
Therapy of Patients with Cardiac Malposition


Children’s Heart Institute, Children’s Memorial Hermann Hospital, McGovern Medical School, University of Texas-Houston, 6410 Fannin Street, UTPB Suite # 425, Houston, TX 77030, USA
Children 2023, 10(4), 739; https://doi.org/10.3390/children10040739
Submission received: 10 March 2023
/
Revised: 31 March 2023
/
Accepted: 14 April 2023
/
Published: 17 April 2023
(This article belongs to the Section Pediatric Cardiology)
Abstract
:Positional abnormalities per se do not require treatment, but in their place, the accompanying pulmonary pathology in dextroposition patients and pathophysiologic hemodynamic abnormalities resulting from multiple defects in patients with cardiac malposition should be the focus of treatment. At the time of the first presentation, treating the pathophysiologic aberrations caused by the defect complex, whether it is by improving the pulmonary blood flow or restricting it, is the first step. Some patients with simpler or single defects are amenable to surgical or transcatheter therapy and should be treated accordingly. Other associated defects should also be treated appropriately. Biventricular or univentricular repair dependent on the patient’s cardiac structure should be planned. Complications in-between Fontan stages and after conclusion of Fontan surgery may occur and should be promptly diagnosed and addressed accordingly. Several other cardiac abnormalities unrelated to the initially identified heart defects may manifest in adulthood, and they should also be treated.
1. Introduction
In a previous paper on the “Diagnosis of Dextrocardia with a Pictorial Rendition of Terminology and Diagnosis”, a detailed discussion of the diagnosis of dextrocardia including other cardiac malpositions was presented [1]. In that review, a pictorial presentation of terminology and diagnosis was made. Following exclusion of dextroposition, segmental analysis is undertaken examining the visceroatrial situs, ventricular localization, atrioventricular connections, great artery relationship, and conotruncal alignment. Electrocardiogram, chest X-ray, echocardiogram, and other imaging studies, including selective cineangiography, are utilized for this assessment. Once the atrial, ventricular, and great artery sites are identified, septal defects and obstructive lesions of cardiac valves and blood vessels are diagnosed using the conventional cardiovascular evaluation methodology. Treatment of cardiac malposition was not included in that paper [1] because of space limitations. In the current paper, therapy of cardiac malposition is reviewed.
2. Therapy
Abnormal positions themselves do not require therapy; however, the associated boney and pulmonary abnormalities in dextroposition subjects and hemodynamic anomalies caused by multiple associated defects in patients with cardiac malposition should be treated. The management of dextroposition and dextrocardia, including other cardiac malpositions, will be reviewed separately. Discussion of management of other cardiac malpositions, namely, ectopia cordis and pericardial defects, is not included in this paper.
3. Management of Dextroposition
In patients with dextroposition secondary to a thoracic cage boney abnormality, no treatment is necessary because the heart is usually just displaced without any compression of the cardiac chambers. On extremely rare occasions, when obstruction of a given cardiac chamber occurs [2], treatment may be warranted to relieve the obstructive element. In patients with cardiac displacement due to empyema, pneumothorax, congenital pulmonary cyst, lobar emphysema, or left-sided diaphragmatic hernia displacing the heart to the right side and collapse of the right lung, hypoplastic right lung, or right pneumonectomy pulling the heart to the right, the primary lung abnormality should be addressed as detailed in standard textbooks of pediatrics, pediatric surgery, and respiratory system disorders and is not reviewed here. In subjects with scimitar syndrome, the accompanying partial anomalous pulmonary venous return, defects in the atrial septum, and an abnormal systemic vascular connection to the sequestered pulmonary segment should be addressed surgically or by transcatheter methodology, as deemed appropriate, [3,4,5,6] and no treatment of cardiac displacement is necessary.
4. Management of Cardiac Malposition
Positional abnormalities of the heart themselves do not require any therapy, but, in their place, the accompanying heart defects and the ensuing hemodynamic abnormalities should be treated and are reviewed hereunder. The clinical scenarios and their management options are listed in a tabular form in Table 1.
4.1. Management at Initial Presentation
Patients with complex heart defects present with symptomatology early in the newborn period while subjects with simpler and milder heart defects may come to light later in infancy, childhood, and adulthood. Treatment at first presentation of neonates is similar to that utilized for other cyanotic congenital heart defects (CHDs) and is described elsewhere [7,8] and includes avoiding hypothermia, preserving neutral thermal setting, detection and appropriate treatment of hypocalcemia and hypoglycemia, monitoring the acid–base balance, treating metabolic acidosis with NaHCO3, and managing acidosis secondary to respiratory problems with suction, tracheal cannulation, and assisted ventilation as suitable. In patients with suspected ductal dependent lesions, intravenous prostaglandin E1 (PGE1) infusion [9,10,11,12] should begin while waiting for the final diagnosis.
Following stabilization of the baby, treatment should focus on the pathophysiologic anomaly (pulmonary oligemia and pulmonary plethora) produced by the associated cardiac defects that many of the cardiac malposition infants have. Pulmonary oligemia should be addressed at presentation to prevent both short-term adverse effects such as hypoxemia, progressive acidosis, and death and long-term consequences, namely, the development of clubbing of fingers and toes, cerebrovascular accidents, relative anemia, severe polycythemia, paradoxical embolism, brain abscess, coagulation abnormalities, hyperuricemia, uric acid nephropathy, and gout. Pulmonary plethora should be tackled to avoid short-term effects, namely, congestive heart failure (CHF) and death as well as long-term consequences, namely, the development of pulmonary hypertension, progressive dilation of the left ventricle, and pulmonary vascular obstructive disease (PVOD). In addition, addressing both pulmonary oligemia and pulmonary plethora in a timely manner is likely to help normal pulmonary alveolar development.
In infants with decreased pulmonary blood flow secondary to severe narrowing or atresia of the pulmonary artery or valve and a big VSD or a single ventricle, administration of PGE1 starts at an initial dosage of 0.05 to 0.1 μg/kg/min, which may be gradually decreased to 0.015 to 0.02 μg/kg/min. Following stabilization of the infant, a more permanent provision of blood flow to the pulmonary circuit should ensue, usually by a modified Blalock–Taussig (BT) anastomosis [13,14,15] (Figure 1 and Figure 2). Alternative solutions are ductal stenting [16,17,18] and balloon pulmonary valvuloplasty [19], where applicable.
Babies with elevated pulmonary blood flow and CHF should receive decongestive treatment and then surgery to repair the defect if amenable to surgical correction as an infant. If not, pulmonary artery banding [22,23,24] is undertaken (Figure 3 and Figure 4) to decrease the pressures and blood flow in the pulmonary circuit and avoid the development of PVOD. In this scenario, total surgical correction is planned to be performed later. Nevertheless, since there is an elevated pulmonary vascular resistance (PVR) when the baby is born and a slow regression of the PVR in patients with large interventricular communication, most of these neonates may not go into CHF early in life. These infants should be diligently followed and treated to prevent the onset of PVOD.
Neonates with the total anomalous pulmonary venous return (TAPVR) with an obstruction to the pulmonary venous return should have immediate surgical correction [26,27,28,29]. It should be noted that some newborn infants with markedly reduced pulmonary blood flow may manifest TAPVR only after performing BT shunting. Currently, improved echo techniques facilitate accurate identification of TAPVR at the time of the initial presentation.
Other problems, namely, interatrial obstruction, interventricular obstruction, aortic arch interruption, and aortic coarctation may be seen at presentation or may develop later [25] and should be addressed with transcatheter or surgical therapy as appropriate.
Subjects with simpler and single defects such as pulmonary valvar stenosis [30], atrial [31,32,33,34,35] or ventricular [36,37] septal defects and patent ductus arteriosus, though rare, should be addressed with either catheter-based [31,32,33,34,35,36] or surgical [37] procedures, as deemed appropriate.
4.2. Additional Surgery
After initial palliation, as reviewed above, a methodical review of all the available imaging studies should be performed to assess the feasibility of undertaking biventricular repair [38,39,40,41]. If biventricular repair is not possible, consideration for single ventricle palliation via the Fontan route [42,43,44,45] should be given. Currently, the Fontan procedure is accomplished using the concept of total cavopulmonary connection (TCPC) proposed by de Leval et al. [46] in a staged fashion [47]. An extracardiac conduit [48,49] with fenestration [50,51,52] is used for completion of the Fontan operation Subsequently, device occlusion of the fenestration [51,53,54,55,56] is undertaken.
4.2.1. Stage I
This stage is as described in the “Management at Initial Presentation” segment.
4.2.2. Stage II
4.2.3. Stage IIIA
4.2.4. Stage IIIB
5. Management of Noncardiac Issues
As mentioned above, some of the babies with cardiac malposition, particularly those with isolated dextrocardia and isolated levocardia, are likely to have heterotaxy, and these patients with asplenia/polysplenia syndrome usually have a deficient splenic function. Consequently, such infants are at a greater risk of bacterial infections [64,65]. Throughout infancy, these babies should be treated with prophylactic doses of ampicillin/amoxicillin. During childhood, the preventive regimen may be switched to oral penicillin. Furthermore, there is a high risk of occurrence of gastrointestinal obstruction and, therefore, prophylactic Ladd’s procedure [66,67] is recommended at most institutions caring for such babies to prevent the development of an obstruction of the gastrointestinal tract.
6. Interstage Issues
In patients with single ventricles, both the pulmonary and systemic circulations work in parallel in place of the normal in-series circulation. Consequently, a finite equilibrium connecting both circulations should be preserved to ensure an adequate flow into both systemic and pulmonary circuits [25,68]. In case such an equilibrium cannot be preserved, significant morbidity and mortality may ensue in these susceptible babies. Mortality in-between stages has been reported, which varies from 5 to 15% [25,69,70]. The identified causes of interstage mortality are obstructed patent foramen ovale (PFO), aortic coarctation, aortic arch interruption, narrowing of the pulmonary arteries, atrioventricular valve insufficiency, obstruction of the surgically created aortopulmonary shunts, and intercurrent illnesses [69,70]. The stated interstage mortality occurs more often in-between Stages I and II than in-between Stages II and III. Although these studies [69,70] mostly involve hypoplastic left heart syndrome subjects, these findings are equally relevant to patients with a single ventricle seen in malposition of the heart. Strategies to avert and manage interstage issues are timely assessment by careful history and physical examination, including echocardiography and other imaging investigations, namely, magnetic resonance imaging (MRI) and computed tomography (CT), to detect the anomalies listed in the preceding section and provide a suitable management of these problems to avert/decrease the mortality and morbidity [20,25,71,72]. Intercurrent illnesses resulting in dehydration, acidosis, or high temperature may interrupt the balance in-between the systemic and pulmonary circuits, and the infants could develop serious illness [71,72]. Rapid attention to treat intercurrent illnesses is important [25,71,72]. Further review of the methods of treatment of interstage issues is beyond the scope of this paper and the involved persons may refer to other reviews [20,25,73].
7. Postintervention Complications
Several complications were reported in subjects who had a Fontan operation. The reported complications were arrhythmias, obstructed Fontan pathways, residual intra-/extracardiac shunts, cyanosis, thromboembolism, transient ischemic attacks, cerebrovascular accidents, collateral vessel formation, congestion of the systemic venous circuit, and protein-losing enteropathy [63,74,75,76]. Coincidentally, such problems happen less often in babies who had undergone the presently utilized staged TCPC with an extracardiac conduit than in subjects who had previously utilized the atriopulmonary anastomosis type of Fontan surgery. Clinical and echocardiographic evaluation for the existence of the abovelisted complications during follow-up and prompt treatment by either surgical or transcatheter methodology, as deemed appropriate, should be pursued. A review of these management options is beyond the scope of this paper; this information may be found elsewhere [63,73,75,76].
8. Management of Cardiac Malposition Patients during Adulthood
Adult patients with cardiac malposition, apart from the postintervention problems reviewed in the aforementioned sections, may also develop problems akin to those seen in normal (levocardia) adults. Management of these issues is reviewed in this section.
8.1. Coronary Artery Disease
Coronary artery obstruction and myocardial infarction do occur in cardiac malposition patients; the prevalence of coronary problems is generally thought to be comparable to that seen in the general population [77]. It is necessary to record right chest leads to detect the ST segment elevation to identify myocardial infarction [78,79,80,81]. Percutaneous coronary intervention (PCI) [82,83,84,85,86,87,88,89] or surgical coronary artery bypass (CAB) [90], as deemed appropriate, should be performed promptly. Transradial approach for PCI has also been used successfully [91,92]. Immediate results of both PCIs and CAB [77,82,83,84,85,86,87,88,89,90,91,92] appear to be beneficial while long-term results have not been documented.
8.2. Supraventricular Arrhythmias
Supraventricular arrhythmias also occur in dextrocardia patients, and it is generally thought that the incidence of these arrhythmias is not substantially different from that observed in the normal population (levocardia). Atrial fibrillation/flutter appear to be the most common among these arrhythmias while supraventricular tachycardia (SVT), including atrioventricular reentrant tachycardia (AVRT) and SVT associated with WPW (Wolff–Parkinson–White) syndrome, can also occur. Arrhythmias are usually treated with antiarrhythmic medications and patients without adequate control are subjected to catheter ablation procedures (cryoablation or radiofrequency (RF) ablation). The feasibility of catheter ablation procedures for atrial fibrillation/flutter [93,94,95,96,97,98,99,100], supraventricular tachycardia [101,102,103], including AVRT [101] and WPW syndrome [104], was demonstrated. Patients with an interrupted inferior vena cava should undergo the procedure using the jugular venous approach. Integration of echocardiograms, cardiac CT, three-dimensional (3D) imaging, and 3D reconstruction are necessary to accomplish catheter ablation procedures.
