
Association between Eruption Sequence of Posterior Teeth, Dental Crowding, Arch Dimensions, Incisor Inclination, and Skeletal Growth Pattern

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample Selection
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Demographic Characteristics of the Sample
3.2. Sequence of Eruption
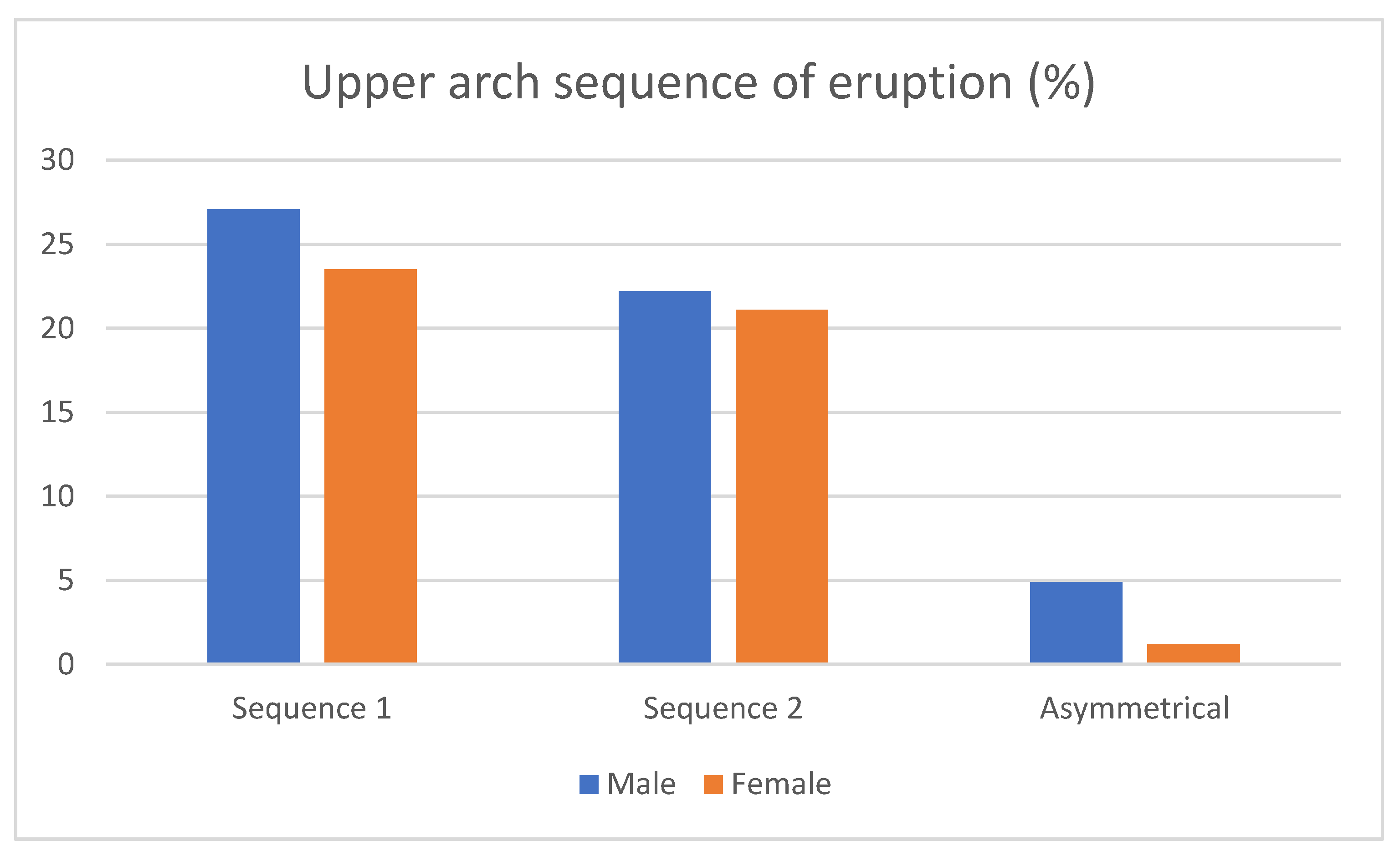
- Maxillary sequences: the prevalence of Seq1 (3–5) was 50.6%, whereas for Seq2 (5–3), it was 43.2%. 6.1% were asymmetrical cases. Regarding gender differences, 27.1% of men and 23.5% of women showed Seq1, while 22.2 of men and 21.1% of women presented Seq2. In addition, 4.9% of men and 1.2 % of women had asymmetrical sequences (Figure 2). Differences between sexes were not statistically significant (p = 0.689).Figure 2. Sex-related frequencies of upper eruption sequences.
