
Pediatric Bowel Management Options and Organizational Aspects

{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
3. Antegrade Continence Enemas
3.1. Definition and Indications
3.2. Appendicostomy vs. Cecostomy
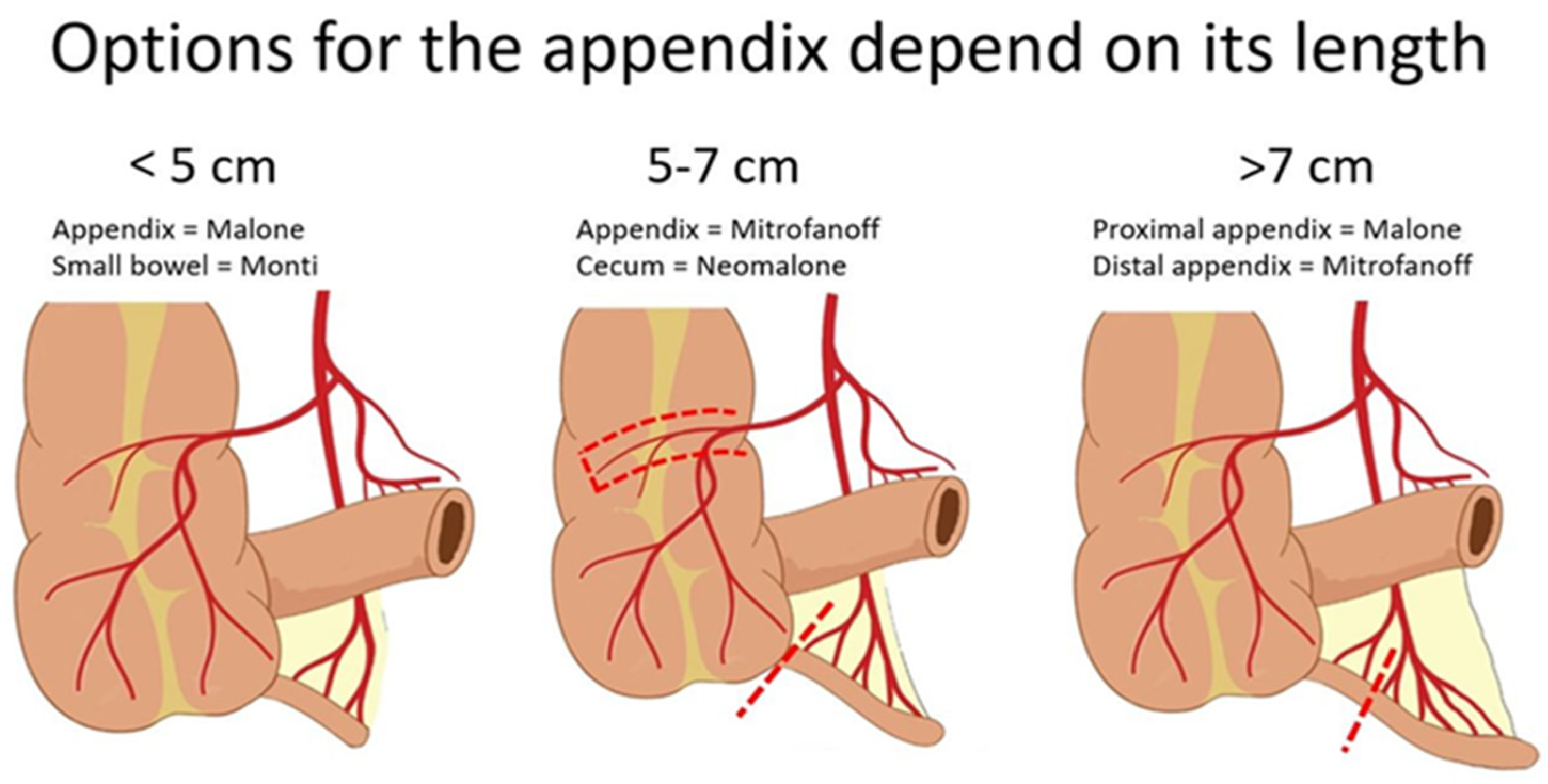
3.3. Intraoperative Decision-Making
3.4. Postoperative Care
3.5. Outcomes
4. Long-Term Collaboration and Bowel Management Program
4.1. Collaborative Approach
4.2. Importance of Family Education
4.3. Telemedicine
5. Bowel Management Boot Camps
5.1. Assessment of Quality of Life and Fecal Continence Scoring
5.2. Outcomes of the Bowel Management Program
6. Transition of Care
6.1. Indications for Transition
6.2. Multidisciplinary Transition
6.3. The Right Time for Transition
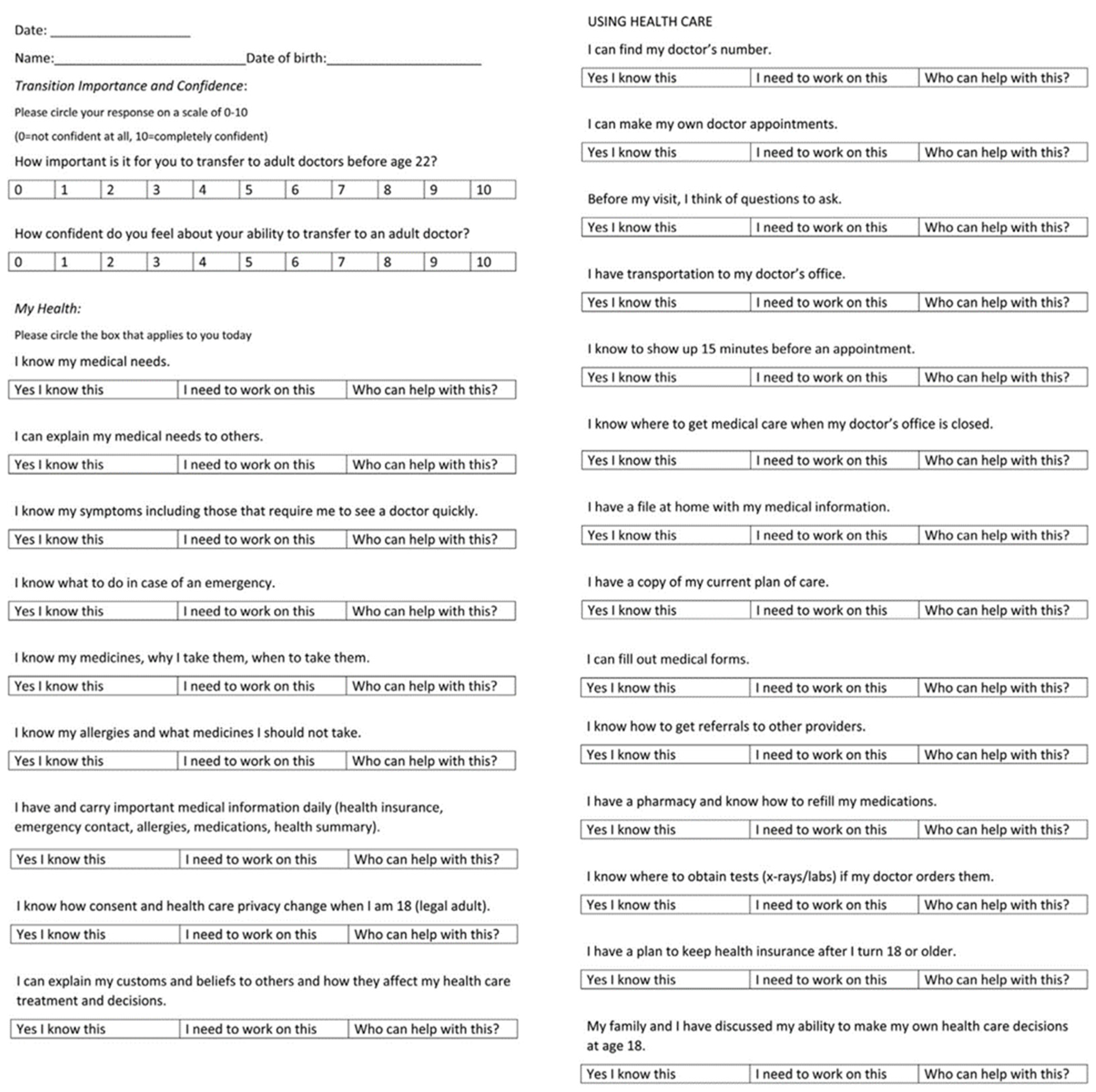
6.4. Readiness for Transition
6.4.1. Providers
6.4.2. Patient
6.4.3. Family
6.5. Components of the Transition Program
6.6. Keys to Success and Barriers to Transition
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Russell, K.W.; Barnhart, D.C.; Zobell, S.; Scaife, E.R.; Rollins, M.D. Effectiveness of an Organized Bowel Management Program in the Management of Severe Chronic Constipation in Children. J. Pediatr. Surg. 2015, 50, 444–447. [Google Scholar] [CrossRef] [PubMed]
- Lim, I.I.P.; Cushing, C.C.; Jenkins, T.; Troutt, M.; Zeller, M.H.; Hossain, M.; Rymeski, B.; Helmrath, M.; Frischer, J.S. Prospective Quality of Life Outcomes in Pediatric Fecal Incontinence Following Bowel Management. J. Pediatr. Surg. 2021, 56, 1459–1464. [Google Scholar] [CrossRef] [PubMed]
- Wood, R.J.; Vilanova-Sanchez, A.; El-Gohary, Y.; Ahmad, H.; Halleran, D.R.; Reck-Burneo, C.A.; Rentea, R.; Sebastiao, Y.; Nash, O.; Booth, K.; et al. One-Year Impact of a Bowel Management Program in Treating Fecal Incontinence in Patients with Anorectal Malformations. J. Pediatr. Surg. 2021, 56, 1689–1693. [Google Scholar] [CrossRef] [PubMed]
- Vilanova-Sánchez, A.; Choueiki, J.; Smith, C.A.; Callicot, S.; Frischer, J.S.; Levitt, M.A. Creating a Collaborative Program for the Care of Children with Colorectal and Pelvic Problems. Semin. Pediatr. Surg. 2020, 29, 150985. [Google Scholar] [CrossRef]
- Bischoff, A.; Levitt, M.A.; Bauer, C.; Jackson, L.; Holder, M.; Peña, A. Treatment of Fecal Incontinence with a Comprehensive Bowel Management Program. J. Pediatr. Surg. 2009, 44, 1278–1284. [Google Scholar] [CrossRef]
- Bischoff, A.; Levitt, M.A.; Peña, A. Bowel Management for the Treatment of Pediatric Fecal Incontinence. Pediatr. Surg. Int. 2009, 25, 1027–1042. [Google Scholar] [CrossRef] [Green Version]
