
Pain during Rapid Maxillary Expansion: A Systematic Review
by
 ,
,
Martina Barone
1,
Alberto De Stefani
1,2 ,
,
Filippo Cavallari
3,
Antonio Gracco
1,† and 
Giovanni Bruno
1,4,*,†
1
Department of Neuroscience, School of Dentistry, University of Padova, 35122 Padova, Italy
2
Department of Pharmacological Sciences, University of Padova, 35122 Padova, Italy
3
Azienda Ospedaliera di Padova, 35122 Padova, Italy
4
Department of Industrial Engineering, University of Roma Tor Vergata, 00133 Roma, Italy
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Children 2023, 10(4), 666; https://doi.org/10.3390/children10040666
Submission received: 13 February 2023
/
Revised: 20 March 2023
/
Accepted: 27 March 2023
/
Published: 31 March 2023
(This article belongs to the Special Issue 10th Anniversary of Children: Pediatric Dentistry Progress)
Abstract
:Aim: The aim of the present systematic review is to evaluate the pain perceived by patients during rapid maxillary expansion (RME) in relation to factors such as demographic characteristics, appliance type, activation protocol, and the eventual use of medication or pain management strategies. Materials and methods: An electronic search of available articles on the subject was conducted on three electronic databases, using predefined keywords. Sequential screenings based on pre-established eligibility criteria were performed. Results: Ten studies were ultimately included in this systematic review. The main data of the reviewed studies were extracted according to the PICOS approach. Conclusions: Pain is a common effect of RME treatment that tends to decrease over time. Gender and age differences in pain perception are not clear. Perceived pain is influenced by the expander design and expansion protocol used. Some pain management strategies can be useful for reducing RME-associated pain.
1. Background
Rapid maxillary expansion (RME) is an orthodontic–orthopedic treatment routinely performed worldwide in growing subjects with transversal deficiency of the maxillary arch, with or without a crossbite [1,2,3,4]. This treatment can be performed in primary, mixed, or permanent dentition [1,5,6].
According to Baccetti et al. [7], while an RME performed before the peak of pubertal growth leads to significant and more effective long-term skeletal changes in maxillary and circum-maxillary structures, the same treatment performed after the peak tends to have greater effects at the dentoalveolar level than at the skeletal one. This is due to the different mid-palatal suture maturation stages that can be observed in various age ranges: in the ‘‘infantile’’ stage (<10 years), the suture is broad and smooth; in the ‘‘juvenile’’ stage (10–13 years), it appears with a more typical squamous aspect, with overlapping sections; and in the ‘‘adolescent’’ stage (13–14 years), the suture is wavier, with increased interdigitation [7,8].
The type of appliance used for RME treatment can include a dental, skeletal, or dento-skeletal anchorage. However, the rationale for the appliance is always the same: to separate the mid-palatal suture [9,10,11]. Therefore, RME requires the use of heavy dentofacial orthopedic forces, to produce skeletal effects by minimizing the unwanted dental ones, such as molar tipping and alveolar bending [1,10]. The expansion protocol chosen by the clinician generally prescribes one to three activations per day, for a period ranging from approximately two to four weeks [1,10].
Patients often report having pain or discomfort during the active phase of RME [3,5], especially during the first activations. The literature suggests that pain is the most commonly reported symptom, with a frequency of >90% among children [2,12].
The purpose of this systematic review of the literature is to evaluate the pain perception reported by patients during RME in relation to factors such as age, gender, appliance type, activation protocol, and the eventual use of medication or pain control strategies.
2. Materials and Methods
The PRISMA (preferred reporting items for systematic reviews and meta-analyses) guidelines [13,14] were followed for the present systematic review of the existing literature. This review protocol was registered on the International Prospective Register of Systematic Reviews (PROSPERO; registration number: CRD42023403349).
The focused PICOS question pursued by the authors in this systematic literature review was: “Is the pain experienced by patients during rapid maxillary expansion (RME) related to factors such as demographic characteristics, appliance design, activation protocol, and/or the use of any medication or strategy to control the pain?”.
A search of the electronic databases PubMed, Scopus, and Web of Science was conducted in October 2022. The keywords used by the researchers were: “pain,” “rapid palatal expansion,” and “rapid maxillary expansion.” The same keywords were used in all three of the databases, and no filters were set.
2.1. Selection of Studies
After the removal of duplicate results, the study selection phase was performed based on pre-established eligibility criteria.
Automation tools were not used for the study selection process. Instead, two authors independently performed an accurate analysis of the titles and abstracts of the articles that emerged from the research on the electronic databases. To calibrate inter-examiner reproducibility, the following method was used: in case of disagreement regarding the inclusion of a study, the two authors discussed and reached a mutual consensus before coming to a final decision.
The selection process was based on the type of article (publications as reviews, meta-analysis, letters, comments, case reports/series, surveys not on human were not included), the language (only articles in English were included), the age of the study sample (articles in which the study sample presented a mean age higher than 13 years or in which an age range over 13 years was evaluated were excluded), the availability of the abstract and/or the full-text article (if those were not available, the study was excluded), and the article’s relevance to the aim of the present systematic review (the studies whose aims were not relevant to those of the review were excluded). For articles that met a combination of inclusion and exclusion criteria, a full-text analysis was performed before selecting those to be included and reviewed in this investigation.