![Children 10 00674 g002]()

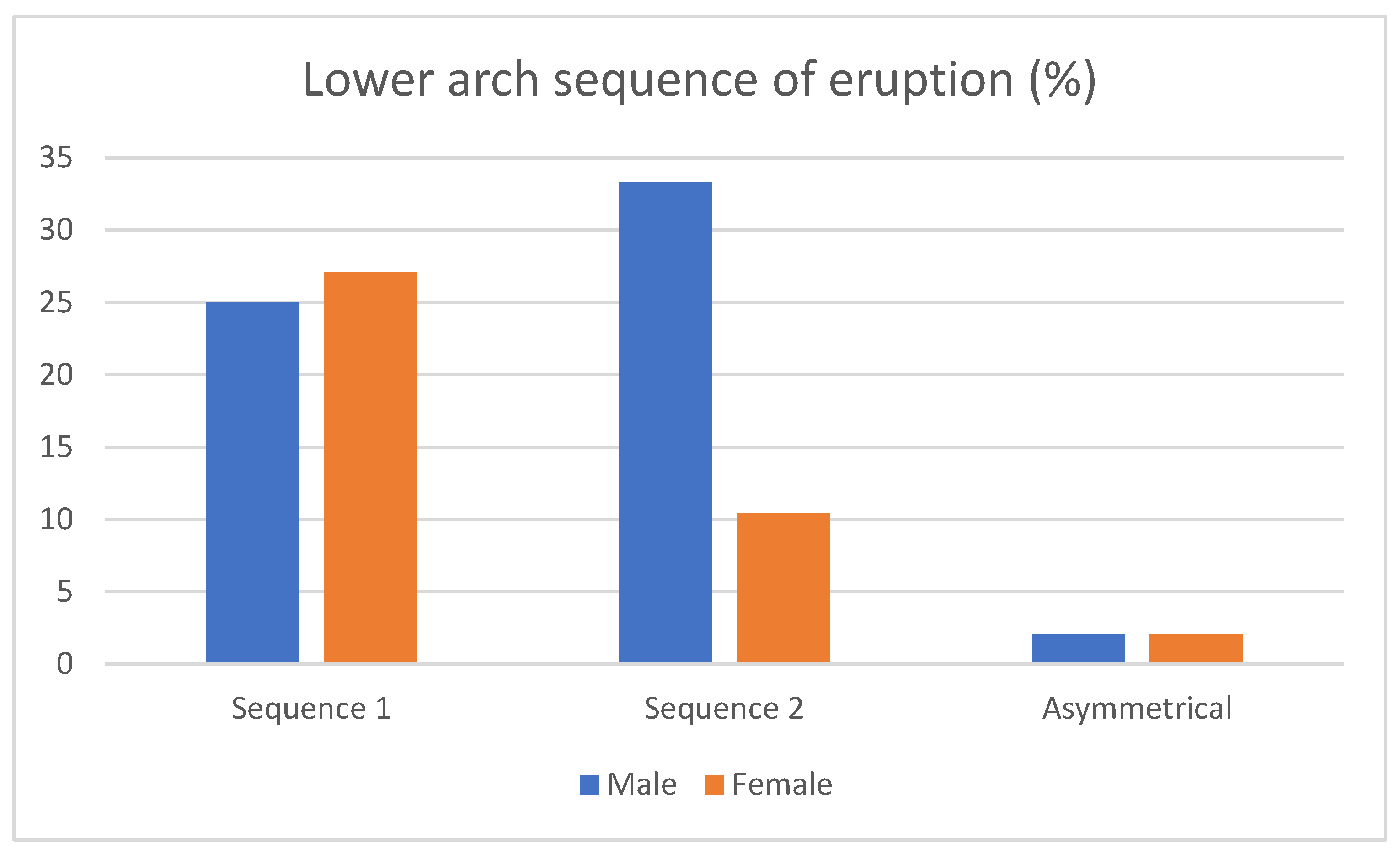
- Mandibular sequences: the prevalence of Seq3 (3_4) was 52.1%, whereas for Seq4 (4_3), it was 43.7%. Additionally, 4.2% of the patients showed asymmetrical sequences in the lower arch. On the one hand, 25% of men and 27.1% of women showed Seq3, and 33.3 % of men and 10.4% of women presented Seq4, leaving an equal distribution of asymmetrical patients (2.1 of men and 2.1 of women) (Figure 3). We found no difference between sexes for the mandibular sequences according to the Chi-square test (p = 0.153).Figure 3. Sex-related frequencies of lower eruption sequences.
