
Narrative Identity within Mentalization-Based Group Therapy for Adolescents: A Feasibility Study

Abstract
:1. Introduction
The Present Study
2. Method
Participants and Procedure
3. Measures
3.1. Narrative Analysis and Coding of Video Recorded Therapy Sessions
Symptomatology and Global Functioning at Baseline and End of Treatment
4. Results
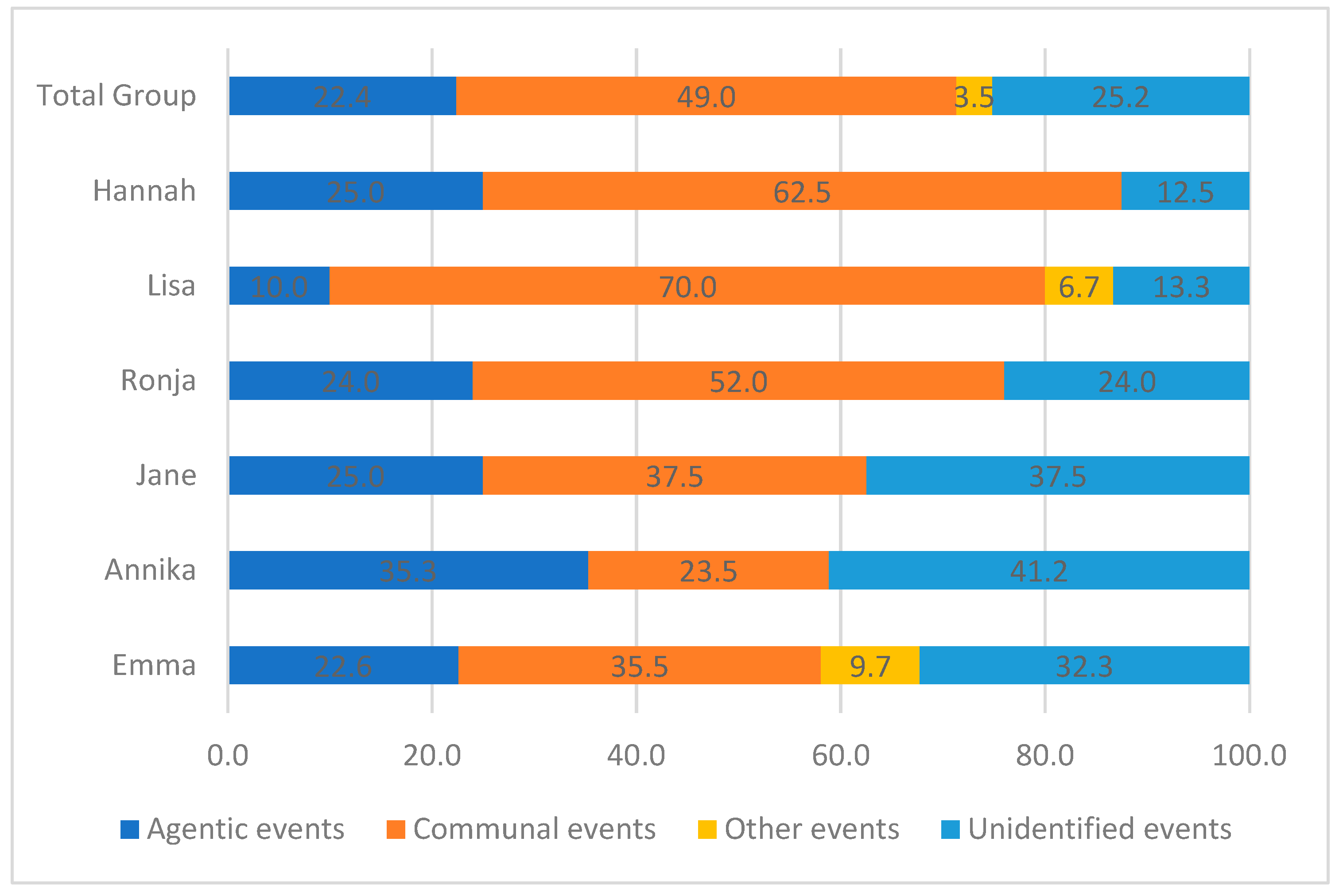
4.1. Nature of Narrated Events: Agency and Communion
4.2. Change of Narrated Events: Agency and Communion
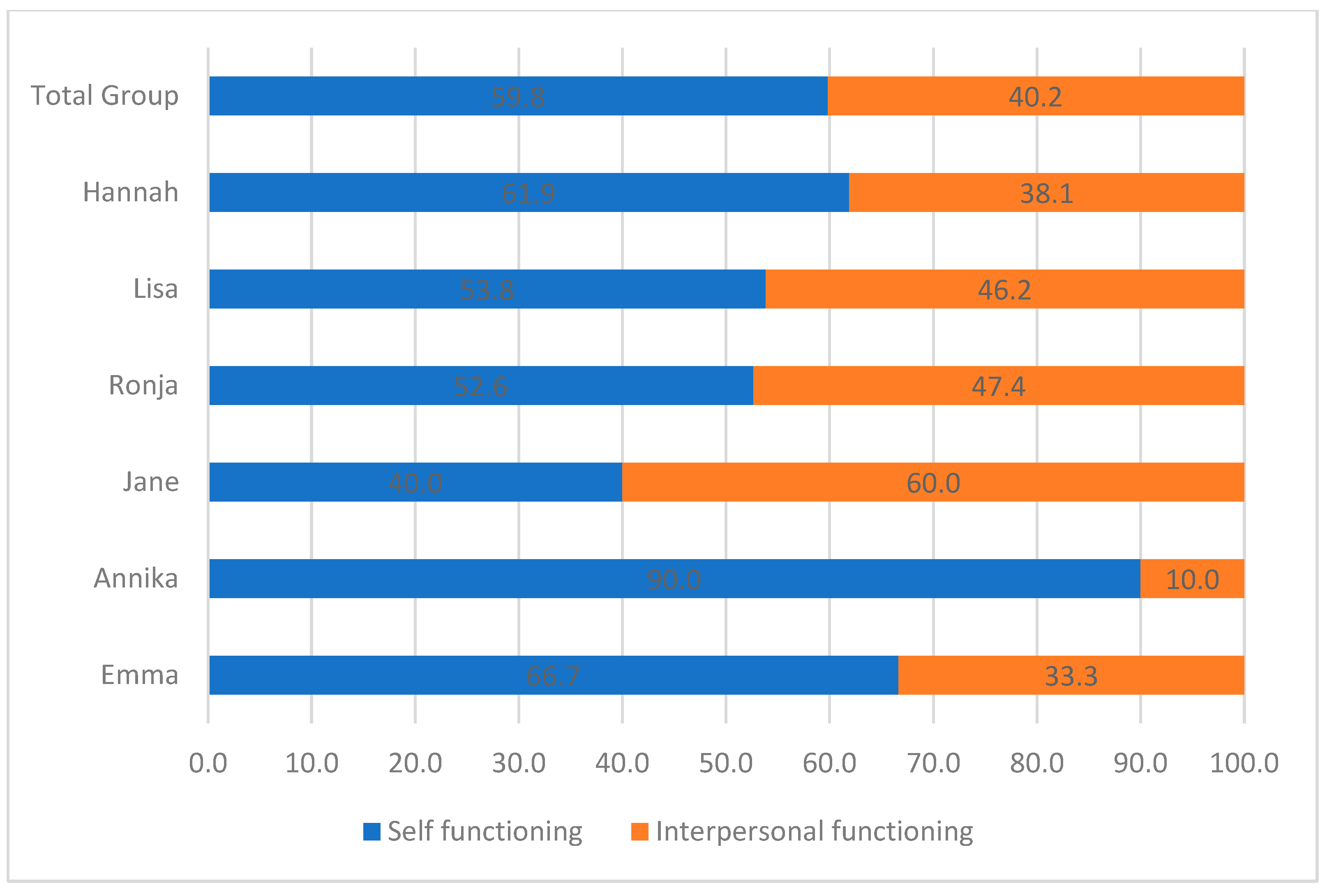
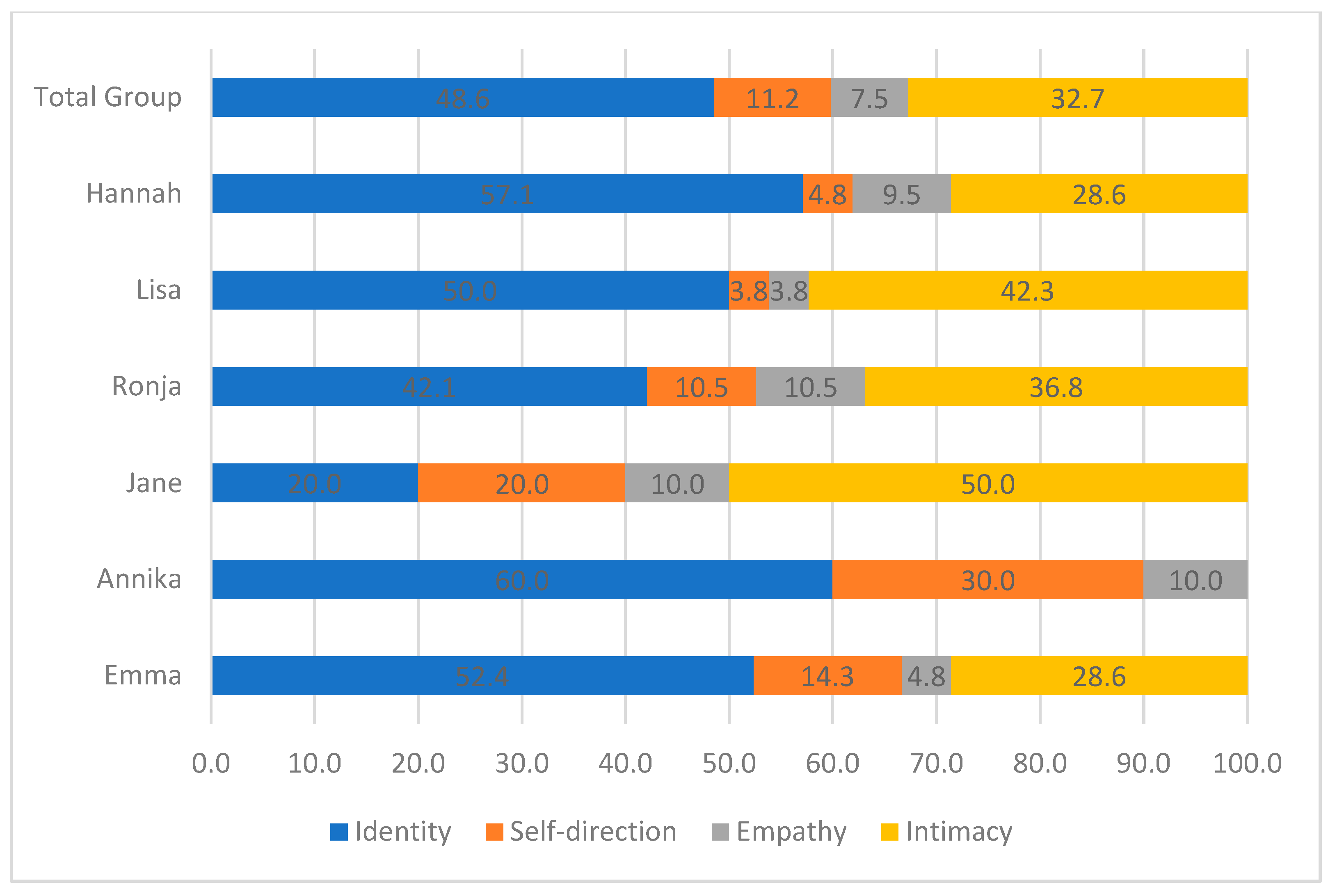
4.3. Nature of Narrated Reactions: Personality Functioning
4.4. Change in Narrated Reactions: Personality Functioning
4.5. Symptomatology and Global Functioning
5. Discussion
5.1. A Shift from Other-Functioning (Communion) towards a Focus on Self-Functioning in Both Nature and Reaction of the Narration
5.2. Study Limitations
5.3. Concluding Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- APA. Diagnostic and Statistical Manual of Mental Disorders: DSM-5-TR, 5th ed.; American Psychiatric Association Publishing: Washington, DC, USA, 2022. [Google Scholar]
- Wall, K.; Leavitt, J.; Sharp, C. Personality Disorders in Adolescence. In The Encyclopedia of Child and Adolescent Development; Hupp, S., Jewell, J., Eds.; John Wiley and Sons: Hoboken, NJ, USA, 2023. [Google Scholar]
- Chanen, A.M. Borderline Personality Disorder in Young People: Are We There Yet? J. Clin. Psychol. 2015, 71, 778–791. [Google Scholar] [CrossRef]
- Kongerslev, M.T.; Chanen, A.M.; Simonsen, E. Personality Disorder in Childhood and Adolescence comes of Age: A Review of the Current Evidence and Prospects for Future Research. Scand. J. Child Adolesc. Psychiatry Psychol. 2014, 3, 31–48. [Google Scholar] [CrossRef]
- Vogt, K.S.; Norman, P. Is mentalization-based therapy effective in treating the symptoms of borderline personality disorder? A systematic review. Psychol. Psychother. 2019, 92, 441–464. [Google Scholar] [CrossRef]
