

Identifying the Aetiology of Acute Liver Failure Is Crucial to Impact Positively on Outcome
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Diagnosis and Management
2.3. Division into Two Groups and Statistics
- -
- Group 1 (G1): patients diagnosed with ALF from 1997 to 2009.
- -
- Group 2 (G2): patients diagnosed with ALF from 2010 to 2022.
3. Results
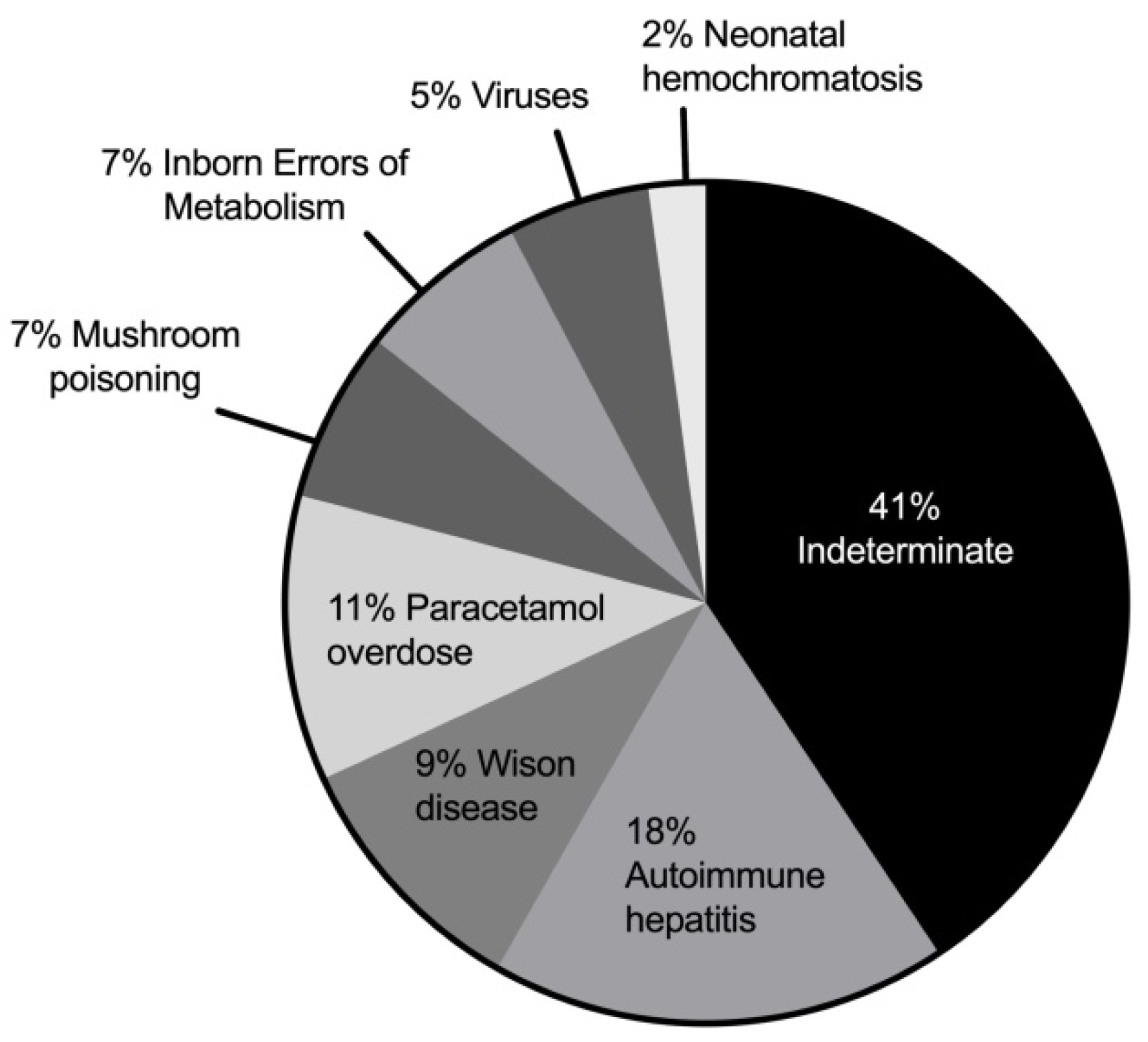
3.1. ALF Aetiology
3.2. Clinical Features and Laboratory Investigations
3.3. Management of PALF
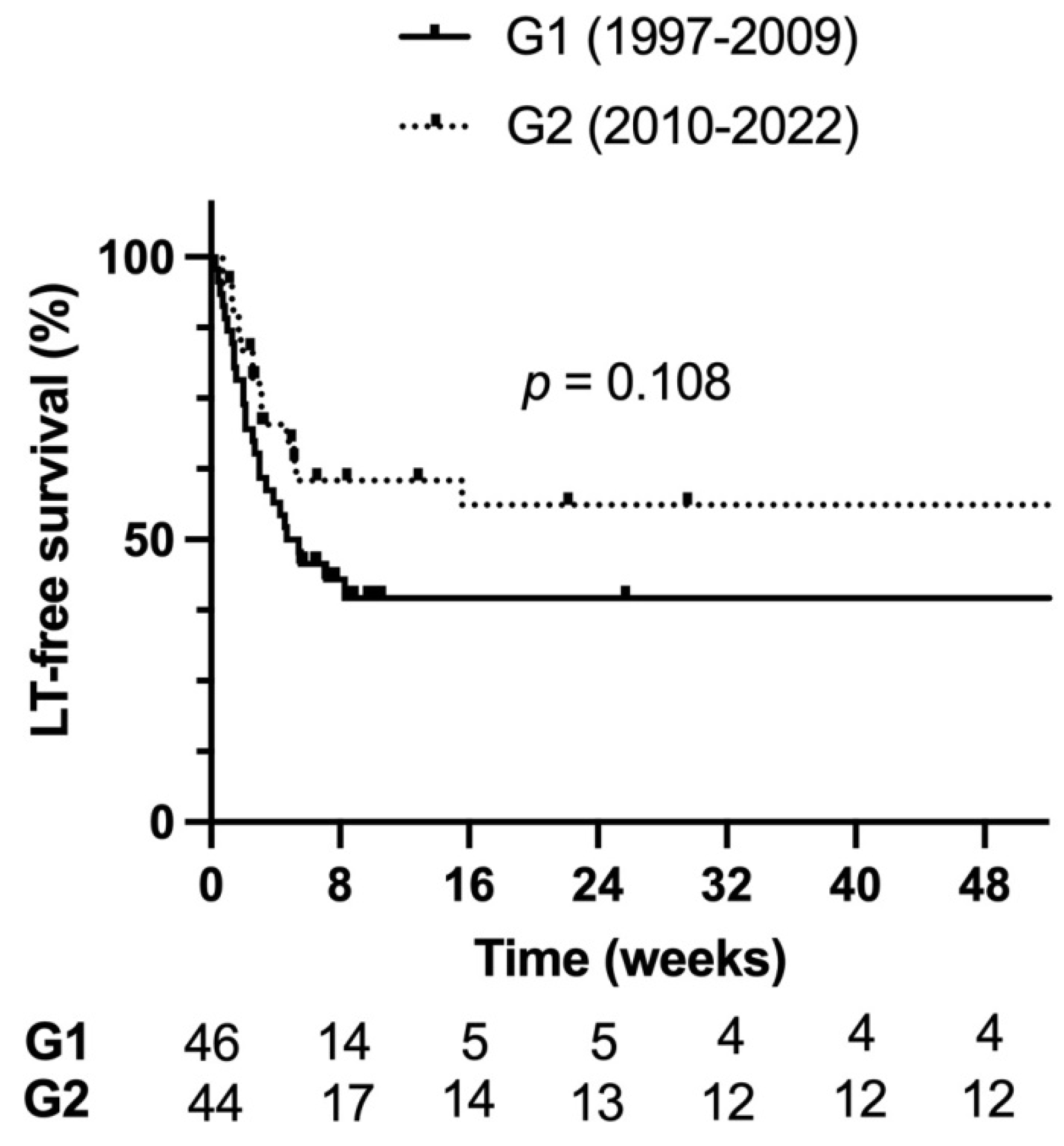
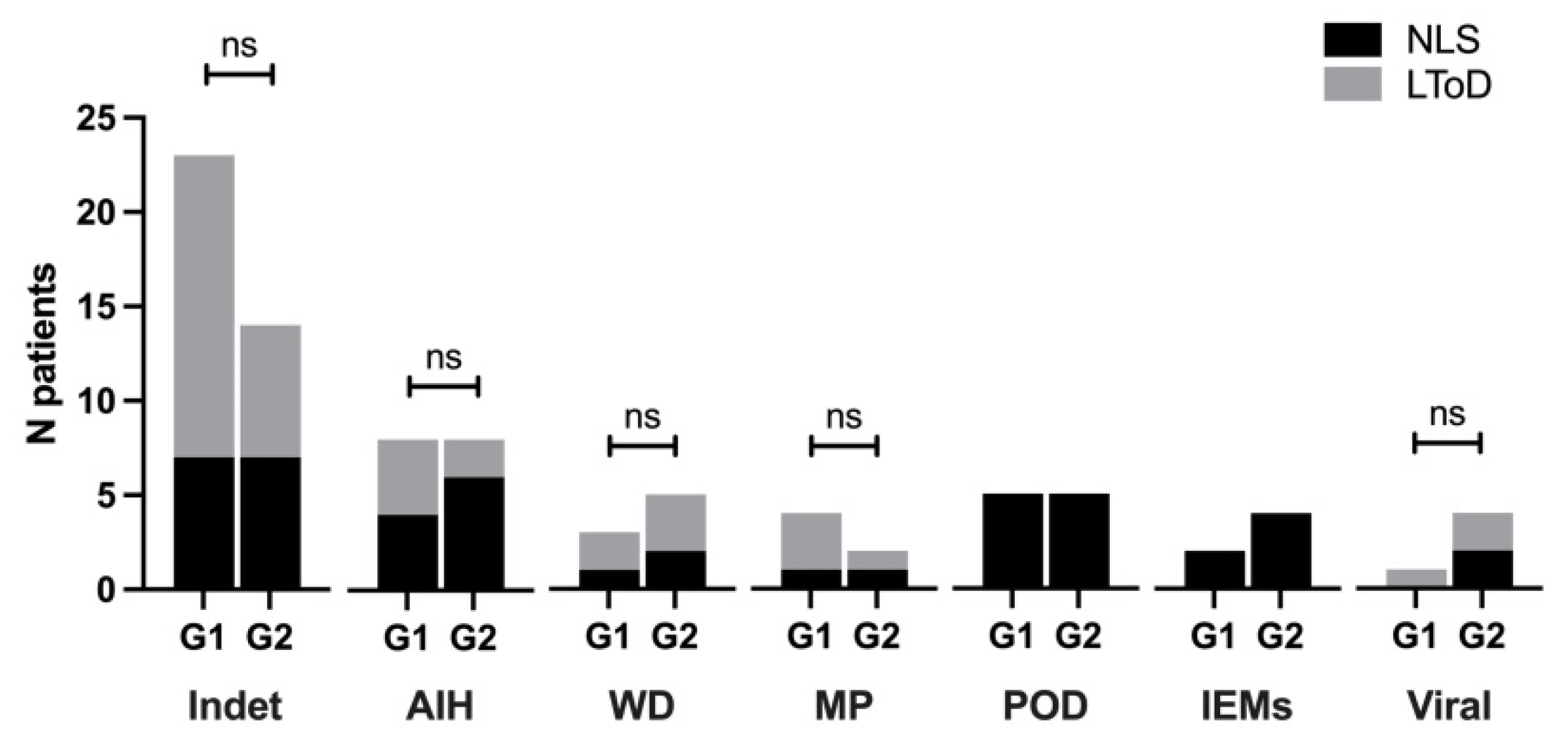
3.4. Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Squires, R.H., Jr.; Shneider, B.L.; Bucuvalas, J.; Alonso, E.; Sokol, R.J.; Narkewicz, M.R.; Dhawan, A.; Rosenthal, P.; Rodriguez-Baez, N.; Murray, K.F.; et al. Acute liver failure in children: The first 348 patients in the pediatric acute liver failure study group. J. Pediatr. 2006, 148, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Bucuvalas, J.; Yazigi, N.; Squires, R.H. Acute liver failure in children. Clin. Liver Dis. 2006, 10, 149–168. [Google Scholar]
- Dhawan, A. Acute liver failure in children and adolescents. Clin. Res. Hepatol. Gastroenterol. 2012, 36, 278–283. [Google Scholar]
- Black, D.D. The continuing challenge of “indeterminate” acute liver failure. J. Pediatr. 2009, 155, 769–770. [Google Scholar]
- Narkewicz, M.R.; Horslen, S.; Hardison, R.M. Squires RH and pediatric acute liver failure study group. A learning collaborative approach increases specificity of diagnosis of acute liver failure in pediatric patients. Clin. Gastroenterol. Hepatol. 2018, 16, 1801–1810. [Google Scholar]
- Di Giorgio, A.; Bartolini, E.; Calvo, P.L.; Cananzi, M.; Cirillo, F.; Della Corte, C.; Dionisi-Vici, C.; Indolfi, G.; Iorio, R.; Maggiore, G.; et al. Diagnostic Approach to Acute Liver Failure in Children: A Position Paper by the SIGENP Liver Disease Working Group. Dig. Liver Dis. 2021, 53, 545–557. [Google Scholar]