2.2. Data Extraction
The characteristics and main data of the included studies were extracted according to the PICOS approach:
P (patients/problem/population): patients aged up to 13 years being treated with rapid maxillary expansion.
I (intervention): rapid maxillary expansion.
C (comparison): if a comparison was done.
O (outcome): pain.
S (study design): randomized clinical trials and observational analytical studies, though only studies with human participants.
Relevant data from each included article were collected and organized in a table (Microsoft® Office 365® Excel). No automation tools were used for the data collection process.
2.3. Study Quality Assessment
The articles included in the full-text analysis were evaluated for their quality based on methodological quality criteria adapted from the CONSORT statement, the Jadad quality assessment scale, and previous studies (Table 1) [4].
Two reviewers independently scored each study; disagreement in the scoring was solved with discussion and, if necessary, consultation with a third author. The total possible score for each article was 11 points, and studies were classified as follows: good, with a total of >9 points; moderate, with 7–9 points; and poor, with <7 points.
3. Results
3.1. Study Selection
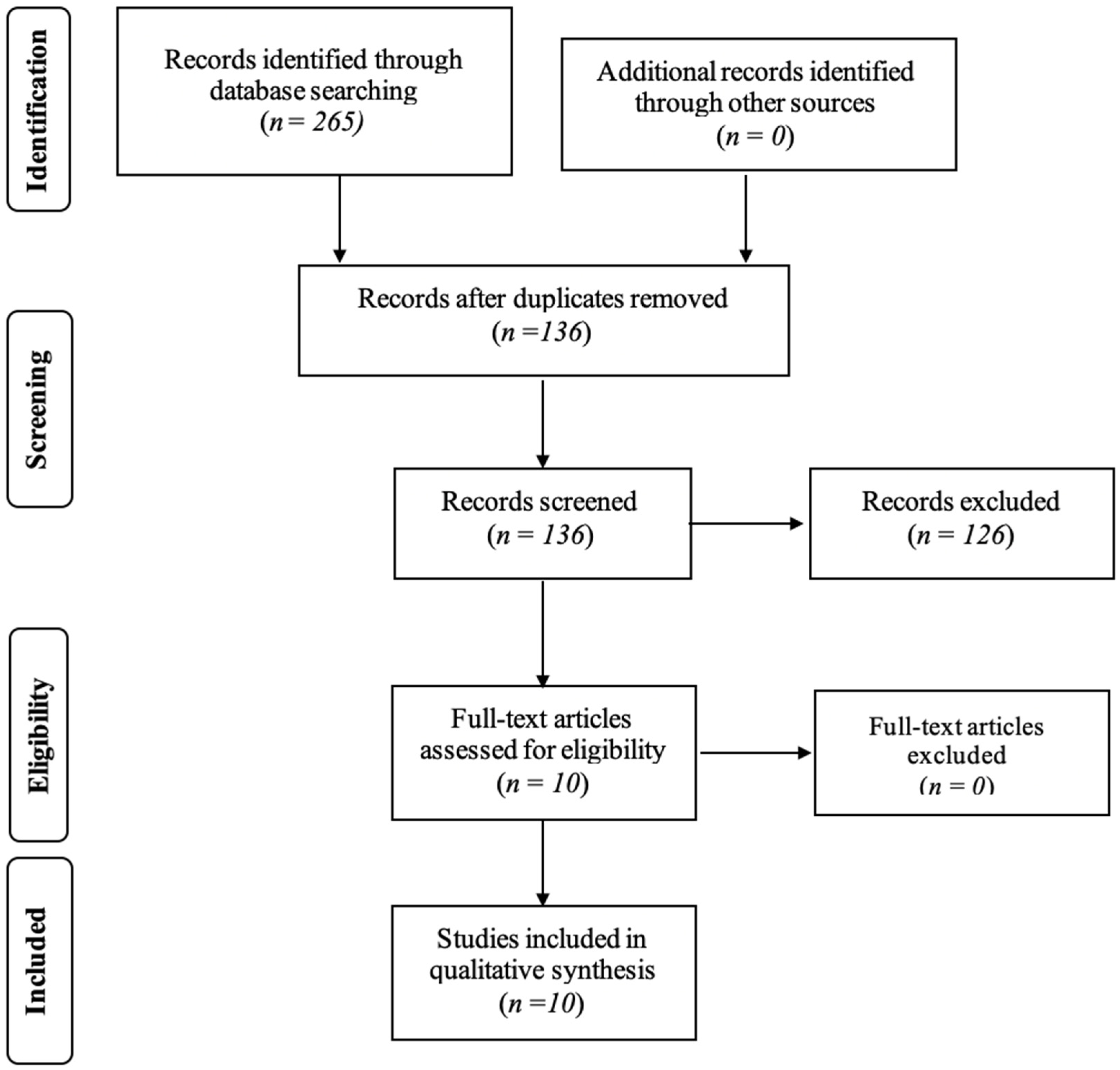
The research conducted on the PubMed, Scopus, and Web of Science databases led to a total of 265 articles (83 on PubMed, 97 on Scopus, and 85 on Web of Science). After the process of removing duplicates, a title and abstract analysis was performed for 136 articles. This process led to the exclusion of another 126 articles. Ten studies were included in the full-text analysis, and all of them were then included in the final systematic review.
Figure 1 shows the study selection phase. The figure describes the number of studies that were identified, screened, deemed eligible, and ultimately included in the present review.