- Halleran, D.R.; Lane, V.A.; Leonhart, K.L.; Fischer, B.; Sebastião, Y.V.; Chisolm, D.J.; Levitt, M.A.; Wood, R.J.; Minneci, P.C.; Deans, K.J. Development of a Patient-Reported Experience and Outcome Measures in Pediatric Patients Undergoing Bowel Management for Constipation and Fecal Incontinence. J. Pediatr. Gastroenterol. Nutr. 2019, 69, e34. [Google Scholar] [CrossRef]
- Mugie, S.M.; Benninga, M.A.; Di Lorenzo, C. Epidemiology of Constipation in Children and Adults: A Systematic Review. Best Pract. Res. Clin. Gastroenterol. 2011, 25, 3–18. [Google Scholar] [CrossRef]
- MacGeorge, C.A.; Simpson, K.N.; Basco, W.T.; Bundy, D.G. Constipation-Related Emergency Department Use, and Associated Office Visits and Payments Among Commercially Insured Children. Acad. Pediatr. 2018, 18, 952–956. [Google Scholar] [CrossRef]
- Wood, R.J.; Yacob, D.; Levitt, M.A. Surgical Options for the Management of Severe Functional Constipation in Children. Curr. Opin. Pediatr. 2016, 28, 370. [Google Scholar] [CrossRef]
- Kuizenga-Wessel, S.; Mousa, H.M.; Benninga, M.A.; Di Lorenzo, C. Lack of Agreement on How to Use Antegrade Enemas in Children. J. Pediatr. Gastroenterol. Nutr. 2016, 62, 71. [Google Scholar] [CrossRef] [PubMed]
- Malone, P.S.J. The Antegrade Continence Enema Procedure. BJU Int. 2004, 93, 248–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chatoorgoon, K.; Pena, A.; Lawal, T.; Hamrick, M.; Louden, E.; Levitt, M.A. Neoappendicostomy in the Management of Pediatric Fecal Incontinence. J. Pediatr. Surg. 2011, 46, 1243–1249. [Google Scholar] [CrossRef]
- Shandling, B.; Chait, P.G.; Richards, H.F. Percutaneous Cecostomy: A New Technique in the Management of Fecal Incontinence. J. Pediatr. Surg. 1996, 31, 534–537. [Google Scholar] [CrossRef] [PubMed]
- Gasior, A.; Reck, C.; Vilanova-Sanchez, A.; Diefenbach, K.A.; Yacob, D.; Lu, P.; Vaz, K.; Di Lorenzo, C.; Levitt, M.A.; Wood, R.J. Surgical Management of Functional Constipation: An Intermediate Report of a New Approach Using a Laparoscopic Sigmoid Resection Combined with Malone Appendicostomy. J. Pediatr. Surg. 2018, 53, 1160–1162. [Google Scholar] [CrossRef]
- Mohamed, H.; Wayne, C.; Weir, A.; Partridge, E.A.; Langer, J.C.; Nasr, A. Tube Cecostomy versus Appendicostomy for Antegrade Enemas in the Management of Fecal Incontinence in Children: A Systematic Review. J. Pediatr. Surg. 2020, 55, 1196–1200. [Google Scholar] [CrossRef]
- Li, C.; Shanahan, S.; Livingston, M.H.; Walton, J.M. Malone Appendicostomy versus Cecostomy Tube Insertion for Children with Intractable Constipation: A Systematic Review and Meta-Analysis. J. Pediatr. Surg. 2018, 53, 885–891. [Google Scholar] [CrossRef]
- Halleran, D.R.; Vilanova-Sanchez, A.; Rentea, R.M.; Vriesman, M.H.; Maloof, T.; Lu, P.L.; Onwuka, A.; Weaver, L.; Vaz, K.K.; Yacob, D.; et al. A Comparison of Malone Appendicostomy and Cecostomy for Antegrade Access as Adjuncts to a Bowel Management Program for Patients with Functional Constipation or Fecal Incontinence. J. Pediatr. Surg. 2019, 54, 123–128. [Google Scholar] [CrossRef]