- Locatelli, F.; Jordan, M.B.; Allen, C.; Cesaro, S.; Rizzari, C.; Rao, A.; Degar, B.; Garrington, T.P.; Sevilla, J.; Putti, M.C.; et al. Emapalumab in children with primary hemophagocytic lymphohistiocytosis. N. Engl. J. Med. 2020, 382, 1811–1822. [Google Scholar]
- Alvarez, F.; Berg, P.A.; Bianchi, F.B.; Bianchi, L.; Burroughs, A.K.; Cancado, E.L.; Chapman, R.W.; Cooksley, W.G.; Czaja, A.J.; Desmet, V.J.; et al. International autoimmune hepatitis group report: Review of criteria for diagnosis of autoimmune hepatitis. J. Hepatol. 1999, 31, 929–938. [Google Scholar]
- Hennes, E.M.; Zeniya, M.; Czaja, A.J.; Parés, A.; Dalekos, G.N.; Krawitt, E.L.; Bittencourt, P.L.; Porta, G.; Boberg, K.M.; Hofer, H.; et al. Simplified criteria for the diagnosis of autoimmune hepatitis. Hepatology 2008, 48, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Alonso, E.M.; Horslen, S.P.; Beherens, E.M.; Doo, E. Pediatric acute liver failure of undetermined cause: A research workshop. Hepatology 2017, 65, 1026–1037. [Google Scholar] [PubMed]
- Lee, W.S.; McKiernan, P.; Kelly, D.A. Etiology, outcome and prognostic indicators of childhood fulminant hepatic failure in the United Kingdom. J. Pediatr. Gastroenterol. Nutr. 2005, 40, 575–581. [Google Scholar] [CrossRef] [PubMed]
- McKiernan, P.J. Nitisinone in the treatment of hereditary tyrosinaemia type 1. Drugs 2006, 66, 743–750. [Google Scholar] [CrossRef] [PubMed]
- Di Giorgio, A.; Bravi, M.; Bonanomi, E.; Alessio, G.; Sonzogni, A.; Zen, Y.; Colledan, M.; D’Antiga, L. Fulminant hepatic failure of autoimmune aetiology in children. J. Pediatr. Gastroenterol. Nutr. Feb. 2015, 60, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Di Giorgio, A.; Sonzogni, A.; Piccichè, A.; Alessio, G.; Bonanomi, E.; Colledan, M.; D’Antiga, L. Successful management of acute liver failure in Italian children: A 16-year experience at a referral centre for paediatric liver transplantation. Dig. Liver Dis. 2017, 49, 1139–1145. [Google Scholar] [CrossRef] [PubMed]