3.2. Study Characteristics
Table 2 and Table 3 summarize the main data collected from analysis of the studies included in the present systematic review. It must be specified that, for the aim of the present review, only the portion of the included studies concerning RME-associated pain and the relevant reported data were considered. These extracted data are reported in Table 1.
The most recent study included was published in 2022 by Caccianiga et al. [2], while the oldest one was published in 2000 by Needleman et al. [10]. Regarding study design, five studies were randomized clinical trials [2,12,15,16,17], one was a prospective study [3], one was a parallel cohort study [1], and one was divided into two phases, the first of which was a randomized, controlled clinical trial and the second of which was a prospective case series (The authors decided to include the second part of this study in the review too because, although it was defined as a prospective case series, a statistical analysis of the data was still performed) [9]. For two studies, the study design was not clearly defined by the authors [5,10].
Pain level was assessed in the included studies using different scales. Some studies used a single scale, while others utilized two scales to measure pain in their study sample. The scales used were of five types:
The Wong–Baker Faces Pain Scale (FPS) was used in five studies [1,3,10,12,15], while one study utilized a revised FPS [5].
The Graphic Rating Scale (GRS) was used in one study [1].
The Color Analog Scale (CAS) was used in one study [10].
In the majority of the included studies, patients registered their pain daily after each activation of the appliance during the active phase of the maxillary expansion, according to the activation protocol used.
3.3. Quality Assessment of the Selected Studies
Table 4 shows the evaluation of the methodological quality of the studies included in this systematic review.
4. Discussion
Rapid maxillary expansion is a procedure that is widely and routinely performed in cases of maxillary contraction, with the aim to correct transverse discrepancy and normalize the transverse relationship between the upper and lower dental arches. A common side effect is the pain associated with the active expansion phase, during which one or more appliance screw activations are performed in order to open the mid-palatal suture.
The present systematic review of the literature aims to evaluate the pain perceived during rapid maxillary expansion in relation to age, gender, appliance type, activation protocol, and the eventual strategies of pain management used.
In all of the included studies, patients reported some pain. The pain appeared to be higher during the first days of treatment (usually within the first weeks) or the first screw activations, decreasing as treatment progressed. This data is in agreement with the literature [6,11,16,18].
4.1. Pain and Gender
Not all of the included studies provided information about the difference in pain perception during RME between the two sexes. Some studies [5,10,15] described the absence of a statistically significant difference between the two sexes in reported pain. However, de Araújo et al. [3] reported higher pain levels in females than in males during RME treatment, while Feldman et al. [17] reported that females complained of more dental tension than males, even if with minimal differences. Cesur et al. [5] focused on the level of pain at different dental arch sectors, and reported significantly lower pain levels in males in the posterior teeth area on the sixth day of expansion compared to the first and second days.
These findings reflect the existing literature, there is an absence of agreement on whether pain perception may or may not be influenced by gender. While some studies report the absence of a difference between the sexes, some others report that females appear to be more sensitive to pain [6,11,16,18].
4.2. Pain and Age
The authors of this article decided to exclude from the review studies that had sample populations with a mean age or age range higher than 13 years old. The aim of this study is to evaluate pain perception during RME only in children and pre-teens, since this population constitutes the age at which this procedure is more frequently executed. Since pain perception could be different in adults versus children/pre-teens, these exclusion criteria reduce the possible bias a wider age range could introduce.
Not all of the included studies provided information about the difference in pain perception at different ages. Needleman et al. described the absence of a statistically significant difference in reported pain according to patient age, or between expansion rate and age. According to the study by Feldman et al., age was positively correlated with overall pain and discomfort on the fourth day of treatment. In the study by Matos et al. it was observed that younger patients tended to experience less pain; specifically, 7-year-old children experienced less pain than 11-year-olds.
Therefore, based on the literature [16], it is not clear whether or not age influences the perception of pain.
4.3. Pain and Type of Expander Used
Some studies compared the influence of different RME appliance types on pain perception reported by patients.
De Araujo et al. [3] compared two types of traditional maxillary expanders, Hyrax and Haas appliances, and reported significantly higher pain after 1 day of therapy in patients treated with the Hyrax expander. However, with the exception of the first treatment day, the authors concluded that the type of appliance used did not significantly influence the perception of pain consequent to RME. The expander design could explain the higher pain level reported during the first day of activation by the patients treated with the Hyrax appliance. In fact, the two types of expanders are both anchored to the tooth with cemented bands, but in the Hyrax appliance the screw is connected to the bands only with a rigid stainless-steel structure, while in the Haas appliance there are also two acrylic pads connected to the stainless-steel structure and rested on the palate. Thus, if the Hyrax transmits the forces only to the periodontium of the supporting teeth, the Haas distributes them to the palate and buccal bone plate areas too [3,19].
Two included studies compared tooth-borne with tooth–bone/bone-borne RME appliances. Feldmann et al. [17] did not find statistically significant differences between the two groups in terms of pain, although patients with tooth-borne RME appliances generally reported higher pain levels than those with tooth–bone-borne RME appliances. In the opinion of the authors of the study, this could be explained by the fact that the center of the force generated by the screw activation is closer to the mid-palatal suture in tooth–bone-borne RME appliances, because of the skeletal anchorage, so the quantity of force distributed to the dentition could be reduced and attenuated, resulting in less pain experienced by the patient. Conversely, in the study by Altieri et al. [1], patients with bone-borne RME devices reported statistically significant higher pain levels during the first day of activation compared to those with tooth-borne RME expanders. They did not show statistically significant differences on subsequent days, even if patients with bone-borne RME appliances generally reported higher pain levels. According to the authors, the pain during the first day could have been partly caused by the insertion of miniscrews.