8.3. Complete Atrioventricular Block or Sick Sinus Syndrome
8.4. Prevention
8.4.1. Prevention of Sudden Death
Some patients with dextrocardia have a higher propensity for sudden cardiac death; such patients may need implantable cardioverter–defibrillators (ICD). While transvenous ICDs are the first-line therapy, transvenous access may be difficult because of congenital venous anomalies or acquired venous obstruction. In such patients, subcutaneous ICDs (S-ICDs) (Emblem A219; Boston Scientific, Marlborough, MA, USA) may be implanted. The reported experience with this form of therapy is encouraging [113,114,115,116,117].
8.4.2. Prevention of Embolic Episodes
Subjects who have atrial fibrillation/flutter are at risk of developing embolic episodes and, therefore, initial anticoagulation and subsequent occlusion of the left atrial appendage are recommended. While closure of the appendage of the left atrium is challenging in dextrocardia subjects, it can be successfully accomplished [118,119,120].
8.5. Aortic Valve Disease
Aortic valve (AV) abnormalities causing severe aortic regurgitation or severe stenosis may occur in dextrocardia patients [121,122,123,124,125,126]. Simpler balloon aortic valvuloplasty or surgical repair may be offered in younger populations. Transcatheter [121,122,123,124,125] or surgical [126] replacement of the AV may be offered for the elderly to address AV abnormalities [121,122,123,124,125,126].
8.6. Mitral Valve Disease
Mitral valve abnormalities producing severe mitral regurgitation have been seen in dextrocardia. Surgical repair [127] or replacement [128,129,130] of the mitral valve can be safely performed [127,128,129,130].
Rheumatic fever appears to occur in dextrocardia patients as well, resulting in mitral stenosis. When mitral stenosis is severe, surgical commissurotomy [131] or balloon mitral valvuloplasty with either conventional balloons or Inoue balloons [132,133,134,135,136,137,138,139,140] could be successfully performed.
8.7. Hypertrophic Cardiomyopathy and Subaortic Obstruction
Hypertrophic cardiomyopathy (HCM), while rarely reported in patients with cardiac malposition, has been described [141,142,143]. Some patients with HCM may have a severe obstruction of the outflow tract of the left ventricle [144]. If betablocker therapy does not relieve the left ventricular outflow tract (LVOT) obstruction, surgical myectomy or alcohol septal ablation (ASA) [144] may become necessary. In this report [144], the authors were able to reduce the LVOT gradient from 136 to 50 mm Hg along with symptomatic improvement. The presented case illustrates the feasibility of performing ASA in dextrocardia patients.
9. Summary and Conclusions
Addressing pulmonary pathology in patients with dextroposition as per the guidelines established in standard textbooks is appropriate. In cardiac malposition, treatment of the pathophysiologic abnormality produced by multiple defects at the time of initial presentation by either increasing the pulmonary blood flow or restricting it is first undertaken. Other cardiac defects are also addressed to optimize the care. The feasibility of biventricular repair should be explored, and if that is not feasible, a single ventricular repair option (Fontan) should be offered. Antibiotic prophylaxis and prophylactic Ladd’s procedure are prescribed in heterotaxy patients. Complications following initial palliative procedures and subsequent Fontan surgery may occur, and these should be promptly detected and treated in a timely manner. Adult patients with dextrocardia, in addition to postintervention complications, may develop other disease entities, similar to those seen in the normal population, and these should be treated with either surgical or transcatheter methodology, as deemed appropriate. It is concluded that most of the problems encountered in patients with dextroposition and dextrocardia can be effectively treated with the currently available therapeutic modalities.
Funding
This research received no external funding.
Institutional Review Board Statement
Institutional review boards approved the respective studies.
Informed Consent Statement
Informed consent was obtained from all the subjects involved in the respective studies.
Data Availability Statement
Not applicable.
Conflicts of Interest
The author declares no conflict of interest.
References
- Rao, P.S.; Rao, N.S. Diagnosis of dextrocardia with a pictorial rendition of terminology and diagnosis. Children 2022, 9, 1977. [Google Scholar] [CrossRef] [PubMed]
- Mazur, L.; deYbarrondo, L.; Pickard, L.; Rao, P.S. Development of supravalvular pulmonary artery stenosis following a Nuss procedure. J. Pediatr. Surg. 2012, 47, e61–e64. [Google Scholar] [CrossRef] [PubMed]
- Neill, C.A.; Ferencz, C.; Sabiston, D.C.; Sheldon, H. The familial occurrence of hypoplastic right lung with systemic arterial supply and venous drainage “scimitar syndrome”. Bull. Johns Hopkins Hosp. 1960, 107, 1–21. [Google Scholar] [PubMed]
- Dickinson, D.F.; Galloway, R.W.; Massey, R.; Sankey, R.; Arnold, R. Scimitar syndrome in infancy. Role of embolisation of systemic arterial supply to right lung. Br. Heart J. 1982, 47, 468–472. [Google Scholar] [CrossRef]
- Mardini, M.K.; Rao, P.S. Scimitar syndrome: Experience with four patients and review of literature. Arab J. Med. 1984, 3, 13–23. [Google Scholar]
- Poncelet, A.J.; Carbonez, K.; Rubay, J.E. Autologous vascularized pericardial flap tunneling technique in Scimitar syndrome repair with dextrocardia: Lessons from the Senning procedure. Cardiol. Young 2021, 31, 859–861. [Google Scholar] [CrossRef]
- Rowe, R.D.; Freedom, R.M.; Mehrizi, A. The Neonate with Congenital Heart Disease; W.B. Saunders Co.: Philadelphia, PA, USA, 1981; pp. 1–70. [Google Scholar]
- Rao, P.S. Principles of management of the neonate with congenital heart disease. In A Multidisciplinary Approach to Perinatal Cardiology; Rao, P.S., Vidyasagar, D., Eds.; Cambridge Scholars Publishing: New Castle upon Tyne, UK, 2021; Volume 1, pp. 474–509. [Google Scholar]
- Olley, P.M.; Coceani, F. Use of prostaglandins in cardiopulmonary diseases of the newborn. Semin. Perinatol. 1980, 4, 135–141. [Google Scholar]
- Heymann, M.A.; Rudolph, A.M. Neonatal manipulation: Patent ductus arteriosus. Clin. Cardiol. 1981, 11, 301–310. [Google Scholar]
- Singh, Y.; Mikrou, P. Use of prostaglandins in duct-dependent congenital heart conditions. Arch. Dis. Child. Educ. Pract. 2018, 103, 137–140. [Google Scholar] [CrossRef]
- Hew, M.R.; Gerriets, V. Prostaglandin E1. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Blalock, A.; Taussig, H.B. The surgical treatment of malformations of the heart in which there is pulmonary stenosis or atresia. J. Am. Med. Assoc. 1945, 128, 189–194. [Google Scholar] [CrossRef]
- De Leval, M.R.; McKay, R.; Jones, M.; Stark, J.; Macartney, F.J. Modified Blalock-Taussig shunt: Use of subclavian orifice as a flow regulator in prosthetic systemic-pulmonary artery shunts. J. Thorac. Cardiovasc. Surg. 1981, 18, 112–119. [Google Scholar] [CrossRef]
- Li, D.; Wang, Y.; Lin, K.; An, Q. Modified Blalock-Taussig shunt: A single-center experience and follow-up. Heart Surg. Forum 2020, 23, E053–E057. [Google Scholar] [CrossRef]
- Siblini, G.; Rao, P.S.; Singh, G.K.; Tinker, K.; Balfour, I.C. Transcatheter management of neonates with pulmonary atresia and intact ventricular septum. Catheter. Cardiovasc. Diagn. 1997, 42, 395–402. [Google Scholar] [CrossRef]
- Alwi, M.; Choo, K.K.; Latiff, H.A.; Kandavello, G.; Samion, H.; Mulyadi, M.D. Initial results, and medium-term follow-up of stent implantation of patent ductus arteriosus in duct-dependent pulmonary circulation. J. Am. Coll. Cardiol. 2004, 44, 438–445. [Google Scholar] [CrossRef]
- Ruiz, C.E. Ductal stents in the management of congenital heart defects. Catheter. Cardiovasc. Interv. 2001, 53, 75–80. [Google Scholar] [CrossRef]
- Rao, P.S.; Brais, M. Balloon pulmonary valvuloplasty for congenital cyanotic heart defects. Am. Heart J. 1988, 115, 1105–1110. [Google Scholar] [CrossRef]
- Rao, P.S. Double-Inlet left ventricle. Children 2022, 9, 1274. [Google Scholar] [CrossRef]
- Rao, P.S. Echocardiography in the diagnosis and management of tricuspid atresia. Appl. Sci. 2021, 11, 9472. [Google Scholar] [CrossRef]
- Muller, W.H., Jr.; Danimann, J.F., Jr. The treatment of certain congenital malformations of the heart by the creation of pulmonic stenosis to reduce pulmonary hypertension and excessive pulmonary blood flow, a preliminary report. Surg. Gynecol. Obstet. 1952, 95, 213–219. [Google Scholar]
- Afifi, A.R.S.A.; Seale, A.N.; Chaudhari, M.; Khan, N.E.; Jones, T.J.; Stumper, O.; Botha, P. Pulmonary artery banding: Still a role for staged bi-ventricular repair of intracardiac shunts? Cardiol. Young 2022, 14, 1–7. [Google Scholar] [CrossRef]
- Agasthi, P.; Graziano, J.N. Pulmonary Artery Banding. 1 October 2022. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Rao, P.S. Single ventricle—A comprehensive review. Children 2021, 8, 441. [Google Scholar] [CrossRef] [PubMed]
- Bando, K.; Turrentine, M.W.; Ensing, G.J.; Sun, K.; Sharp, T.G.; Sekine, Y.; Girod, D.A.; Brown, J.W. Surgical treatment of total anomalous pulmonary venous connection. Circulation 1996, 94 (Suppl. SII), 12–16. [Google Scholar]
- Whitfield, C.K.; Rao, P.S. Total anomalous pulmonary venous connection in the neonate. Neonatol. Today 2013, 8, 1–7. [Google Scholar]
- Spigel, Z.A.; Edmunds, E.E.; Caldarone, C.A.; Hickey, E.J.; Binsalamah, Z.M.; Heinle, J.S. Total anomalous pulmonary venous connection: Influence of heterotaxy and venous obstruction on outcomes. J. Thorac. Cardiovasc. Surg. 2022, 163, 387–395.e3. [Google Scholar] [CrossRef] [PubMed]
- Cervantes-Salazar, J.L.; Calderón-Colmenero, J.; Martínez-Guzmán, A.; García-Montes, J.A.; Rivera-Buendía, F.; Ortega-Zhindón, D.B. Total anomalous pulmonary venous connection: 16 years of surgical results in a single center. J. Card. Surg. 2022, 37, 2980–2987. [Google Scholar] [CrossRef]
- Rao, P.S. Role of balloon pulmonary valvuloplasty in the management of pulmonary stenosis. J. Clin. Cardiol. Cardiovasc. Interv. 2021, 4, 1–41. [Google Scholar] [CrossRef]
- Yerram, S.; Aramalla, S.; Bhyravavajhala, S. Unconventional deployment of atrial septal occluder in a patient with atrial septal defect, dextrocardia, and interrupted inferior vena cava. Cardiol. Young 2020, 30, 1206–1208. [Google Scholar] [CrossRef]
- Hakim, F.; Madani, A.; Samara, Y.; Ata, I.A.; Hiari, A.; Goussous, Y.; Hijazi, Z.M. Transcatheter closure of secundum atrial septal defect in a patient with dextrocardia using the Amplatzer septal occluder. Catheter. Cardiovasc. Diagn. 1998, 43, 291–294. [Google Scholar] [CrossRef]
- Galal, M.O.; Khan, M.A.; El-Segaier, M. Percutaneous closure of atrial septal defect with situs solitus and dextrocardia. Asian Cardiovasc. Thorac. Ann. 2015, 23, 202–205. [Google Scholar] [CrossRef]
- Bafna, A.; Deokate, V. Percutaneous atrial septal defect closure in a case of Poland syndrome with dextrocardia: ASD closure in Poland syndrome with dextrocardia. AsiaIntervention 2022, 8, 56–57. [Google Scholar] [CrossRef]
- Aristizábal-Villa, G.J.; Plata-Marriaga, A.E.; Torres-Nieto, M.L. Percutaneous closure of interventricular septal defect in a pediatric patient with dextrocardia. Clinical case report. Arch. Cardiol. Mex. 2022, 92, 289–291. [Google Scholar] [CrossRef]
- Yücel, İ.K.; Aslan Çınar, A.; Sürücü, M.; Çelebi, A. Successful transjugular percutaneous atrial septal defect closure in a dextrocardia patient with Kartagener’s syndrome, situs inversus, interrupted inferior vena cava, and bilateral superior vena cava. Anatol. J. Cardiol. 2023, 27, 47–49. [Google Scholar] [CrossRef]
- Yarrabolu, T.R.; Thapar, M.K.; Rao, P.S. Subpulmonary obstruction due to aneurysmal ventricular septum in a patient with congenitally corrected transposition of the great arteries and dextrocardia. Congenit. Cardiol. Today 2014, 12, 590–592. [Google Scholar]
- Nathan, M.; Liu, H.; Pigula, F.A.; Fynn-Thompson, F.; Emani, S.; Baird, C.A.; Marx, G.; Mayer, J.E.; Del Nido, P.J. Biventricular conversion after single-ventricle palliation in unbalanced atrioventricular canal defects. Ann. Thorac. Surg. 2013, 95, 2086–2095; discussion 2095–2096. [Google Scholar] [CrossRef]
- Emani, S.M.; McElhinney, D.B.; Tworetzky, W.; Myers, P.O.; Schroeder, B.; Zurakowski, D.; Pigula, F.A.; Marx, G.R.; Lock, J.E.; del Nido, P.J. Staged left ventricular recruitment after single-ventricle palliation in patients with borderline left heart hypoplasia. J. Am. Coll. Cardiol. 2012, 60, 1966–1974. [Google Scholar] [CrossRef]