- Gomez-Suarez, R.A.; Gomez-Mendez, M.; Petty, J.K.; Fortunato, J.E. Associated Factors for Antegrade Continence Enemas for Refractory Constipation and Fecal Incontinence. J. Pediatr. Gastroenterol. Nutr. 2016, 63, e63. [Google Scholar] [CrossRef] [Green Version]
- Fuchs, M.E.; Halleran, D.R.; Bourgeois, T.; Sebastião, Y.; Weaver, L.; Farrell, N.; Vilanova-Sánchez, A.; Gasior, A.; Halaweish, I.; Jayanthi, V.R.; et al. Correlation of Anorectal Malformation Complexity and Associated Urologic Abnormalities. J. Pediatr. Surg. 2021, 56, 1988–1992. [Google Scholar] [CrossRef]
- Johnston, A.W.; Wiener, J.S.; Todd Purves, J. Pediatric Neurogenic Bladder and Bowel Dysfunction: Will My Child Ever Be out of Diapers? Eur. Urol. Focus 2020, 6, 838–867. [Google Scholar] [CrossRef] [PubMed]
- VanderBrink, B.A.; Cain, M.P.; Kaefer, M.; Meldrum, K.K.; Misseri, R.; Rink, R.C. Split-Appendix Technique for Simultaneous Appendicovesicostomy and Appendicocecostomy. J. Pediatr. Surg. 2011, 46, 259–262. [Google Scholar] [CrossRef] [PubMed]
- Halleran, D.R.; Sloots, C.E.J.; Fuller, M.K.; Diefenbach, K. Adjuncts to Bowel Management for Fecal Incontinence and Constipation, the Role of Surgery; Appendicostomy, Cecostomy, Neoappendicostomy, and Colonic Resection. Semin. Pediatr. Surg. 2020, 29, 150998. [Google Scholar] [CrossRef]
- Zann, A.; Sebastiao, Y.; Ching, C.C.; Fuchs, M.; Jayanthi, V.R.; Wood, R.J.; Levitt, M.A.; DaJusta, D. Split Appendix Mitrofanoffs Have Higher Risk of Complication than Intact Appendix or Monti Channels. J. Pediatr. Urol. 2021, 17, 700.e1–700.e6. [Google Scholar] [CrossRef]
- Short, S.S.; Zobell, S.; Gaddis, K.; Mammen, L.; Wynne, E.; Rollins, M.D. Use of Expedited Post-Operative Protocol for Children Undergoing Appendicostomy Reduces Length of Hospitalization. J. Pediatr. Surg. 2022, 57, 406–409. [Google Scholar] [CrossRef] [PubMed]
- Lopez, J.J.; Svetanoff, W.J.; Bruns, N.; Lewis, W.E.; Warner, C.N.; Fraser, J.A.; Briggs, K.B.; Carrasco, A.; Gatti, J.M.; Rosen, J.M.; et al. Single Institution Review of Mini-ACE® Low-Profile Appendicostomy Button for Antegrade Continence Enema Administration. J. Pediatr. Surg. 2022, 57, 359–364. [Google Scholar] [CrossRef]
- Dolejs, S.C.; Smith, J.K.; Sheplock, J.; Croffie, J.M.; Rescorla, F.J. Contemporary Short- and Long-Term Outcomes in Patients with Unremitting Constipation and Fecal Incontinence Treated with an Antegrade Continence Enema. J. Pediatr. Surg. 2017, 52, 79–83. [Google Scholar] [CrossRef]