![Children 10 00674 g003]()

- Maxillary sequences: Table 2 shows the comparisons for different outcomes between children with eruption sequences 1 and 2. The t-test showed non-significant differences for all outcomes. Intercanine width was slightly larger in the Seq 1 children (mean: 33.9 mm; SD: 2.85) than in Seq 2 (mean: 32.25 mm; SD: 2.82) (p = 0.052, almost significant).Table 2. Comparisons between upper eruption sequences, TS-ALD (tooth size- arch length discrepancy), arch dimensions, sagittal and vertical growth patterns, and incisor position and inclination. SD: standard deviation.Table 2. Comparisons between upper eruption sequences, TS-ALD (tooth size- arch length discrepancy), arch dimensions, sagittal and vertical growth patterns, and incisor position and inclination. SD: standard deviation.
Maxillary Arch Sequence 1 Sequence 2 Mean Difference (Diff.) 95% Confidence Interval of the Mean Diff. p Value Mean SD Mean SD Lower Upper Age (years) 11.56 1.25 11.29 1.42 0.28 −0.33 0.89 0.369 TS-ALD (mm) −1.16 4.63 −1.88 4.75 0.72 −1.45 2.88 0.511 Tooh size_5_4_3 (right) (mm) 22.22 1.83 21.99 2.10 0.23 −0.67 1.12 0.618 Tooh size_21_12 (mm) 31.15 2.45 31.05 2.73 0.10 −1.09 1.28 0.871 Tooh size_3_4_5 (left) (mm) 22.48 2.30 21.89 2.08 0.59 −0.42 1.60 0.251 Total arch space (mm) 74.50 4.32 73.11 4.90 1.38 −0.72 3.49 0.195 Space_5_4_3 (right) (mm) 21.94 2.20 21.16 2.49 0.78 −0.29 1.85 0.152 Space_21_12 (mm) 31.43 2.14 31.96 2.30 −0.53 −1.55 0.48 0.298 Space_3_4_5 (left) (mm) 21.31 2.31 20.68 2.55 0.63 −0.48 1.74 0.262 Anterior arch length (mm) 14.07 1.96 13.97 2.57 0.11 −0.93 1.14 0.837 Posterior arch length (mm) 25.83 2.73 25.31 1.35 0.51 −0.50 1.53 0.314 Total arch length (mm) 39.89 3.12 39.28 2.84 0.61 −0.76 1.98 0.378 Intermolar width (mm) 45.64 2.54 44.74 3.08 0.90 −0.39 2.18 0.169 Intercanine width (mm) 33.90 2.85 32.25 2.82 1.65 −0.02 3.32 0.052 Inclination upper incisor_NA (°) 24.89 6.39 22.24 6.68 2.65 −0.35 5.64 0.082 Distance upper incisor_NA (mm) 5.52 2.36 4.47 2.38 1.05 −0.04 2.13 0.059 ANB angle (°) 2.96 2.49 3.86 2.23 −0.89 −1.98 0.20 0.106 Witts (mm) −1.56 2.99 −0.80 3.30 −0.76 −2.20 0.68 0.297 Mandibular plane angle(°) 25.24 7.22 24.49 4.21 0.76 −2.00 3.52 0.586 Lower facial height (°) 44.44 5.27 45.21 3.73 −0.78 −2.90 1.35 0.469

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
- Maxillary eruption sequences and categorized TS-ALD: A Chi-square test was used to compare the two upper eruption sequences between children with negative TS-ALD and children with positive or zero TS-ALD. No significant differences were found (p = 0.161).