- Kalish, B.T.; Banka, P.; Lafranchi, T.; Tworetzky, W.; Del Nido, P.; Emani, S.M. Biventricular conversion after single ventricle palliation in patients with small left heart structures: Short-term outcomes. Ann. Thorac. Surg. 2013, 96, 1406–1412. [Google Scholar] [CrossRef]
- Buratto, E.; Ye, X.T.; King, G.; Shi, W.Y.; Weintraub, R.G.; d’Udekem, Y.; Brizard, C.P.; Konstantinov, I.E. Long-term outcomes of single-ventricle palliation for unbalanced atrioventricular septal defects: Fontan survivors do better than previously thought. J. Thorac. Cardiovasc. Surg. 2017, 153, 430–438. [Google Scholar] [CrossRef]
- Fontan, F.; Baudet, E. Surgical repair of tricuspid atresia. Thorax 1971, 26, 240–248. [Google Scholar] [CrossRef]
- Kreutzer, G.; Galíndez, E.; Bono, H. Una operacion para la correccion de la atresia tricuspidea. In Proceedings of the Ninth Argentinean Congress of Cardiology, Buenos Aires, Argentina, 31 October–6 November 1971. [Google Scholar]
- Lee, M.; Shahjehan, R.D. Fontan completion. 26 September 2022. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Polat, A.B.; Ertürk, M.; Uzunhan, O.; Karademir, N.; Öztarhan, K. 27 years of experience with the Fontan procedure: Characteristics and clinical outcomes of children in a tertiary referral hospital. J. Cardiothorac. Surg. 2023, 18, 38. [Google Scholar] [CrossRef]
- de Leval, M.R.; Kilner, P.; Gewillig, M.; Bull, C.; McGoon, D.C. Total cavopulmonary connection: A logical alternative to atriopulmonary connection for complex Fontan operation. J. Thorac. Cardiovasc. Surg. 1988, 96, 682–695. [Google Scholar] [CrossRef]
- Pridjian, A.K.; Mendelsohn, A.M.; Lupinetti, F.M.; Beekman, R.H., III; Dick, M., II; Serwer, G.; Bove, E.L. Usefulness of the bidirectional Glenn procedure as staged reconstruction for the functional single ventricle. Am. J. Cardiol. 1993, 71, 959–962. [Google Scholar] [CrossRef] [PubMed]
- Marcelletti, C.; Corno, A.; Giannico, S.; Marino, B. Inferior vena cava-pulmonary artery extra-cardiac conduit. A new form of right heart bypass. J. Thorac. Cardiovasc. Surg. 1990, 100, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Marcelletti, C.; Iorio, F.S.; Abella, R.F. Late results of extra-cardiac Fontan repair. Semin. Thorac. Cardiovasc. Surg. Pediatr. Card. Surg. Annu. 1999, 2, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Billingsley, A.M.; Laks, H.; Boyce, S.W.; George, B.; Santulli, T.; Williams, R.G. Definitive repair in patients with pulmonary atresia and intact ventricular septum. J. Thorac. Cardiovasc. Surg. 1989, 97, 746–754. [Google Scholar] [CrossRef] [PubMed]
- Bridges, N.D.; Lock, J.E.; Castaneda, A.R. Baffle fenestration with subsequent transcatheter closure. Modification of the Fontan operation for patients at increased risk. Circulation 1990, 82, 1681–1689. [Google Scholar] [CrossRef]
- Laks, H.; Pearl, J.M.; Haas, G.S.; Drinkwater, D.C.; Milgalter, E.; Jarmakani, J.M.; Isabel-Jones, J.; George, B.L.; Williams, R.G. Partial Fontan: Advantages of an adjustable interatrial communication. Ann. Thorac. Surg. 1991, 52, 1084–1094; discussion 1094–1095. [Google Scholar] [CrossRef]
- Rao, P.S.; Chandar, J.S.; Sideris, E.B. Role of inverted buttoned device in transcatheter occlusion of atrial septal defects or patent foramen ovale with right-to-left shunting associated with previously operated complex congenital cardiac anomalies. Am. J. Cardiol. 1997, 80, 914–921. [Google Scholar] [CrossRef]
- Goff, D.A.; Blume, E.D.; Gauvreau, K.; Mayer, J.E.; Lock, J.E.; Jenkins, K.J. Clinical outcome of fenestrated Fontan patients after closure: The first 10 years. Circulation 2000, 102, 2094–2099. [Google Scholar] [CrossRef]
- Boudjemline, Y.; Bonnet, D.; Sidi, D.; Agnoletti, G. Closure of extracardiac Fontan fenestration by using the Amplatzer duct occluder. Arch. Mal. Du Coeur Vaiss. 2005, 98, 449–454. [Google Scholar]
- Rothman, A.; Evans, W.N.; Mayman, G.A. Percutaneous fenestration closure with problematic residual native atrial septum. Catheter. Cardiovasc. Interv. 2005, 66, 286–290. [Google Scholar] [CrossRef]
- Azzolina, G.; Eufrate, S.; Pensa, P. Tricuspid atresia: Experience in surgical management with a modified cavopulmonary anastomosis. Thorax 1972, 27, 111–115. [Google Scholar] [CrossRef]
- Kawashima, Y.; Kitamura, S.; Matsuda, H.; Shimazaki, Y.; Nakano, S.; Hirose, H. Total cavopulmonary shunt operation in complex cardiac anomalies. J. Thorac. Cardiovasc. Surg. 1984, 87, 74–81. [Google Scholar] [CrossRef]
- Hopkins, R.A.; Armstrong, S.E.; Serwer, G.A.; Peterson, R.J.; Oldham, H.N., Jr. Physiologic rationale for a bidirectional cavopulmonary shunt: A versatile complement to the Fontan principle. J. Thorac. Cardiovasc. Surg. 1985, 90, 391–398. [Google Scholar] [CrossRef]
- Naik, R.B.; Srivastava, C.P.; Arsiwala, S.; Mathur, A.; Sharma, S. Early outcomes after the on pump bidirectional Glenn procedure: A single center experience. J. Card. Surg. 2021, 36, 3207–3214. [Google Scholar] [CrossRef]
- Imai, K.; Hoashi, T.; Okuda, N.; Ohuchi, H.; Kurosaki, K.; Ichikawa, H. Impact of bilateral bidirectional Glenn anastomosis on staged Fontan strategy and Fontan circulation. Eur. J. Cardiothorac. Surg. 2021, 60, 930–938. [Google Scholar] [CrossRef]
- Salik, I.; Mehta, B.; Ambati, S. Bidirectional Glenn Procedure or Hemi-Fontan. 26 September 2022. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Rao, P.S. Fontan operation: Indications, short- and long-term outcomes. Indian J. Pediatr. 2015, 82, 1147–1156. [Google Scholar] [CrossRef]
- Waldman, J.D.; Rosenthal, A.; Smith, A.L.; Shurin, S.; Nadas, A.S. Sepsis and congenital asplenia. J. Pediatr. 1977, 90, 555–559. [Google Scholar] [CrossRef]
- Wang, J.K.; Hsieh, K.H. Immunologic study of the asplenia syndrome. Pediatr. Infect. Dis. J. 1991, 10, 819–822. [Google Scholar] [CrossRef]
- Sharma, M.S.; Guleserian, K.J.; Forbess, J.M. Ladd’s procedure in functional single ventricle and heterotaxy syndrome: Does timing affect outcome? Ann. Thorac. Surg. 2013, 95, 1403–1407; discussion 1407–1408. [Google Scholar] [CrossRef]
- Arnaud, A.P.; Suply, E.; Eaton, S.; Blackburn, S.C.; Giuliani, S.; Curry, J.I.; Cross, K.M.; De Coppi, P. Laparoscopic Ladd’s procedure for malrotation in infants and children is still a controversial approach. J. Pediatr. Surg. 2019, 54, 1843–1847. [Google Scholar] [CrossRef]
- Yarrabolu, T.R.; Douglas, W.I. Single ventricle physiology. In A Multidisciplinary Approach to Perinatal Cardiology; Rao, P.S., Vidyasagar, D., Eds.; Cambridge Scholars Publishing: New Castle upon Tyne, UK, 2021; Volume 2, pp. 616–645. [Google Scholar]
- Bartram, U.; Grunenfelder, J.; Van Praagh, R. Causes of death after the modified Norwood procedure: A study of 122 postmortem cases. Ann. Thorac. Surg. 1997, 64, 1795–1802. [Google Scholar] [CrossRef] [PubMed]
- Tweddell, J.S.; Hoffman, G.M.; Mussatto, K.A.; Fedderly, R.T.; Berger, S.; Jaquiss, R.D.; Ghanayem, N.S.; Frisbee, S.J.; Bert Litwin, S. Improved survival of patients undergoing palliation of hypoplastic left heart syndrome: Lessons learned from 115 consecutive patients. Circulation 2002, 106, 82–89. [Google Scholar] [CrossRef]
- Cashen, K.; Gupta, P.; Lieh-Lai, M.; Mastropietro, C. Infants with single ventricle physiology in the emergency department: Are physicians prepared? J. Pediatr. 2011, 159, 273–277.e1. [Google Scholar] [CrossRef]
- Yates, M.C.; Rao, P.S. Pediatric cardiac emergencies. Emerg. Med. 2013, 3, 164. [Google Scholar] [CrossRef]
- Rao, P.S. Fontan operation: A comprehensive review. In Fontan Surgery; Khan, I., Ed.; InTechOpen: Rijeka, Croatia, 2020. [Google Scholar] [CrossRef]
- Rao, P.S.; Pediatric Tricuspid Atresia. Medscape Drugs & Diseases. Updated 17 January 2017. Available online: http://emedicine.medscape.com/article/900832-overview (accessed on 29 July 2022).
- Rao, P.S. Protein-losing enteropathy following the Fontan operation (editorial). J. Invasive Cardiol. 2007, 19, 447–448. [Google Scholar]
- Rao, P.S. What an adult cardiologist should know about cyanotic congenital heart disease? J. Cardiovasc. Dis. Diagn. 2013, 1, 104. [Google Scholar] [CrossRef]
- Toselli, M.; Solinas, E.; Vignali, L. Percutaneous coronary intervention in dextrocardia: A case report and a brief review of the literature. J. Cardiovasc. Med. 2020, 21, 613–615. [Google Scholar] [CrossRef]
- Marsden, G.; Folk, J.; Rosenberg, J. An ST-elevation myocardial infarction in situs inversus totalis (DEXTROCARDIA). J. Emerg. Med. 2020, 59, 597–599. [Google Scholar] [CrossRef]
- Elliott, S.; Levy, D.; Brown, H. ST-elevation myocardial infarction in a patient having dextrocardia with situs inversus. J. Emerg. Med. 2020, 58, 797–801. [Google Scholar] [CrossRef]
- Winter, J.L. Recognition of anterior STEMI in dextrocardia and the importance of right-sided chest leads. JACC Case Rep. 2020, 2, 1222–1226. [Google Scholar] [CrossRef]
- Yoo, M.J.; Bridwell, R.E.; Oliver, J.J. Acute coronary syndrome in dextrocardia. Am. J. Emerg. Med. 2021, 42, 262.e1–262.e2. [Google Scholar] [CrossRef]
- Yamazaki, T.; Tomaru, A.; Wagatsuma, K.; Kudo, M.; Baba, J.; Takikawa, K.; Miho, O.; Yoshikawa, M. Percutaneous transluminal coronary angioplasty for morphologic left anterior descending artery lesion in a patient with dextrocardia. A case report and literature review. Angiology 1997, 48, 451–456. [Google Scholar] [CrossRef]
- Khalil, S.; Kamal, A.; Ahmed, S. Acute myocardial infarction in a patient with dextrocardia and situs inversus. J. Electrocardiol. 2005, 38, 412–413. [Google Scholar] [CrossRef]
- Bariş, N.; Kirimli, O.; Ozpelit, E.; Akdeniz, B. Right coronary artery intervention with mirror image in a patient with dextrocardia. Anadolu Kardiyol. Derg. 2005, 5, 340–341. [Google Scholar]
- Wild, J.; Gori, T.; Münzel, T.; Wenzel, P. Successful percutaneous coronary intervention for an in-stent chronic total occlusion in a patient with dextrocardia: A case report. BMC Cardiovasc. Disord. 2017, 17, 281. [Google Scholar] [CrossRef]
- Kong, B.; Wang, N.; Dou, L.; Cao, D. Coronary angioplasty in an adult with dextrocardia and single coronary artery with the right coronary artery originating from the left anterior descending artery. Coron. Artery Dis. 2019, 30, 390–392. [Google Scholar] [CrossRef]
- Siraj, M.M.; Khondokar, N.N.; Alam, K.; Talukder, A.; Khanal, A.; Habib, S.A.; Shakil, S.S.; Rahman, F. Successful multi-vessel percutaneous coronary intervention for recent myocardial infarction in a patient with dextrocardia and situs inversus. Mymensingh Med. J. 2020, 29, 464–468. [Google Scholar]
- Koga, M.; Sugimoto, A.; Ito, D.; Hoshiba, Y.; Aizawa, T.; Iseki, H. Percutaneous coronary intervention for left main coronary artery stenosis in a patient with dextrocardia. Cardiovasc. Interv. Ther. 2020, 35, 300–301. [Google Scholar] [CrossRef]
- Vijayvergiya, R.; Gawalkar, A.A.; Kasinadhuni, G.; Kaushal, S.; Batta, A.; Kumar, B. Percutaneous coronary intervention in dextrocardia patients with situs inversus. AsiaIntervention 2022, 8, 132–135. [Google Scholar] [CrossRef]
- Ravikumar, M.S.; Palanisamy, V.; Tamilselvan, M.; Sangili, S.; Sethuratnam, R. Technical aspects: Coronary artery bypass grafting in a case of dextrocardia with situs inversus. Cureus 2021, 13, e14932. [Google Scholar] [CrossRef]
- Sinner, G.J.; George, B.; Messerli, A.W. Transradial approach to coronary angiography and percutaneous intervention in patients with dextrocardia. J. Invasive Cardiol. 2019, 31, E83–E88. [Google Scholar] [PubMed]
- Bhambhani, A.; Joshi, A. Transradial coronary intervention in chronic total occlusion in a patient with mirror image dextrocardia. Cureus 2021, 13, e13991. [Google Scholar] [CrossRef] [PubMed]
- Soneji, N.; Mohammad, K.; Heinzman, K. A rare case of superior approach for fluoroless atrial flutter ablation in a patient with dextrocardia, situs inversus, and interruption of the inferior vena cava. HeartRhythm Case Rep. 2022, 8, 335–338. [Google Scholar] [CrossRef] [PubMed]
- Meulet, J.; Trim, G.; Hunt, B.; Lim, K.T.; James, A.; Henry, A.; Pirihi, W.; Davies, P.; Brabant, J. Radiofrequency pulmonary vein isolation in a patient with dextrocardia with situs inversus totalis. Heart Lung Circ. 2017, 26, e33–e36. [Google Scholar] [CrossRef] [PubMed]
- Yamada, T.; McElderry, H.T.; Doppalapudi, H.; Platonov, M.; Epstein, A.E.; Plumb, V.J.; Kay, G.N. Successful catheter ablation of atrial fibrillation in a patient with dextrocardia. Europace 2008, 10, 1120–1122. [Google Scholar] [CrossRef]