- Chong, C.; Featherstone, N.; Sharif, S.; Cherian, A.; Cuckow, P.; Mushtaq, I.; De Coppi, P.; Cross, K.; Curry, J. 5 Years after an ACE: What Happens Then? Pediatr. Surg. Int. 2016, 32, 397–401. [Google Scholar] [CrossRef]
- Brophy, S.; Brennan, K.; Woodgate, E.; Pinaud, B.; McLaughlin, E.; Gillespie, J.; Grover, Z.; Blackmore, C.; Romao, R.L. Comparing Quality of Life Improvement after Antegrade Continence Enema (ACE) Therapy for Patients with Organic and Functional Constipation/Encopresis. J. Pediatr. Surg. 2022, 57, 855–860. [Google Scholar] [CrossRef]
- Reeder, R.W.; Wood, R.J.; Avansino, J.R.; Levitt, M.A.; Durham, M.M.; Sutcliffe, J.; Midrio, P.; Calkins, C.M.; de Blaauw, I.; Dickie, B.H.; et al. The Pediatric Colorectal and Pelvic Learning Consortium (PCPLC): Rationale, Infrastructure, and Initial Steps. Tech. Coloproctol. 2018, 22, 395–399. [Google Scholar] [CrossRef]
- Vilanova-Sánchez, A.; Reck, C.A.; Wood, R.J.; Garcia Mauriño, C.; Gasior, A.C.; Dyckes, R.E.; McCracken, K.; Weaver, L.; Halleran, D.R.; Diefenbach, K.; et al. Impact on Patient Care of a Multidisciplinary Center Specializing in Colorectal and Pelvic Reconstruction. Front. Surg. 2018, 5, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vilanova-Sanchez, A.; Halleran, D.R.; Reck-Burneo, C.A.; Gasior, A.C.; Weaver, L.; Fisher, M.; Wagner, A.; Nash, O.; Booth, K.; Peters, K.; et al. A Descriptive Model for a Multidisciplinary Unit for Colorectal and Pelvic Malformations. J. Pediatr. Surg. 2019, 54, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Style, C.C.; Hsu, D.M.; Verla, M.A.; Mittal, A.G.; Austin, P.; Seth, A.; Dietrich, J.E.; Adeyemi-Fowode, O.A.; Bercaw-Pratt, J.L.; Chiou, E.H.; et al. Development of a Multidisciplinary Colorectal and Pelvic Health Program: Program Implementation and Clinical Impact. J. Pediatr. Surg. 2020, 55, 2397–2402. [Google Scholar] [CrossRef] [PubMed]
- Baxter, K.J.; Garza, J.M.; Rollins, M.D.; Drake, K.; Reeder, R.W.; Wood, R.; Avansino, J.; Calkins, C.M.; Ralls, M.; Garvey, E.M.; et al. Multi-Institutional Review of Bowel Management Strategies in Children with Anorectal Malformations. J. Pediatr. Surg. 2020, 55, 2752–2757. [Google Scholar] [CrossRef]
- Vermeire, E.; Hearnshaw, H.; Van Royen, P.; Denekens, J. Patient Adherence to Treatment: Three Decades of Research. A Comprehensive Review. J. Clin. Pharm. Ther. 2001, 26, 331–342. [Google Scholar] [CrossRef] [Green Version]
- Dingemans, A.J.M.; Krois, W.; Rios, J.C.; Wood, R.J.; Levitt, M.A.; Reck-Burneo, C.A. Health Literacy and Health-Related Quality of Life in Patients with Anorectal Malformations: A Comparison between a Charity Hospital in Honduras and a Tertiary Care Center in the United States. J. Pediatr. Surg. 2018, 53, 1951–1954. [Google Scholar] [CrossRef]
