
The Contribution of Bullying Involvement and Alexithymia to Somatic Complaints in Preadolescents

Abstract
:1. Introduction
1.1. Involvement in Bullying
1.2. The Role of Alexithymia
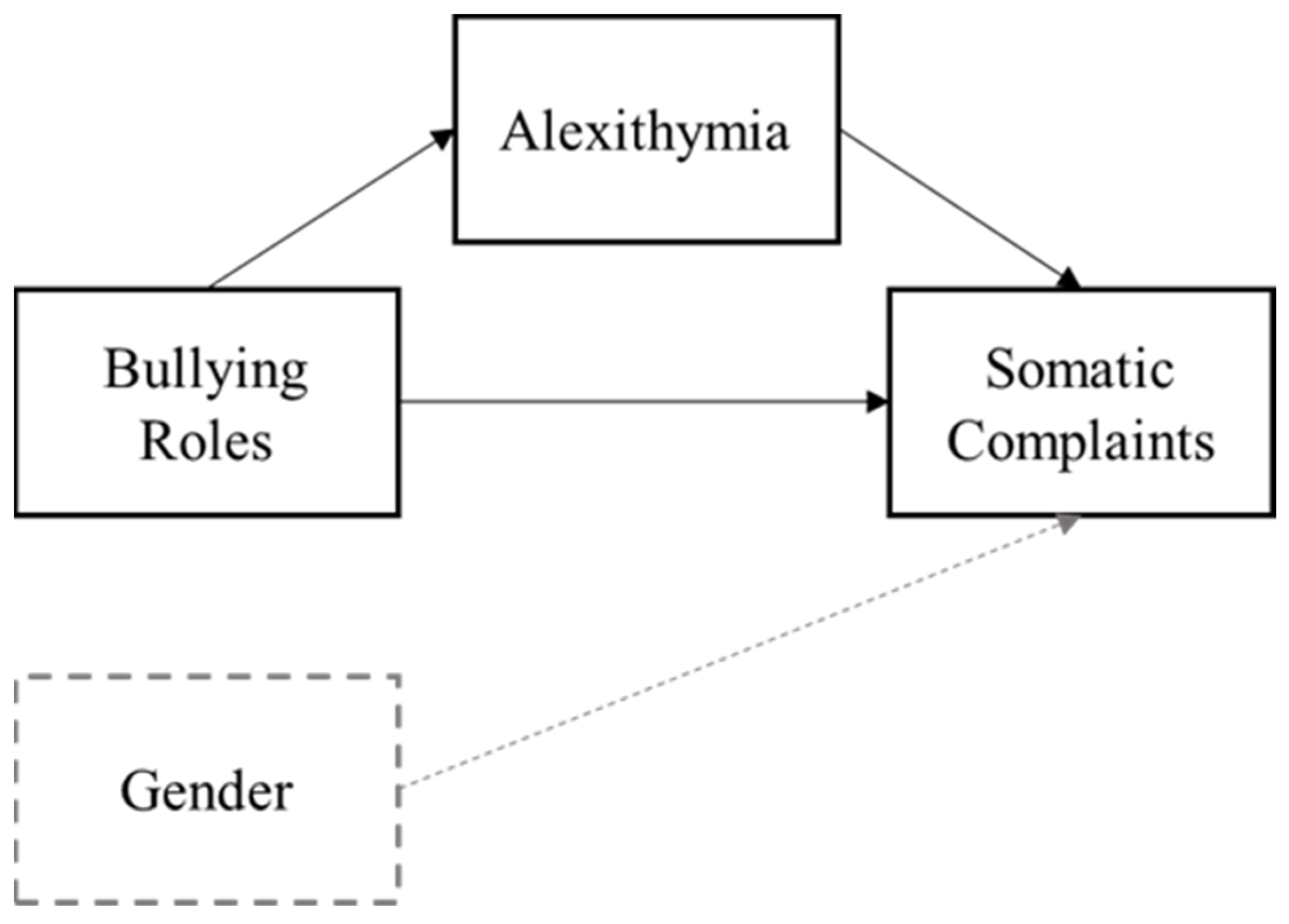
1.3. The Current Study
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.3. Statistical Analyses
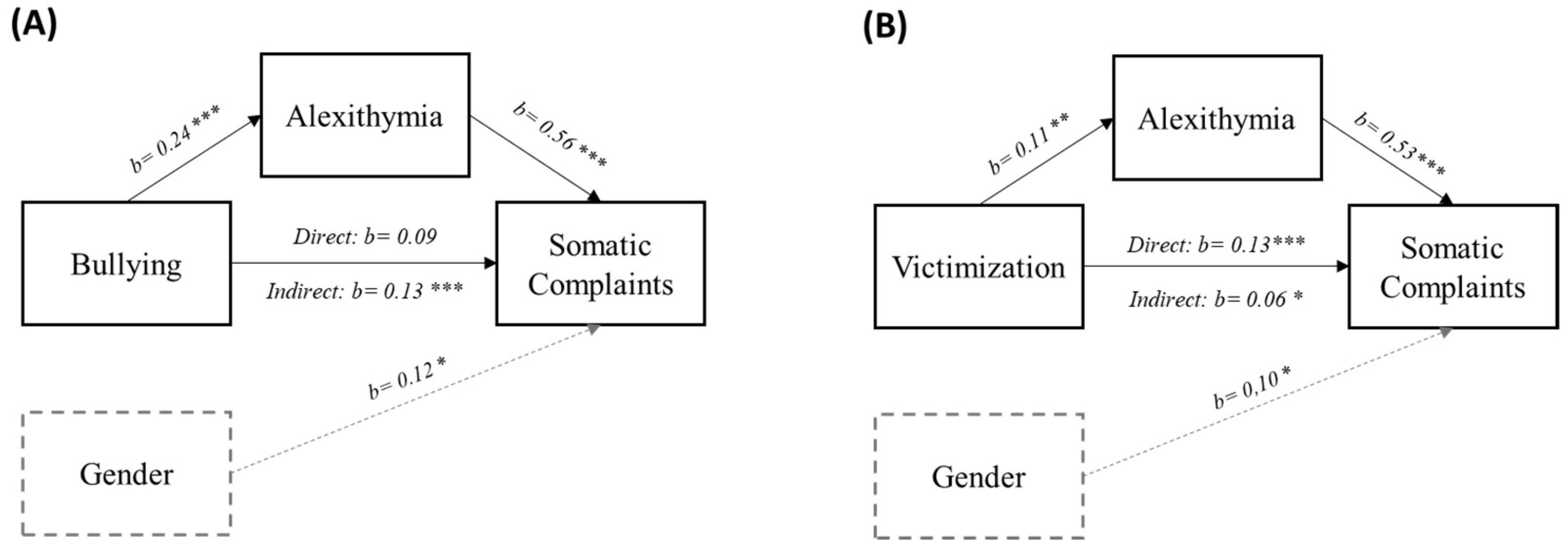
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- King, S.; Chambers, C.T.; Huguet, A.; MacNevin, R.C.; McGrath, P.J.; Parker, L.; Macdonald, A.J. The epidemiology of chronic pain in children and adolescents revisited: A systematic review. Pain 2011, 152, 2729–2738. [Google Scholar] [CrossRef] [PubMed]
- Mohapatra, S.; Deo, S.J.K.; Satapathy, A.; Rath, N. Somatoform Disorders in Children and Adolescents. Ger. J. Psychiatry 2014, 17, 19–24. [Google Scholar]
- Spear, L. The adolescent brain and age-related behavioral manifestations. Neurosci. Biobehav. Rev. 2000, 24, 417–463. [Google Scholar] [CrossRef] [PubMed]
- Wigfield, A.; Lutz, S.L.; Wagner, A.L. Early adolescents’ development across the middle school years: Implications for school counselors. Prof. Sch. Couns. 2005, 9, 2156759X0500900206. [Google Scholar] [CrossRef]
- Blum, R.W.; Astone, N.M.; Decker, M.R.; Mouli, V.C. A conceptual framework for early adolescence: A platform for research. Int. J. Adolesc. Med. Health 2014, 26, 321–331. [Google Scholar] [CrossRef]
- Jindal-Snape, D.; Miller, D.J. A Challenge of Living? Understanding the Psycho-social Processes of the Child During Primary-secondary Transition Through Resilience and Self-esteem Theories. Educ. Psychol. Rev. 2008, 20, 217–236. [Google Scholar] [CrossRef]
- Larson, R.W.; Moneta, G.; Richards, M.H.; Wilson, S. Continuity, Stability, and Change in Daily Emotional Experience across Adolescence. Child Dev. 2002, 73, 1151–1165. [Google Scholar] [CrossRef]
- Rieffe, C.; Terwogt, M.M.; Bosch, J.D.; Kneepkens, C.M.F.; Douwes, A.C.; Jellesma, F.C. Interaction between emotions and somatic complaints in children who did or did not seek medical care. Cogn. Emot. 2007, 21, 1630–1646. [Google Scholar] [CrossRef]
- Shanahan, L.; Zucker, N.; Copeland, W.E.; Bondy, C.L.; Egger, H.L.; Costello, E.J. Childhood somatic complaints predict generalized anxiety and depressive disorders during young adulthood in a community sample. Psychol. Med. 2014, 45, 1721–1730. [Google Scholar] [CrossRef]
- Wolke, D.; Lereya, S.T. Long-term effects of bullying. Arch. Dis. Child. 2015, 100, 879–885. [Google Scholar] [CrossRef]