- Ulus, T.; Dural, M.; Şener, E.; Al, A.; Mert, K.U.; Görenek, B. Atrial fibrillation and atrial flutter ablation using mirror image in a patient with dextrocardia with situs inversus. Anatol. J. Cardiol. 2020, 24, 282–284. [Google Scholar] [CrossRef]
- Kohli, U.; Hassan, S. Dextrocardia and atrial fibrillation ablation: Relevance of anatomy. J. Interv. Card. Electrophysiol. 2021, 60, 155–157. [Google Scholar] [CrossRef]
- Zhao, X.; Su, X.; Long, D.Y.; Sang, C.H.; Bai, R.; Tang, R.B.; Liu, N.; Jiang, C.X.; Li, S.N.; Guo, X.Y.; et al. Catheter ablation of atrial fibrillation in situs inversus dextrocardia: Challenge, improved procedure, outcomes, and literature review. Pacing Clin. Electrophysiol. 2021, 44, 293–305. [Google Scholar] [CrossRef]
- Hu, X.; Wu, S.; Qin, M.; Jiang, W.; Liu, X. Radiofrequency ablation for paroxysmal atrial fibrillation in a patient with dextrocardia and interruption of the inferior vena cava: A case report. Eur. Heart J. 2021, 5, ytab191. [Google Scholar] [CrossRef]
- Masumoto, A.; Kobori, A.; Sasaki, Y.; Pak, M.; Furukawa, Y. Successful catheter ablation of persistent atrial fibrillation and common atrial flutter in a patient with dextrocardia, situs inversus, and interrupted inferior vena cava with azygos continuation. HeartRhythm Case Rep. 2021, 7, 403–407. [Google Scholar] [CrossRef]
- Zhou, G.B.; Ma, J.; Zhang, J.L.; Guo, X.G.; Yang, J.D.; Liu, S.W.; Ouyang, F.F. Catheter ablation of supraventricular tachycardia in patients with dextrocardia and situs inversus. J. Cardiovasc. Electrophysiol. 2019, 30, 557–564. [Google Scholar] [CrossRef]
- Zheng, Z.; Zeng, Z.; Zhou, Y.; Li, C.; Zhang, W. Radiofrequency catheter ablation in a patient with dextrocardia, persistent left superior vena cava, and atrioventricular nodal reentrant tachycardia: A case report. Medicine 2020, 99, e22086. [Google Scholar] [CrossRef]
- Zhang, Y.; Sun, L.; Luo, F.; Li, J.; Sun, Y.; Chen, Y.; Dong, J. Result and technique consideration of radiofrequency catheter ablation of tachycardia in patients with dextrocardia. Pacing Clin. Electrophysiol. 2022, 45, 340–347. [Google Scholar] [CrossRef]
- Zhao, L.; Li, R.; Bai, L.; Wang, D.; Zhang, J.; Yang, X. Successful radiofrequency catheter ablation of Wolff-Parkinson-White syndrome in a patient with dextrocardia: A case report. Front. Cardiovasc. Med. 2022, 9, 1006435. [Google Scholar] [CrossRef]
- Song, L.; Fan, C.; Zhang, H.; Liu, H.; Iroegbu, C.D.; Luo, C.; Liu, L. Case Report: The Cox-Maze IV procedure in the mirror: The use of three-dimensional printing for pre-operative planning in a patient with situs inversus dextrocardia. Front. Cardiovasc. Med. 2021, 8, 722413. [Google Scholar] [CrossRef]
- Luo, C.; Fan, C.; Zhang, H.; Song, L.; Liu, Y.; Liu, L. Cox-Maze IV procedure concomitant with valvular surgery in situs inversus dextrocardia: A single-center experience in China. J. Vis. Exp. 2022, 180. [Google Scholar] [CrossRef]
- Augusto, J.B.; Faustino, M.; Santos, M.B.; Cabanelas, N.; Madeira, F.; Morais, C. Implantation of a dual-chamber pacemaker in a patient with situs inversus and dextrocardia using a novel ultrasound technique. J. Cardiovasc. Echogr. 2019, 29, 129–131. [Google Scholar] [CrossRef]
- Hakimi, M.; Yabumoto, M.; Sun, J.; Rochon-Duck, M.; Donaldson, D. Implantation of a dual-chamber pacemaker in a patient with dextrocardia, situs inversus, and sick sinus syndrome. Innov. Card. Rhythm. Manag. 2022, 13, 4889–4893. [Google Scholar] [CrossRef]
- Luo, J.; Zhou, Z.; Chen, K.; Lin, J.; Cai, C.; Zeng, Z. Implantation of a dual-chamber pacemaker in a patient with dextrocardia and sick sinus syndrome: A case report. J. Int. Med. Res. 2022, 50, 3000605221088551. [Google Scholar] [CrossRef]
- Aizawa, Y.; Ichiki, T.; Yoshizawa, A.; Monma, Y.; Nakayama, T.; Kato, T.S.; Inami, S.; Fujimoto, Y.; Kawamura, A. Successful leadless pacemaker implantation in an elderly patient with dextrocardia and situs inversus. Cureus 2021, 13, e17858. [Google Scholar] [CrossRef]
- Bontempi, L.; Fundaliotis, A.; Moretti, M.; Sammartino, A.M.; Saino, A.T.; Arabia, G.; Pitì, A.; Curnis, A.; Dell’Aquila, A. Leadless pacemaker implantation in dextrocardia with situs viscerum inversus: A case report and literature review. Pacing Clin. Electrophysiol. 2023, 46, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.J.; Cheng, Y.T.; Li, C.H.; Weng, C.J.; Hsieh, Y.C.; Chen, S.A. Leadless pacemaker implantation in a patient with dextrocardia and situs inversus: Tips and tricks. Acta Cardiol. Sin. 2022, 38, 103–105. [Google Scholar] [CrossRef] [PubMed]
- Ceresnak, S.R.; Motonaga, K.S.; Rogers, I.S.; Viswanathan, M.N. Right-sided subcutaneous implantable cardioverter-defibrillator placement in a patient with dextrocardia, tetralogy of Fallot, and conduction disease. HeartRhythm Case Rep. 2015, 1, 186–189. [Google Scholar] [CrossRef] [PubMed]
- González-Cordero, A.; López-Puebla, J.; Franqui-Rivera, H. Implantation of a completely right sided subcutaneous cardioverter-defibrillator in a patient with situs inversus dextrocardia. Indian Pacing Electrophysiol. J. 2019, 19, 72–74. [Google Scholar] [CrossRef] [PubMed]
- Al-Ghamdi, B. Right-sided subcutaneous implantable cardioverter defibrillator system implantation in a patient with complex congenital heart disease and dextrocardia: A case report and literature review. Case Rep. Cardiol. 2019, 2019, 3907190. [Google Scholar] [CrossRef] [PubMed]
- Lüker, J.; Padala, S.K.; Cano, Ó.; Beiert, T.; Osswald, B.; Koneru, J.N.; Schrickel, J.W.; Kron, J.; Franqui-Rivera, H.; Gonzalez-Cordero, A.; et al. Multicenter experience of subcutaneous implantable cardioverter-defibrillator therapy in patients with dextrocardia. JACC Clin. Electrophysiol. 2019, 5, 1226–1228. [Google Scholar] [CrossRef]
- Wiedmann, F.; De Simone, R.; Rose, P.; Karck, M.; Gorenflo, M.; Frey, N.; Schmidt, C. Case report of an S-ICD implantation for secondary prevention in a patient with complex congenital heart disease, dextrocardia, and situs solitus. Eur. Heart J. Case Rep. 2022, 6, ytac253. [Google Scholar] [CrossRef]
- Lador, A.; Patel, A.; Valderrábano, M. Trans-coronary sinus puncture for catheter ablation and left atrial appendage closure device implantation in a patient with dextrocardia and persistent right superior vena cava. HeartRhythm Case Rep. 2020, 6, 903–906. [Google Scholar] [CrossRef]
- Xu, J.; Jiang, G.; Zhang, L.; Chen, Z.; Wang, H.; Bai, M.; Zeng, J. Successful percutaneous left atrial appendage occlusion for atrial fibrillation in a patient with mirror-image dextrocardia: A case report. BMC Cardiovasc. Disord. 2022, 22, 20. [Google Scholar] [CrossRef]
- Tian, B.; Ma, C.; Su, J.W.; Luo, J.; Sun, H.X.; Su, J.; Ning, Z.P. Left atrial appendage occlusion in a mirror image dextrocardia: A case report and review of literature. World J. Clin. Cases 2022, 10, 1357–1365. [Google Scholar] [CrossRef]
- Morita, Y.; Okimoto, T.; Nagamoto, Y.; Mochizuki, S.; Yamada, K. Transcatheter aortic valve implantation for severe aortic stenosis in dextrocardia with situs inversus using a self-expanding aortic valve. J. Cardiol. Cases 2018, 17, 208–211. [Google Scholar] [CrossRef]
- Overtchouk, P.; Delhaye, C.; Sudre, A.; Modine, T. Successful transcatheter aortic valve implantation for severe aortic stenosis of a bicuspid valve with situs inversus totalis guided by advanced image processing: A case report. Eur. Heart J. Case Rep. 2018, 2, yty049. [Google Scholar] [CrossRef]
- Pattakos, G.; Chrissoheris, M.; Halapas, A.; Papadopoulos, K.; Kourkoveli, P.; Bouboulis, N.; Pattakos, S.; Spargias, K. Transcatheter aortic valve replacement in a patient with dextrocardia and situs inversus totalis. Ann. Thorac. Surg. 2019, 107, e33–e35. [Google Scholar] [CrossRef]
- Malasana, G.R.; Zeglin, M.; McElveen, R. Transcatheter aortic valve replacement in dextrocardia with situs inversus. JACC Case Rep. 2020, 2, 860–861. [Google Scholar] [CrossRef]
- Chen, D.Y.; Hsieh, M.J.; Chen, C.C.; Liu, Y.C.; Hsieh, I.C. Transcatheter aortic valve implantation in a patient with dextrocardia situs inversus, and functional bicuspid aortic valve stenosis. Acta Cardiol. Sin. 2021, 37, 652–656. [Google Scholar] [CrossRef]
- Aoyagi, S.; Tobinaga, S.; Wada, K.; Nata, S.I.; Yasunaga, H. Aortic valve replacement for dextrocardia with situs inversus totalis. J. Card. Surg. 2021, 36, 3378–3380. [Google Scholar] [CrossRef]
- Bhatia, I.; Chan, D.T.; Lam, S.C.; Au, T.W. Feasibility of novel transapical off pump beating heart mitral valve repair in a patient with dextrocardia and situs inversus. Eur. J. Cardiothorac. Surg. 2020, 58, 392–394. [Google Scholar] [CrossRef]
- García Vieites, M.; Martinez-Sapiña Llanas, M.J.; Gómez Zincke, M.; Bouzas Zubeldía, B.; Bautista-Hernandez, V. Mitral valve replacement via a left thoracotomy in dextrocardia and situs solitus. Asian Cardiovasc. Thorac. Ann. 2018, 26, 142–145. [Google Scholar] [CrossRef]
- Stiru, O.; Geana, R.C.; Ilie, R.R.; Chioncel, O.; Tulin, R.; Valeanu, L.; Bubenek, S.; Filipescu, D.; Iliescu, V.A. Transseptal approach for mitral valve replacement in dextrocardia with situs inversus totalis: A case report and review of the literature. Heart Surg. Forum 2020, 23, E030–E033. [Google Scholar] [CrossRef]
- Sahin, M.A.; Guler, A.; Kaya, E. Mitral valve replacement in a patient with situs inversus and dextrocardia. Thorac. Cardiovasc. Surg. 2011, 59, 305–306. [Google Scholar] [CrossRef]
- Said, S.A.; Veerbeek, A.; van der Wieken, L.R. Dextrocardia, situs inversus and severe mitral stenosis in a pregnant woman: Successful closed commissurotomy. Eur. Heart J. 1991, 12, 825–828. [Google Scholar] [PubMed]
- Raju, R.; Singh, S.; Kumar, P.; Rao, S.; Kapoor, S.; Raju, B.S. Percutaneous balloon valvuloplasty in mirror-image dextrocardia and rheumatic mitral stenosis. Catheter. Cardiovasc. Diagn. 1993, 30, 138–140. [Google Scholar] [CrossRef]
- Patel, T.M.; Dani, S.I.; Thakore, S.B.; Chaq, M.C.; Shah, S.C.; Shah, U.G.; Thomas, V.M.; Patel, T.K. Balloon mitral and aortic valvuloplasty in mirror-image dextrocardia. J. Invasive Cardiol. 1996, 8, 164–168. [Google Scholar]
- Nallet, O.; Lung, B.; Cormier, B.; Porte, J.M.; Garbarz, E.; Michel, P.L.; Vahanian, A. Specifics of technique in percutaneous mitral commissurotomy in a case of dextrocardia and situs inversus with mitral stenosis. Catheter. Cardiovasc. Diagn. 1996, 39, 85–88. [Google Scholar] [CrossRef]
- Chow, W.H.; Fan, K.; Chow, T.C. Balloon mitral commissurotomy in a patient with situs inversus and dextrocardia. J. Heart Valve Dis. 1996, 5, 307–308. [Google Scholar]
- Verma, P.K.; Bali, H.K.; Suresh, P.V.; Varma, J.S. Balloon mitral valvotomy using Inoue technique in a patient of isolated dextrocardia with rheumatic mitral stenosis. Indian Heart J. 1999, 51, 315–317. [Google Scholar]
- Namboodiri, N.; Harikrishnan, S.P.; Ajitkumar, V.; Tharakan, J.A. Percutaneous mitral commissurotomy in a case of mirror-image dextrocardia and rheumatic mitral stenosis. J. Invasive Cardiol. 2008, 20, E33–E35. [Google Scholar]
- Hussain, S.; Ahmed, W. Percutaneous transvenous mitral commissurotomy in mitral restenosis with situs inversus. J. Coll. Physicians Surg. Pak. 2009, 19, 117–119. [Google Scholar]
- Kulkarni, P.; Halkati, P.; Patted, S.; Ambar, S.; Yavagal, S. Percutaneous mitral balloon valvotomy in a case of situs inversus dextrocardia with severe rheumatic mitral stenosis. Cardiovasc. Revascularization Med. 2012, 13, 246–248. [Google Scholar] [CrossRef]
- Nivargi, V.; Makhale, C.; Kulkarni, V. Balloon mitral valvuloplasty in mirror image dextrocardia with rheumatic mitral stenosis with suprasystemic pulmonary arterial hypertension. J. Assoc. Physicians India 2019, 67, 94–95. [Google Scholar]
- Agirbasli, M.; Hamid, R.; Jennings, H.S., 3rd; Tiller, G.E. Situs inversus with hypertrophic cardiomyopathy in identical twins. Am. J. Med. Genet. 2000, 91, 327–330. [Google Scholar] [CrossRef]
- Kuznetsov, G.P.; Dupliakov, D.V.; Popova, I.V.; Avramenko, A.A.; Suslina, E.A.; Tukhbatova, A.A.; Adonina, E.V. Hypertrophic cardiomyopathy in a patient with dextrocardia. Kardiologiia 2015, 55, 92–95. [Google Scholar] [CrossRef]
- Fang, F.; Cui, F.M.; He, Y.M.; Yang, X.J.; Zhao, X.; Xu, H.F.; Yu, C.M. Dextrocardia and symmetric hypertrophic cardiomyopathy with multiple mutations of genes encoding the sarcomere proteins. Int. J. Cardiol. 2015, 187, 581–584. [Google Scholar] [CrossRef]
- Aoyama, R.; Takano, H.; Sangen, H.; Shimizu, W. Effective alcohol septal ablation for left ventricular outflow tract obstruction in a patient with isolated dextrocardia. BMJ Case Rep. 2019, 12, e231922. [Google Scholar] [CrossRef]
Figure 1.