- Taylor, M.A.; Bucher, B.T.; Reeder, R.W.; Avansino, J.R.; Durham, M.; Calkins, C.M.; Wood, R.J.; Levitt, M.A.; Drake, K.; Rollins, M.D. Comparison of Hirschsprung Disease Characteristics between Those with a History of Postoperative Enterocolitis and Those without: Results from the Pediatric Colorectal and Pelvic Learning Consortium. Eur. J. Pediatr. Surg. 2021, 31, 207–213. [Google Scholar] [CrossRef]
- Abdulhai, S.; Glenn, I.C.; McNinch, N.L.; Craner, D.; Chou, E.; Ponsky, T.A. Public Perception of Telemedicine and Surgical Telementoring in the Pediatric Population: Results of a Parental Survey. J. Laparoendosc. Adv. Surg. Tech. 2018, 28, 215–217. [Google Scholar] [CrossRef]
- Knaus, M.E.; Ahmad, H.; Metzger, G.A.; Beyene, T.J.; Thomas, J.L.; Weaver, L.J.; Gasior, A.C.; Wood, R.J.; Halaweish, I. Outcomes of a Telemedicine Bowel Management Program during COVID-19. J. Pediatr. Surg. 2022, 57, 80–85. [Google Scholar] [CrossRef]
- Stathopoulos, E.; Skerritt, C.; Fitzpatrick, G.; Hooker, E.; Lander, A.; Gee, O.; Jester, I. Children with Congenital Colorectal Malformations during the UK SARS-CoV-2 Pandemic Lockdown: An Assessment of Telemedicine and Impact on Health. Pediatr. Surg. Int. 2021, 37, 1593–1599. [Google Scholar] [CrossRef]
- Knaus, M.E.; Kersey, K.; Ahmad, H.; Weaver, L.; Thomas, J.L.; Metzger, G.A.; Wood, R.J.; Gasior, A.C. Both Sides of the Screen: Provider and Patient Perspective on Telemedicine in Pediatric Surgery. J. Pediatr. Surg. 2022, 57, 1614–1621. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.D.; Zhou, C.; Stanford, S.; Haaland, W.; Varni, J.W.; Mangione-Smith, R.M. Validity and Responsiveness of the Pediatric Quality of Life Inventory (PedsQL) 4.0 Generic Core Scales in the Pediatric Inpatient Setting. JAMA Pediatr. 2014, 168, 1114–1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cushing, C.C.; Threlkeld, M.R.S.; Martinez-Leo, B.; Hall, J.; Hossain, M.; Dickie, B.H.; Rymeski, B.; Helmrath, M.; Zeller, M.H.; Frischer, J.S. Initial Development and Validation of a Fecal Incontinence-Specific Quality of Life Measure. J. Pediatr. Surg. 2018, 53, 1148–1153. [Google Scholar] [CrossRef]
- Afshar, K.; Mirbagheri, A.; Scott, H.; MacNeily, A.E. Development of a Symptom Score for Dysfunctional Elimination Syndrome. J. Urol. 2009, 182, 1939–1944. [Google Scholar] [CrossRef] [PubMed]
- Kilpatrick, J.A.; Zobell, S.; Leeflang, E.J.; Cao, D.; Mammen, L.; Rollins, M.D. Intermediate and Long-Term Outcomes of a Bowel Management Program for Children with Severe Constipation or Fecal Incontinence. J. Pediatr. Surg. 2020, 55, 545–548. [Google Scholar] [CrossRef]
- 2005–2006 National Survey of Children with Special Health Care Needs. Available online: https://www.cdc.gov/Nchs/Slaits/Cshcn.Htm (accessed on 22 March 2023).