- Wong, J.; Bahji, A.; Khalid-Khan, S. Psychotherapies for Adolescents with Subclinical and Borderline Personality Disorder: A Systematic Review and Meta-Analysis. Can. J. Psychiatry 2020, 65, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Bo, S.; Vilmar, J.W.; Jensen, S.L.; Jørgensen, M.S.; Kongerslev, M.; Lind, M.; Fonagy, P. What works for adolescents with borderline personality disorder: Towards a developmentally informed understanding and structured treatment model. Curr. Opin. Psychol. 2021, 37, 7–12. [Google Scholar] [CrossRef]
- Jørgensen, M.S.; Storebø, O.J.; Simonsen, E. Systematic Review and Meta-Analyses of Psychotherapies for Adolescents with Subclinical and Borderline Personality Disorder: Methodological Issues. Can. J. Psychiatry 2020, 65, 59–60. [Google Scholar] [CrossRef] [PubMed]
- Beck, E.; Bo, S.; Gondan, M.; Poulsen, S.; Pedersen, L.; Pedersen, J.; Simonsen, E. Mentalization-based treatment in groups for adolescents with borderline personality disorder (BPD) or subthreshold BPD versus treatment as usual (M-GAB): Study protocol for a randomized controlled trial. Trials 2016, 17, 314. [Google Scholar] [CrossRef] [PubMed]
- Beck, E.; Bo, S.; Jørgensen, M.S.; Gondan, M.; Poulsen, S.; Storebø, O.J.; Fjellerad Andersen, C.; Folmo, E.; Sharp, C.; Pedersen, J.; et al. Mentalization-based treatment in groups for adolescents with borderline personality disorder: A randomized controlled trial. J. Child Psychol. Psychiatry 2020, 61, 594–604. [Google Scholar] [CrossRef]
- Jørgensen, M.S.; Storebø, O.J.; Bo, S.; Poulsen, S.; Gondan, M.; Beck, E.; Chanen, A.M.; Bateman, A.; Pedersen, J.; Simonsen, E. Mentalization-based treatment in groups for adolescents with Borderline Personality Disorder: 3- and 12-month follow-up of a randomized controlled trial. Eur. Child Adolesc. Psychiatry 2021, 30, 699–710. [Google Scholar] [CrossRef]
- Bach, B.; First, M.B. Application of the ICD-11 classification of personality disorders. BMC Psychiatry 2018, 18, 351. [Google Scholar] [CrossRef]
- Sharp, C.; Wall, K. DSM-5 Level of Personality Functioning: Refocusing Personality Disorder on What It Means to Be Human. Annu. Rev. Clin. Psychol. 2021, 17, 313–337. [Google Scholar] [CrossRef] [PubMed]
- McAdams, D.P. Narrative Identity: What Is It? What Does It Do? How Do You Measure It? Imagin. Cogn. Personal. 2018, 37, 359–372. [Google Scholar] [CrossRef]