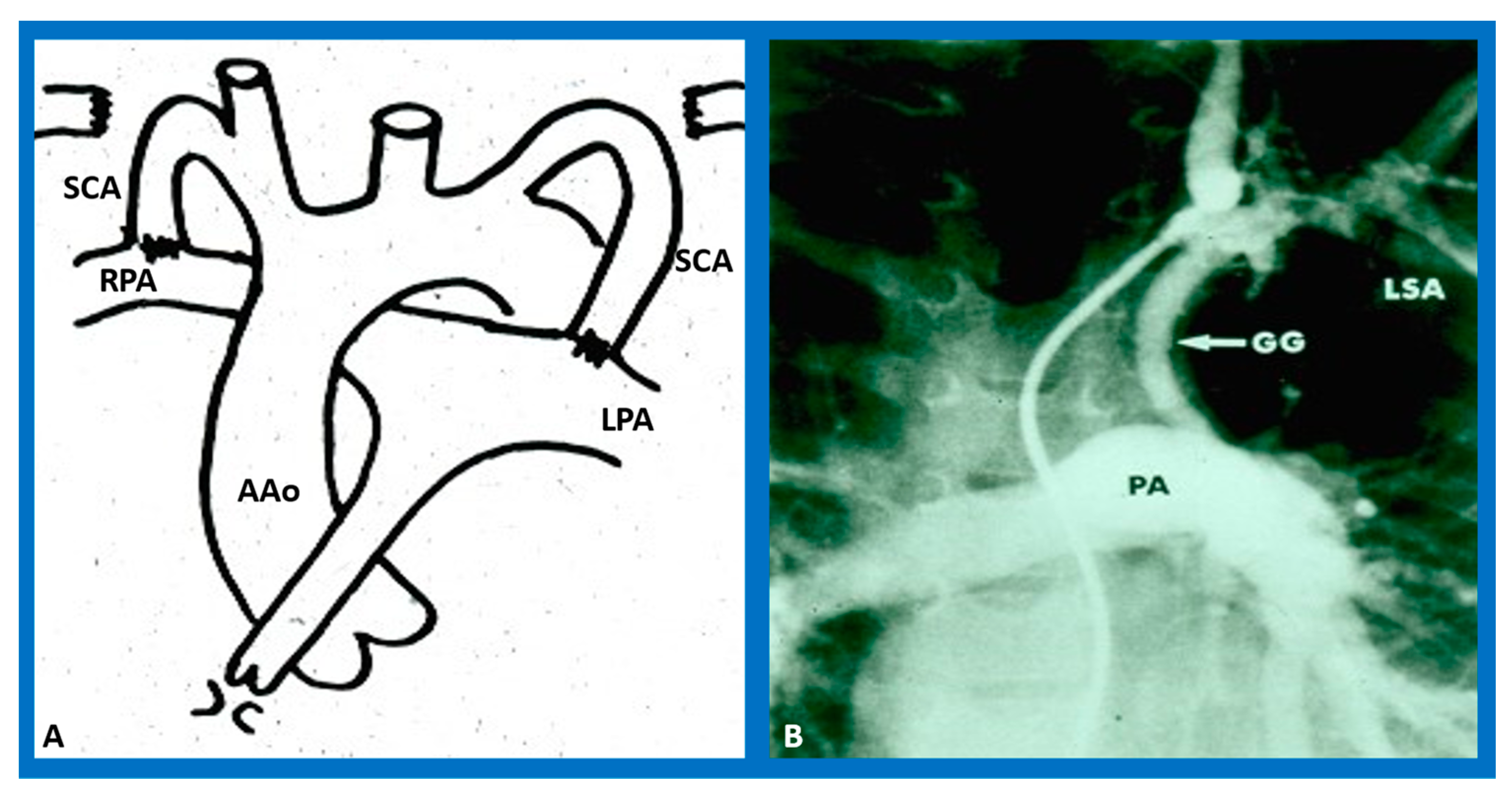
(A) The diagram drawn by hand by Dr. Taussig herself demonstrating the idea of the Blalock–Taussig shunt [9] indicating the connection of subclavian arteries (SCAs) to the right (RPA) or left (LPA) pulmonary artery, correspondingly. (B) Selected cineangiographic frame of a modified Blalock–Taussig anastomosis with a Gore-Tex graft (GG) connecting the left subclavian artery (LSA) with the pulmonary artery (PA) [10]. This figure reveals a wide-open Blalock–Taussig anastomosis and good opacification of the PA. AAo, ascending aorta. Reproduced from [20].
Figure 1.
(A) The diagram drawn by hand by Dr. Taussig herself demonstrating the idea of the Blalock–Taussig shunt [9] indicating the connection of subclavian arteries (SCAs) to the right (RPA) or left (LPA) pulmonary artery, correspondingly. (B) Selected cineangiographic frame of a modified Blalock–Taussig anastomosis with a Gore-Tex graft (GG) connecting the left subclavian artery (LSA) with the pulmonary artery (PA) [10]. This figure reveals a wide-open Blalock–Taussig anastomosis and good opacification of the PA. AAo, ascending aorta. Reproduced from [20].

Figure 2.
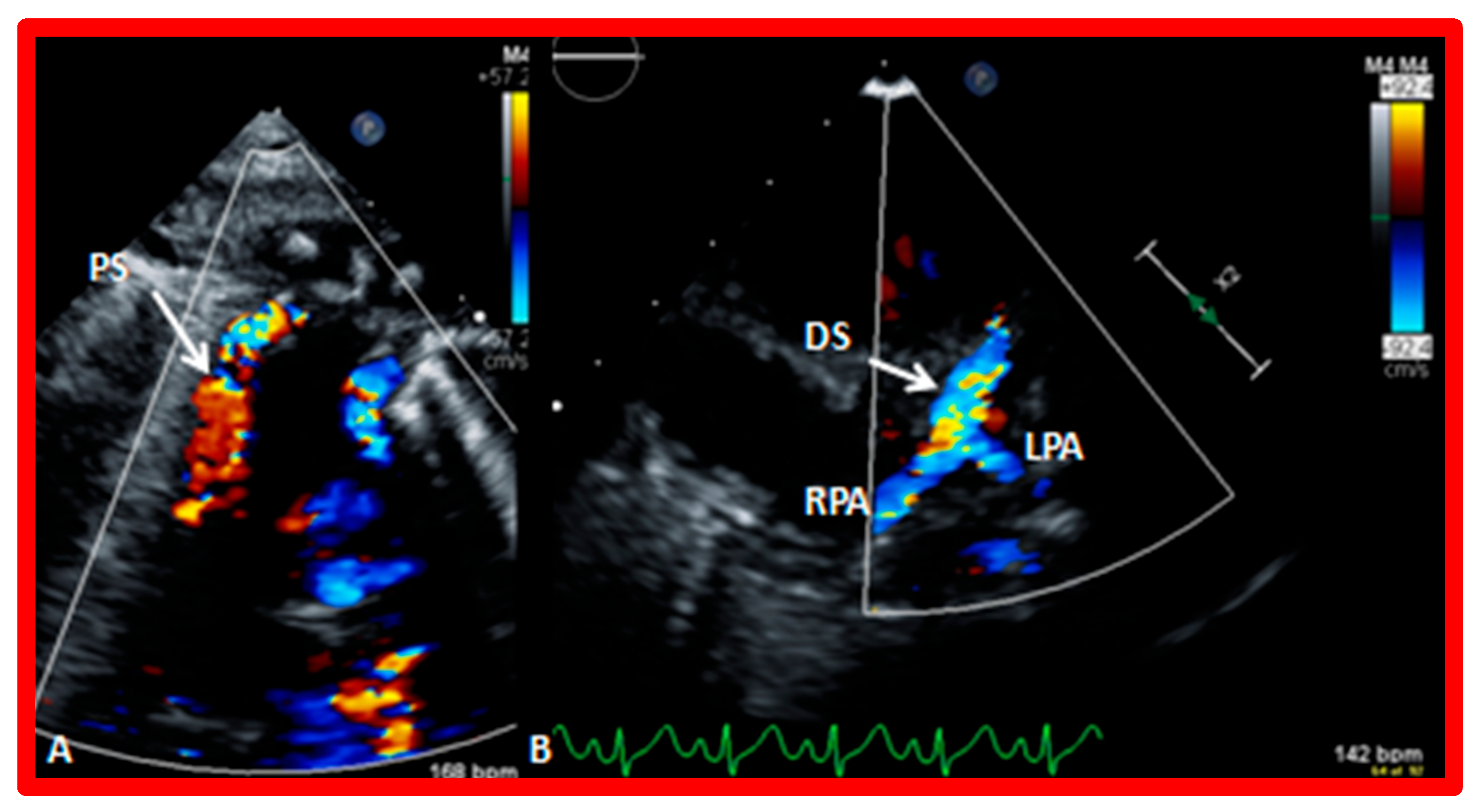
Echo–Doppler recordings acquired with a transducer positioned in the suprasternal notch view illustrating the proximal portion of the shunt (PS) by color Doppler (A). With a somewhat separate angulation (B), the distal part of the shunt (DS) is shown with flow into the right (RPA) and left (LPA) pulmonary arteries. Reproduced from [21].
Figure 2.
Echo–Doppler recordings acquired with a transducer positioned in the suprasternal notch view illustrating the proximal portion of the shunt (PS) by color Doppler (A). With a somewhat separate angulation (B), the distal part of the shunt (DS) is shown with flow into the right (RPA) and left (LPA) pulmonary arteries. Reproduced from [21].

Figure 3.