- Cooley, W.C.; Sagerman, P.J.; American Academy of Pediatrics, A.A. of F.P., and American College of Physicians. Transitions Clinical Report Authoring Group Supporting the Health Care Transition from Adolescence to Adulthood in the Medical Home. Pediatrics 2011, 128, 182–200. [Google Scholar] [CrossRef] [Green Version]
- Harrington, A.W.; Gasior, A.C.; Einarsdottir, H.; Rothstein, D.H.; Rollins, M.D.; Ozgediz, D.E. Hirschsprung Disease: The Rise of Structured Transition and Long-Term Care. J. Pediatr. Gastroenterol. Nutr. 2019, 69, 306. [Google Scholar] [CrossRef]
- Granström, A.L.; Danielson, J.; Husberg, B.; Nordenskjöld, A.; Wester, T. Adult Outcomes after Surgery for Hirschsprung’s Disease: Evaluation of Bowel Function and Quality of Life. J. Pediatr. Surg. 2015, 50, 1865–1869. [Google Scholar] [CrossRef] [Green Version]
- Xiong, X.; Chen, X.; Wang, G.; Feng, J. Long Term Quality of Life in Patients with Hirschsprung’s Disease Who Underwent Heart-Shaped Anastomosis during Childhood: A Twenty-Year Follow-up in China. J. Pediatr. Surg. 2015, 50, 2044–2047. [Google Scholar] [CrossRef]
- Danielson, J.; Karlbom, U.; Graf, W.; Wester, T. Outcome in Adults with Anorectal Malformations in Relation to Modern Classification—Which Patients Do We Need to Follow beyond Childhood? J. Pediatr. Surg. 2017, 52, 463–468. [Google Scholar] [CrossRef]
- Ahmad, H.; Knaus, M.E.; Minneci, P.C.; Wood, R.J.; Gasior, A.C. Transition of Care Barriers in Pediatric Patients With Anorectal Malformation. Dis. Colon Rectum 2022, 65, 955. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.R.; John, M.; Singh, S.J.; Williams, A.R. Transition from Paediatric Surgery: How Many Patients Do We Need to Plan For? Ann. R. Coll. Surg. Engl. 2016, 98, 586–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cairo, S.B.; Gasior, A.; Rollins, M.D.; Rothstein, D.H. Challenges in Transition of Care for Patients With Anorectal Malformations: A Systematic Review and Recommendations for Comprehensive Care. Dis. Colon Rectum 2018, 61, 390–399. [Google Scholar] [CrossRef]
- Acker, S.; Peña, A.; Wilcox, D.; Alaniz, V.; Bischoff, A. Transition of Care: A Growing Concern in Adult Patients Born with Colorectal Anomalies. Pediatr. Surg. Int. 2019, 35, 233–237. [Google Scholar] [CrossRef]
- Rigueros Springford, L.; Connor, M.J.; Jones, K.; Kapetanakis, V.V.; Giuliani, S. Prevalence of Active Long-Term Problems in Patients With Anorectal Malformations: A Systematic Review. Dis. Colon Rectum 2016, 59, 570. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, J.; Tomuschat, C.; Puri, P. Long-Term Results of Transanal Pull-through for Hirschsprung’s Disease: A Meta-Analysis. Pediatr. Surg. Int. 2016, 32, 743–749. [Google Scholar] [CrossRef]
- Muise, E.D.; Cowles, R.A. Transition of Care in Pediatric Surgical Patients with Complex Gastrointestinal Disease. Semin. Pediatr. Surg. 2015, 24, 65–68. [Google Scholar] [CrossRef]
- Shemesh, E.; Annunziato, R.A.; Arnon, R.; Miloh, T.; Kerkar, N. Adherence to Medical Recommendations and Transition to Adult Services in Pediatric Transplant Recipients. Curr. Opin. Organ Transplant. 2010, 15, 288. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, L.A.; Brumley, L.D.; Tuchman, L.K.; Barakat, L.P.; Hobbie, W.L.; Ginsberg, J.P.; Daniel, L.C.; Kazak, A.E.; Bevans, K.; Deatrick, J.A. Stakeholder Validation of a Model of Readiness for Transition to Adult Care. JAMA Pediatr. 2013, 167, 939–946. [Google Scholar] [CrossRef] [Green Version]
- Bower, W.F.; Christie, D.; DeGennaro, M.; Latthe, P.; Raes, A.; Romao, R.L.P.; Taghizadeh, A.; Wood, D.; Woodhouse, C.R.J.; Bauer, S.B. The Transition of Young Adults with Lifelong Urological Needs from Pediatric to Adult Services: An International Children’s Continence Society Position Statement. Neurourol. Urodyn. 2017, 36, 811–819. [Google Scholar] [CrossRef]
- Zhao, J.Y.; Chiu, P.P.L.; Dasgupta, R.; Jen, H.C.; Rothstein, D.H. Defining the Need for Transitional Care From Pediatric to Adult Surgery for Young Adult Patients With Surgically Corrected Congenital Anomalies. JAMA Surg. 2016, 151, 393–394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brennan, L.J.; Rolfe, P.M. Transition from Pediatric to Adult Health Services: The Perioperative Care Perspective: Transition from Pediatric to Adult Health Services. Pediatr. Anesth. 2011, 21, 630–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naiditch, J.A.; Rothstein, D.H. Transitional Care From Pediatric to Adult Surgery. JAMA Surg. 2014, 149, 1099. [Google Scholar] [CrossRef]