- Lind, M.; Sharp, C.; Dunlop, W.L. Why, how, and when to integrat narrative identity within dimensional approaches to personality disorders. J. Personal. Disord. 2022, 36, 377–398. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Classification of Diseases, 11th Revision; World Health Organization (WHO): Geneva, Switzerland, 2022. [Google Scholar]
- Adler, J.M.; Clark, L.A. Incorporating narrative identity into structural approaches to personality and psychopathology. J. Res. Personal. 2019, 82, 103857. [Google Scholar] [CrossRef]
- Lind, M.; Adler, J.M.; Clark, L.A. Narrative Identity and Personality Disorder: An Empirical and Conceptual Review. Curr. Psychiatry Rep. 2020, 22, 67. [Google Scholar] [CrossRef]
- Shiner, R.L.; Klimstra, T.A.; Denissen, J.J.A.; See, A.Y. The development of narrative identity and the emergence of personality disorders in adolescence. Curr. Opin. Psychol. 2021, 37, 49–53. [Google Scholar] [CrossRef]
- Habermas, T.; Bluck, S. Getting a Life: The Emergence of the Life Story in Adolescence. Psychol. Bull. 2000, 126, 748–769. [Google Scholar] [CrossRef]
- Lind, M.; Vanwoerden, S.; Penner, F.; Sharp, C. Inpatient Adolescents with Borderline Personality Disorder Features: Identity Diffusion and Narrative Incoherence. Personal. Disord. 2019, 10, 389–393. [Google Scholar] [CrossRef]
- Lind, M.; Vanwoerden, S.; Bo, S.; Sharp, C. Borderline Personality Disorder in Adolescence: The Role of Narrative Identity in the Intrapsychic Reasoning System. Personal. Disord. 2022, 13, 451–459. [Google Scholar] [CrossRef]
- Bender, D.S.; Morey, L.C.; Skodol, A.E. Toward a Model for Assessing Level of Personality Functioning in DSM-5, Part I: A Review of Theory and Methods. J. Personal. Assess. 2011, 93, 332–346. [Google Scholar] [CrossRef]
- Dimitrova, J.; Simms, L.J. Construct Validation of Narrative Coherence: Exploring Links With Personality Functioning and Psychopathology. Personal. Disord. 2022, 13, 482–493. [Google Scholar] [CrossRef] [PubMed]
- Cruitt, P.J.; Boudreaux, M.J.; King, H.R.; Oltmanns, J.R.; Oltmanns, T.F. Examining Criterion A: DSM-5 Level of Personality Functioning as Assessed Through Life Story Interviews. Personal. Disord. 2019, 10, 224–234. [Google Scholar] [CrossRef]