Therefore, in the studies included in the present review there was not a clear agreement on the role of anchorage type (i.e., dental vs skeletal/dento-skeletal) in pain associated with RME.
Two of the included studies [12,16] compared the traditional RME appliance with the Leaf expander (LE), which is made up of a shape memory double nickel–titanium leaf spring. The rationale of the shape memory leaf spring is to apply continuous force that, along with the superelastic property of the nickel–titanium, leads to a more physiologic, calibrated, and comfortable expansion for the patient with the LE compared to one with a traditional RME expander [12,20,21]. The forces transmitted to the bone and sutural complex appear decreased thanks to the slow and continuous activation performed by the LE, causing a consequent inhibition of the tissues’ inflammatory response, which clinically results in reduced pain perception for the patient during the appliance activation [12,22]. Both of the studies reported a statistically significant decrease in pain in patients treated with LE, in the first 4 days according to Ugolini et al. and in the first week according to Nieri et al. Thereafter, pain tended to decrease in both groups in both studies, without other significant differences. However, Nieri et al. considered the difference between the LE and RME probably not clinically significant, since the difference in VAS score between the two studied groups was very small (i.e., 0.3 points).
4.4. Pain and Activation Protocol Used
Different activation protocols were used by authors in the included studies. For each study, the activation protocol described in Table 2 was maintained during the entire period of investigation. In all of the included studies, a certain level of pain was reported by patients, which is why it appeared difficult to define a relationship between pain reported and activation protocol used. In the study by Needleman et al., some patients were prescribed 1 activation/day while others were prescribed 2 activations/day, based on the individual preference of the treating orthodontist. It emerged that patients whose activation protocol was 2 activations/day were 2.1 times more likely to report pain than patients with an activation protocol of 1 activation/day (three times more for the first 10 activations). This finding accords with the literature; the type of activation protocol can influence the pain perceived during RME. Specifically, a slower activation protocol (i.e., less screw activation per day) is correlated with a lower pain level for the patient [6,11,23].
4.5. Pain and Strategy of Pain Management Used
In two of the included studies [2,15] the effect of photobiomodulation therapy (PBMT) on pain occurring during/after RME was evaluated. For the purpose of these studies, a control group not receiving PBMT was enrolled. PBMT uses low-powered laser light within the red-to-near-infrared range to achieve biological responses. Its likely capacity for orthodontic pain reduction is due to the inhibition of arachidonic acid release, with a consequent decrease of prostaglandin E levels, and to the induction of beta-endorphin release, which causes an efficient analgesic reaction [2]. The two studies had a similar sample size (34 [15] vs. 30 [2] patients), but the mean age of the sample was slightly lower in the Caccianiga et al. study. The type of laser used, as well as the protocol of irradiation, were different between the two studies: Caccianiga et al. utilized a laser for extraoral irradiation and only performed this on the day of expander positioning. Matos et al. performed the irradiation with an intraoral laser in the mid-palatal suture area, and patients received four irradiations during the active expansion phase (the first one at the expander positioning) and eight more irradiations after screw fixation (one per week for 8 weeks).
Caccianiga et al. found the laser to be efficient for alleviating pain intensity and reducing pain duration during the active RME phase. Pain scores reported by the patients were always significantly lower in the laser group at each detection than in the non-laser group. Conversely, Matos et al. reported a greater risk of experiencing high pain levels in the laser group than in the control group. It must be mentioned that in this study the control group was exposed to placebo irradiation; it is natural to wonder, therefore, if the placebo effect could have effected a greater action in terms of pain perception than the laser itself. However, this data was not statistically significant, and the authors of the study concluded that the laser had no effects in terms of painful sensation alleviation during the active phase of expansion.
It might come as a surprise that the study in which a statistically significant result was obtained for the management of RME-associated pain is the one by Caccianiga et al. In this study, the irradiation did not occur directly near the area of the mid-palatal suture (where the expander exerts its action), as instead an extraoral PBMT laser was used. These patients received the irradiation only once, on the day of appliance application (so even before the beginning of the active phase of expansion). Nevertheless, as explained by Caccianiga et al., the laser they used (ATP38®) allowed the simultaneous irradiation of all the circummaxillary sutures; this may have allowed the laser to exert a greater effect on the overall manifestation of pain, compared to a device acting only at the level of the mid-palatal suture.
Despite the fact that PBMT is a technology with various different applications in medicine and dentistry today [2,24,25], it is not available in all dental clinics, whether public or private. Therefore, even if it is useful to know its effects on RME-associated pain alleviation, PBMT cannot be considered a routine tool for this purpose. However, since it has no side effects, dental clinics that already use PBMT may find it useful for relieving pain in patients starting RME therapy.
