
Outcomes of Window Therapy with Carboplatin and Ifosfamide for Pediatric Osteosarcoma: A Case Series
 , , ,
, , ,
Abstract
:1. Introduction
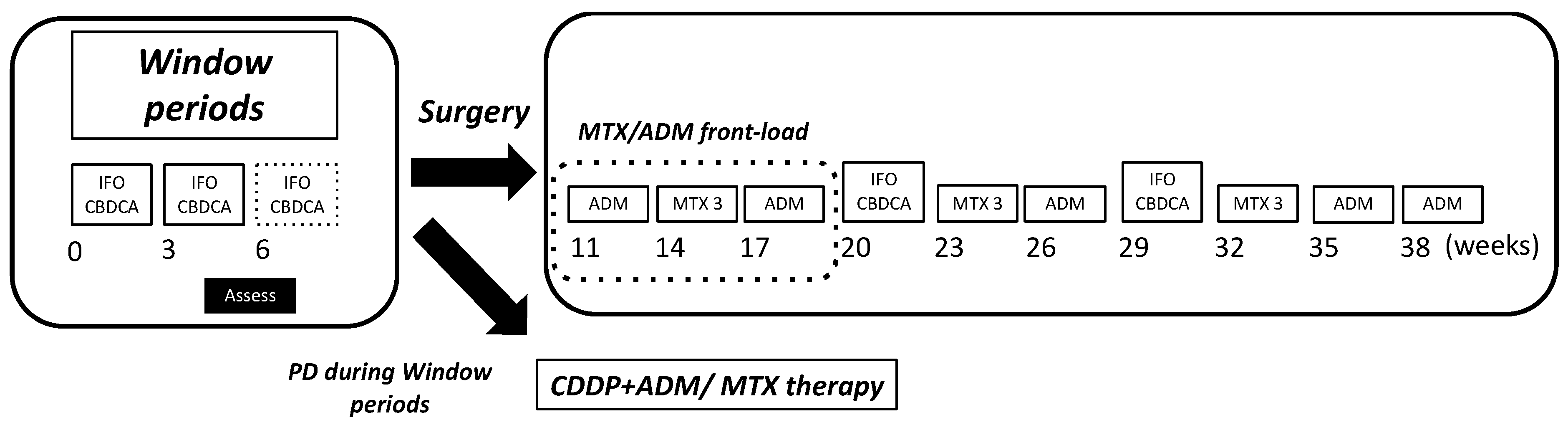
2. Materials and Methods
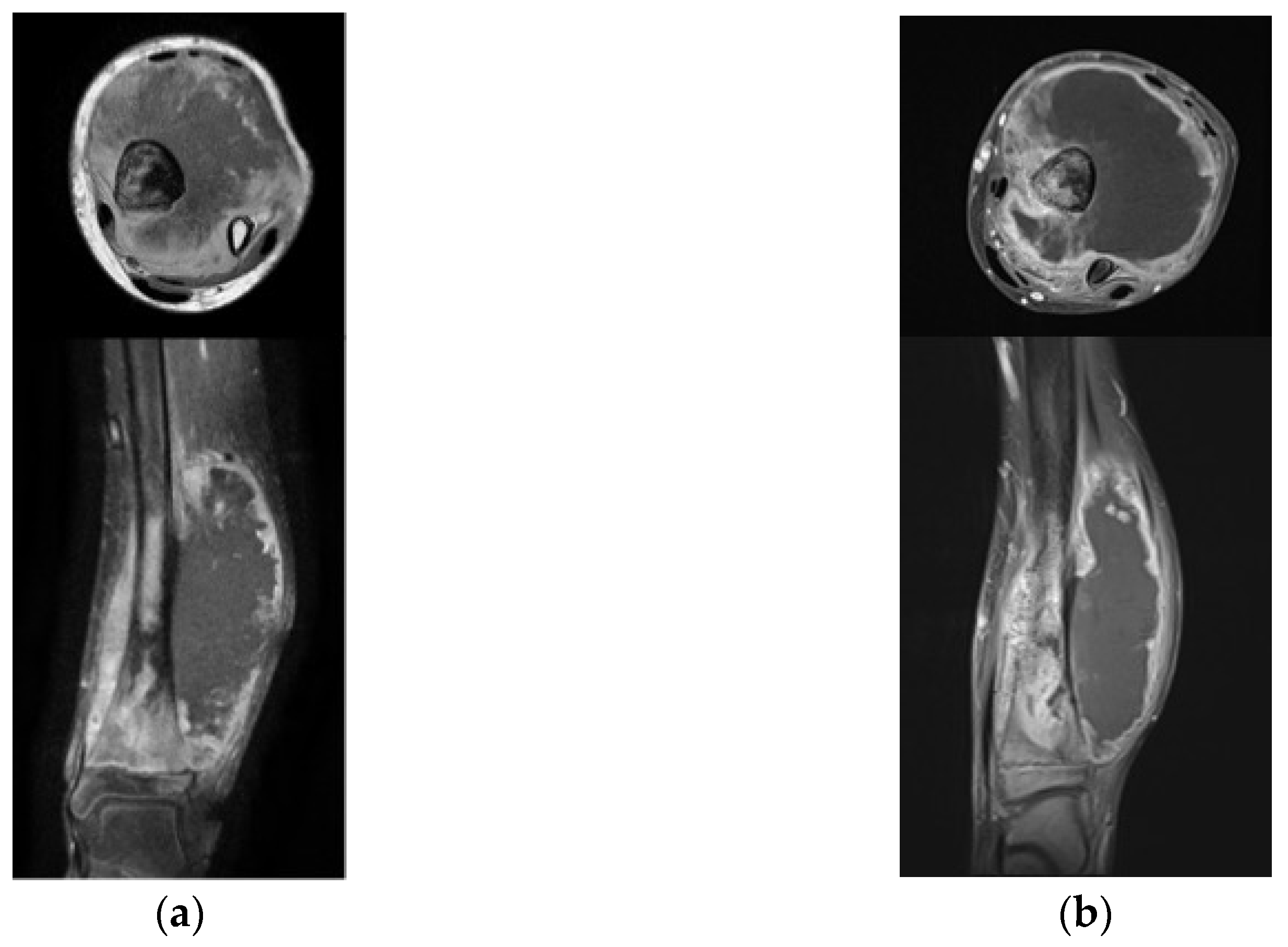
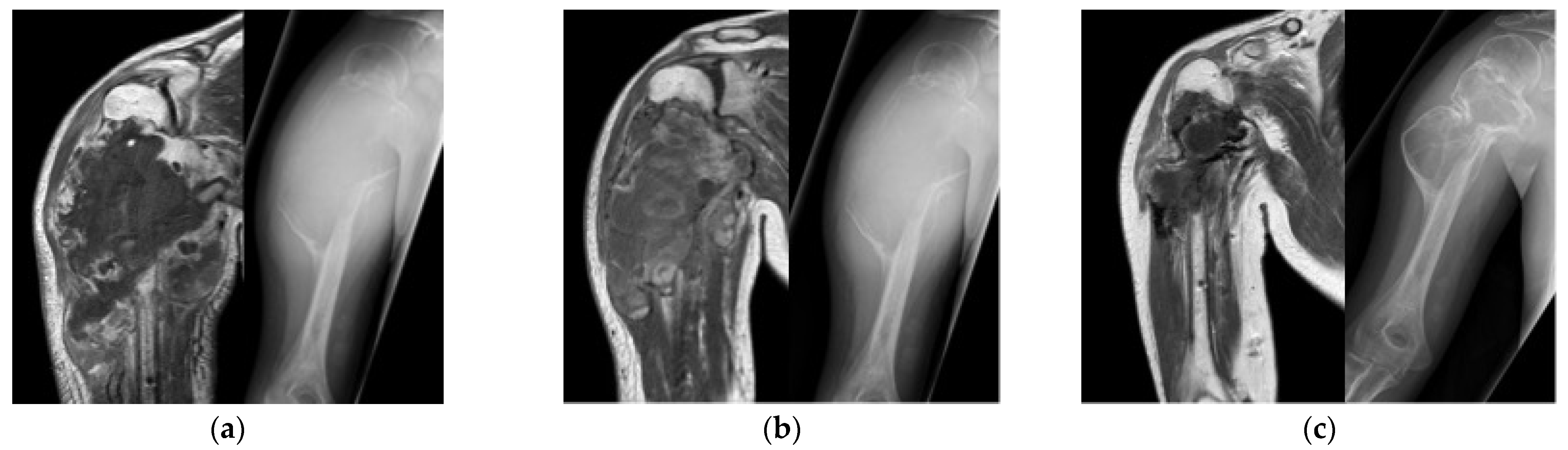
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mirabello, L.; Troisi, R.J.; Savage, S.A. Osteosarcoma incidence and survival rates from 1973 to 2004. Cancer 2009, 115, 1531–1543. [Google Scholar] [CrossRef]
- Cole, S.; Gianferante, D.M.; Zhu, B.; Mirabello, L. Osteosarcoma: A Surveillance, Epidemiology, and End Results program-based analysis from 1975 to 2017. Cancer 2022, 128, 2107–2118. [Google Scholar] [CrossRef] [PubMed]
- Hrushesky, W.J.; Shimp, W.; Kennedy, B.J. Lack of age-dependent cisplatin nephrotoxicity. Am. J. Med. 1984, 76, 579–584. [Google Scholar] [CrossRef]
- McHaney, V.A.; Thibadoux, G.; Hayes, F.A.; Green, A.A. Hearing loss in children receiving cisplatin chemotherapy. J. Pediatr. 1983, 102, 314–317. [Google Scholar] [CrossRef]
- Zhang, J.; Ye, Z.W.; Tew, K.D.; Townsend, D.M. Cisplatin chemotherapy and renal function. Adv. Cancer Res. 2021, 152, 305–327. [Google Scholar] [PubMed]
- Mohindra, N.A. Preventing, Monitoring, and Managing Ototoxicity Related to Cisplatin: Proactive Rather Than Reactive Approaches Are Needed. JCO Oncol. Pract. 2023. [Google Scholar] [CrossRef] [PubMed]
- Lokich, J.; Anderson, N. Carboplatin versus cisplatin in solid tumors: An analysis of the literature. Ann. Oncol. 1998, 9, 13–21. [Google Scholar] [CrossRef]
- Meyer, W.H.; Pratt, C.B.; Poquette, C.A.; Rao, B.N.; Parham, D.M.; Marina, N.M.; Pappo, A.S.; Mahmoud, H.H.; Jenkins, J.J.; Harper, J.; et al. Carboplatin/ifosfamide window therapy for osteosarcoma: Results of the St Jude Children’s Research Hospital OS-91 trial. J. Clin. Oncol. 2001, 19, 171–182. [Google Scholar] [CrossRef]
