children and Adolescents. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Abdel-Mannan, O.; Eyre, M.; Löbel, U.; Bamford, A.; Eltze, C.; Hameed, B.; Hemingway, C.; Hacohen, Y. Neurologic and Radiographic Findings Associated With COVID-19 Infection in Children. JAMA Neurol. 2020. [Google Scholar] [CrossRef]
- Kontzialis, M.; Soares, B.P.; Huisman, T.A. Lesions in the Splenium of the Corpus Callosum on MRI in Children: A Review. J. Neuroimaging 2017, 27, 549–561. [Google Scholar] [CrossRef] [PubMed]
- Abrams, J.Y.; Godfred-Cato, S.E.; Oster, M.E.; Chow, E.J.; Koumans, E.H.; Bryant, B.; Leung, J.W.; Belay, E.D. Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with SARS-CoV-2: A Systematic Review. J. Pediatr. 2020, 22. [Google Scholar] [CrossRef] [PubMed]
- Iroegbu, J.D.; Ifenatuoha, C.W.; Ijomone, O.M. Potential neurological impact of coronaviruses: Implications for the novel SARS-CoV-2. Neurol. Sci. 2020, 41, 1329–1337. [Google Scholar] [CrossRef] [PubMed]
- Sungnak, W.; Network, H.L.B.; Huang, N.; Bécavin, C.; Berg, M.; Queen, R.; Litvinukova, M.; Talavera-López, C.; Maatz, H.; Reichart, D.; et al. SARS-CoV-2 entry factors are highly expressed in nasal epithelial cells together with innate immune genes. Nat. Med. 2020, 26, 681–687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schett, G.; Sticherling, M.; Neurath, M.F. COVID-19: Risk for cytokine targeting in chronic inflammatory diseases. Nat. Rev. Immunol. 2020, 20, 271–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coperchini, F.; Chiovato, L.; Croce, L.; Magri, F.; Rotondi, M. The cytokine storm in COVID-19: An overview of the involvement of the chemokine/chemokine-receptor system. Cytokine Growth Factor Rev. 2020, 53, 25–32. [Google Scholar] [CrossRef]
- Channappanavar, R.; Perlman, S. Pathogenic human coronavirus infections: Causes and consequences of cytokine storm and immunopathology. Semin. Immunopathol. 2017, 39, 529–539. [Google Scholar] [CrossRef]
- Kempuraj, D.; Selvakumar, G.P.; Ahmed, M.E.; Raikwar, S.P.; Thangavel, R.; Khan, A.; Zaheer, S.A.; Iyer, S.S.; Burton, C.; James, D.; et al. COVID-19, Mast Cells, Cytokine Storm, Psychological Stress, and Neuroinflammation. Neuroscience 2020, 1–13. [Google Scholar] [CrossRef]
- Jiang, N.M.; Cowan, M.; Moonah, S.N.; Petri, W.A. The Impact of Systemic Inflammation on Neurodevelopment. Trends Mol. Med. 2018, 24, 794–804. [Google Scholar] [CrossRef]
- Nye, S.; Whitley, R.J.; Kong, M.Y.F. Viral Infection in the Development and Progression of Pediatric Acute Respiratory Distress Syndrome. Front. Pediatr. 2016, 4, 128. [Google Scholar] [CrossRef] [Green Version]
- South, A.M.; Brady, T.M.; Flynn, J.T. ACE2, COVID-19, and ACE inhibitor and ARB use during the pandemic: The pediatric perspective. Hypertension 2020, 76, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, E.J.; Manguiat, K.; Wood, H.; Derbot, M. Two detailed plaque assay protocols for the quantification of infectious SARS-CoV-2. Curr. Protoc. Microbiol. 2020, 57, 105. [Google Scholar] [CrossRef] [PubMed]
- Desforges, M.; Le Coupanec, A.; Stodola, J.K.; Meessen-Pinard, M.; Talbot, P.J. Human coronaviruses: Viral and cellular factors involved in neuroinvasiveness and neuropathogenesis. Virus Res. 2014, 194, 145–158. [Google Scholar] [CrossRef] [PubMed]