With regard to pharmacological pain management, in some included studies the use of analgesic and/or anti-inflammatory drugs during the observation period was completely prohibited [2], prohibited without prescription [1], or allowed at one’s discretion (i.e., without indicating the type of medication or regimen) [3,12,17]. In the study by de Araújo et al., in which patients were treated with Hyrax- and Haas-type appliances, no analgesic use was declared, although 100% of them reported some pain during the expansion period. Ugolini et al. reported that the 25.2% of patients treated with traditional RME devices used analgesics, compared to 0% of patients treated with LEs. In the study by Feldmann et al., a low use of analgesics was reported by the patients of both studied groups (i.e., tooth-borne expanders and tooth–bone-borne expanders), without statistically significant differences between them; the most used analgesics by patients in this study were Paracetamol and Ibuprofen.
Needleman et al. reported how the 48% of studied patients used drugs at least once during the expansion phase, with no differences based on age or gender. Drugs were taken after 7% of activations and 69% of the time during the first six screw activations; no differences were reported during the last 10 days of appliance activation. The reported drugs were Tylenol® (i.e., Paracetamol), Advil® (i.e., Ibuprofen), and Motrin® (i.e., Ibuprofen).
The study by Cossellu et al. [9] was the only one which specifically analyzed the effects of the use of analgesic drugs on pain management during RME. In its first phase, the study compared the effect of 40 mg ketoprofen lysine salt (KLS) to that of 250 mg paracetamol/acetaminophen (P), by evaluating which of the two drugs was the most effective in pain reduction. Furthermore, the study evaluated whether the use of an analgesic during the first 3 days of appliance activation could be effective in significantly reducing pain from the first treatment day. Patients did not receive a pharmacological regimen prescription to follow: they were only asked to report if and on what day/s they used the indicated analgesics.
KLS appeared to be more effective than P, probably due to its anti-inflammatory as well as analgesic properties. In fact, KLS belongs to the class of drugs defined as NSAIDs, which block COX-1 and/or COX-2, whereas P blocks COX-3, which is only expressed in the brain and spinal cord. Therefore, while KLS acts across cell membranes and is able to produce effects that reduce local synthesis of PGs (i.e., molecules that enhance the transmission of painful stimuli and increase sensitivity to noxious stimuli), P acts only on the central nervous system, with minimal peripheral consequences [26,27,28]. Thus, KLS appears to be more effective for inhibiting the acute inflammation response caused by the vasodilation resulting from the orthopedic forces exerted by the maxillary expander [29].
The second phase of this study by Cossellu et al. showed that the use of KLS during the first 3 days of screw activation seemed to be even more effective at reducing pain from the first day, with patients reporting almost no pain for the whole active phase of RME. It should be mentioned that, as stated by the study authors themselves, patients treated with RME can have different perceptions of pain. Therefore, it’s possible that in this phase of the study, the KLS group might have been composed of patients who otherwise would not have needed analgesic—which could constitute a bias. Nevertheless, as all patients in the first phase of the study reported pain and the necessity for a medication to manage it, the authors believed that an analgesic should be suggested during the first day of RME.
4.6. Limitation and Future Suggestions
The sensation of pain is complex; pain perception, as well as individual tolerance level, can vary between different subjects [6]. It therefore appears difficult to objectively quantify pain. A limit of the present systematic review is that in all the included studies pain was subjectively evaluated using questionnaires, thus only the pain as reported by patients was considered; it was not measured with any dedicated, appropriate device. In fact, individual levels of pain perception and tolerance can cause subjects with the same objective degree of pain to subjectively declare different levels of pain on the same pain scale. For a more precise and objective pain assessment and to reduce the risk of subjective-perception-related bias, studies in which pain assessment is objectively performed with proper devices would be needed. However, it appears that this type of study could be very difficult to achieve.
Another limitation of this review is that none of the included studies evaluating the use of analgesics for the management of RME-associated pain indicated a clear pharmacological regimen to follow. Future studies evaluating the efficacy of different types of analgesic and/or anti-inflammatory drugs, with a regimen defined by clinicians, would be interesting and useful for identifying the most effective drug types and respective dosages for controlling RME-associated pain. Such a study might also be able to define a standardized pharmacological protocol that all orthodontists could prescribe to their patients.
5. Conclusions
Pain is a common effect of RME treatment, which tends to occur during the first few days/activations and then decrease over time.
No clear difference in perceived pain was observed between different ages or genders.
Expander design may affect perceived pain: Haas and LE appliances appear to result in a lower patient pain levels, though there is no clear agreement about appliances with dental vs skeletal/dentoskeletal anchorage.
A slower expansion protocol (i.e., fewer screw activations per day) correlates with less pain perceived by the patient.
Extraoral PBMT can be a useful adjunct in the management of RME-associated pain.
KLS seems to be the most valid drug option for reducing and preventing RME-associated pain, thanks to its analgesic and anti-inflammatory properties.
Author Contributions
Conceptualization, M.B.; methodology, M.B., G.B. and A.D.S.; investigation, M.B. and F.C.; data curation, M.B. and F.C.; writing—original draft preparation, M.B. and F.C.; writing—review and editing, G.B. and A.D.S.; supervision, A.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
All of the authors declare that they have no conflict of interest.