- Daw, N.C.; Neel, M.D.; Rao, B.N.; Billups, C.A.; Wu, J.; Jenkins, J.J.; Villarroel, M.; Luchtman-Jones, L.; Quintana, J.; Santana, V.M. Frontline treatment of localized osteosarcoma without methotrexate: Results of the St. Jude Children’s Research Hospital OS99 trial. Cancer 2011, 117, 2770–2778. [Google Scholar] [CrossRef]
- van Winkle, P.; Angiolillo, A.; Krailo, M.; Cheung, Y.-K.; Anderson, B.; Davenport, V.; Reaman, G.; Cairo, M.S. Ifosfamide, carboplatin, and etoposide (ICE) reinduction chemotherapy in a large cohort of children and adolescents with recurrent/refractory sarcoma: The Children’s Cancer Group (CCG) experience. Pediatr. Blood Cancer 2005, 44, 338–347. [Google Scholar] [CrossRef]
- Bielack, S.S.; Kempf-Bielack, B.; Delling, G.; Exner, G.U.; Flege, S.; Helmke, K.; Kotz, R.; Salzer-Kuntschik, M.; Werner, M.; Winkelmann, W.; et al. Prognostic factors in high-grade osteosarcoma of the extremities or trunk: An analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J. Clin. Oncol. 2002, 20, 776–790. [Google Scholar] [CrossRef]
- Horie, S.; Oya, M.; Nangaku, M.; Yasuda, Y.; Komatsu, Y.; Yanagita, M.; Kitagawa, Y.; Kuwano, H.; Nishiyama, H.; Ishioka, C.; et al. Guidelines for treatment of renal injury during cancer chemotherapy 2016. Clin. Exp. Nephrol. 2018, 22, 210–244. [Google Scholar] [CrossRef] [PubMed]
- Sleijfer, D.T.; Smit, E.F.; Meijer, S.; Mulder, N.H.; Postmus, P.E. Acute and cumulative effects of carboplatin on renal function. Br. J. Cancer 1989, 60, 116–120. [Google Scholar] [CrossRef]
- van der Hulst, R.J.; Dreschler, W.A.; Urbanus, N.A. High frequency audiometry in prospective clinical research of ototoxicity due to platinum derivatives. Ann. Otol. Rhinol. Laryngol. 1988, 97, 133–137. [Google Scholar] [CrossRef]
- Hudson, M.; Jaffe, M.R.; Jaffe, N.; Ayala, A.; Raymond, A.K.; Carrasco, H.; Wallace, S.; Murray, J.; Robertson, R. Pediatric osteosarcoma: Therapeutic strategies, results, and prognostic factors derived from a 10-year experience. J. Clin. Oncol. 1990, 8, 1988–1997. [Google Scholar] [CrossRef]