- Ferenci, P.; Lockwood, A.; Mullen, K.; Tarter, R.; Weissenborn, K.; Blei, A.T. Hepatic encephalopathy–definition, nomenclature, diagnosis, and quantification: Final report of the working party at the 11th World Congresses of Gastroenterology, Vienna, 1998. Hepatology 2002, 35, 716–721. [Google Scholar] [CrossRef]
- Lizardi-Cervera, J.; Almeda, P.; Guevara, L.; Uribe, M. Hepatic encephalopathy: A review. Ann. Hepatol. 2003, 2, 122–130. [Google Scholar] [CrossRef]
- Di Giorgio, A.; Nicastro, E.; Dalla Rosa, D.; Nebbia, G.; Sonzogni, A.; D’Antiga, L. Transplant-free Survival in Chronic Liver Disease Presenting as Acute Liver Failure in Childhood. Transplantation 2019, 103, 544–551. [Google Scholar] [CrossRef]
- Tüfekçi, Ö.; Özdemir, H.H.; Malbora, B.; Özbek, N.Y.; Yarali, N.; Erdem, A.; Evim, M.; Baytan, B.; Güneş, A.M.; Karapinar, T.; et al. Hepatitis-Associated Aplastic Anemia: Etiology, Clinical Characteristics and Outcome. J. Pediatr. Hematol. Oncol. 2022, 44, e223–e226. [Google Scholar] [CrossRef]
- Indolfi, G.; Bèrczes, R.; Pelliccioli, I.; Bosisio, M.; Agostinis, C.; Resti, M.; Zambelli, M.; Lucianetti, A.; Colledan, M.; D’Antiga, L. Neonatal haemochromatosis with reversible pituitary involvement. Transpl. Int. 2014, 27, 76–79. [Google Scholar] [CrossRef]
- Narkewicz, M.R.; Dell Olio, D.; Karpen, S.J.; Murray, K.F.; Schwarz, K.; Yazigi, N.; Zhang, S.; Belle, S.H.; Squires, R.H. Pediatric Acute Liver Failure Study Group. Pattern of diagnostic evaluation for the causes of pediatric acute liver failure: An opportunity for quality improvement. J. Pediatr. 2009, 155, 801–806. [Google Scholar] [CrossRef]
- Devictor, D.; Tissieres, P.; Afanetti, M.; Debray, D. Acute liver failure in children. Clin. Res. Hepatol. Gastroenterol. 2011, 35, 430–437. [Google Scholar] [CrossRef] [PubMed]
