
State of the Art Bowel Management for Pediatric Colorectal Problems: Anorectal Malformations
 ,
,
Abstract
:1. Introduction
2. Methods
3. Anatomic Considerations
3.1. Initial Repair
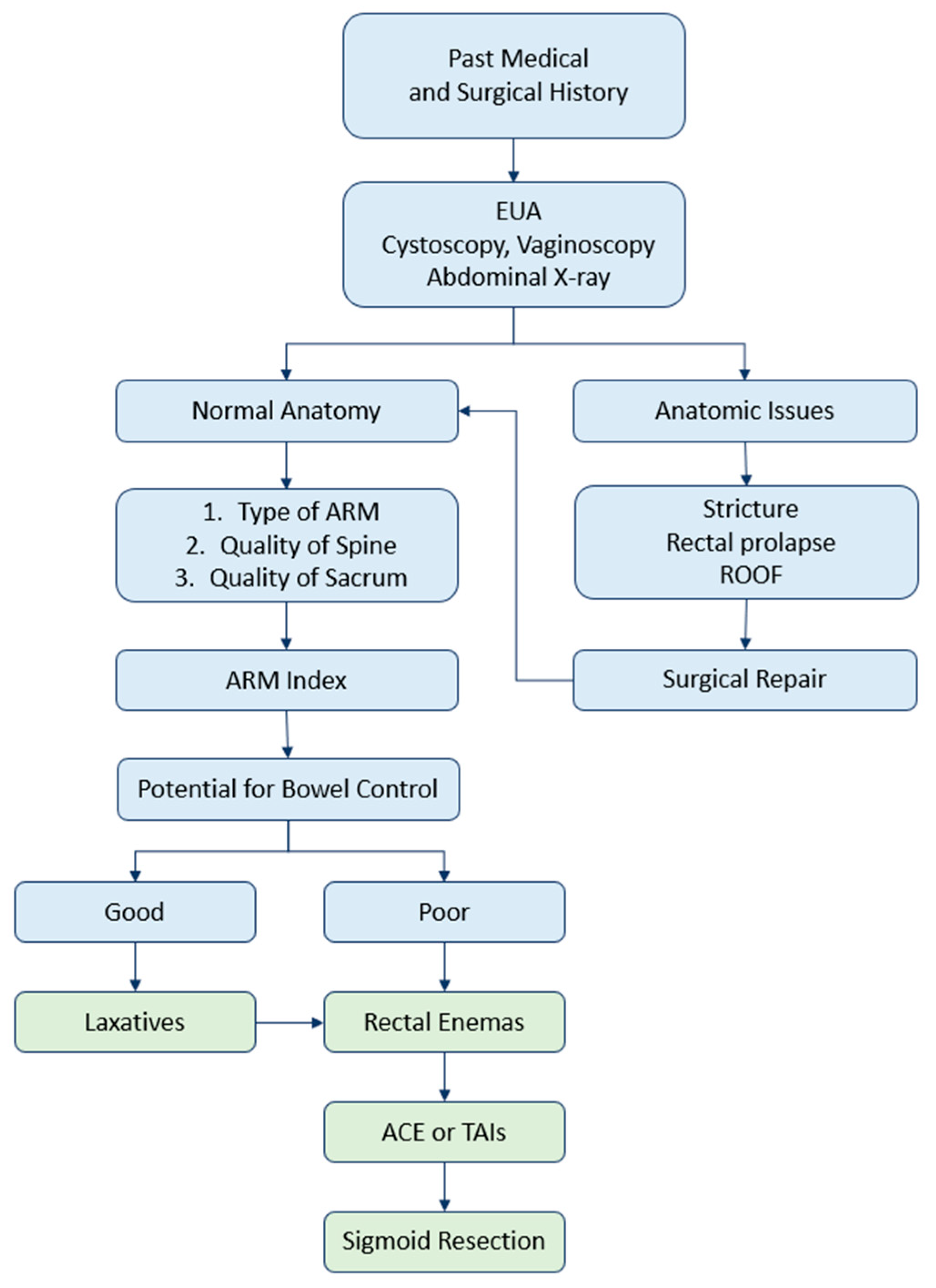
3.2. Postoperative Assessment
3.3. Anatomic Characteristics
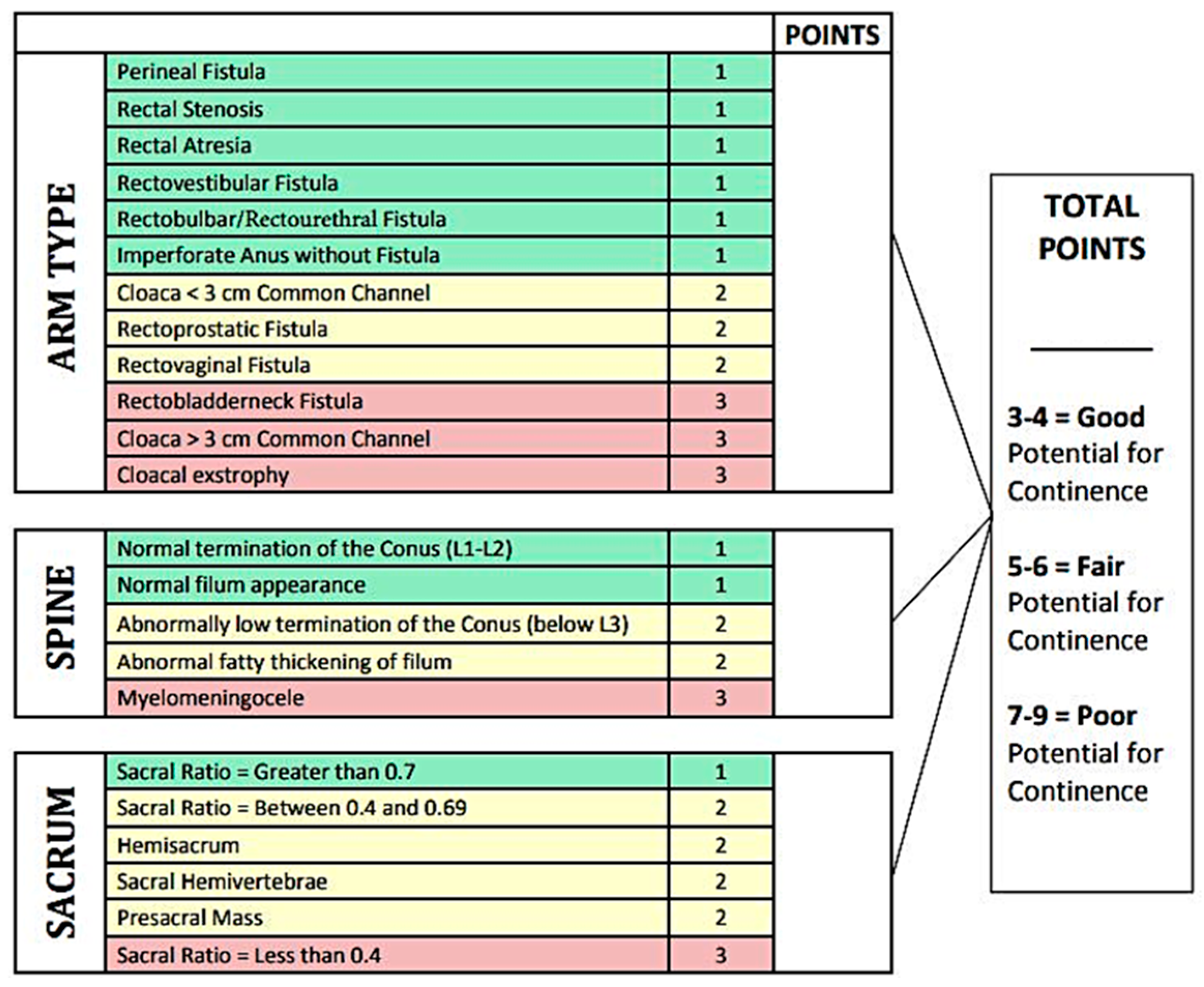
4. Potential for Continence
4.1. Type of Malformation
4.2. Sacral Development
4.3. Spinal Anomalies
4.4. ARM Index
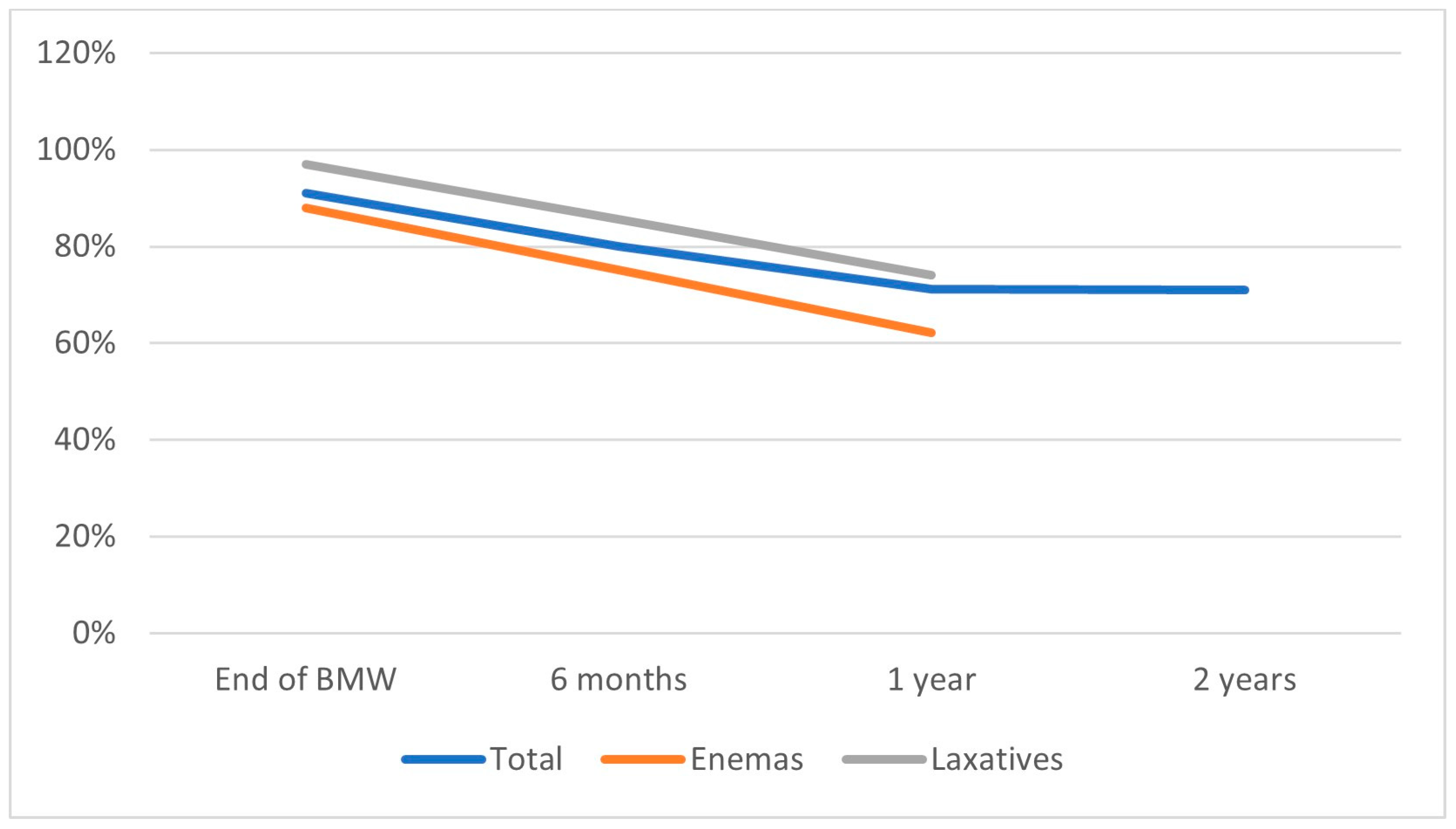
5. Bowel Management Options
5.1. Laxatives
5.2. Rectal Enemas
5.3. Transanal Irrigations
5.4. Antegrade Continence Enemas
5.5. Sigmoid Resection
6. Reoperative (Redo) Procedures—Maximizing the Anatomy
6.1. Indications
6.2. Simultaneous ACE Creation
7. Heineke–Mikulicz-like Anoplasty
8. Prognosis
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Santulli, T.V. The Treatment of Imperforate Anus and Associated Fistulas. Surg. Gynecol. Obstet. 1952, 95, 601–614. [Google Scholar] [PubMed]
- Kluth, D. Embryology of Anorectal Malformations. Semin. Pediatr. Surg. 2010, 19, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.W. Associations of Anorectal Malformations and Related Syndromes. Pediatr. Surg. Int. 2013, 29, 665–676. [Google Scholar] [CrossRef] [PubMed]
- Trusler, G.A.; Wilkinson, R.H. Imperforate Anus: A Review of 147 Cases. Can. J. Surg. 1962, 5, 269–277. [Google Scholar]