- Mandibular sequences: Table 3 shows the comparisons for different outcomes between children with eruption sequences 3 and 4. The t-test showed non-significant differences for all outcomes.Table 3. Comparisons between lower eruption sequences, TS-ALD (tooth size- arch length discrepancy), arch dimensions, sagittal and vertical growth patterns, and incisor position and inclination. SD: standard deviation.Table 3. Comparisons between lower eruption sequences, TS-ALD (tooth size- arch length discrepancy), arch dimensions, sagittal and vertical growth patterns, and incisor position and inclination. SD: standard deviation.
Mandibular Arch Sequence 3 Sequence 4 Mean Difference (Diff.) 95% Confidence Interval of the Mean Diff. p Value Mean SD Mean SD Lower Upper Age (years) 11.40 1.41 10.76 1.60 0.65 −0.25 1.54 0.152 TS-ALD (mm) −0.15 4.43 0.22 3.34 −0.37 −2.74 2.00 0.754 Tooh size_5_4_3 (right) (mm) 21.96 2.04 21.98 1.01 −0.01 −1.00 0.97 0.98 Tooh size_21_12 (mm) 23.15 1.38 22.65 2.72 0.50 −0.75 1.76 0.421 Tooh size_3_4_5 (left) (mm) 21.96 2.07 21.87 1.09 0.10 −0.92 1.11 0.847 Total arch space (mm) 66.80 3.33 66.72 4.08 0.07 −2.13 2.27 0.948 Space_5_4_3 (right) (mm) 22.04 1.73 21.97 2.61 0.06 −1.23 1.36 0.921 Space_21_12 (mm) 22.32 1.25 22.41 1.66 −0.09 −0.96 0.77 0.829 Space_3_4_5 (left) (mm) 22.60 1.65 22.10 2.09 0.50 −0.61 1.61 0.365 Anterior arch length (mm) 8.70 2.07 8.92 2.27 −0.23 −1.52 1.06 0.724 Posterior arch length (mm) 27.03 1.96 26.36 2.29 0.67 −0.59 1.93 0.29 Total arch length (mm) 35.72 2.54 35.28 2.38 0.45 −1.02 1.92 0.543 Intermolar width (mm) 37.25 6.75 38.32 4.76 −1.07 −4.53 2.40 0.538 Intercanine width (mm) 25.63 1.52 