- Olweus, D.; Limber, S.P.; Breivik, K. Addressing Specific Forms of Bullying: A Large-Scale Evaluation of the Olweus Bullying Prevention Program. Int. J. Bullying Prev. 2019, 1, 70–84. [Google Scholar] [CrossRef]
- Salmivalli, C. Bullying and the peer group: A review. Aggress. Violent Behav. 2010, 15, 112–120. [Google Scholar] [CrossRef]
- Hawkins, D.L.; Pepler, D.J.; Craig, W.M. Naturalistic Observations of Peer Interventions in Bullying. Soc. Dev. 2001, 10, 512–527. [Google Scholar] [CrossRef]
- Oh, I.; Hazler, R.J. Contributions of Personal and Situational Factors to Bystanders’ Reactions to School Bullying. Sch. Psychol. Int. 2009, 30, 291–310. [Google Scholar] [CrossRef]
- Arseneault, L.; Walsh, E.; Trzesniewski, K.; Newcombe, R.; Caspi, A.; Moffitt, T.E. Bullying Victimization Uniquely Contributes to Adjustment Problems in Young Children: A Nationally Representative Cohort Study. Pediatrics 2006, 118, 130–138. [Google Scholar] [CrossRef]
- Stein, J.A.; Dukes, R.L.; Warren, J.I. Adolescent Male Bullies, Victims, and Bully-Victims: A Comparison of Psychosocial and Behavioral Characteristics. J. Pediatr. Psychol. 2007, 32, 273–282. [Google Scholar] [CrossRef]
- Gini, G.; Pozzoli, T. Bullied Children and Psychosomatic Problems: A Meta-analysis. Pediatrics 2013, 132, 720–729. [Google Scholar] [CrossRef] [PubMed]
- Meland, E.; Rydning, J.H.; Lobben, S.; Breidablik, H.-J.; Ekeland, T.-J. Emotional, self-conceptual, and relational characteristics of bullies and the bullied. Scand. J. Public Health 2010, 38, 359–367. [Google Scholar] [CrossRef]
- Hesapcioglu, S.T.; Ercan, F. Traditional and cyberbullying co-occurrence and its relationship to psychiatric symptoms. Pediatr. Int. 2016, 59, 16–22. [Google Scholar] [CrossRef]
- Fekkes, M.; Pijpers, F.I.M.; Fredriks, A.M.; Vogels, T.; Verloove-Vanhorick, S.P. Do Bullied Children Get Ill, or Do Ill Children Get Bullied? A Prospective Cohort Study on the Relationship between Bullying and Health-Related Symptoms. Pediatrics 2006, 117, 1568–1574. [Google Scholar] [CrossRef]
- Janson, G.R.; Hazler, R.J. Trauma Reactions of Bystanders and Victims to Repetitive Abuse Experiences. Violence Vict. 2004, 19, 239–255. [Google Scholar] [CrossRef]
- Nishina, A.; Juvonen, J. Daily Reports of Witnessing and Experiencing Peer Harassment in Middle School. Child Dev. 2005, 76, 435–450. [Google Scholar] [CrossRef] [PubMed]
- Rieffe, C.; Camodeca, M. Empathy in adolescence: Relations with emotion awareness and social roles. Br. J. Dev. Psychol. 2016, 34, 340–353. [Google Scholar] [CrossRef] [PubMed]