- Roche, M.J.; Jacobson, N.C.; Phillips, J.J. Expanding the Validity of the Level of Personality Functioning Scale Observer Report and Self-Report Versions Across Psychodynamic and Interpersonal Paradigms. J. Personal. Assess. 2018, 100, 571–580. [Google Scholar] [CrossRef] [PubMed]
- Lind, M. Fulfilling or failing to fulfill narrative developmental themes: An indicator of living into the good life in late adolescence. J. Res. Personal. 2022, 100, 104283. [Google Scholar] [CrossRef]
- Bach, B.; Simonsen, S. How does level of personality functioning inform clinical management and treatment? Implications for ICD-11 classification of personality disorder severity. Curr. Opin. Psychiatry 2021, 34, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Lind, M.; Jørgensen, C.R.; Heinskou, T.; Simonsen, S.; Bøye, R.; Thomsen, D.K. Patients with Borderline Personality Disorder Show Increased Agency in Life Stories After 12 Months of Psychotherapy. Psychotherapy 2019, 56, 274–284. [Google Scholar] [CrossRef]
- Zanarini, M.C. The Childhood Interview for DSM-IV Borderline Personality Disorder (CI-BPD); McLean Hospital and Harvard Medical School: Belmont, MA, USA, 2003. [Google Scholar]
- McAdams, D. Coding Autobiographical Episodes for Themes of Agency and Communion—Revised; Northwestern University: Evanston, IL, USA, 2002. [Google Scholar]
- Crick, N.R.; Murray–Close, D.; Woods, K. Borderline personality features in childhood: A short-term longitudinal study. Dev. Psychopathol. 2005, 17, 1051–1070. [Google Scholar] [CrossRef]
- Chang, B.; Sharp, C.; Ha, C. The criterion validity of the Borderline Personality Features Scale for Children in an adolescent inpatient setting. J. Personal. Disord. 2011, 25, 492–503. [Google Scholar] [CrossRef]
- Aschenbach, T.M. Manual for the Child Behavior Checklist 4-18 and 1991 Profile; University of Vermont Department of Psychiatry: Burlington, VT, USA, 1991. [Google Scholar]
- Aschenbach, T.M. Manual for the Youth Self-Report and 1991 Profile; University of Vermont Department of Psychiatry: Burlington, VT, USA, 1991. [Google Scholar]