- Cuschieri, A.; Group, E.W. Anorectal Anomalies Associated with or as Part of Other Anomalies. Am. J. Med. Genet. 2002, 110, 122–130. [Google Scholar] [CrossRef]
- Qi, B.Q.; Williams, A.; Beasley, S.; Frizelle, F. Clarification of the Process of Separation of the Cloaca into Rectum and Urogenital Sinus in the Rat Embryo. J. Pediatr. Surg. 2000, 35, 1810–1816. [Google Scholar] [CrossRef]
- Solomon, B.D. VACTERL/VATER Association. Orphanet J. Rare Dis. 2011, 6, 56. [Google Scholar] [CrossRef]
- Wood, R.J.; Halleran, D.R.; Ahmad, H.; Vilanova-Sanchez, A.; Rentea, R.M.; Stallings, P.; Ganesh, N.; Gasior, A.; Levitt, M.A. Assessing the Benefit of Reoperations in Patients Who Suffer from Fecal Incontinence after Repair of Their Anorectal Malformation. J. Pediatr. Surg. 2020, 55, 2159–2165. [Google Scholar] [CrossRef]
- Lautz, T.B.; Mandelia, A.; Radhakrishnan, J. VACTERL Associations in Children Undergoing Surgery for Esophageal Atresia and Anorectal Malformations: Implications for Pediatric Surgeons. J. Pediatr. Surg. 2015, 50, 1245–1250. [Google Scholar] [CrossRef]
- Vilanova-Sanchez, A.; Gasior, A.C.; Toocheck, N.; Weaver, L.; Wood, R.J.; Reck, C.A.; Wagner, A.; Hoover, E.; Gagnon, R.; Jaggers, J.; et al. Are Senna Based Laxatives Safe When Used as Long Term Treatment for Constipation in Children? J. Pediatr. Surg. 2018, 53, 722–727. [Google Scholar] [CrossRef]