- Rivers, I.; Poteat, V.P.; Noret, N.; Ashurst, N. Observing bullying at school: The mental health implications of witness status. Sch. Psychol. Q. 2009, 24, 211–223. [Google Scholar] [CrossRef]
- Hutchinson, M. Exploring the impact of bullying on young bystanders. Educ. Psychol. Pract. 2012, 28, 425–442. [Google Scholar] [CrossRef]
- De Gucht, V.; Heiser, W. Alexithymia and somatisation: A quantitative review of the literature. J. Psychosom. Res. 2003, 54, 425–434. [Google Scholar] [CrossRef]
- Mazzone, A.; Camodeca, M. Emotion awareness and somatic complaints in preadolescence: The mediating role of coping strategies. Infant Child Dev. 2018, 27, e2075. [Google Scholar] [CrossRef]
- Rieffe, C.; Oosterveld, P.; Terwogt, M.M. An alexithymia questionnaire for children: Factorial and concurrent validation results. Pers. Individ. Differ. 2006, 40, 123–133. [Google Scholar] [CrossRef]
- Hadji-Michael, M.; McAllister, E.; Reilly, C.; Heyman, I.; Bennett, S. Alexithymia in children with medically unexplained symptoms: A systematic review. J. Psychosom. Res. 2019, 123, 109736. [Google Scholar] [CrossRef]
- Jellesma, F.C.; Rieffe, C.; Terwogt, M.M.; Westenberg, M. Do I feel sadness, fear or both? Comparing self-reported alexithymia and emotional task-performance in children with many or few somatic complaints. Psychol. Health 2009, 24, 881–893. [Google Scholar] [CrossRef]
- Subic-Wrana, C. Emotion Regulation and Mentalization in Somatoform Disorders. In Emotion Regulation and Well-Being; Springer: New York, NY, USA, 2010; pp. 245–260. [Google Scholar]
- Pandey, R.; Saxena, P.; Dubey, A. Emotion regulation difficulties in alexithymia and mental health. Eur. J. Psychol. 2011, 7, 604–623. [Google Scholar] [CrossRef]
- Allen, L.B.; Lu, Q.; Tsao, J.C.I.; Hayes, L.P.; Zeltzer, L.K. Depression partially mediates the relationship between alexithymia and somatization in a sample of healthy children. J. Health Psychol. 2011, 16, 1177–1186. [Google Scholar] [CrossRef] [PubMed]
- Lumley, M.A.; Mader, C.B.; Gramzow, J.B.; Papineau, K.B. Family Factors Related to Alexithymia Characteristics. Psychosom. Med. 1996, 58, 211–216. [Google Scholar] [CrossRef]
- Nylund, K.; Bellmore, A.; Nishina, A.; Graham, S. Subtypes, Severity, and Structural Stability of Peer Victimization: What Does Latent Class Analysis Say? Child Dev. 2007, 78, 1706–1722. [Google Scholar] [CrossRef] [PubMed]
- Pabian, S.; Vandebosch, H. An Investigation of Short-Term Longitudinal Associations between Social Anxiety and Victimization and Perpetration of Traditional Bullying and Cyberbullying. J. Youth Adolesc. 2016, 45, 328–339. [Google Scholar] [CrossRef]