- Aschenbach, T.M. Integrative Guide for the 1991 CBCL; University of Vermont Department of Psychiatry: Burlington, VT, USA, 1991. [Google Scholar]
- Beck, J.S.; Beck, A.T.; Jolly, J.B.; Steer, R.A. Beck Youth Inventories of Emotional and Social Impairment, 2nd ed.; Dansk Psykologisk Forlag: Copenhagen, Denmark, 2012. [Google Scholar]
- Thastum, M.; Ravn, K.; Sommer, S.; Trillingsgaard, A. Reliability, validity and normative data for the Danish Beck Youth Inventories. Scand. J. Psychol. 2009, 50, 47–54. [Google Scholar] [CrossRef]
- Shaffer, D.; Gould, M.S.; Brasic, J.; Ambrosini, P.; Fisher, P.; Bird, H.; Aluwahlia, S. A Children’s Global Assessment Scale (CGAS). Arch. Gen. Psychiatry 1983, 40, 1228–1231. [Google Scholar] [CrossRef]
- Lind, M. Situating personality disorder within its maladaptive narrative identity ecology. Front. Psychiatry 2023, 14, 1117525. [Google Scholar] [CrossRef] [PubMed]
- Pol, S.M.; Schug, F.; Chakhssi, F.; Westerhof, G.J. Life stories of patients with personality disorders before and after treatment: Change and stability in agency and communion. Front. Psychiatry 2023, 14, 1134796. [Google Scholar] [CrossRef] [PubMed]
- Sharp, C. Adolescent Personality Pathology and the Alternative Model for Personality Disorders: Self Development as Nexus. Psychopathology 2020, 53, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Erikson, E.H. Identity and the Life Cycle; Norton: New York, NY, USA, 1994. [Google Scholar]
- Jørgensen, C.R.; Bøye, R. How Does it Feel to have a Disturbed Identity? The Phenomenology of Identity Diffusion on Patients with Borderline Personality Disorder: A Qualitative Study. J. Personal. Disord. 2022, 36, 40–69. [Google Scholar] [CrossRef]
- McAdams, D.P. The Life Story Interview; Northwestern University: Evanston, IL, USA, 2008. [Google Scholar]
- Bender, D.S.; Skodol, A.E.; First, M.B.; Oldham, J.M. Module I: Structured Clinical Interview for the Level of Personality Functioning Scale. In Structured Clinical Interview for the DSM-5 Alternative Model for Personality Disorders (SCID-5-AMPD); First, M.B., Skodol, A.E., Bender, D.S., Oldham, J.M., Eds.; American Psychiatric Association: Washington, DC, USA, 2018. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Narrated Events | n | Examples | |