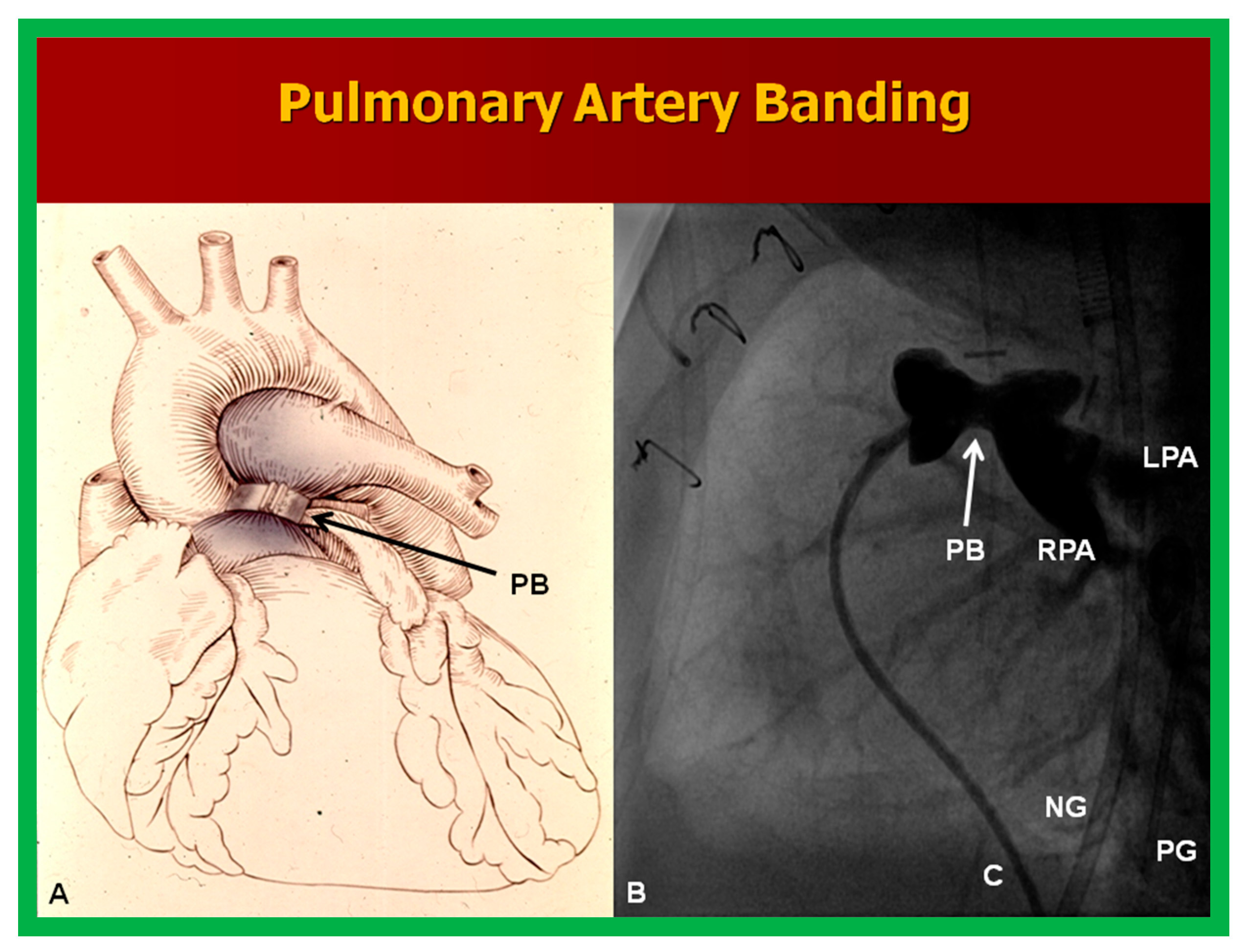
(A) A diagram illustrating pulmonary artery banding (PB) for patients with a severely increased blood flow into the pulmonary circuit and severe heart failure. (B) Cineangiographic image of the pulmonary artery angiogram in the lateral projection illustrating the narrowing of the pulmonary artery shown with an arrow in a baby who had surgical PB. Note: catheter (C); left pulmonary artery (LPA); nasogastric tube (NG); pigtail catheter (PG); and right pulmonary artery (RPA). Reproduced from [25].
Figure 3.
(A) A diagram illustrating pulmonary artery banding (PB) for patients with a severely increased blood flow into the pulmonary circuit and severe heart failure. (B) Cineangiographic image of the pulmonary artery angiogram in the lateral projection illustrating the narrowing of the pulmonary artery shown with an arrow in a baby who had surgical PB. Note: catheter (C); left pulmonary artery (LPA); nasogastric tube (NG); pigtail catheter (PG); and right pulmonary artery (RPA). Reproduced from [25].

Figure 4.
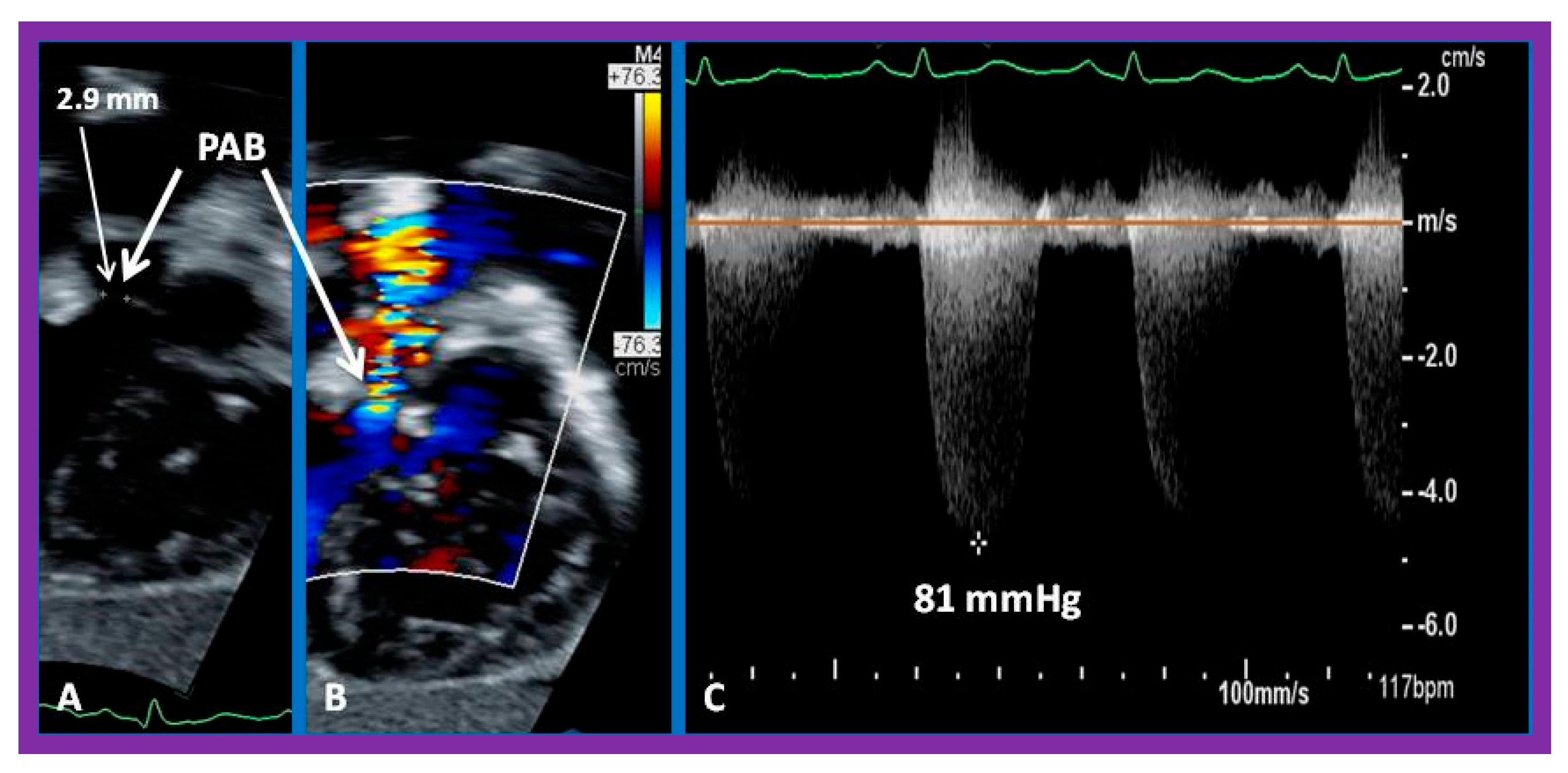
Echo–Doppler recordings demonstrating pulmonary artery banding (PAB) with a narrow two-dimensional width of 2.9 mm (A) and by color Doppler imaging (B). A significant pressure gradient of 81 mm Hg was recorded by CW Doppler (C). Reproduced from [21].
Figure 4.
Echo–Doppler recordings demonstrating pulmonary artery banding (PAB) with a narrow two-dimensional width of 2.9 mm (A) and by color Doppler imaging (B). A significant pressure gradient of 81 mm Hg was recorded by CW Doppler (C). Reproduced from [21].

Figure 5.
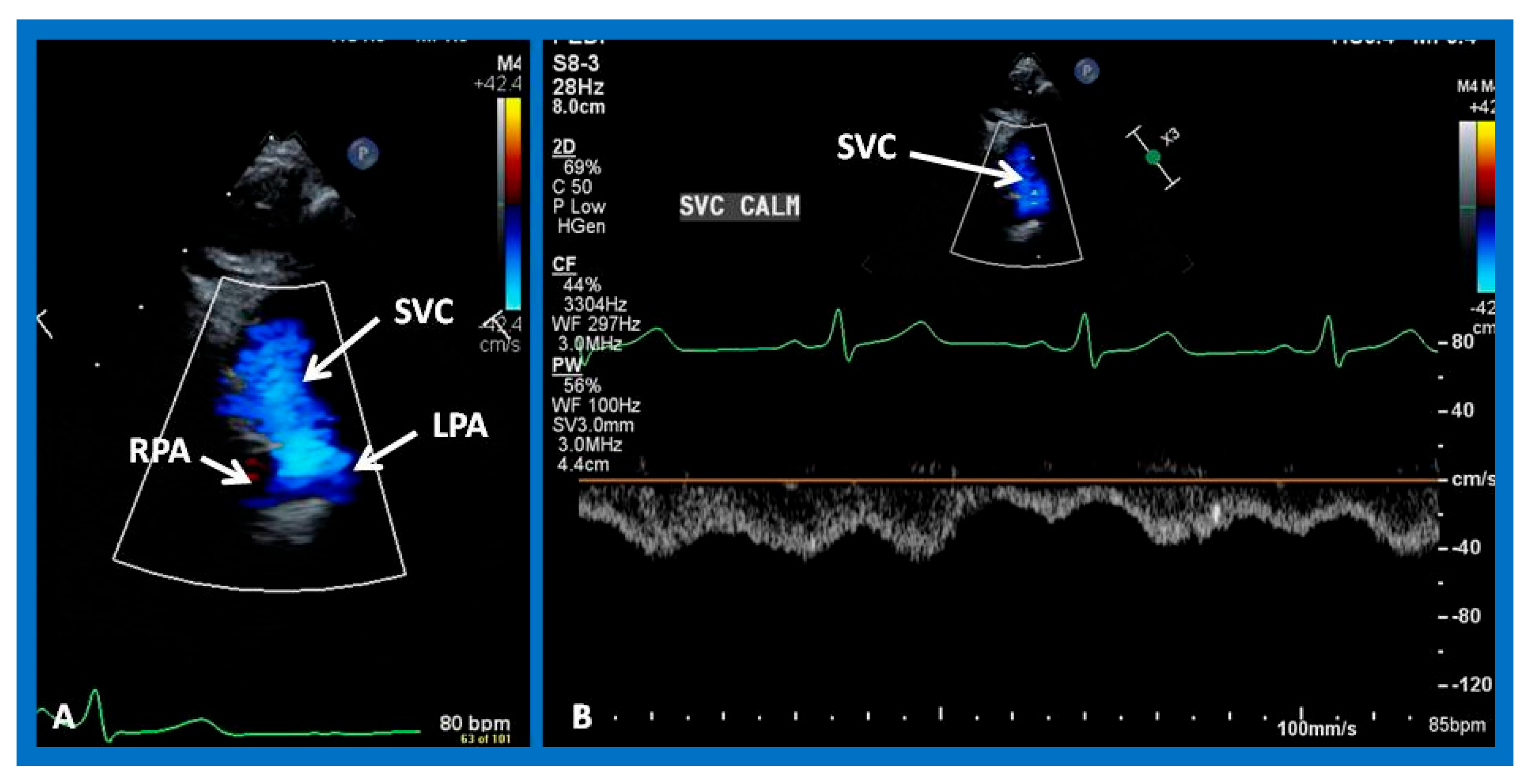
Selected video images from the suprasternal notch view demonstrating bidirectional Glenn anastomosis. The superior vena cava (SVC) emptying into the left (LPA) and right (RPA) pulmonary arteries by color flow imaging (A). Normal Doppler flow velocities across the Glenn shunt (B) suggests that the anastomotic site is not occluded. Reproduced from [21].
Figure 5.
Selected video images from the suprasternal notch view demonstrating bidirectional Glenn anastomosis. The superior vena cava (SVC) emptying into the left (LPA) and right (RPA) pulmonary arteries by color flow imaging (A). Normal Doppler flow velocities across the Glenn shunt (B) suggests that the anastomotic site is not occluded. Reproduced from [21].

Figure 6.