- Taylor, G.J.; Parker, J.D.A.; Bagby, R.M.; Acklin, M.W.; Burns, J.A. Alexithymia and somatic complaints in psychiatric out-patients. J. Psychosom. Res. 1992, 36, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Hébert, M.; Boisjoli, C.; Blais, M.; Oussaïd, E. Alexithymia as a mediator of the relationship between child sexual abuse and psychological distress in adolescence: A short-term longitudinal study. Psychiatry Res. 2018, 260, 468–472. [Google Scholar] [CrossRef]
- Schimmenti, A.; Passanisi, A.; Caretti, V.; La Marca, L.; Granieri, A.; Iacolino, C.; Gervasi, A.M.; Maganuco, N.R.; Billieux, J. Traumatic experiences, alexithymia, and Internet addiction symptoms among late adolescents: A moderated mediation analysis. Addict. Behav. 2017, 64, 314–320. [Google Scholar] [CrossRef]
- Tomaszek, A.; Wróblewska, A.; Zdankiewicz-Ścigała, E.; Rzońca, P.; Gałązkowski, R.; Gozdowska, J.; Lewandowska, D.; Kosson, D.; Kosieradzki, M.; Danielewicz, R. Post-Traumatic Growth among Patients after Living and Cadaveric Donor Kidney Transplantation: The Role of Resilience and Alexithymia. Int. J. Environ. Res. Public Health 2021, 18, 2164. [Google Scholar] [CrossRef]
- Wise, T.N.; Mann, L.S.; Mitchell, J.D.; Hryvniak, M.; Hill, B. Secondary alexithymia: An empirical validation. Compr. Psychiatry 1990, 31, 284–288. [Google Scholar] [CrossRef]
- Guzzo, G.; Pace, U.; Cascio, V.L.; Craparo, G.; Schimmenti, A. Bullying Victimization, Post-Traumatic Symptoms, and the Mediating Role of Alexithymia. Child Indic. Res. 2014, 7, 141–153. [Google Scholar] [CrossRef]
- Garisch, J.A.; Wilson, M.S. Vulnerabilities to deliberate self-harm among adolescents: The role of alexithymia and victimization. Br. J. Clin. Psychol. 2010, 49, 151–162. [Google Scholar] [CrossRef]
- Prino, L.E.; Longobardi, C.; Fabris, M.A.; Parada, R.H.; Settanni, M. Effects of Bullying Victimization on Internalizing and Externalizing Symptoms: The Mediating Role of Alexithymia. J. Child Fam. Stud. 2019, 28, 2586–2593. [Google Scholar] [CrossRef]
- Wachs, S.; Wright, M.F. Bullying and alexithymia: Are there differences between traditional, cyber, combined bullies, and nonbullies in reading their own emotions? Crim. Behav. Ment. Health 2018, 28, 409–413. [Google Scholar] [CrossRef]
- Aricak, O.T.; Ozbay, A. Investigation of the relationship between cyberbullying, cybervictimization, alexithymia and anger expression styles among adolescents. Comput. Hum. Behav. 2016, 55, 278–285. [Google Scholar] [CrossRef]