|---|---|---|---|
| Agency themes | |||
| Generalized plots | 15 | “She felt that everyday life was boring” “She was in her room, and suddenly felt stressed out” | |
| School | 10 | “She had a panic attack at school, and does not want to go there anymore” “She had to meet with the headmaster due to truancy” | |
| Transitions | 7 | “She has been suggested to move to her cousins place in another city to start over” “She got told to move out of home” | |
| Communion themes | |||
| Romantic relationships | 33 | “She had a fight with her boyfriend, because he texted with another girl” “She had started dating a new guy, but felt that he was moving too fast” | |
| Parents/family | 24 | “She visited her father” “She ended up discussing with her sister, because of guy” | |
| Friendships | 13 | “She tried to help a friend with relationship issues” “She went on a trip with a group of friends, but they ended up having a row” | |
| Other themes | 5 | “She talked to her doctor about stopping medication” “She had her brace removed” | |
| Narrated Reactions | n | Examples | |
| Identity | |||
| Coherence | 13 | “She suddenly felt empty” | |
| Self-esteem | 10 | “His message made her feel weak” | |
| Emotion Regulation | 26 | “She ended up self-harming” | |
| Self-direction | |||
| Goal-striving | 12 | “She could not decide whether she wanted to marry him” | |
| Internal standards of behavior | 0 | none | |
| Self-reflection | 5 | “She got confused about her feelings and did not know how to react” | |
| Empathy | |||
| Comprehension of others’ experiences | 4 | “Her boyfriend did not answer her, because he was at school, which made her angry and anxious” | |
| Tolerance of others’ perspectives | 2 | “She felt she had wasted her time on him because he did not change opinion” | |
| Effect of one’s behavior on others | 3 | “She did not want to make her mom sad, so she stopped herself from self-harming” | |
| Intimacy | |||
| Depth and duration | 11 | “She withdrew from him” | |
| Desire and capacity for closeness | 14 | “She turned to him to get calmed down” | |
| Reciprocity | 7 | “She scolded him, because she felt he was unrespectful” | |