References
- Altieri, F.; Cassetta, M. The impact of tooth-borne vs computer-guided bone-borne rapid maxillary expansion on pain and oral health–related quality of life: A parallel cohort study. Am. J. Orthod. Dentofac. Orthop. 2020, 158, e83–e90. [Google Scholar] [CrossRef] [PubMed]
- Caccianiga, G.; Caccianiga, P.; Baldoni, M.; Lo Giudice, A.; Perillo, L.; Moretti, N.; Ceraulo, S. Pain Reduction during Rapid Palatal Expansion Due to LED Photobiomodulation Irradiation: A Randomized Clinical Trial. Life 2021, 12, 37. [Google Scholar] [CrossRef] [PubMed]
- de Araújo, M.C.; Bocato, J.R.; Berger, S.B.; Oltramari, P.V.P.; de Castro Ferreira Conti, A.C.; de Almeida, M.R.; Freire Fernandes, T.M. Perceived pain during rapid maxillary expansion in children with different expanders. Angle Orthod. 2021, 91, 484–489. [Google Scholar] [CrossRef]
- De Stefani, A.; Bruno, G.; Visentin, S.; Lucchi, P.; Gracco, A. Rapid maxillary expansion for interceptive orthodontic treatment of palatally displaced canine: A systematic review. Eur. J. Paediatr. Dent. 2021, 22, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Geçgelen Cesur, M.; Aksoy, A. Evaluation of Perceived Pain During the First Week of Rapid Maxillary Expansion Treatment. Meandros 2018, 19, 39–44. [Google Scholar] [CrossRef]
- Baldini, A.; Nota, A.; Santariello, C.; Assi, V.; Ballanti, F.; Cozza, P. Influence of activation protocol on perceived pain during rapid maxillary expansion. Angle Orthod. 2015, 85, 1015–1020. [Google Scholar] [CrossRef] [Green Version]
- Baccetti, T.; Franchi, L.; Cameron, C.G.; McNamara, J.A. Treatment timing for rapid maxillary expansion. Angle Orthod. 2001, 71, 343–350. [Google Scholar]
- Melsen, B. Palatal growth studied on human autopsy material. A histologic microradiographic study. Am. J. Orthod. 1975, 68, 42–54. [Google Scholar] [CrossRef]
- Cossellu, G.; Lanteri, V.; Lione, R.; Ugolini, A.; Gaffuri, F.; Cozza, P.; Farronato, M. Efficacy of ketoprofen lysine salt and paracetamol/acetaminophen to reduce pain during rapid maxillary expansion: A randomized controlled clinical trial. Int. J. Paediatr. Dent. 2019, 29, 58–65. [Google Scholar] [CrossRef]
- Needleman, H.L.; Hoang, D.C.D.; Allred, D.E.; Hertzberg, J.; Berde, C. Reports of pain by children undergoing rapid palatal expansion. Pediatr. Dent. 2000, 6, 221–226. [Google Scholar]
- Halıcıo, K. Subjective symptoms of RME patients treated with three different screw activation protocols: A randomised clinical trial. Aust. Orthod. J. 2012, 28, 8. [Google Scholar]
- Ugolini, A.; Cossellu, G.; Farronato, M.; Silvestrini-Biavati, A.; Lanteri, V. A multicenter, prospective, randomized trial of pain and discomfort during maxillary expansion: Leaf expander versus hyrax expander. Int. J. Paediatr. Dent. 2020, 30, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Matos, D.S.; Palma-Dibb, R.G.; de Oliveira Santos, C.; da Conceição Pereira Saraiva, M.; Marques, F.V.; Matsumoto, M.A.N.; Romano, F.L. Evaluation of photobiomodulation therapy to accelerate bone formation in the mid palatal suture after rapid palatal expansion: A randomized clinical trial. Lasers Med. Sci. 2021, 36, 1039–1046. [Google Scholar] [CrossRef]
- Nieri, M.; Paoloni, V.; Lione, R.; Barone, V.; Marino Merlo, M.; Giuntini, V.; Cozza, P.; Franchi, L. Comparison between two screws for maxillary expansion: A multicenter randomized controlled trial on patient’s reported outcome measures. Eur. J. Orthod. 2021, 43, 293–300. [Google Scholar] [CrossRef]
- Feldmann, I.; Bazargani, F. Pain and discomfort during the first week of rapid maxillary expansion (RME) using two different RME appliances: A randomized controlled trial. Angle Orthod. 2017, 87, 391–396. [Google Scholar] [CrossRef] [Green Version]
- De Felippe, N.L.O.; Da Silveira, A.C.; Viana, G.; Smith, B. Influence of palatal expanders on oral comfort, speech, and mastication. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 48–53. [Google Scholar] [CrossRef]
- Erverdi, N.; Okar, I.; Kücükkeles, N.; Arbak, S. A comparison of two different rapid palatalexpansion techniques from the point of root resorption. Am. J. Orthod. Dentofac. Orthop. 1994, 106, 47–51. [Google Scholar] [CrossRef]
- Romanyk, D.L.; Lagravere, M.O.; Toogood, R.W.; Major, P.W.; Carey, J.P. Review of Maxillary Expansion Appliance Activation Methods: Engineering and Clinical Perspectives. J. Dent. Biomech. 2010, 1, 496906. [Google Scholar] [CrossRef]
- Lanteri, V.; Cossellu, G.; Gianolio, A.; Beretta, M.; Lanteri, C.; Cherchi, C.; Farronato, G. Comparison between RME, SME and Leaf Expander in growing patients: A retrospective postero-anterior cephalometric study. Eur. J. Paediatr. Dent. 2018, 19, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Arndt, W.V. Nickel titanium palatal expander. J. Clin. Orthod. 1993, 27, 129–137. [Google Scholar] [PubMed]
- Schuster, G.; Borel-Scherf, I.; Schopf, P.M. Frequency of and Complications in the Use of RPE Appliances? Results of a Survey in the Federal State of Hesse, Germany. J. Orofac. Orthop. 2005, 66, 148–161. [Google Scholar] [CrossRef] [PubMed]