- Minneci, P.C.; Kabre, R.S.; Mak, G.Z.; Halleran, D.R.; Cooper, J.N.; Afrazi, A.; Calkins, C.M.; Downard, C.D.; Ehrlich, P.; Fraser, J.; et al. Screening Practices and Associated Anomalies in Infants with Anorectal Malformations: Results from the Midwest Pediatric Surgery Consortium. J. Pediatr. Surg. 2018, 53, 1163–1167. [Google Scholar] [CrossRef]
- Rollins, M.D.; Bucher, B.T.; Wheeler, J.C.; Horns, J.J.; Paudel, N.; Hotaling, J.M. Healthcare Burden and Cost in Children with Anorectal Malformation During the First 5 Years of Life. J. Pediatr. 2022, 240, 122–128.e2. [Google Scholar] [CrossRef]
- Huang, C.-F.; Lee, H.-C.; Yeung, C.-Y.; Chan, W.-T.; Jiang, C.-B.; Sheu, J.-C.; Wang, N.-L.; Lin, J.-R. Constipation Is a Major Complication after Posterior Sagittal Anorectoplasty for Anorectal Malformations in Children. Pediatr. Neonatol. 2012, 53, 252–256. [Google Scholar] [CrossRef]
- Stenström, P.; Kockum, C.C.; Emblem, R.; Arnbjörnsson, E.; Bjørnland, K. Bowel Symptoms in Children with Anorectal Malformation—A Follow-up with a Gender and Age Perspective. J. Pediatr. Surg. 2014, 49, 1122–1130. [Google Scholar] [CrossRef]
- Rome Foundation. Available online: Https://Theromefoundation.Org/Rome-Iv/Rome-Iv-Criteria/ (accessed on 20 December 2022).