- Shabahang, R.; Sedighian, S.F.; Nezhad, A.R.; Shal, R.S. Role of Difficulties in Emotional Regulation and Alexithymia in Prediction of Bullying. Q. J. Child Ment. Health 2019, 6, 40–50. [Google Scholar] [CrossRef]
- Jellesma, F.C.; Rieffe, C.; Terwogt, M.M. My peers, my friend, and I: Peer interactions and somatic complaints in boys and girls. Soc. Sci. Med. 2008, 66, 2195–2205. [Google Scholar] [CrossRef]
- Greene, J.W.; Walker, L.S.; Hickson, G.; Thompson, J. Stressful Life Events and Somatic Complaints in Adolescents. Pediatrics 1985, 75, 19–22. [Google Scholar] [CrossRef]
- Chapman, M.V. Neighborhood quality and somatic complaints among American youth. J. Adolesc. Health 2005, 36, 244–252. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. Contexts of child rearing: Problems and prospects. Am. Psychol. 1979, 34, 844. [Google Scholar] [CrossRef]
- Smith, P.K.; López-Castro, L.; Robinson, S.; Görzig, A. Consistency of gender differences in bullying in cross-cultural surveys. Aggress. Violent Behav. 2019, 45, 33–40. [Google Scholar] [CrossRef]
- Ogrodniczuk, J.S.; Kealy, D.; Joyce, A.S.; Abbass, A.A. Body talk: Sex differences in the influence of alexithymia on physical complaints among psychiatric outpatients. Psychiatry Res. 2018, 261, 168–172. [Google Scholar] [CrossRef]
- Romero-Acosta, K.; Zolog, T.C. Age and gender differences of somatic symptoms in children and adolescents. J. Ment. Health 2013, 22, 33–41. [Google Scholar] [CrossRef]
- Jellesma, F.C.; Rieffe, C.; Terwogt, M.M. The Somatic Complaint List: Validation of a self-report questionnaire assessing somatic complaints in children. J. Psychosom. Res. 2007, 63, 399–401. [Google Scholar] [CrossRef]
- Sijtsma, K. Reliability Beyond Theory and into Practice. Psychometrika 2009, 74, 169–173. [Google Scholar] [CrossRef]
- Pozzoli, T.; Gini, G.; Vieno, A. The Role of Individual Correlates and Class Norms in Defending and Passive Bystanding Behavior in Bullying: A Multilevel Analysis. Child Dev. 2012, 83, 1917–1931. [Google Scholar] [CrossRef]
- Clark, L.A.; Watson, D. Constructing validity: Basic issues in objective scale development. Psychol. Assess. 1995, 7, 309–319. [Google Scholar] [CrossRef]
- Di Trani, M.; Tomassetti, N.; Bonadies, M.; Capozzi, F.; De Gennaro, L.; Presaghi, F.; Solano, L. Un Questionario italiano per l’alessitimia in età evolutiva: Struttura fattoriale e attendibilità. Psicol. Salut. 2009, 2, 131–143. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2017; ISBN 1462534651. [Google Scholar]
- Gini, G.; Pozzoli, T. Association between Bullying and Psychosomatic Problems: A Meta-analysis. Pediatrics 2009, 123, 1059–1065. [Google Scholar] [CrossRef]