- Netland, J.; Meyerholz, D.K.; Moore, S.A.; Cassell, M.; Perlman, S. Severe Acute Respiratory Syndrome Coronavirus Infection Causes Neuronal Death in the Absence of Encephalitis in Mice Transgenic for Human ACE2. J. Virol. 2008, 82, 7264–7275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Natoli, S.; Oliveira, V.; Calabresi, P.; Maia, L.F.; Pisani, A. Does SARS-Cov-2 invade the brain? Translational lessons from animal models. Eur. J. Neurol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Yuan, L.; Tang, Q.; Cheng, T.; Xia, N. Animal models for emerging coronavirus: Progress and new insights. Emerg. Microbes Infect. 2020, 9, 949–961. [Google Scholar] [CrossRef]
- Sellner, J. Of mice and men: COVID-19 challenges translational neuroscience. Eur. J. Neurol. 2020. [Google Scholar] [CrossRef]
- Yazdanpanah, N.; Saghazadeh, A.; Rezaei, N. Anosmia: A Missing Link in the Neuroimmunology of Coronavirus Disease 2019 (COVID-19). Rev. Neurosci. 2020, 1. Available online: 10:/j/revneuro.ahead-of-print/revneuro-2020-0039/revneuro-2020-0039.xml (accessed on 10 August 2020). [CrossRef]
- Chen, M.; Shen, W.; Rowan, N.R.; Kulaga, H.; Hillel, A.; Jr, M.R.; Lane, A.P. Elevated ACE2 expression in the olfactory neuroepithelium: Implications for anosmia and upper respiratory SARS-CoV-2 entry and replication. Eur. Respir. J. 2020, 2001948. [Google Scholar] [CrossRef]
- Jacomy, H.; Fragoso, G.; Almazan, G.; Mushynski, W.E.; Talbot, P.J. Human coronavirus OC43 infection induces chronic encephalitis leading to disabilities in BALB/C mice. Virology 2006, 349, 335–346. [Google Scholar] [CrossRef]
- Li, Y.-C.; Bai, W.-Z.; Hashikawa, T. The neuroinvasive potential of SARS-CoV2 may play a role in the respiratory failure of COVID-19 patients. J. Med. Virol. 2020, 92, 552–555. [Google Scholar] [CrossRef] [PubMed]
- Lamouroux, A.; Attie-Bitach, T.; Martinovic, J.; Leruez-Ville, M.; Yves, V. Evidence for and against vertical transmission for severe acute respiratory syndrome coronavirus 2. Am. J. Obstet. Gynecol. 2020, 223, 91.e1–91.e4. [Google Scholar] [CrossRef] [PubMed]
- Obermeier, B.; Daneman, R.; Ransohoff, R.M. Development, maintenance and disruption of the blood-brain barrier. Nat. Med. 2013, 19, 1584–1596. [Google Scholar] [CrossRef] [PubMed]
- Goasdoue, K.; Miller, S.M.; Colditz, P.B.; Björkman, S.T. Review: The blood-brain barrier; protecting the developing fetal brain. Placenta 2017, 54, 111–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bostanciklioğlu, M. SARS-CoV2 entry and spread in the lymphatic drainage system of the brain. Brain Behav. Immun. 2020, 87, 122–123. [Google Scholar] [CrossRef] [PubMed]
- Takayama, K. In Vitro and Animal Models for SARS-CoV-2 research. Trends Pharmacol. Sci. 2020, 41, 513–517. [Google Scholar] [CrossRef]
- Gandhi, S.; Srivastava, A.K.; Ray, U.; Tripathi, P.P. Is the Collapse of the Respiratory Center in the Brain Responsible for Respiratory Breakdown in COVID-19 Patients. ACS Chem. Neurosci. 2020, 11, 1379–1381. [Google Scholar] [CrossRef]
- Cave, E. COVID-19 Super-spreaders: Definitional Quandaries and Implications. Asian Bioeth. Rev. 2020, 12, 235–242. [Google Scholar] [CrossRef]
- Rubin, M.A.; Bonnie, R.J.; Epstein, L.; Hemphill, C.; Kirschen, M.; Lewis, A.; Suarez, J.I. Ethics, Law, and Humanities Committee, a joint committee of the American Academy of Neurology, American Neurological Association, and Child Neurology Society; in collaboration with the Neurocritical Care Society Ethics Committee AAN position statement. Neurology 2020, 95, 167–172. [Google Scholar] [CrossRef]
- Condie, L.O. Neurotropic mechanisms in COVID-19 and their potential influence on neuropsychological outcomes in children. Child Neuropsychol. 2020, 26, 1–20. [Google Scholar] [CrossRef]


{kind=link}