- Marina, N.M.; Smeland, S.; Bielack, S.S.; Bernstein, M.; Jovic, G.; Krailo, M.D.; Hook, J.M.; Arndt, C.; van den Berg, H.; Brennan, B.; et al. Comparison of MAPIE versus MAP in patients with a poor response to preoperative chemotherapy for newly diagnosed high-grade osteosarcoma (EURAMOS-1): An open-label, international, randomised controlled trial. Lancet Oncol. 2016, 17, 1396–1408. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, Y.; Tanaka, K.; Isu, K.; Kawai, A.; Tatezaki, S.-I.; Ishii, T.; Kushida, K.; Beppu, Y.; Usui, M.; Tateishi, A.; et al. Multiinstitutional phase II study of neoadjuvant chemotherapy for osteosarcoma (NECO study) in Japan: NECO-93J and NECO-95J. J. Orthop. Sci. 2009, 14, 397–404. [Google Scholar] [CrossRef]
- Hiraga, H.; Ozaki, T. Adjuvant and neoadjuvant chemotherapy for osteosarcoma: JCOG Bone and Soft Tissue Tumor Study Group. Jpn. J. Clin. Oncol. 2021, 51, 1493–1497. [Google Scholar] [CrossRef] [PubMed]
- Choeyprasert, W.; Natesirinilkul, R.; Charoenkwan, P.; Sittipreechacharn, S. Carboplatin and doxorubicin in treatment of pediatric osteosarcoma: A 9-year single institute experience in the Northern Region of Thailand. Asian Pac. J. Cancer Prev. 2013, 14, 1101–1106. [Google Scholar] [CrossRef]
- Skinner, R. Late renal toxicity of treatment for childhood malignancy: Risk factors, long-term outcomes, and surveillance. Pediatr. Nephrol. 2018, 33, 215–225. [Google Scholar] [CrossRef]
- Marina, N.M.; Poquette, C.A.; Cain, A.M.; Jones, D.; Pratt, C.B.; Meyer, W.H. Comparative renal tubular toxicity of chemotherapy regimens including ifosfamide in patients with newly diagnosed sarcomas. J. Pediatr. Hematol. Oncol. 2000, 22, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Hecker-Nolting, S.; Langer, T.; Blattmann, C.; Kager, L.; Bielack, S.S. Current insights into the management of late chemotherapy toxicities in pediatric osteosarcoma patients. Cancer Manag. Res. 2021, 13, 8989–8998. [Google Scholar] [CrossRef] [PubMed]