| Events | n (%) | First 5 n (%) | Last 5 n (%) | χ2(3) | p |
|---|---|---|---|---|---|
| Total | 143 (100) | 30 (100) | 30 (100) | 8.8 | 0.03 |
| Agency | 32 (22.4) | 5 (16.7) | 11 (36.7) | ||
| Communion | 70 (49.0) | 20 (66.7) | 10 (33.3) | ||
| Other | 5 (3.5) | 0 (0.0) | 4 (13.3) | ||
| Unidentified | 36 (25.2) | 5 (16.7) | 5 (16.7) | ||
| Reactions | |||||
| Total | 107 (100) | 30 (100) | 30 (100) | 5.7 | 0.13 |
| Identity | 52 (48.6) | 15 (50) | 13 (43.3) | ||
| Self-Direction | 12 (11.2) | 1 (3.3) | 7 (23.3) | ||
| Empathy | 8 (7.5) | 3 (10.0) | 1 (3.3) | ||
| Intimacy | 35 (32.7) | 11 (36.7) | 9 (30.0) |
| Clinical Measures (n = 6) | Baseline M (SD) | EOT M (SD) | t(5) | p | Difference * (95% CI) | Hedges’ g |
|---|---|---|---|---|---|---|
| BPFS-C | 86.2 (11.6) | 76.8 (13.2) | 1.69 | 0.15 | 9.3 (−4.9; 23.2) | 0.58 |
| BPFS-P | 82.9 (14.2) | 63.2 (15.4) | 2.56 | 0.06 | 19.7 (−1.7; 41.1) | 0.91 |
| CBCL-P | ||||||
| Externalizing | 24.3 (12.7) | 4.6 (9.2) | 2.51 | 0.066 | 19.8 (−2.1; 41.7) | 0.90 |
| Internalizing | 24.8 (10.8) | 2.7 (6.0) | 3.59 | 0.023 | 22.1 (5.0; 39.3) | 1.3 |
| YSR | ||||||
| Externalizing | 26.7 (7.6) | 7.0 (4.3) | 4.98 | 0.008 | 19.7 (8.7; 30.7) | 1.8 |
| Internalizing | 34.6 (5.5) | 12.8 (9.8) | 4.26 | 0.013 | 21.8 (7.6; 36.0) | 1.5 |
| BDI-Y | 30.9 (4.7) | 29.0 (7.9) | 0.51 | 0.634 | 1.9 (−7.9; 11.8) | 0.17 |
| C-GAS | 37.5 (4.7) | 47.7 (6.8) | −4.07 | 0.01 | −10.2 (−16.6; −3.8) | −1.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lind, M.; Kiel, L.; Hansen, S.B.; Jørgensen, M.S.; Simonsen, E. Narrative Identity within Mentalization-Based Group Therapy for Adolescents: A Feasibility Study. Children 2023, 10, 854. https://doi.org/10.3390/children10050854
Lind M, Kiel L, Hansen SB, Jørgensen MS, Simonsen E. Narrative Identity within Mentalization-Based Group Therapy for Adolescents: A Feasibility Study. Children. 2023; 10(5):854. https://doi.org/10.3390/children10050854
Chicago/Turabian StyleLind, Majse, Lennart Kiel, Sune Bo Hansen, Mie Sedoc Jørgensen, and Erik Simonsen. 2023. "Narrative Identity within Mentalization-Based Group Therapy for Adolescents: A Feasibility Study" Children 10, no. 5: 854. https://doi.org/10.3390/children10050854