- Koppen, I.J.N.; Nurko, S.; Saps, M.; Di Lorenzo, C.; Benninga, M.A. The Pediatric Rome IV Criteria: What’s New? Expert Rev. Gastroenterol. Hepatol. 2017, 11, 193–201. [Google Scholar] [CrossRef]
- Rintala, R.J.; Pakarinen, M.P. Outcome of Anorectal Malformations and Hirschsprung’s Disease beyond Childhood. Semin. Pediatr. Surg. 2010, 19, 160–167. [Google Scholar] [CrossRef]
- Rintala, R.J.; Lindahl, H.G.; Rasanen, M. Do Children with Repaired Low Anorectal Malformations Have Normal Bowel Function? J. Pediatr. Surg. 1997, 32, 823–826. [Google Scholar] [CrossRef]
- Pelizzo, G.; Canonica, C.P.M.; Destro, F.; Meroni, M.; Rizzo, D.; Canazza, L.; Selvaggio, G.G.O.; Durante, E.; Zuccotti, G.; Calcaterra, V. Anorectal Malformations: Ideal Surgery Timing to Reduce Incontinence and Optimize QoL. Children 2023, 10, 404. [Google Scholar] [CrossRef]
- Martynov, I.; Feng, X.; Duess, J.W.; Gosemann, J.-H.; Lacher, M.; Mayer, S. Global Development of Research on Anorectal Malformations over the Last Five Decades: A Bibliometric Analysis. Children 2022, 9, 253. [Google Scholar] [CrossRef]
- Holschneider, A.; Hutson, J.; Peña, A.; Beket, E.; Chatterjee, S.; Coran, A.; Davies, M.; Georgeson, K.; Grosfeld, J.; Gupta, D.; et al. Preliminary Report on the International Conference for the Development of Standards for the Treatment of Anorectal Malformations. J. Pediatr. Surg. 2005, 40, 1521–1526. [Google Scholar] [CrossRef]
- Lacher, M.; Badillo, A.; Vilanova-Sánchez, A.; Rentea, R.M.; Gosemann, J.-H.; Levitt, M.A. Laparoscopic Approach in Anorectal Malformations: How We Do It. J. Laparoendosc. Adv. Surg. Tech. 2021, 31, 1200–1208. [Google Scholar] [CrossRef] [PubMed]
- Nash, O.; Zobell, S.; Worst, K.; Rollins, M.D. Bowel Management for the Treatment of Fecal Incontinence and Constipation in Patients with Anorectal Malformations. Semin. Pediatr. Surg. 2020, 29, 150993. [Google Scholar] [CrossRef] [PubMed]
- Lane, V.A.; Skerritt, C.; Wood, R.J.; Reck, C.; Hewitt, G.D.; McCracken, K.A.; Jayanthi, V.R.; DaJusta, D.; Ching, C.; Deans, K.J.; et al. A Standardized Approach for the Assessment and Treatment of Internationally Adopted Children with a Previously Repaired Anorectal Malformation (ARM). J. Pediatr. Surg. 2016, 51, 1864–1870. [Google Scholar] [CrossRef] [PubMed]
- Rentea, R.M.; Halleran, D.R.; Vilanova-Sanchez, A.; Lane, V.A.; Reck, C.A.; Weaver, L.; Booth, K.; DaJusta, D.; Ching, C.; Fuchs, M.E.; et al. Diagnosis and Management of a Remnant of the Original Fistula (ROOF) in Males Following Surgery for Anorectal Malformations. J. Pediatr. Surg. 2019, 54, 1988–1992. [Google Scholar] [CrossRef]
- Alam, S.; Lawal, T.A.; Peña, A.; Sheldon, C.; Levitt, M.A. Acquired Posterior Urethral Diverticulum Following Surgery for Anorectal Malformations. J. Pediatr. Surg. 2011, 46, 1231–1235. [Google Scholar] [CrossRef]
- Scottoni, F.; Iacobelli, B.D.; Zaccara, A.M.; Totonelli, G.; Schingo, A.M.S.; Bagolan, P. Spinal Ultrasound in Patients with Anorectal Malformations: Is This the End of an Era? Pediatr. Surg. Int. 2014, 30, 829–831. [Google Scholar] [CrossRef]
- Wood, R.J.; Levitt, M.A. Anorectal Malformations. Clin. Colon. Rectal. Surg. 2018, 31, 61–70. [Google Scholar] [CrossRef]
- Bischoff, A.; Levitt, M.A.; Bauer, C.; Jackson, L.; Holder, M.; Peña, A. Treatment of Fecal Incontinence with a Comprehensive Bowel Management Program. J. Pediatr. Surg. 2009, 44, 1278–1284. [Google Scholar] [CrossRef]
- Bharucha, A.E. High Amplitude Propagated Contractions. Neurogastroenterol. Motil. 2012, 24, 977–982. [Google Scholar] [CrossRef]