- Bernal, W.; Ma, Y.; Smith, H.M.; Portmann, B.; Wendon, J.; Vergani, D. The significance of autoantibodies and immunoglobulins in acute liver failure: A cohort study. J. Hepatol. 2007, 47, 664–670. [Google Scholar] [CrossRef]
- Rochling, F.A.; Jones, W.F.; Chau, K.; DuCharme, L.; Mimms, L.T.; Moore, B.; Scheffel, J.; Cuthbert, J.A.; Thiele, D.L. Acute sporadic non-A, non-B, non-C, non-D, non-E hepatitis. Hepatology 1997, 25, 478–483. [Google Scholar] [CrossRef]
- Miraglia, R.; Luca, A.; Gruttadauria, S.; Minervini, M.I.; Vizzini, G.; Arcadipane, A.; Gridelli, B. Contribution of transjugular liver biopsy in patients with the clinical presentation of acute liver failure. Cardiovasc. Interv. Radiol. 2006, 29, 1008–1010. [Google Scholar] [CrossRef]
- Jain, V.; Dhawan, A. Prognostic modeling in pediatric acute liver failure. Liver Transpl. 2016, 22, 1418–1430. [Google Scholar] [CrossRef]
- Chapin, C.A.; Horslen, S.P.; Squires, J.E.; Lin, H.; Blondet, N.; Mohammad, S.; Alonso, E.M. Corticosteroid Therapy for Indeterminate Pediatric Acute Liver Failure and Aplastic Anemia with Acute Hepatitis. J. Pediatr. 2019, 208, 23–29. [Google Scholar] [CrossRef]
- Chapin, C.A.; Burn, T.; Meijome, T.; Loomes, K.M.; Melin-Aldana, H.; Kreiger, P.A.; Whitington, P.F.; Behrens, E.M.; Alonso, E.M. Indeterminate pediatric acute liver failure is uniquely characterized by a CD103+ CD8+ T-cell infiltrate. Hepatology 2018, 68, 1087–1100. [Google Scholar] [CrossRef] [PubMed]
- Ichai, P.; Duclos-Vallée, J.C.; Guettier, C.; Hamida, S.B.; Antonini, T.; Delvart, V.; Saliba, F.; Azoulay, D.; Castaing, D.; Samuel, D. Usefulness of corticosteroids for the treatment of severe and fulminant forms of autoimmune hepatitis. Liver Transpl. 2007, 13, 996–1003. [Google Scholar] [CrossRef]