25.46 1.99 0.17 −1.06 1.39 0.784 Inclination lower incisor_NB (°) 24.96 5.09 25.29 4.64 −0.33 −3.24 2.59 0.823 Distance lower incisor_NB(mm) 5.20 2.22 4.64 1.93 0.56 −0.69 1.81 0.373 ANB angle (°) 3.42 2.00 4.31 1.67 −0.89 −2.00 0.22 0.113 Witts (mm) −1.54 3.29 −0.48 2.72 −1.06 −2.88 0.75 0.244 Mandibular plane angle(°) 27.40 8.07 24.52 4.55 2.88 −1.12 6.88 0.154 Lower facial height (°) 46.30 6.10 44.67 3.94 1.63 −1.49 4.75 0.297
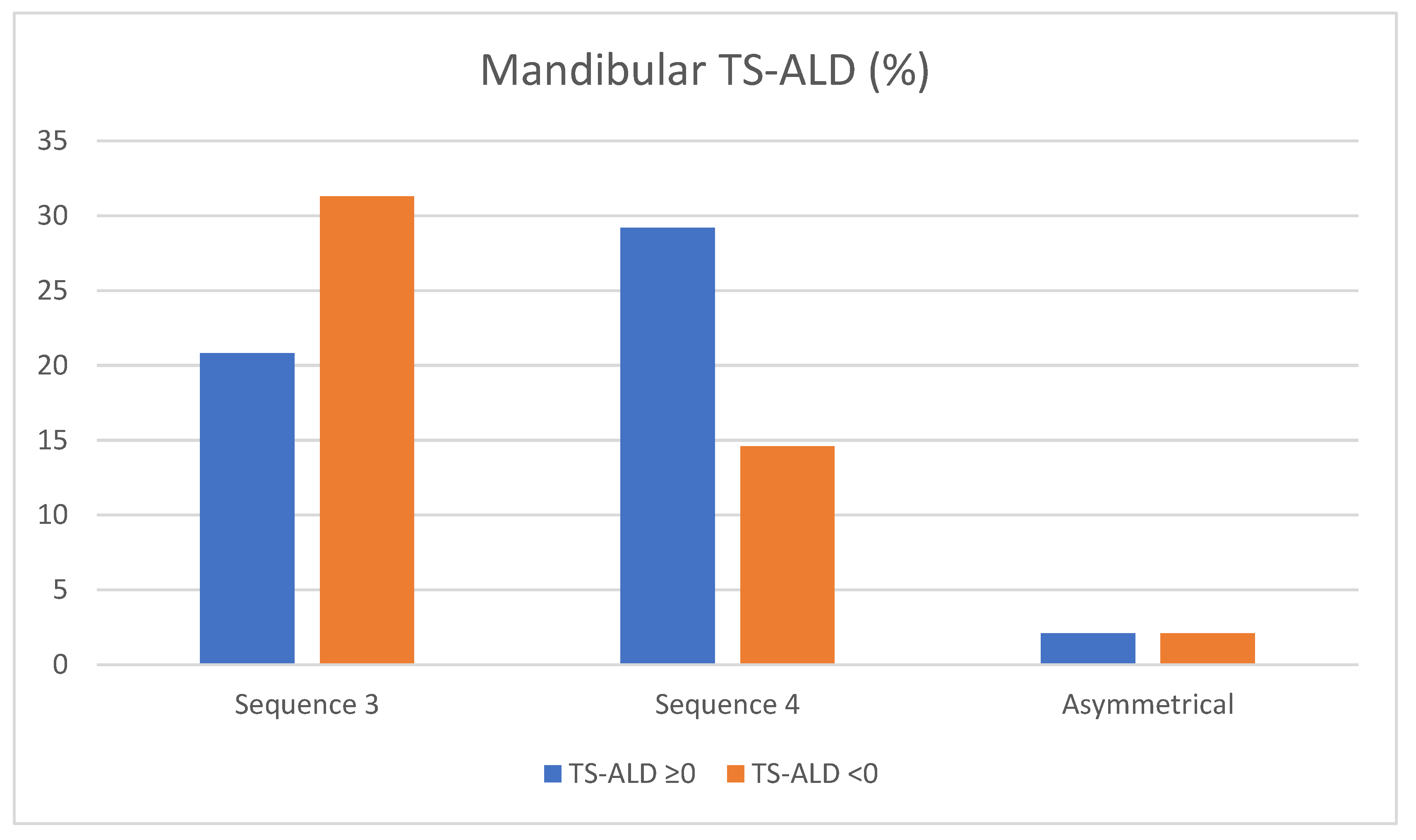
- Mandibular sequence and categorized TS-ALD: In order to compare the two lower eruption sequences between children with negative TS-ALD and children with positive or zero TS-ALD, a Chi-square test was used. There were no significant differences (p = 0.196).
3.3. Gender-Specific Analysis of TS-ALD, Arch Dimensions, Sagittal and Vertical Growth Patterns, and Incisor Position and Inclination
3.4. Bivariate Correlations (Pearson’s Correlation Coefficient)
4. Discussion
4.1. Sequence of Eruption
4.2. Gender
4.3. Arch Dimensions
4.4. Incisors Inclination and Position
4.5. Sagittal Skeletal Relationship
4.6. Vertical Growth Pattern
5. Conclusions
- In our study, eruption sequences 1 and 2 in the maxilla and 3 and 4 in the mandible were equally prevalent.
- Males and females showed similar eruption sequences both in the maxilla and in the mandible.
- Maxillary crowding occurred more frequently during eruption sequences 3-5 (Seq1), but the lack of space was evident in both maxillary sequences. There was more crowding in the mandible when the eruption sequence was 3-4 (Seq3), whereas diastemas and no space problems were prevalent when the eruption sequence was 4-3 (Seq4).