- Minneci, P.C.; Kabre, R.S.; Mak, G.Z.; Halleran, D.R.; Cooper, J.N.; Afrazi, A.; Calkins, C.M.; Corkum, K.; Downard, C.D.; Ehrlich, P.; et al. Can Fecal Continence Be Predicted in Patients Born with Anorectal Malformations? J. Pediatr. Surg. 2019, 54, 1159–1163. [Google Scholar] [CrossRef]
- Rintala, R.J.; Pakarinen, M.P. Imperforate Anus: Long- and Short-Term Outcome. Semin. Pediatr. Surg. 2008, 17, 79–89. [Google Scholar] [CrossRef]
- Ahmad, H.; Halleran, D.R.; Stanek, J.R.; Thompson, B.P.; Bates, D.G.; Rusin, J.A.; Minneci, P.C.; Levitt, M.A.; Wood, R.J. Correlation between the Lateral and Anteroposterior Sacral Ratios in Anorectal Malformations. Pediatr. Radiol. 2021, 51, 1867–1872. [Google Scholar] [CrossRef]
- Metzger, G.; Cooper, J.N.; Kabre, R.S.; Mak, G.Z.; Halleran, D.R.; Boyd, K.; Chan, S.; Corea, D.; Dydynski, P.; Gill, K.; et al. Inter-Rater Reliability of Sacral Ratio Measurements in Patients with Anorectal Malformations. J. Surg. Res. 2020, 256, 272–281. [Google Scholar] [CrossRef]
- Krois, W.; Palmisani, F.; Gröpel, P.; Feil, P.; Metzelder, M.L.; Patsch, J.M.; Reck-Burneo, C.A. Assessment of Sacral Ratio in Patients with Anorectal Malformations: Can Magnetic Resonance Imaging Replace Conventional Radiograph? J. Pediatr. Surg. 2021, 56, 1993–1997. [Google Scholar] [CrossRef]
- Dewberry, L.; Peña, A.; Mirsky, D.; Ketzer, J.; Bischoff, A. Sacral Agenesis and Fecal Incontinence: How to Increase the Index of Suspicion. Pediatr. Surg. Int. 2019, 35, 239–242. [Google Scholar] [CrossRef]
- Golonka, N.R.; Haga, L.J.; Keating, R.P.; Eichelberger, M.R.; Gilbert, J.C.; Hartman, G.E.; Powell, D.M.; Vezina, G.; Newman, K.D. Routine MRI Evaluation of Low Imperforate Anus Reveals Unexpected High Incidence of Tethered Spinal Cord. J. Pediatr. Surg. 2002, 37, 966–969. [Google Scholar] [CrossRef]
- Sato, S.; Shirane, R.; Yoshimoto, T. Evaluation of Tethered Cord Syndrome Associated with Anorectal Malformations. Neurosurgery 1993, 32, 1025–1027. [Google Scholar] [CrossRef]
- Tsuda, T.; Iwai, N.; Kimura, O.; Kubota, Y.; Ono, S.; Sasaki, Y. Bowel Function after Surgery for Anorectal Malformations in Patients with Tethered Spinal Cord. Pediatr. Surg. Int. 2007, 23, 1171–1174. [Google Scholar] [CrossRef]
- Heij, H.A.; Nievelstein, R.A.; de Zwart, I.; Verbeeten, B.W.; Valk, J.; Vos, A. Abnormal Anatomy of the Lumbosacral Region Imaged by Magnetic Resonance in Children with Anorectal Malformations. Arch. Dis. Child. 1996, 74, 441–444. [Google Scholar] [CrossRef]
- Gennaro, M.D.; Rivosecchi, M.; Lucchetti, M.C.; Silveri, M.; Fariello, G.; Schingo, P. The Incidence of Occult Spinal Dysraphism and the Onset of Neurovesical Dysfunction in Children with Anorectal Anomalies. Eur. J. Pediatr. Surg. 1994, 4, 12–14. [Google Scholar] [CrossRef]
- Tunell, W.P.; Austin, J.C.; Barnes, P.D.; Reynolds, A. Neuroradiologic Evaluation of Sacral Abnormalities in Imperforate Anus Complex. J. Pediatr. Surg. 1987, 22, 58–61. [Google Scholar] [CrossRef] [PubMed]
- Karrer, F.M.; Flannery, A.M.; Nelson, M.D.; McLone, D.G.; Raffensperger, J.G. Anorectal Malformations: Evaluation of Associated Spinal Dysraphic Syndromes. J. Pediatr. Surg. 1988, 23, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Davidoff, A.M.; Thompson, C.V.; Grimm, J.K.; Shorter, N.A.; Filston, H.C.; Jerry Oakes, W. Occult Spinal Dysraphism in Patients with Anal Agenesis. J. Pediatr. Surg. 1991, 26, 1001–1005. [Google Scholar] [CrossRef] [PubMed]
- Kyrklund, K.; Pakarinen, M.P.; Taskinen, S.; Kivisaari, R.; Rintala, R.J. Spinal Cord Anomalies in Patients with Anorectal Malformations without Severe Sacral Abnormalities or Meningomyelocele: Outcomes after Expectant, Conservative Management. SPI 2016, 25, 782–789. [Google Scholar] [CrossRef] [PubMed]