- Psacharopoulos, H.T.; Mowat, A.P.; Davies, M.; Portmann, B.; Silk, D.B.; Williams, R. Fulminant hepatic failure in childhood: An analysis of 31 cases. Arch. Dis. Child. 1980, 55, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Hadzić, N.; Height, S.; Ball, S.; Rela, M.; Heaton, N.D.; Veys, P.; Mieli-Vergani, G. Evolution in the management of acute liver failure-associated aplastic anaemia in children: A single centre experience. J. Hepatol. 2008, 48, 68–73. [Google Scholar] [CrossRef]
- Rogers, Z.R.; Nakano, T.A.; Olson, T.S.; Bertuch, A.A.; Wang, W.; Gillio, A.; Coates, T.D.; Chawla, A.; Castillo, P.; Kurre, P.; et al. Immunosuppressive therapy for pediatric aplastic anemia: A North American Pediatric Aplastic Anemia Consortium study. Haematologica 2019, 104, 1974–1983. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients n = 90 | Group 1 (1997–2009) n = 46 | Group 2 (2010–2022) n = 44 | p Value |
|---|---|---|---|---|
| Males, n (%) | 43 (48%) | 25 (54%) | 18 (41%) | 0.214 |
| Age at onset, years | 4.6 (1.2–10.4) | 3.1 (0.7–8.7) | 5.0 (1.8–12.1) | 0.124 |
| Aetiologies | ||||
| Indeterminate | 37 (41%) | 23 (50%) | 14 (32%) | 0.09 |
| AIH | 16 (18%) | 8 (17%) | 8 (18%) | 1.00 |
| Type 1 | 8 | 3 | 5 | - |
| Type 2 | 8 | 5 | 3 | - |
| Wilson disease | 8 (9%) | 3 (7%) | 5 (11%) | 0.48 |
| Neonatal hemochromatosis | 2 (2%) | 0 | 2 (5%) | 0.23 |
| Inborn errors of metabolisms | 6 (7%) | 2 (4%) | 4 (9%) | 0.42 |
| Galactosemia | 1 | 0 | 1 | - |
| Urea cycle defect | 2 | 1 | 1 | - |
| Glycogen storage disease IV | 1 | 0 | 1 | - |
| Mitochondrial respiratory Chain defects | 2 | 1 | 1 | - |
| Mushroom poisoning | 6 (7%) | 4 (9%) | 2 (5%) | 0.67 |
| Paracetamol | 10 (11%) | 5 (11%) | 5 (11%) | 1.00 |
| Viral infection | 5 (5%) | 1 (2%) | 4 (9%) | 0.19 |
| Symptoms at onset | ||||
| Fever | 19 (21%) | 11 (24%) | 8 (18%) | 0.60 |
| GI symptoms | 45 (50%) | 18 (39%) | 27 (61%) | 0.05 |
| Jaundice | 48 (53%) | 22 (48%) | 26 (59%) | 0.30 |
| Laboratory features | ||||
| ALT, IU/L | 2090 (695–4426) | 2187 (801–4798) | 2037 (354–3488) | 0.08 |
| INR | 3.4 (2.8–4.8) | 3.8 (2.9–4.8) | 3.2 (2.4–4.8) | 0.80 |