- Freyer, D.R.; Brock, P.R.; Chang, K.W.; Dupuis, L.; Epelman, S.; Knight, K.; Mills, D.; Phillips, R.; Potter, E.; Risby, D.; et al. Prevention of cisplatin-induced ototoxicity in children and adolescents with cancer: A clinical practice guideline. Lancet Child Adolesc. Health 2020, 4, 141–150. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Grade 3/4 Toxicity (15 Cycles in 7 Patients) | The Number of Events | |
|---|---|---|
| Blood and lymphatic disorders | Neutropenia | 13 |
| Anemia | 11 | |
| Thrombocytopenia | 8 | |
| Febrile neutropenia | 2 | |
| Renal and urinary/metabolism disorders | Creatinine elevation | 0 |
| Electrolyte imbalance | 0 | |
| Gastrointestinal disorders/hepatobiliary disorders | Vomiting | 0 |
| Nausea | 0 | |
| Anorexia | 0 | |
| Alanine/aspartate aminotransferase increased | 0 | |
| Increased blood bilirubin level | 0 | |
| Cardiac disorders | Heart failure | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aiba, H.; Kamei, M.; Ito, Y.; Takeda, R.; Yamada, S.; Okamoto, H.; Hayashi, K.; Miwa, S.; Kawaguchi, Y.; Saito, S.; et al. Outcomes of Window Therapy with Carboplatin and Ifosfamide for Pediatric Osteosarcoma: A Case Series. Children 2023, 10, 736. https://doi.org/10.3390/children10040736
Aiba H, Kamei M, Ito Y, Takeda R, Yamada S, Okamoto H, Hayashi K, Miwa S, Kawaguchi Y, Saito S, et al. Outcomes of Window Therapy with Carboplatin and Ifosfamide for Pediatric Osteosarcoma: A Case Series. Children. 2023; 10(4):736. https://doi.org/10.3390/children10040736
Chicago/Turabian StyleAiba, Hisaki, Michi Kamei, Yasuhiko Ito, Risa Takeda, Satoshi Yamada, Hideki Okamoto, Katsuhiro Hayashi, Shinji Miwa, Yohei Kawaguchi, Shiro Saito, and et al. 2023. "Outcomes of Window Therapy with Carboplatin and Ifosfamide for Pediatric Osteosarcoma: A Case Series" Children 10, no. 4: 736. https://doi.org/10.3390/children10040736