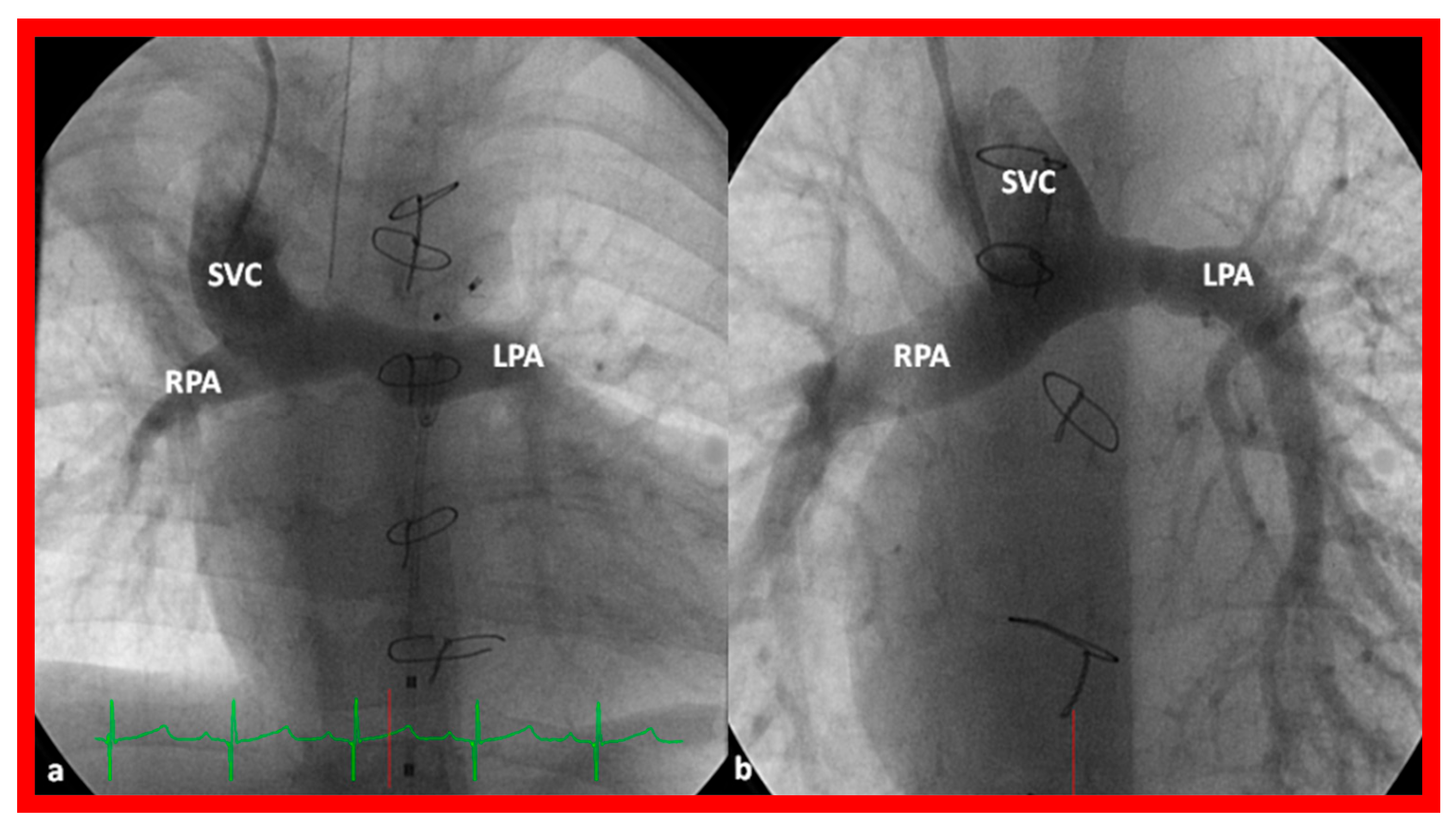
Selected cine frames demonstrating a bidirectional Glenn anastomosis in two different patients, (a,b). Unrestricted blood flow from the superior vena cava (SVC) to the left (LPA) and right (RPA) pulmonary arteries is seen. Sternal wires from a previous operation are visualized (not marked). Reproduced from [63].
Figure 6.
Selected cine frames demonstrating a bidirectional Glenn anastomosis in two different patients, (a,b). Unrestricted blood flow from the superior vena cava (SVC) to the left (LPA) and right (RPA) pulmonary arteries is seen. Sternal wires from a previous operation are visualized (not marked). Reproduced from [63].

Figure 7.
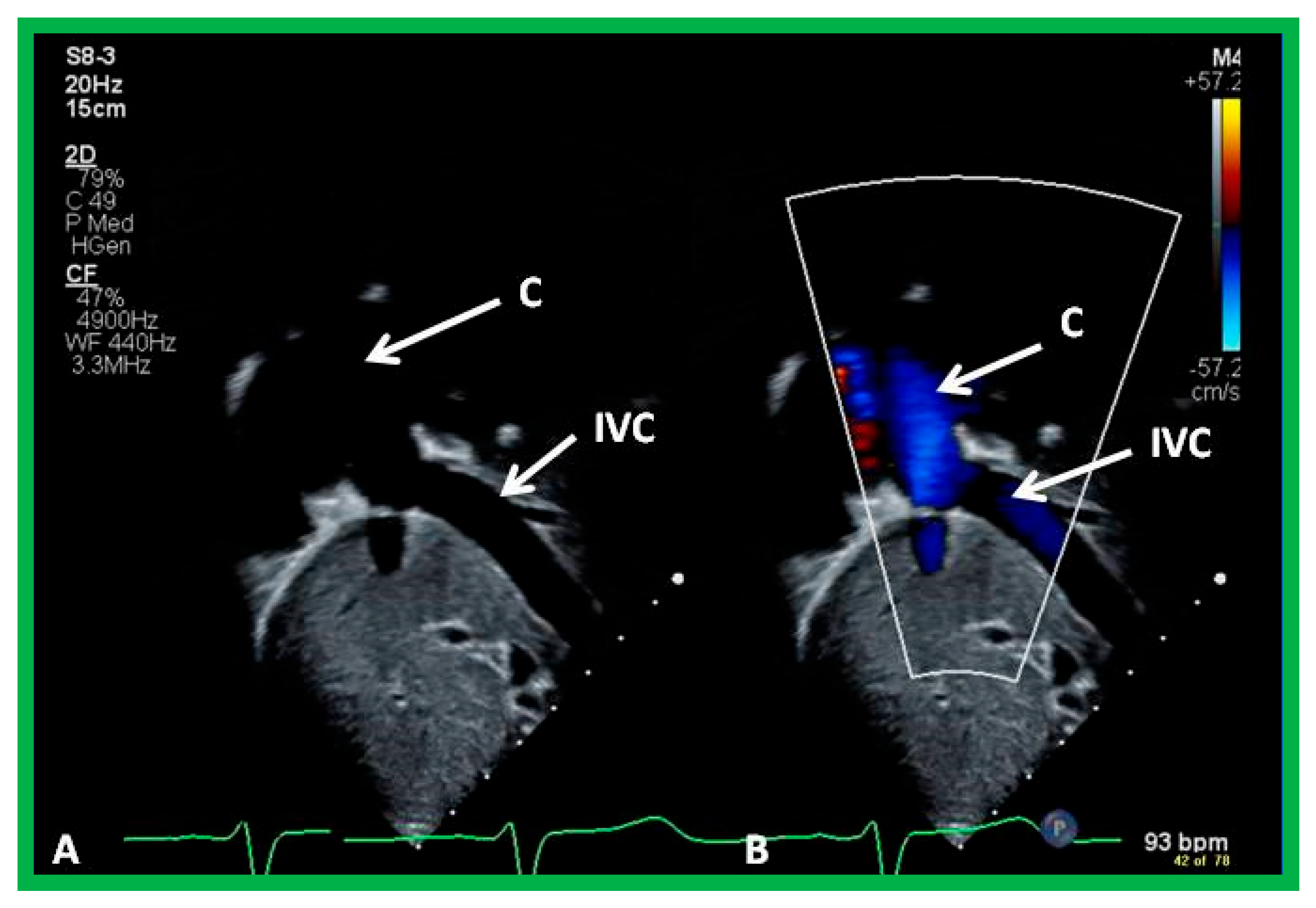
Selected video images by two-dimensional (A) and color echo–Doppler (B) illustrating anastomosis of the inferior vena cava (IVC) with a non-valved conduit (C). Note that the inferior vena cava to conduit connection is wide open. Reproduced from [21].
Figure 7.
Selected video images by two-dimensional (A) and color echo–Doppler (B) illustrating anastomosis of the inferior vena cava (IVC) with a non-valved conduit (C). Note that the inferior vena cava to conduit connection is wide open. Reproduced from [21].

Figure 8.
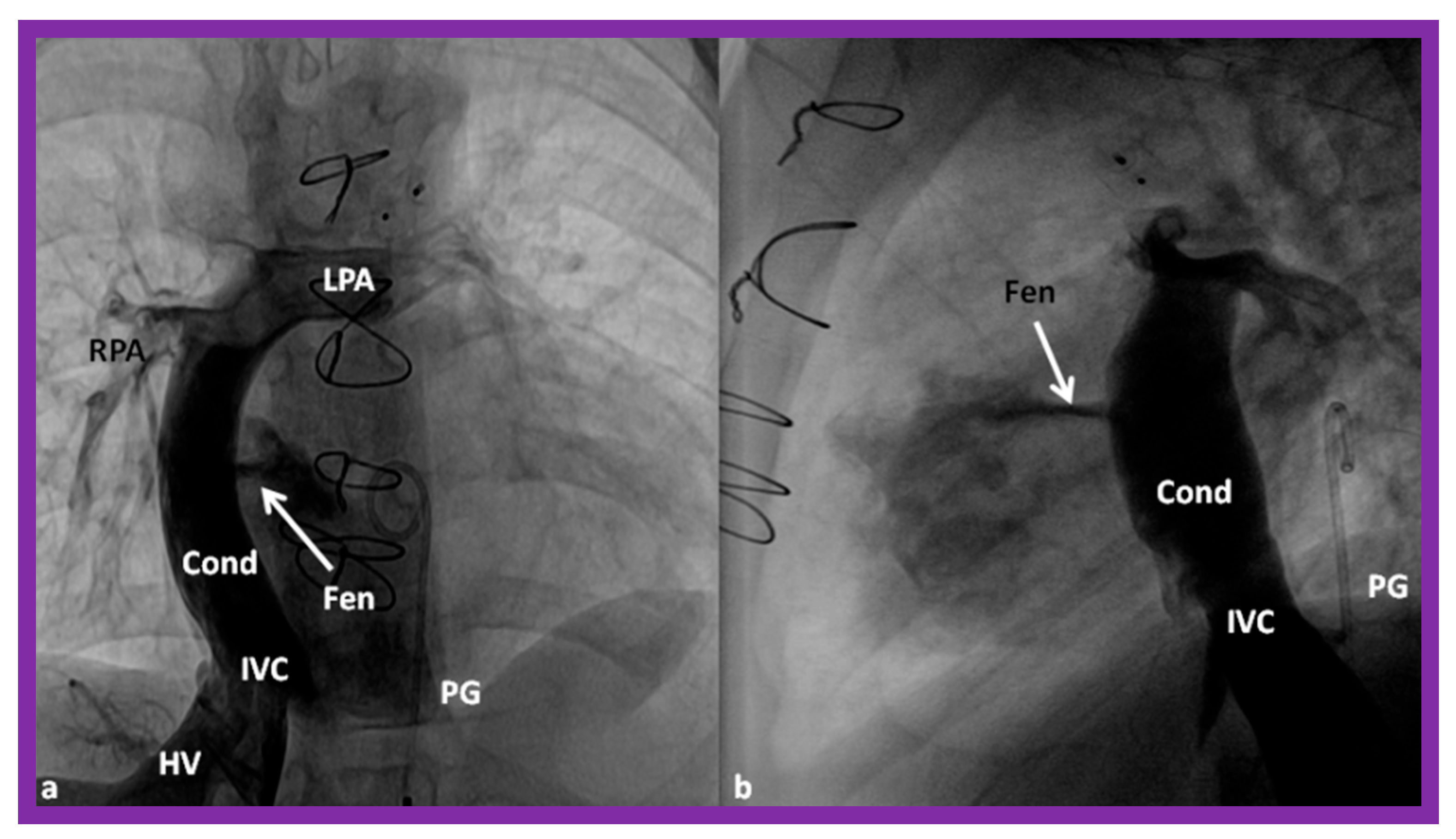
Selected cine frames in the posteroanterior (a) and lateral (b) projections, demonstrating Stage IIIA of the Fontan procedure redirecting the inferior vena caval (IVC) blood flow into the left (LPA) and right (RPA) pulmonary arteries via a non-valved conduit (Cond). The flow of the angiographic material across the fenestration (Fen) is pointed out with arrows in both (a,b). The hepatic veins (HV) and pigtail catheter (PG) in the descending aorta are labeled. Modified from [63].
Figure 8.
Selected cine frames in the posteroanterior (a) and lateral (b) projections, demonstrating Stage IIIA of the Fontan procedure redirecting the inferior vena caval (IVC) blood flow into the left (LPA) and right (RPA) pulmonary arteries via a non-valved conduit (Cond). The flow of the angiographic material across the fenestration (Fen) is pointed out with arrows in both (a,b). The hepatic veins (HV) and pigtail catheter (PG) in the descending aorta are labeled. Modified from [63].

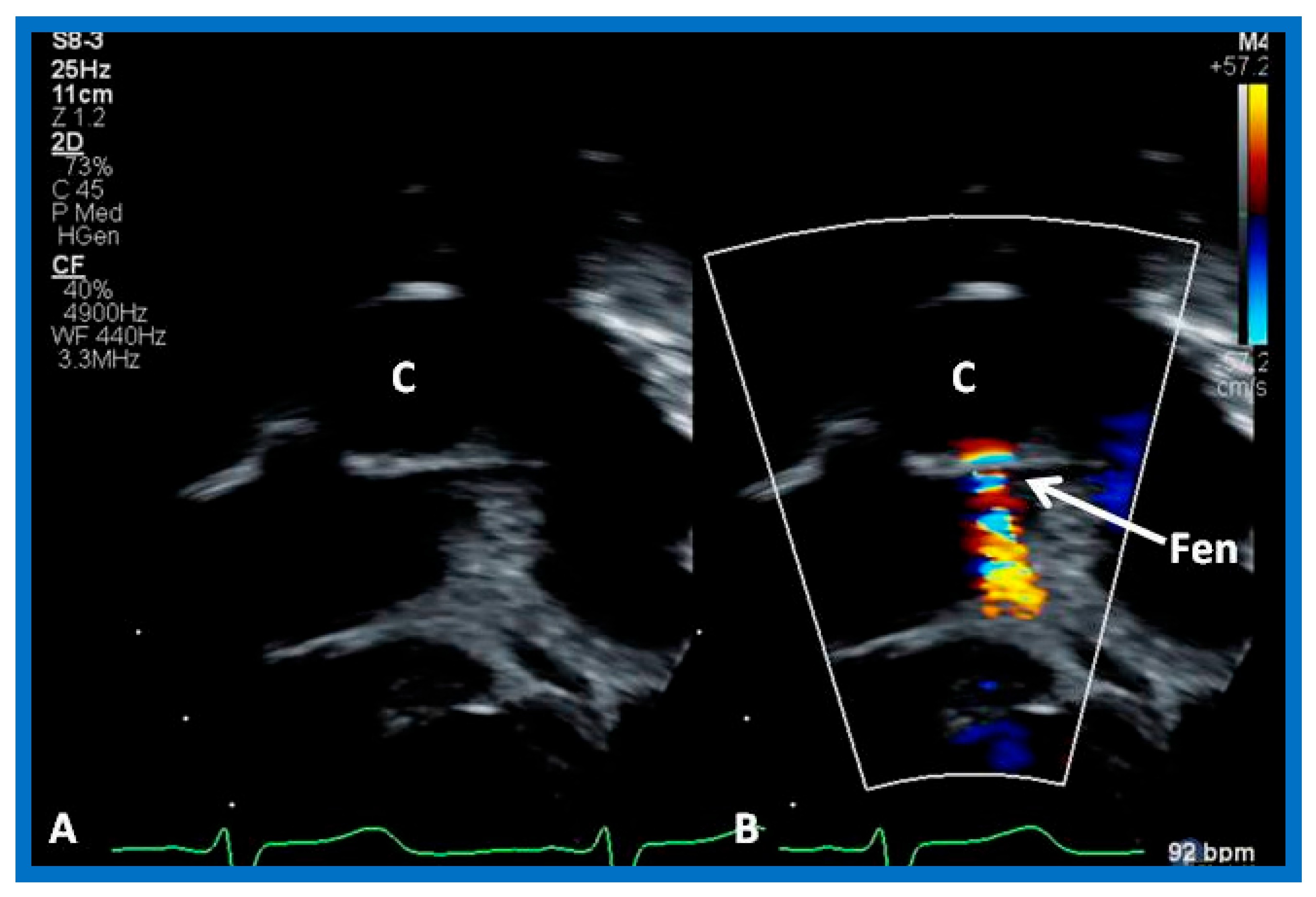
Figure 9.