- Di Cesare, A.; Leva, E.; Macchini, F.; Canazza, L.; Carrabba, G.; Fumagalli, M.; Mosca, F.; Torricelli, M. Anorectal Malformations and Neurospinal Dysraphism: Is This Association a Major Risk for Continence? Pediatr. Surg. Int. 2010, 26, 1077–1081. [Google Scholar] [CrossRef]
- Hashish, M.S.; Dawoud, H.H.; Hirschl, R.B.; Bruch, S.W.; El Batarny, A.M.; Mychaliska, G.B.; Drongowski, R.A.; Ehrlich, P.F.; Hassaballa, S.Z.; El-Dosuky, N.I.; et al. Long-Term Functional Outcome and Quality of Life in Patients with High Imperforate Anus. J. Pediatr. Surg. 2010, 45, 224–230. [Google Scholar] [CrossRef]
- Wong, C.W.Y.; Chung, P.H.Y.; Tam, P.K.H.; Wong, K.K.Y. Quality of Life and Defecative Function 10 Years or Longer after Posterior Sagittal Anorectoplasty and Laparoscopic-Assisted Anorectal Pull-through for Anorectal Malformation. Pediatr. Surg. Int. 2020, 36, 289–293. [Google Scholar] [CrossRef]
- Baxter, K.J.; Garza, J.M.; Rollins, M.D.; Drake, K.; Reeder, R.W.; Wood, R.; Avansino, J.; Calkins, C.M.; Ralls, M.; Garvey, E.M.; et al. Multi-Institutional Review of Bowel Management Strategies in Children with Anorectal Malformations. J. Pediatr. Surg. 2020, 55, 2752–2757. [Google Scholar] [CrossRef]
- Rintala, R.J.; Marttinen, E.; Virkola, K.; Rasanen, M.; Baillie, C.; Lindahl, H. Segmental Colonic Motility in Patients with Anorectal Malformations. J. Pediatr. Surg. 1997, 32, 453–456. [Google Scholar] [CrossRef]
- Lim, I.I.P.; Cushing, C.C.; Jenkins, T.; Troutt, M.; Zeller, M.H.; Hossain, M.; Rymeski, B.; Helmrath, M.; Frischer, J.S. Prospective Quality of Life Outcomes in Pediatric Fecal Incontinence Following Bowel Management. J. Pediatr. Surg. 2021, 56, 1459–1464. [Google Scholar] [CrossRef]
- Wood, R.J.; Vilanova-Sanchez, A.; El-Gohary, Y.; Ahmad, H.; Halleran, D.R.; Reck-Burneo, C.A.; Rentea, R.; Sebastiao, Y.; Nash, O.; Booth, K.; et al. One-Year Impact of a Bowel Management Program in Treating Fecal Incontinence in Patients with Anorectal Malformations. J. Pediatr. Surg. 2021, 56, 1689–1693. [Google Scholar] [CrossRef]
- Santos-Jasso, K.A.; Arredondo-García, J.L.; Maza-Vallejos, J.; Lezama-Del Valle, P. Effectiveness of Senna vs Polyethylene Glycol as Laxative Therapy in Children with Constipation Related to Anorectal Malformation. J. Pediatr. Surg. 2017, 52, 84–88. [Google Scholar] [CrossRef]
- Cogley, K.; Echevarria, A.; Correa, C.; De la Torre-Mondragón, L. Contact Burn with Blister Formation in Children Treated with Sennosides. Pediatr. Dermatol. 2017, 34, e85–e88. [Google Scholar] [CrossRef]
- Skin Breakdown and Blisters from Senna-Containing Laxatives in Young Children. Available online: https://journals.sagepub.com/doi/epub/10.1345/aph.1C439 (accessed on 24 January 2023).
- Smith, W.A.; Taintor, A.R.; Kos, L.; Drolet, B. Senna-Containing Laxative Inducing Blistering Dermatitis in Toddlers. Arch. Dermatol. 2012, 148, 402–404. [Google Scholar] [CrossRef]
- Leventhal, J.M.; Griffin, D.; Duncan, K.O.; Starling, S.; Christian, C.W.; Kutz, T. Laxative-Induced Dermatitis of the Buttocks Incorrectly Suspected to Be Abusive Burns. Pediatrics 2001, 107, 178–180. [Google Scholar] [CrossRef]
- MacDuff, S.; Sun, J.; Bell, D.E.; Lentz, C.W.; Kahn, S.A. Accidental Burn by Intentional Laxative Use. Pediatr. Emerg. Care 2016, 32, 541–543. [Google Scholar] [CrossRef]
- Durani, P.; Agarwal, R.; Wilson, D.I. Laxative-Induced Burns in a Child. J. Plast. Reconstr. Aesthetic Surg. 2006, 59, 1129. [Google Scholar] [CrossRef]
- Accidental, but Initially Suspicious, Injury—McManus—2014—Journal of Paediatrics and Child Health—Wiley Online Library. Available online: https://onlinelibrary.wiley.com/doi/10.1111/jpc.12459 (accessed on 24 January 2023).