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Janson, G.; Goizueta, O.E.; Garib, D.G.; Janson, M. Relationship between maxillary and mandibular base lengths and dental crowding in patients with complete Class II malocclusions. Angle Orthod. 2011, 81, 217–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faruqui, S.; Frida, M.; Shaikh, A. Comparison of tooth and arch dimensions in dental crowding and spacing. Pak. Orthod. J. 2012, 4, 48–55. [Google Scholar]
- Crossley, A.M.; Campbell, P.M.; Tadlock, L.P.; Schneiderman, E.; Buschang, P.H. Is there a relationship between dental crowding and the size of the maxillary or mandibular apical base? Angle Orthod. 2020, 90, 216–223. [Google Scholar] [CrossRef] [Green Version]
- Normando, D.; Almeida, M.A.; Quintao, C.C. Dental crowding: The role of genetics and tooth wear. Angle Orthod. 2013, 83, 10–15. [Google Scholar] [CrossRef] [PubMed]
- González, A.M.G.; Rodríguez, L.L.V. Prevalence, types and etiologic factors of mandibular crowding in orthodontic patients in Tabasco, Mexico, 2015–2016. Rev. Mex. Ortod. 2018, 6, 22–27. [Google Scholar]
- Alhammadi, M.S.; Halboub, E.; Fayed, M.S.; Labib, A.; El-Saaidi, C. Global distribution of malocclusion traits: A systematic review. Dent. Press J. Orthod. 2018, 23, 40.e1–40.e10. [Google Scholar] [CrossRef]
- Lombardo, G.; Vena, F.; Negri, P.; Pagano, S.; Barilotti, C.; Paglia, L.; Colombo, S.; Orso, M.; Cianetti, S. Worldwide prevalence of malocclusion in the different stages of dentition: A systematic review and meta-analysis. Eur. J. Paediatr. Dent. 2020, 21, 115–122. [Google Scholar] [CrossRef]
- Bell, R.A.; Sonis, A. Space supervision and guidance of eruption in management of lower transitional crowding: A non-extraction approach. Semin. Orthod. 2014, 20, 16–35. [Google Scholar] [CrossRef]
- Bernabe, E.; del Castillo, C.E.; Flores-Mir, C. Intra-arch occlusal indicators of crowding in the permanent dentition. Am. J. Orthod. Dentofac. Orthop. 2005, 128, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Bishara, S.E.; Khadivi, P.; Jakobsen, J.R. Changes in tooth size-arch length relationships from the deciduous to the permanent dentition: A longitudinal study. Am. J. Orthod. Dentofac. Orthop. 1995, 108, 607–613. [Google Scholar] [CrossRef]
- Abid, A.M.; Mahmood, A.; Hussain, A.; Rafi, S. The correlation between lower incisor crowding and arch length discrepancy (ALD). Pak. Orthod. J. 2012, 8, 56–62. [Google Scholar]
- Allen, T.R.; Trojan, T.M.; Harris, E.F. Evidence favoring a secular reduction in mandibular leeway space. Angle Orthod. 2017, 87, 576–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berg, R. Crowding of the dental arches: A longitudinal study of the age period between 6 and 12 years. Eur. J. Orthod. 1986, 8, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Sampson, W.J.; Richards, L.C. Prediction of mandibular incisor and canine crowding changes in the mixed dentition. Am. J. Orthod. 1985, 88, 47–63. [Google Scholar] [CrossRef] [PubMed]
- Leighton, B.C.; Hunter, W.S. Relationship between lower arch spacing/crowding and facial height and depth. Am. J. Orthod. 1982, 82, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Alhadlaq, A. Anterior alveolar dimensions among different classifications of sagittal jaw relationship in Saudi subjects. Saudi Dent. J. 2010, 22, 69–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. PLoS Med. 2007, 4, e296. [Google Scholar] [CrossRef] [Green Version]
- Pourhoseingholi, M.A.; Vahedi, M.; Rahimzadeh, M. Sample size calculation in medical studies. Gastroenterol. Hepatol. Bed Bench 2013, 6, 14–17. [Google Scholar]
- Sharma, P.S.; Brown, R.V. The arch-length of the mixed dentition. An aid to diagnosis. Br. Dent. J. 1967, 123, 98–102. [Google Scholar]
- Moshkelgosha, V.; Khosravifard, N.; Golkari, A. Tooth eruption sequence and dental crowding: A case-control study. F1000Res 2014, 3, 122. [Google Scholar] [CrossRef]