Echo–Doppler recordings in an apical four-chamber view by two-dimensional (A) and color Doppler (B) illustrating a cross-sectional view of the conduit (C) as shown in (A) and the fenestration (Fen) as demonstrated in (B). Turbulent flow is seen through the fenestration. Reproduced from [21].
Figure 9.
Echo–Doppler recordings in an apical four-chamber view by two-dimensional (A) and color Doppler (B) illustrating a cross-sectional view of the conduit (C) as shown in (A) and the fenestration (Fen) as demonstrated in (B). Turbulent flow is seen through the fenestration. Reproduced from [21].

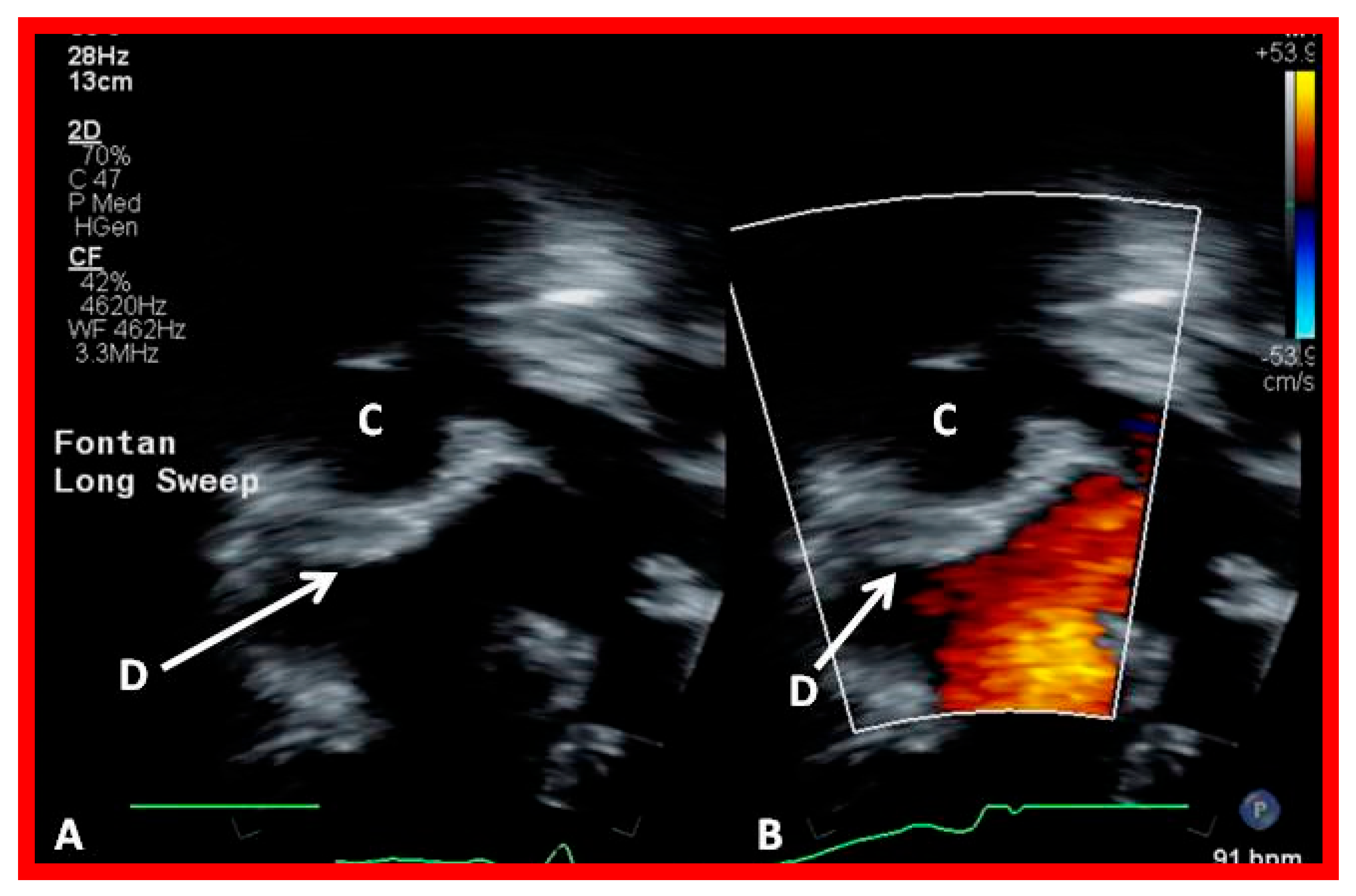
Figure 10.
Echo–Doppler recordings in an apical four-chamber view illustrating the location of the Amplatzer Occluder device (D) (arrows in (A,B)). No residual shunt is demonstrated (B). Conduit (C) is labeled. Reproduced from [21].
Figure 10.
Echo–Doppler recordings in an apical four-chamber view illustrating the location of the Amplatzer Occluder device (D) (arrows in (A,B)). No residual shunt is demonstrated (B). Conduit (C) is labeled. Reproduced from [21].

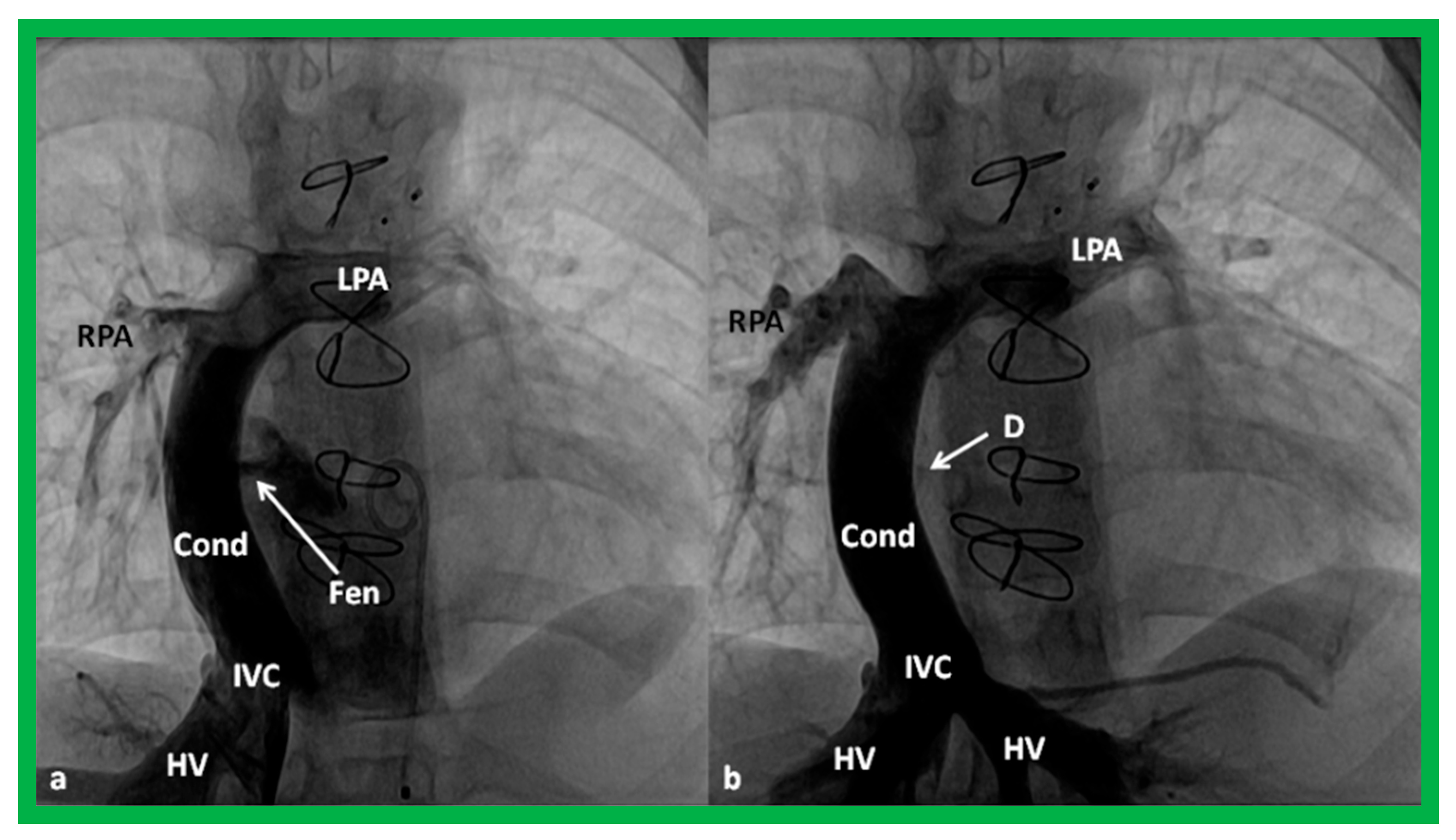
Figure 11.
Cineangiographic images in the posteroanterior projection illustrating Stage IIIA of the Fontan operation transferring the blood from the inferior vena cava (IVC) into the pulmonary arteries via a non-valved conduit (Cond). The fenestration (Fen) is pointed out with an arrow in (a). The fenestration is occluded with an Amplatzer device (D), again, pointed out with an arrow in (b) (Stage IIIB). The hepatic vein (HV), left pulmonary artery (LPA), and right pulmonary artery (RPA) are marked. Reproduced from [63].
Figure 11.
Cineangiographic images in the posteroanterior projection illustrating Stage IIIA of the Fontan operation transferring the blood from the inferior vena cava (IVC) into the pulmonary arteries via a non-valved conduit (Cond). The fenestration (Fen) is pointed out with an arrow in (a). The fenestration is occluded with an Amplatzer device (D), again, pointed out with an arrow in (b) (Stage IIIB). The hepatic vein (HV), left pulmonary artery (LPA), and right pulmonary artery (RPA) are marked. Reproduced from [63].


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Therapy of cardiac malposition.
| Clinical Scenario | Treatment Options |
|---|---|
| Neonates, infants, and children | |
| Pulmonary oligemia | Prostaglandin E1 infusion, modified Blalock–Taussig anastomosis, stenting of the ductus arteriosus, and balloon pulmonary valvuloplasty, as deemed appropriate |
| Pulmonary plethora | Decongestive treatment, pulmonary artery banding |
| Total anomalous pulmonary venous return | Surgical connection of the common pulmonary vein and the left atrium |
| Pulmonary valvar stenosis | Balloon pulmonary valvuloplasty |
| Atrial septal defect | Device occlusion or surgical closure, as appropriate |
| Ventricular septal defect | Surgical repair |
| Patent ductus arteriosus | Device occlusion or surgical closure, as appropriate |
| Lesions with adequate-sized ventricles | Biventricular repair |
| Lesions with hypoplasia of the right or left ventricle | Staged total cavopulmonary connection (Fontan) |
| Patients with decreased splenic function (asplenia and polysplenia) | Antibiotic prophylaxis and Ladd’s procedure (if appropriate) |
| Interstage issues and postintervention complications | As summarized in Section 6 and Section 7 |
| Adults | |
| Coronary artery disease | Percutaneous coronary intervention or surgical coronary artery bypass, as deemed appropriate |
| Supraventricular arrhythmias | Antiarrhythmic medications, catheter ablation (cryoablation or radiofrequency (RF) ablation), Maze procedure, as deemed appropriate |
| Complete atrioventricular block or sick sinus syndrome | Pacemaker therapy (dual-chamber pacemaker or leadless pacemaker implantation) |
| Prevention of sudden death | Implantation of a cardioverter–defibrillator (ICD) or subcutaneous ICDs, as appropriate |
| Prevention of embolic episodes | Initial anticoagulation and subsequent occlusion of the left atrial appendage |
| Aortic valve disease | Balloon aortic valvuloplasty or repair by surgery in younger patients. Transcatheter or surgical replacement of the aortic valve in the elderly |
| Mitral valve disease | Surgical repair or replacement of the mitral valve, as appropriate |
| Hypertrophic cardiomyopathy | Betablocker therapy, surgical myectomy, or alcohol septal ablation, as appropriate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Rao, P.S. Therapy of Patients with Cardiac Malposition. Children 2023, 10, 739. https://doi.org/10.3390/children10040739
AMA Style
Rao PS. Therapy of Patients with Cardiac Malposition. Children. 2023; 10(4):739. https://doi.org/10.3390/children10040739
Chicago/Turabian StyleRao, P. Syamasundar. 2023. "Therapy of Patients with Cardiac Malposition" Children 10, no. 4: 739. https://doi.org/10.3390/children10040739
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.