- Caccianiga, G.; Crestale, C.; Cozzani, M.; Piras, A.; Mutinelli, S.; Lo Giudice, A.; Cordasco, G. Low-level laser therapy and invisible removal aligners. J. Biol. Regul. Homeost. Agents 2016, 30, 107–113. [Google Scholar]
- Sousa, M.V.S.; Pinzan, A.; Consolaro, A.; Henriques, J.F.C.; de Freitas, M.R. Systematic literature review: Influence of low-level laser on orthodontic movement and pain control in humans. Photomed. Laser Surg. 2014, 32, 592–599. [Google Scholar] [CrossRef]
- Mehlisch, D.R.; Sollecito, W.A.; Helfrick, J.F.; Leibold, D.G.; Markowitz, R.; Schow, C.E.; Shultz, R.; Waite, D.E. Multicenter clinical trial of ibuprofen and acetaminophen in the treatment of postoperative dental pain. J. Am. Dent. Assoc. 1990, 121, 257–263. [Google Scholar] [CrossRef]
- Bartzela, T.; Türp, J.C.; Motschall, E.; Maltha, J.C. Medication effects on the rate of orthodontic tooth movement: A systematic literature review. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 16–26. [Google Scholar] [CrossRef]
- Bianchi, M.; Panerai, A.E. The dose-related effects of paracetamol on hyperalgesia and nociception in the rat. Br. J. Pharm. 1996, 117, 130–132. [Google Scholar] [CrossRef] [Green Version]
- Ngan, P.; Wilson, S.; Shanfeld, J.; Amini, H. The effect of ibuprofen on the level of discomfort in patients undergoing orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 1994, 106, 88–95. [Google Scholar] [CrossRef]
Figure 1.
Article screening: four-phase PRISMA (preferred reporting items for systematic reviews and meta-analyses) flow diagram for study collection, showing the number of studies identified, screened, deemed eligible, and included in the present review.
Figure 1.
Article screening: four-phase PRISMA (preferred reporting items for systematic reviews and meta-analyses) flow diagram for study collection, showing the number of studies identified, screened, deemed eligible, and included in the present review.


{kind=link}
Table 1.
Methodological quality criteria.
| Sr No. | Items | Scoring |
|---|---|---|
| A | Design of randomized clinical trial | 1 |
| B | Eligibility criteria for study participants | 1 |
| C | Sample size determination | 1 |
| D | Details about clinical diagnostic criteria | 1 |
| E | Ethical considerations | 1 |
| F | Method of blinding | 1 |
| G | Methods and type of randomization | 1 |
| H | Description of recruitment period and follow-up | 1 |
| I | Withdrawals and dropouts | 1 |
| J | Clearly defined outcomes | 1 |
| K | Appropriate statistical analysis | 1 |
| Total score | 11 |
Table 2.
Characteristics and main data of the reviewed studies, extracted according to the PICOS approach. Part 1.
Table 2.
Characteristics and main data of the reviewed studies, extracted according to the PICOS approach. Part 1.
| Author/Year | Patients/Problem/ Population | Intervention |
|---|---|---|
| Caccianiga et al., 2022 [2] | 30 patients (15 PBMT G, 15 no PBMT G). 16 F, 14 M. M.a. 7.8 years (7.6 years PBMT G, 8 no PBMT G). |
|
| de Araújo et al., 2021 [3] | 39 patients with posterior crossbite or maxillary atresia: 20 Hyrax G, 19 Haas G. M.a.: 9.35 years (9.56 Hyrax G, 9.13 Haas G). Hyrax G: 56.5% F, 43.7% M. Haas G: 43.5% F, 56.3% M. |
|
| Matos et al., 2021 [15] | 34 patients (18 PBMT G, 16 no PMBT G). PMBT G: 45.5% F, 55.5% M. M.a. 9.2 years. No PBMT G: 55.6% F, 44.4% M. M.a.8.2 years. |
|
| Nieri et al., 2021 [16] | 56 patients (28 LE G, 28 RME G) equally divided in two Italian centers. LE G: 61% F, 39% M. M.a. 8 years. RME G: 43% F, 57% M. M.a. 8.4 years. |
|
| Altieri et al., 2020 [1] | 38 patients (18 TBE G, BBE G) 44% F, 56% M. M.a. 12.3 years. |
|
| Ugolini et al., 2019 [12] | 101 patients (48 RME G, 53 LE G). RME G: 26 F, 23 M. M.a. 9.4 years. LE G: 28 F, 25 M. M.a. 9.1. years. |
|
| Cesur et al., 2018 [5] | 62 patients (32 F, 30 M). F m.a.: 13.16 years. M m.a.: 12.91 years. |
|
| Cossellu et al., 2018 [9] | Phase 1: 101 patients. KLS G: 28 patients (17 F, 11 M), m.a. 8.5 ± 1.8 years. P G: 35 patients (17 F, 18 M), m.a. 8.7 ± 1.8 years. CTRL G: 35 patients (17 F, 19 M), m.a. 8.9 ± 1.2 years. Phase 2: added KLS-B 31 patients (15 F, 16 M), m.a. 8.7 ± 1.6 years. |
|
| Feldmann et al., 2017 [17] | 50 patients (25 TBE G, 25 TBBE G). M.a.: 9.7 years TBE G, 10 years TBBE G. |
|
| Needleman et al., 2000 [10] | 97 patients: 61% F, 39% M. M.a.: 7.7 years. |
|
F = female/s, M = male/s, m.a. = mean age, G = group, RME = rapid palatal expansion/expander, LE = Leaf expander, min = minutes, h = hour/s, d = day/s, w = week/s, m = month/s, pt = point/s, NRS = Numerical Rating Scale, FPS = Faces Pain Scale, FPS-R = Faces Pain Scale-Revised, GRS = Graphic Rating Scale, CAS = Color Analog Scale, PBMT = photobiomodulation therapy, TBE = tooth-borne expander, BBE = bone-borne expander, TBBE = tooth–bone-borne expander, KLS = ketoprofen lysine salt, P = paracetamol/acetaminophen, CTR = control.