| Neuroinvasive | Virus is capable of accessing and entering the nervous system |
| Neurotropic | Virus is capable of infecting nerve cells once in the nervous system |
| Neurovirulent | Neurotropic virus is capable of causing disease in the nervous system |
| Neuroinflammatory | Virus causes secondary inflammatory response within the nervous system |
| Publication | Newborns (n) | SARS-CoV-2 Positive (n) | Comments |
|---|---|---|---|
| Chen et al. 2020 [25] | 9 | 0 | All C-sections |
| Zhang et al. 2020 [26] | 16 | 0 | All C-sections; same institution as Chen et al. 2020 [25] |
| Zeng et al. 2020 [27] | 33 | 3 | Tested 2-3 days postpartum; two full terms and one 31-wga premature infant; all developed pneumonia but recovered by ~1-2 weeks of life |
| Liu et al. 2020 [28] | 19 | 0 | PCR negative on body fluids * None developed symptoms |
| Schwartz et al. 2020 [29] | 38 | 0 | “No evidence that SARS-CoV-2 undergoes intrauterine or transplacental transmission from infected pregnant women to their fetuses.” |
| Lu & Shi 2020 [30] | - | 3 | 3 cases mentioned; diagnosed 2-17 DOL. Details sparse |
| Salvatore et al. 2020 [31] | 120 (DOL 1) 79 (DOL 5-7) 72 (DOL 14) | 0 0 0 | Cohort of infants born to SARS-CoV-2 mothers, followed through 2 weeks of life |
| Neonates (n) | Age | Presenting Symptoms | SARS-CoV-2 Testing | SARS-CoV-2 CSF | Reference |
|---|---|---|---|---|---|
| 5 | <3 y | Hypotonia, drowsiness | NP + | 4/4 - | [71] |
| 1 | 26 d | Upward eye deviation, stiffening | NP + Blood, cEEG, HUS - | NR | [72] |
| 1 | 1 d | Lethargy, encephalopathy | NP +, rectal + | - | [73] |
| 1 | 6 w | Upward eye deviation, leg stiffening | NP + | - | [74] |
| 1 | 11 y | Seizure | NP + | NR | [75] |
| 1 | 3 d | Irritability, hypertonia | Brain MRI + (transient gliosis of periventricular white matter and subcortical structures) | - | [24] |
| Severe infection caused by the novel coronavirus, SARS-Cov-2, has predominant pulmonary involvement but can also affect multiple other organ systems, including the CNS and PNS. |
| Symptoms are less frequent and usually less severe in children and particularly in neonates. |
| Vertical transmission of SARS-CoV-2 from pregnant mother to fetus is rare but anecdotal case reports support this possibility. |
| Most cases of COVID-19 in early life are due to exposures to infected patients (horizontal transmission). |
| There is no reported transmission of SARS-CoV-2 via breast milk. |
| Acute neurological involvement in adults with COVID-19 can include decrease taste/smell, headache, confusion, peripheral nerve dysfunction, strokes, and encephalopathy. |
| Neurological involvement of COVID-19 in neonates and children is still quite rare but recent case reports warrant vigilant surveillance. |
| Neurological involvement of COVID-19 in neonates and children is still quite rare but recent case reports warrant vigilant surveillance. |
| SARS-CoV-2 has not been recovered from CSF or brain samples. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stafstrom, C.E.; Jantzie, L.L. COVID-19: Neurological Considerations in Neonates and Children. Children 2020, 7, 133. https://doi.org/10.3390/children7090133
Stafstrom CE, Jantzie LL. COVID-19: Neurological Considerations in Neonates and Children. Children. 2020; 7(9):133. https://doi.org/10.3390/children7090133
Chicago/Turabian StyleStafstrom, Carl E., and Lauren L. Jantzie. 2020. "COVID-19: Neurological Considerations in Neonates and Children" Children 7, no. 9: 133. https://doi.org/10.3390/children7090133