- Padma Kumari, B.; Retnakumari, N. Loss of space and changes in the dental arch after premature loss of the lower primary molar: A longitudinal study. J Indian Soc. Pedod. Prev. Dent. 2006, 24, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Hoffding, J.; Maeda, M.; Yamaguchi, K.; Tsuji, H.; Kuwabara, S.; Nohara, Y.; Yoshida, S. Emergence of permanent teeth and onset of dental stages in Japanese children. Community Dent. Oral Epidemiol. 1984, 12, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Savara, B.S.; Steen, J.C. Timing and sequence of eruption of permanent teeth in a longitudinal sample of children from Oregon. J. Am. Dent. Assoc. 1978, 97, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.S.; Nagar, P.; Singh, P.; Bharti, M. Changes in the Sequence of Eruption of Permanent Teeth; Correlation between Chronological and Dental Age and Effects of Body Mass Index of 5-15-year-old Schoolchildren. Int. J. Clin. Pediatr. Dent. 2020, 13, 368–380. [Google Scholar] [CrossRef]
- Selmani, M.; Gjorgova, J. Relationship among lower arch length, arch width and arch perimeter in crowding and non-crowding groups. Balk. J. Dent. Med. 2015, 19, 8–12. [Google Scholar] [CrossRef] [Green Version]
- Ikoma, M.; Arai, K. Craniofacial morphology in women with Class I occlusion and severe maxillary anterior crowding. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 36–45. [Google Scholar] [CrossRef] [Green Version]
- Turkkahraman, H.; Sayin, M.O. Relationship between mandibular anterior crowding and lateral dentofacial morphology in the early mixed dentition. Angle Orthod. 2004, 74, 759–764. [Google Scholar] [CrossRef]
- Fernandez, C.C.A.; Pereira, C.; Luiz, R.R.; Vieira, A.R.; De Castro Costa, M. Dental anomalies in different growth and skeletal malocclusion patterns. Angle Orthod. 2018, 88, 195–201. [Google Scholar] [CrossRef] [Green Version]
- Sardarian, A.; Ghaderi, F. Prediction of the occurrence and severity of mandibular incisor crowding in the early mixed dentition using craniofacial parameters. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 701–707. [Google Scholar] [CrossRef]
- Richardson, M.E. Late lower arch crowding in relation to skeletal and dental morphology and growth changes. Br. J. Orthod. 1996, 23, 249–254. [Google Scholar] [CrossRef]
- Siecola, G.S.; Capelozza, L.F.; Lorenzoni, D.C.; Janson, G.; Henriques, J.F.C. Subjective facial analysis and its correlation with dental relationships. Dent. Press J. Orthod. 2017, 22, 87–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lupacheva, N.V. Orthodontic status and head morphology in young males. J. Physiol. Anthr. 2007, 26, 387–402. [Google Scholar] [CrossRef] [PubMed]



| Sequence (Seq) of eruption |
|
| Sex |
|
| Age (years) | |
| TS-ALD (tooth size—arch length discrepancy) (mm) |
|
| Tooth size (mm) |
|
| Available space in the arch (mm) |
|
| Arch length (mm) |
|
| Intermolar width (mm) |
|
| Intercanine width (mm) |
|
| Incisor inclination (°) (according to Steiner cephalometric analysis) |
|
| Incisor distance (mm) (according to Steiner cephalometric analysis) |
|
| Sagittal skeletal relationship (from Steiner and Wits cephalometric analysis) |
|
| Growth pattern (°) (from Ricketts cephalometric studies) |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Gil, M.; Alarcón, J.A.; Cacho, A.; Yañez-Vico, R.; Palma-Fernández, J.C.; Martin, C. Association between Eruption Sequence of Posterior Teeth, Dental Crowding, Arch Dimensions, Incisor Inclination, and Skeletal Growth Pattern. Children 2023, 10, 674. https://doi.org/10.3390/children10040674
García-Gil M, Alarcón JA, Cacho A, Yañez-Vico R, Palma-Fernández JC, Martin C. Association between Eruption Sequence of Posterior Teeth, Dental Crowding, Arch Dimensions, Incisor Inclination, and Skeletal Growth Pattern. Children. 2023; 10(4):674. https://doi.org/10.3390/children10040674
Chicago/Turabian StyleGarcía-Gil, Marta, José Antonio Alarcón, Alberto Cacho, Rosa Yañez-Vico, Juan C. Palma-Fernández, and Conchita Martin. 2023. "Association between Eruption Sequence of Posterior Teeth, Dental Crowding, Arch Dimensions, Incisor Inclination, and Skeletal Growth Pattern" Children 10, no. 4: 674. https://doi.org/10.3390/children10040674