| WBCs·103/μL | 8000 (5490–10,370) | 8265 (5915–11,835) | 7895 (5167–9662) | 0.58 |
| Lymphocytes·103/μL | 2250 (1425–3895) | 2620 (1685–4625) | 2040 (1180–3530) | 0.08 |
| Hb, g/dL | 10 (9–12) | 9.9 (8.8–11.7) | 10.6 (9.1–11.5) | 0.75 |
| Platelets·103/μL | 181,000 (96,000–280,000) | 193,500 (116,000–265,750) | 163,500 (84,250–288,575) | 0.87 |
| Albumin, g/dL | 3.3 (3–3.8) | 3.3 (3.1–4) | 3.1 (2.8–3.4) | 0.009 |
| Tot bilirubin, mg/dL | 13.1 (4–21.7) | 17.1 (6.5–23.5) | 11.5 (3.4–19.1) | 0.15 |
| Ammonia, µmol/L | 134 (66–195) | 153 (99.5–220.5) | 94 (58–145) | 0.01 |
| Positive autoantibodies | 40 (44%) | 25 (54%) | 15 (34%) | 0.06 |
| ANA (≥1:20): n (%) | 16 (18%) | 6 (13%) | 10 (23%) | 0.27 |
| SMA (≥1:20): n (%) | 19 (21%) | 5 (11%) | 14 (32%) | 0.02 |
| Anti-LKM-1 (≥1:10): n (%) | 7 (7%) | 5 (11%) | 2 (4%) | 0.43 |
| Anti-LC1: n (%) | 5 (5%) | 3 (6%) | 2 (4%) | 1.00 |
| ANCA: n (%) | 9 (10%) | 1 (2%) | 8 (18%) | 0.01 |
| IgG g/L (nv 5–18 g/L) | 10.6 (8.4–15.1) | 11.1 (8.2–15.1) | 10.5 (8.6–14.1) | 0.64 |
| Ascites, n (%) | 18 (20%) | 3 (6%) | 15 (34%) | 0.001 |
| Splenomegaly *, n (%) | 25 (28%) | 10 (22%) | 15 (34%) | 0.24 |
| HE grade III–IV, n (%) | 50 (55%) | 29 (66%) | 20 (45%) | 0.13 |
| Liver histology (available in 59 patients) § | ||||
| Cirrhosis, n (%) | 18 (20%) | 10 (22%) | 8 (18%) | 0.793 |
| Variables | All Patients n = 90 | Group 1 (1997–2009) n = 46 | Group 2 (2010–2022) n = 44 | p Value |
|---|---|---|---|---|
| Treatment with steroids, n (%) * | 21 (23%) | 9 (20%) | 12 (27%) | ns |
| Extracorporeal liver support, n (%) | 12 (13%) | 7 (15%) | 5 (11%) | ns |
| Listed for transplant, n (%) | 52 (58%) | 29 (63%) | 23 (52%) | ns |
| Median time on waiting list (days) | 6 (2–11) | 6.5 (2–10) | 5 (2–13) | ns |
| Died on waiting list | 3 | 2 | 1 | ns |
| Recovery without TX | 8 | 2 | 6 | ns |
| Transplanted | 41 | 26 | 15 | 0.03 |
| Split graft ** | 34 | 23 | 11 | ns |