- Vanderbilt, D.; Augustyn, M. The effects of bullying. Paediatr. Child Health 2010, 20, 315–320. [Google Scholar] [CrossRef]
- Helmes, E.; McNeill, P.D.; Holden, R.R.; Jackson, C. The construct of alexithymia: Associations with defense mechanisms. J. Clin. Psychol. 2008, 64, 318–331. [Google Scholar] [CrossRef]
- Chung, M.C.; Di, X.; Wan, K.H. Exploring the interrelationship between alexithymia, defense style, emotional suppression, homicide-related posttraumatic stress disorder and psychiatric co-morbidity. Psychiatry Res. 2016, 243, 373–381. [Google Scholar] [CrossRef]
- Loch, A.P.; Astolfi, R.C.; Leite, M.A.; Papa, C.H.G.; Ryngelblum, M.; Eisner, M.; Peres, M.F.T. Victims, bullies and bully–victims: Prevalence and association with negative health outcomes from a cross-sectional study in São Paulo, Brazil. Int. J. Public Health 2020, 65, 1485–1495. [Google Scholar] [CrossRef]
- Berking, M.; Schwarz, J. Affect regulation training. In Handbook of Emotion Regulation; Springer: New York, NY, USA, 2014; Volume 2, pp. 529–547. [Google Scholar]
- Van Beveren, M.-L.; Goossens, L.; Volkaert, B.; Grassmann, C.; Wante, L.; Vandeweghe, L.; Verbeken, S.; Braet, C. How do I feel right now? Emotional awareness, emotion regulation, and depressive symptoms in youth. Eur. Child Adolesc. Psychiatry 2019, 28, 389–398. [Google Scholar] [CrossRef]
- Weissman, D.G.; Nook, E.C.; Dews, A.A.; Miller, A.B.; Lambert, H.K.; Sasse, S.F.; Somerville, L.H.; McLaughlin, K.A. Low Emotional Awareness as a Transdiagnostic Mechanism Underlying Psychopathology in Adolescence. Clin. Psychol. Sci. 2020, 8, 971–988. [Google Scholar] [CrossRef]
- McLaughlin, K.A.; Sheridan, M.A.; Alves, S.; Mendes, W.B. Child Maltreatment and Autonomic Nervous System Reactivity: Identifying Dysregulated Stress Reactivity Patterns using the Biopsychosocial Model of Challenge and Threat. Psychosom. Med. 2014, 76, 538–546. [Google Scholar] [CrossRef]
- Sendzik, L.; Schäfer, J.Ö.; Samson, A.C.; Naumann, E.; Tuschen-Caffier, B. Emotional Awareness in Depressive and Anxiety Symptoms in Youth: A Meta-Analytic Review. J. Youth Adolesc. 2017, 46, 687–700. [Google Scholar] [CrossRef]
- Twemlow, S.W.; Fonagy, P.; Sacco, F.C. The Role of the Bystander in the Social Architecture of Bullying and Violence in Schools and Communities. Ann. N. Y. Acad. Sci. 2006, 1036, 215–232. [Google Scholar] [CrossRef]
- Yun, H. New Approaches to Defender and Outsider Roles in School Bullying. Child Dev. 2020, 91, e814–e832. [Google Scholar] [CrossRef]