Table 3.
Characteristics and main data of the reviewed studies, extracted according to the PICOS approach. Part 2.
Table 3.
Characteristics and main data of the reviewed studies, extracted according to the PICOS approach. Part 2.
| Comparison | Outcome | Study Design |
|---|---|---|
| PBMT G with no PBMT G. |
| Randomized clinical trial. |
| Hyrax G with Haas G. |
| Prospective study. |
| PBMT G with no PBMT G. |
| Two-arm parallel-group randomized clinical trial. |
| LE G with RME G. |
| Multicenter randomized controlled trial. |
| TBE G with BBE G. |
| Parallel cohort study. |
| LE G with RME G. |
| Multicentric randomized study. |
| None. |
| Not defined by authors. |
| Phase 1:
|
|
| TBE G with TBBE G. |
| Randomized controlled trial. |
| None. |
| Not defined by authors. |
F = female/s, M = male/s, m.a. = mean age, G = group, RME = rapid palatal expansion/expander, LE = Leaf expander, min = minutes, h = hour/s, d = day/s, w = week/s, m = month/s, pt = point/s, NRS = Numerical Rating Scale, FPS = Faces Pain Scale, FPS-R = Faces Pain Scale-Revised, GRS = Graphic Rating Scale, CAS = Color Analog Scale, PBMT = photobiomodulation therapy, TBE = tooth-borne expander, BBE = bone-borne expander, TBBE = Tooth–bone-borne expander, KLS = ketoprofen lysine salt, P = paracetamol/acetaminophen, CTR = control.
Table 4.
Methodological Quality of included studies.
| Authors | Items for Methodological Quality Criteria | Total Score | Methodological Quality of the Study | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| A | B | C | D | E | F | G | H | I | J | K | |||
| Caccianiga et al., 2022 [2] | 1 | 1 | 0 | 0.5 | 1 | 0.5 | 1 | 1 | 1 | 1 | 1 | 9 | Moderate (7–9 points) |
| de Araújo et al., 2021 [3] | 0.5 | 1 | 1 | 0.5 | 1 | 0 | 1 | 1 | 1 | 0.5 | 1 | 8.5 | Moderate (7–9 points) |
| Matos et al., 2021 [15] | 1 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 1 | 1 | 1 | 10 | Good (>9 points) |
| Nieri et al., 2021 [16] | 1 | 1 | 1 | 1 | 1 | 0.5 | 1 | 1 | 1 | 1 | 1 | 10.5 | Good (>9 points) |
| Altieri et al., 2020 [1] | 0.5 | 1 | 0 | 0.5 | 1 | 0.5 | 1 | 1 | 1 | 0.5 | 1 | 8 | Moderate (7–9 points) |
| Ugolini et al., 2019 [12] | 1 | 1 | 1 | 1 | 1 | 0.5 | 1 | 1 | 1 | 1 | 1 | 10.5 | Good (>9 points) |
| Cesur et al., 2018 [5] | 0 | 1 | 0 | 0.5 | 1 | 0 | 0 | 1 | 1 | 0.5 | 1 | 6 | Poor (<7) |
| Cossellu et al., 2018 [9] | 1 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 1 | 1 | 1 | 10 | Good (>9 points) |
| Feldmann et al., 2017 [17] | 1 | 1 | 0 | 0.5 | 1 | 0.5 | 1 | 1 | 1 | 0.5 | 1 | 8.5 | Moderate (7–9 points) |
| Needleman et al., 2000 [10] | 0 | 1 | 0 | 0.5 | 1 | 0 | 0 | 1 | 1 | 0.5 | 1 | 6 | Poor (<7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Barone, M.; De Stefani, A.; Cavallari, F.; Gracco, A.; Bruno, G. Pain during Rapid Maxillary Expansion: A Systematic Review. Children 2023, 10, 666. https://doi.org/10.3390/children10040666
AMA Style
Barone M, De Stefani A, Cavallari F, Gracco A, Bruno G. Pain during Rapid Maxillary Expansion: A Systematic Review. Children. 2023; 10(4):666. https://doi.org/10.3390/children10040666
Chicago/Turabian StyleBarone, Martina, Alberto De Stefani, Filippo Cavallari, Antonio Gracco, and Giovanni Bruno. 2023. "Pain during Rapid Maxillary Expansion: A Systematic Review" Children 10, no. 4: 666. https://doi.org/10.3390/children10040666
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.