| Whole graft | 7 | 3 | 4 | ns |
| Outcome at last FU | ||||
| Survived | 85 (94%) | 43 (93%) | 42 (95%) | ns |
| Died | 5 (5%) | 3 (6%) | 2 (4%) | ns |
| Complications after ALF | ||||
| - Aplastic anemia | 6 (7%) | 0 | 6 (14%) | 0.01 |
| - Neurological sequaele | 2 (2%) | 2 (4%) | 0 | ns |
| Causes of ALF | Outcome Whole Period (1997–2022) | Survival | p Value | |||||
|---|---|---|---|---|---|---|---|---|
| Patients | Recovery without TX | LT | Died | Whole Period | G1 (1997–2009) | G2 (2010–2012) | G1 vs. G2 | |
| Autoimmune hepatitis | 16 | 9 | 6 | 1 * | 94% | 87% | 100% | ns |
| Wilson’s disease | 8 | 3 | 5 | 0 | 100% | 100% | 100% | ns |
| Neonatal hemochromatosis | 2 | 1 | 1 | 0 | 100% | - | 100% | - |
| Metabolic disorders | 6 | 6 | 0 | 0 | 100% | 100% | 100% | ns |
| Paracetamol overdose | 10 | 10 | 0 | 0 | 100% | 100% | 100% | ns |
| Mushroom poisoning | 6 | 4 | 2 | 0 | 100% | 100% | 100% | ns |
| Viral infection | 5 | 2 | 2 | 1 * | 80% | 100% | 75% | ns |
| Indeterminate | 37 | 11 | 23 | 3 ** | 92% | 91% | 92% | ns |
| All aetiologies | 90 | 44 | 41 | 5 | 94% | 94% | 95% | ns |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Giorgio, A.; Gamba, S.; Sansotta, N.; Nicastro, E.; Colledan, M.; D’Antiga, L. Identifying the Aetiology of Acute Liver Failure Is Crucial to Impact Positively on Outcome. Children 2023, 10, 733. https://doi.org/10.3390/children10040733
Di Giorgio A, Gamba S, Sansotta N, Nicastro E, Colledan M, D’Antiga L. Identifying the Aetiology of Acute Liver Failure Is Crucial to Impact Positively on Outcome. Children. 2023; 10(4):733. https://doi.org/10.3390/children10040733
Chicago/Turabian StyleDi Giorgio, Angelo, Silvia Gamba, Naire Sansotta, Emanuele Nicastro, Michele Colledan, and Lorenzo D’Antiga. 2023. "Identifying the Aetiology of Acute Liver Failure Is Crucial to Impact Positively on Outcome" Children 10, no. 4: 733. https://doi.org/10.3390/children10040733