- Schulte, I.E.; Petermann, F. Familial Risk Factors for the Development of Somatoform Symptoms and Disorders in Children and Adolescents: A Systematic Review. Child Psychiatry Hum. Dev. 2011, 42, 569–583. [Google Scholar] [CrossRef]
- Gaffney, H.; Ttofi, M.M.; Farrington, D.P. Evaluating the effectiveness of school-bullying prevention programs: An updated meta-analytical review. Aggress. Violent Behav. 2019, 45, 111–133. [Google Scholar] [CrossRef]
- Palladino, B.E.; Nocentini, A.; Menesini, E. Evidence-based intervention against bullying and cyberbullying: Evaluation of the NoTrap! program in two independent trials. Aggress. Behav. 2016, 42, 194–206. [Google Scholar] [CrossRef] [PubMed]
- Salmivalli, C.; Kärnä, A.; Poskiparta, E. Counteracting bullying in Finland: The KiVa program and its effects on different forms of being bullied. Int. J. Behav. Dev. 2011, 35, 405–411. [Google Scholar] [CrossRef]
- Twemlow, S.W.; Fonagy, P.; Sacco, F.C.; Vernberg, E.; Malcom, J.M. Reducing violence and prejudice in a Jamaican all age school using attachment and mentalization theory. Psychoanal. Psychol. 2011, 28, 497–511. [Google Scholar] [CrossRef]
- Muratori, P.; Bertacchi, I.; Catone, G.; Mannucci, F.; Nocentini, A.; Pisano, S.; Lochman, J.E. Coping Power Universal for middle school students: The first efficacy study. J. Adolesc. 2020, 79, 49–58. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | ||
|---|---|---|---|---|---|---|---|
| 1. | Gender | ||||||
| 2. | Somatic complaints | 0.27 ** | |||||
| 3. | Alexithymia | 0.19 ** | 0.54 ** | ||||
| 4. | Bullying | −0.14 | 0.17 * | 0.24 ** | |||
| 5. | Victimization | 0.07 | 0.33 ** | 0.23 ** | 0.10 | ||
| 6. | Outsider behavior | 0.00 | 0.09 | 0.11 | 0.08 | −0.04 | |
| Mean | - | 0.59 | 0.81 | 1.35 | 1.70 | 1.84 | |
| SD | - | 0.35 | 0.30 | 0.34 | 0.59 | 0.59 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levantini, V.; Camodeca, M.; Iannello, N.M. The Contribution of Bullying Involvement and Alexithymia to Somatic Complaints in Preadolescents. Children 2023, 10, 905. https://doi.org/10.3390/children10050905
Levantini V, Camodeca M, Iannello NM. The Contribution of Bullying Involvement and Alexithymia to Somatic Complaints in Preadolescents. Children. 2023; 10(5):905. https://doi.org/10.3390/children10050905
Chicago/Turabian StyleLevantini, Valentina, Marina Camodeca, and Nicolò Maria Iannello. 2023. "The Contribution of Bullying Involvement and Alexithymia to Somatic Complaints in Preadolescents" Children 10, no. 5: 905. https://doi.org/10.3390/children10050905