- Melvin, J.E.; Hickey, R.W. Laxative-Induced Contact Dermatitis. Pediatr. Emerg. Care 2019, 35, e127. [Google Scholar] [CrossRef]
- Bischoff, A.; Tovilla, M. A Practical Approach to the Management of Pediatric Fecal Incontinence. Semin. Pediatr. Surg. 2010, 19, 154–159. [Google Scholar] [CrossRef]
- Märzheuser, S.; Grauel, F.; Rothe, K. Treatment for fecal incontinence in patients with anorectal malformations. Introduction of a therapeutic approach. Pflege Z 2013, 66, 612–615. [Google Scholar]
- Nash, O.; Choueiki, J.; Levitt, M.A. Fecal Incontinence and Constipation in Children: Case Studies; CRC Press: Boca Raton, FL, USA, 2020. [Google Scholar]
- Ambartsumyan, L.; Rodriguez, L. Bowel Management in Children with Spina Bifida. PRM 2018, 11, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Märzheuser, S.; Karsten, K.; Rothe, K. Improvements in Incontinence with Self-Management in Patients with Anorectal Malformations. Eur. J. Pediatr. Surg. 2015, 26, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Corbett, P.; Denny, A.; Dick, K.; Malone, P.S.; Griffin, S.; Stanton, M.P. Peristeen Integrated Transanal Irrigation System Successfully Treats Faecal Incontinence in Children. J. Pediatr. Urol. 2014, 10, 219–222. [Google Scholar] [CrossRef] [PubMed]
- Midrio, P.; Mosiello, G.; Ausili, E.; Gamba, P.; Marte, A.; Lombardi, L.; Iacobelli, B.D.; Caponcelli, E.; Marrello, S.; Meroni, M.; et al. Peristeen® Transanal Irrigation in Paediatric Patients with Anorectal Malformations and Spinal Cord Lesions: A Multicentre Italian Study. Color. Dis. 2016, 18, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Lallemant-Dudek, P.; Cretolle, C.; Hameury, F.; Lemelle, J.L.; Ranke, A.; Louis-Borrione, C.; Forin, V. Multicentric Evaluation of the Adherence to Peristeen® Transanal Irrigation System in Children. Ann. Phys. Rehabil. Med. 2020, 63, 28–32. [Google Scholar] [CrossRef]
- Peeraully, R.; Langley, J.; Hayes, N.; Storry, K.; Richardson, L.; Burridge, D.; More, B. Transition and Reversal: Long-Term Experience of the MACE Procedure in Children. Pediatr. Surg. Int. 2022, 38, 883–889. [Google Scholar] [CrossRef]
- Bokova, E.; Svetanoff, W.J.; Levitt, M.A.; Rentea, R.M. Pediatric Bowel Management Options and Organizational Aspects. Children 2023, 10, 633. [Google Scholar] [CrossRef]
- Keshtgar, A.S.; Ward, H.C.; Richards, C.; Clayden, G.S. Outcome of Excision of Megarectum in Children with Anorectal Malformation. J. Pediatr. Surg. 2007, 42, 227–233. [Google Scholar] [CrossRef]
- Hallows, M.R.; Lander, A.D.; Corkery, J.J. Anterior Resection for Megarectosigmoid in Congenital Anorectal Malformations. J. Pediatr. Surg. 2002, 37, 1464–1466. [Google Scholar] [CrossRef]
- Borg, H.; Bachelard, M.; Sillén, U. Megarectosigmoid in Children with Anorectal Malformations: Long Term Outcome after Surgical or Conservative Treatment. J. Pediatr. Surg. 2014, 49, 564–569. [Google Scholar] [CrossRef]
- Brisighelli, G.; Di Cesare, A.; Morandi, A.; Paraboschi, I.; Canazza, L.; Consonni, D.; Leva, E. Classification and Management of Rectal Prolapse after Anorectoplasty for Anorectal Malformations. Pediatr. Surg. Int. 2014, 30, 783–789. [Google Scholar] [CrossRef]
- Mitrofanoff, P. Trans-appendicular continent cystostomy in the management of the neurogenic bladder. Chir. Pediatr. 1980, 21, 297–305. [Google Scholar]
- Monti, P.R.; Lara, R.C.; Dutra, M.A.; de Carvalho, J.R. New Techniques for Construction of Efferent Conduits Based on the Mitrofanoff Principle. Urology 1997, 49, 112–115. [Google Scholar] [CrossRef]
- Malone, P.S.J. The Antegrade Continence Enema Procedure. BJU Int. 2004, 93, 248–249. [Google Scholar] [CrossRef]
- Chatoorgoon, K.; Pena, A.; Lawal, T.; Hamrick, M.; Louden, E.; Levitt, M.A. Neoappendicostomy in the Management of Pediatric Fecal Incontinence. J. Pediatr. Surg. 2011, 46, 1243–1249. [Google Scholar] [CrossRef]
- Shandling, B.; Chait, P.G.; Richards, H.F. Percutaneous Cecostomy: A New Technique in the Management of Fecal Incontinence. J. Pediatr. Surg. 1996, 31, 534–537. [Google Scholar] [CrossRef]