- Chu, P.Y.; Maslow, G.R.; von Isenburg, M.; Chung, R.J. Systematic Review of the Impact of Transition Interventions for Adolescents With Chronic Illness on Transfer From Pediatric to Adult Healthcare. J. Pediatr. Nurs. 2015, 30, e19–e27. [Google Scholar] [CrossRef] [Green Version]
- Loftus, C.J.; Ahn, J.; Rice-Townsend, S.; Avansino, J.; Schmidt, J.; Hagedorn, J.C.; Wood, R.; Shnorhavorian, M.; Fuchs, M.D.; McCracken, K.A.; et al. Experiences and Attitudes of Young Adults with Congenital Bowel and Bladder Conditions. J. Pediatr. Urol. 2021, 17, 701.e1–701.e8. [Google Scholar] [CrossRef] [PubMed]
- Wajchendler, A.; Anderson, P.; Koyle, M.A. The Transition Process of Spina Bifida Patients to Adult-Centred Care: An Assessment of the Canadian Urology Landscape. Can. Urol. Assoc. J. 2017, 11, S88–S91. [Google Scholar] [CrossRef] [Green Version]
- Blyth, U.E.B.; Lall, A.; Jaffray, B.; Choudhary, M. Transition Care from Adolescence to Adulthood: A 10-Year Service Review of the Gynecological Implications for Young Women and Girls Born with Cloacal Anomalies. J. Pediatr. Adolesc. Gynecol. 2021, 34, 412–414. [Google Scholar] [CrossRef] [PubMed]
- Violani, C.; Grano, C.; Fernandes, M.; Prato, A.P.; Feitz, W.F.J.; Wijnen, R.; Battye, M.; Schwarzer, N.; Lemli, A.; Cavalieri, D.; et al. The Transition of Care for Patients with Anorectal Malformations and Hirschsprung Disease: A European Survey. Eur. J. Pediatr. Surg. 2022. [Google Scholar] [CrossRef]
- Kassa, A.-M.; Engvall, G.; Dellenmark Blom, M.; Engstrand Lilja, H. Understanding of the Transition to Adult Healthcare Services among Individuals with VACTERL Association in Sweden: A Qualitative Study. PLoS ONE 2022, 17, e0269163. [Google Scholar] [CrossRef]
- Starowicz, J.; Cassidy, C.; Brunton, L. Health Concerns of Adolescents and Adults with Spina Bifida. Front. Neurol. 2021, 12, 745814. [Google Scholar] [CrossRef]
- Summers, S.J.; Elliott, S.; McAdams, S.; Oottamasathien, S.; Brant, W.O.; Presson, A.P.; Fleck, J.; West, J.; Myers, J.B. Urologic Problems in Spina Bifida Patients Transitioning to Adult Care. Urology 2014, 84, 440–444. [Google Scholar] [CrossRef]
- Szymanski, K.M.; Cain, M.P.; Hardacker, T.J.; Misseri, R. How Successful Is the Transition to Adult Urology Care in Spina Bifida? A Single Center 7-Year Experience. J. Pediatr. Urol. 2017, 13, 40.e1–40.e6. [Google Scholar] [CrossRef] [PubMed]
- Chua, M.E.; Tse, L.N.; Silangcruz, J.M.; Kim, J.K.; Dos Santos, J.; Varghese, A.; Brownrigg, N.; Rickard, M.; Ming, J.M.; Lorenzo, A.J.; et al. Scoping Review of Neurogenic Bladder Patient-Reported Readiness and Experience Following Care in a Transitional Urology Clinic. Neurourol. Urodyn. 2022, 41, 1650–1658. [Google Scholar] [CrossRef] [PubMed]
- Breech, L. Gynecologic Concerns in Patients with Cloacal Anomaly. Semin. Pediatr. Surg. 2016, 25, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Breech, L. Gynecologic Concerns in Patients with Anorectal Malformations. Semin. Pediatr. Surg. 2010, 19, 139–145. [Google Scholar] [CrossRef]
- Giuliani, S.; Decker, E.; Leva, E.; Riccipetitoni, G.; Bagolan, P. Long Term Follow-up and Transition of Care in Anorectal Malformations: An International Survey. J. Pediatr. Surg. 2016, 51, 1450–1457. [Google Scholar] [CrossRef]
- Fortuna, R.J.; Halterman, J.S.; Pulcino, T.; Robbins, B.W. Delayed Transition of Care: A National Study of Visits to Pediatricians by Young Adults. Acad. Pediatr. 2012, 12, 405–411. [Google Scholar] [CrossRef]
- Giuliani, S.; Grano, C.; Aminoff, D.; Schwarzer, N.; Vorle, M.V.D.; Cretolle, C.; Haanen, M.; Brisighelli, G.; Marzheuser, S.; Connor, M. Transition of Care in Patients with Anorectal Malformations: Consensus by the ARM-Net Consortium. J. Pediatr. Surg. 2017, 52, 1866–1872. [Google Scholar] [CrossRef]
- Hoel, A.T.; Tofft, L.; Bjørnland, K.; Gjone, H.; Teig, C.J.; Øresland, T.; Stenström, P.; Andersen, M.H. Reaching Adulthood with Hirschsprung’s Disease: Patient Experiences and Recommendations for Transitional Care. J. Pediatr. Surg. 2021, 56, 257–262. [Google Scholar] [CrossRef]