- Zann, A.; Sebastiao, Y.; Ching, C.C.; Fuchs, M.; Jayanthi, V.R.; Wood, R.J.; Levitt, M.A.; DaJusta, D. Split Appendix Mitrofanoffs Have Higher Risk of Complication than Intact Appendix or Monti Channels. J. Pediatr. Urol. 2021, 17, 700.e1–700.e6. [Google Scholar] [CrossRef]
- VanderBrink, B.A.; Cain, M.P.; Kaefer, M.; Meldrum, K.K.; Misseri, R.; Rink, R.C. Split-Appendix Technique for Simultaneous Appendicovesicostomy and Appendicocecostomy. J. Pediatr. Surg. 2011, 46, 259–262. [Google Scholar] [CrossRef]
- deVries, P.A.; Peña, A. Posterior Sagittal Anorectoplasty. J. Pediatr. Surg. 1982, 17, 638–643. [Google Scholar] [CrossRef]
- Peña, A.; Devries, P.A. Posterior Sagittal Anorectoplasty: Important Technical Considerations and New Applications. J. Pediatr. Surg. 1982, 17, 796–811. [Google Scholar] [CrossRef]
- Brisighelli, G.; Morandi, A.; Cesare, A.D.; Leva, E. The Practice of Anal Dilations Following Anorectal Reconstruction in Patients with Anorectal Malformations: An International Survey. Eur. J. Pediatr. Surg. 2016, 26, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Peña, A. Anorectal Malformations. Semin. Pediatr. Surg. 1995, 4, 35–47. [Google Scholar] [PubMed]
- Ahmad, H.; Skeritt, C.; Halleran, D.R.; Rentea, R.M.; Reck-Burneo, C.A.; Vilanova-Sanchez, A.; Weaver, L.; Langer, J.C.; Diefenbach, K.A.; Gasior, A.C.; et al. Are Routine Postoperative Dilations Necessary after Primary Posterior Sagittal Anorectoplasty? A Randomized Controlled Trial. J. Pediatr. Surg. 2021, 56, 1449–1453. [Google Scholar] [CrossRef] [PubMed]
- Lawal, T.A.; Reck, C.A.; Wood, R.J.; Lane, V.A.; Gasior, A.; Levitt, M.A. Use of a Heineke-Mikulicz like Stricturoplasty for Intractable Skin Level Anal Strictures Following Anoplasty in Children with Anorectal Malformations. J. Pediatr. Surg. 2016, 51, 1743–1745. [Google Scholar] [CrossRef]
- Halleran, D.R.; Sanchez, A.V.; Rentea, R.M.; Ahmad, H.; Weaver, L.; Reck, C.; Gasior, A.C.; Levitt, M.A.; Wood, R.J. Assessment of the Heineke–Mikulicz Anoplasty for Skin Level Postoperative Anal Strictures and Congenital Anal Stenosis. J. Pediatr. Surg. 2019, 54, 118–122. [Google Scholar] [CrossRef]
- Lombardi, L.; Garrisi, E.; Riccò, M.; Marchesi, F.; Casolari, E.; Gatti, C.; Rossi, C. Study of Intestinal Function in Anorectal Malformations: The Role of Bowel Management in Quality of Life. Acta Bio-Med. Atenei Parm. 2016, 87, 197–204. [Google Scholar]
- Kilpatrick, J.A.; Zobell, S.; Leeflang, E.J.; Cao, D.; Mammen, L.; Rollins, M.D. Intermediate and Long-Term Outcomes of a Bowel Management Program for Children with Severe Constipation or Fecal Incontinence. J. Pediatr. Surg. 2020, 55, 545–548. [Google Scholar] [CrossRef]
- Hassan, L.; Cortenraad, S.A.M.; Rosenberg, C.B.M.; Kimman, M.L.; Haanen, M.; van Gemert, W.G.; Visschers, R.G.J. Protocol for the Development of a Core Outcome Set for the Optimisation of Treatment and Follow-up of Patients with an Anorectal Malformation (ARM): The ARM and OUtcome Review (ARMOUR)-Project. BMJ Paediatr. Open 2023, 7, e001691. [Google Scholar] [CrossRef]
- Reeder, R.W.; Wood, R.J.; Avansino, J.R.; Levitt, M.A.; Durham, M.M.; Sutcliffe, J.; Midrio, P.; Calkins, C.M.; de Blaauw, I.; Dickie, B.H.; et al. The Pediatric Colorectal and Pelvic Learning Consortium (PCPLC): Rationale, Infrastructure, and Initial Steps. Tech. Coloproctol. 2018, 22, 395–399. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Rome IV Criteria for Constipation in Infants and Children * |
|---|
|
|
|
|
|
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bokova, E.; Svetanoff, W.J.; Lopez, J.J.; Levitt, M.A.; Rentea, R.M. State of the Art Bowel Management for Pediatric Colorectal Problems: Anorectal Malformations. Children 2023, 10, 846. https://doi.org/10.3390/children10050846
Bokova E, Svetanoff WJ, Lopez JJ, Levitt MA, Rentea RM. State of the Art Bowel Management for Pediatric Colorectal Problems: Anorectal Malformations. Children. 2023; 10(5):846. https://doi.org/10.3390/children10050846
Chicago/Turabian StyleBokova, Elizaveta, Wendy Jo Svetanoff, Joseph J. Lopez, Marc A. Levitt, and Rebecca M. Rentea. 2023. "State of the Art Bowel Management for Pediatric Colorectal Problems: Anorectal Malformations" Children 10, no. 5: 846. https://doi.org/10.3390/children10050846