- Agrawal, S.; Slocombe, K.; Wilson, T.; Kielb, S.; Wood, H.M. Urologic Provider Experiences in Transitioning Spina Bifida Patients from Pediatric to Adult Care. World J. Urol. 2019, 37, 607–611. [Google Scholar] [CrossRef]
- Bollegala, N.; Nguyen, G.C. Transitioning the Adolescent with IBD from Pediatric to Adult Care: A Review of the Literature. Gastroenterol. Res. Pract. 2015, 2015, e853530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rothstein, D.H.; Dasgupta, R.; on behalf of the Delivery of Surgical Care Committee of the American Academy of Pediatrics Section on Surgery. Transition of Care From Pediatric to Adult Surgery. Pediatrics 2016, 138, e20161303. [Google Scholar] [CrossRef] [Green Version]
- Hopson, B.; MSHA; Alford, E.N.; Zimmerman, K.; Blount, J.P.; Rocque, B.G. Development of an Evidence-Based Individualized Transition Plan for Spina Bifida. Neurosurg. Focus 2019, 47, E17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botelho, A.; Dias, P.N.G.; Tsuji, A.H.S.; Leite, M.T.C. Transition of Care in Pediatric Surgery. Einstein 2021, 19, eAO6314. [Google Scholar] [CrossRef]
- Goudie, A.; Carle, A.C. Ohio Study Shows That Insurance Coverage Is Critical For Children With Special Health Care Needs As They Transition To Adulthood. Health Aff. 2011, 30, 2382–2390. [Google Scholar] [CrossRef]
- Rague, J.T.; Kim, S.; Hirsch, J.A.; Meyer, T.; Rosoklija, I.; Larson, J.E.; Swaroop, V.T.; Bowman, R.M.; Bowen, D.K.; Cheng, E.Y.; et al. Assessment of Health Literacy and Self-Reported Readiness for Transition to Adult Care Among Adolescents and Young Adults With Spina Bifida. JAMA Netw. Open 2021, 4, e2127034. [Google Scholar] [CrossRef] [PubMed]
- Nah, S.A.; Ong, C.C.P.; Lie, D.; Marimuttu, V.J.; Hong, J.; Te-Lu, Y.; Low, Y.; Jacobsen, A.S. Understanding Experiences of Youth Growing Up with Anorectal Malformation or Hirschsprung’s Disease to Inform Transition Care: A Qualitative In-Depth Interview Study. Eur. J. Pediatr. Surg. 2018, 28, 67–74. [Google Scholar] [CrossRef]
- Tofft, L.; Hoel, A.T.; Håkansson, C.; Zawadzki, A.; Gjone, H.; Øresland, T.; Bjørnland, K.; Stenström, P. Key Components of Successful Transition for Adolescents Born with Anorectal Malformations-a Nordic Focus Group Study. Int. J. Adolesc. Med. Health 2020, 34, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Gasior, A.; Midrio, P.; Aminoff, D.; Stanton, M. Ongoing Care for the Patient with an Anorectal Malfromation; Transitioning to Adulthood. Semin. Pediatr. Surg. 2020, 29, 150991. [Google Scholar] [CrossRef]
- Fernandes, S.M.; O’Sullivan-Oliveira, J.; Landzberg, M.J.; Khairy, P.; Melvin, P.; Sawicki, G.S.; Ziniel, S.; Kenney, L.B.; Garvey, K.C.; Sobota, A.; et al. Transition and Transfer of Adolescents and Young Adults with Pediatric Onset Chronic Disease: The Patient and Parent Perspective. J. Pediatr. Rehabil. Med. 2014, 7, 43–51. [Google Scholar] [CrossRef] [Green Version]
- van der Bent, A.; Duggan, E.M.; Fishman, L.N.; Dickie, B.H. Reality Check: What Happens When Patients with Anorectal Malformations Grow up? A Pilot Study of Medical Care Transition from the Adult Patient Perspective. J. Pediatr. Surg. 2018, 53, 1722–1726. [Google Scholar] [CrossRef] [PubMed]
- Virapongse, A.; Misky, G.J. Self-Identified Social Determinants of Health during Transitions of Care in the Medically Underserved: A Narrative Review. J. Gen. Intern. Med. 2018, 33, 1959–1967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, D.; Winter, S.; Jenetzky, E.; Zwink, N.; Schmiedeke, E.; Maerzheuser, S. Sexual Function in Adults with Anorectal Malformation: Psychosocial Adaptation. German Network for Congenital Uro-REctal Malformations (CURE-Net). Pediatr. Surg. Int. 2012, 28, 789–792. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bokova, E.; Svetanoff, W.J.; Levitt, M.A.; Rentea, R.M. Pediatric Bowel Management Options and Organizational Aspects. Children 2023, 10, 633. https://doi.org/10.3390/children10040633
Bokova E, Svetanoff WJ, Levitt MA, Rentea RM. Pediatric Bowel Management Options and Organizational Aspects. Children. 2023; 10(4):633. https://doi.org/10.3390/children10040633
Chicago/Turabian StyleBokova, Elizaveta, Wendy Jo Svetanoff, Marc Aaron Levitt, and Rebecca Maria Rentea. 2023. "Pediatric Bowel Management Options and Organizational Aspects" Children 10, no. 4: 633. https://doi.org/10.3390/children10040633