
Activity-Based Restorative Therapy Promotes Progression from Asymmetry to Symmetry in Posture and Gait in a Child with Chronic, Incomplete Spinal Cord Injury

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
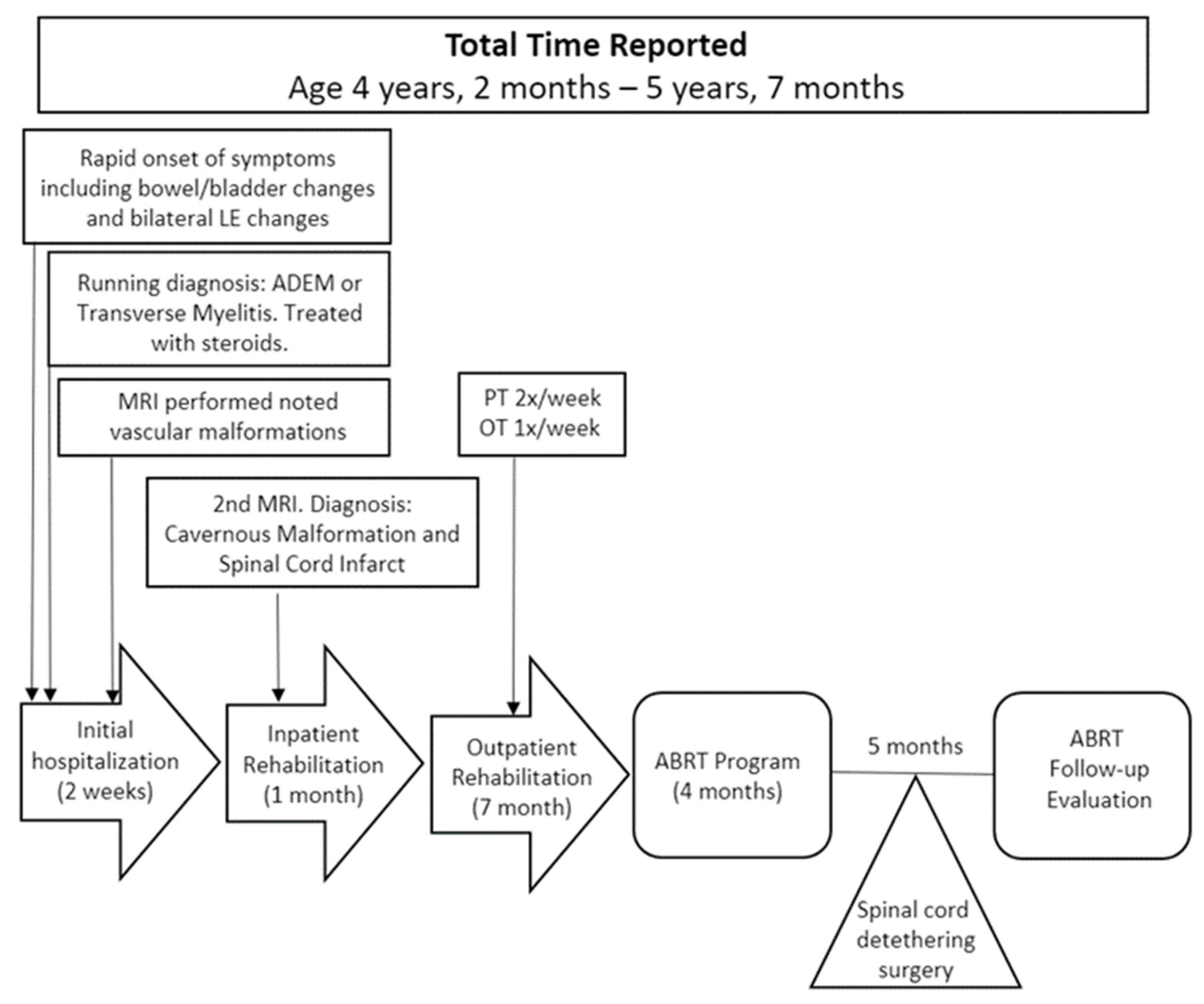
2. Case Presentation
2.1. Medical History from Chart Review
2.2. Initiation of Activity-Based Restorative Therapy
2.3. Postural Alignment
2.4. Gait
2.5. Intervention
2.6. Follow-Up
3. Results
3.1. Postural
3.2. Gait
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Calhoun Thielen, C.; Johnston, T.; Krey, C. Spinal Cord Injury. In Campbell’s Physical Therapy for Children, 5th ed.; Palisano, R., Orlin, M.N., Schreiber, J.S., Eds.; Elsevier Inc.: Toronto, ON, Canada, 2017; pp. 501–524. [Google Scholar]
- Wirz, M.; Zörner, B.; Rupp, R.; Dietz, V. Outcome after incomplete spinal cord injury: Central cord versus Brown-Sequard syndrome. Spinal Cord 2010, 48, 407–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franges, E.Z. Solving the puzzle of Brown-Séquard syndrome. Nursing 2021, 51, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Schottler, J.; Vogel, L.C.; Sturm, P. Spinal cord injuries in young children: A review of children injured at 5 years of age and younger. Dev. Med. Child Neurol. 2012, 54, 1138–1143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulcahey, M.; Gaughan, J.P.; Betz, R.R.; Samdani, A.F.; Barakat, N.; Hunter, L.N. Neuromuscular scoliosis in children with spinal cord injury. Top. Spinal Cord Inj. Rehabil. 2013, 19, 96–103. [Google Scholar] [CrossRef] [Green Version]
- Wang, P.; Low, K.; McGregor, A.H.; Tow, A. Detection of abnormal muscle activations during walking following spinal cord injury (SCI). Res. Dev. Disabil. 2013, 34, 1226–1235. [Google Scholar] [CrossRef]
- Musselman, K.E.; Yang, J.F. Walking tasks encountered by urban-dwelling adults and persons with incomplete spinal cord injuries. J. Rehabil. Med. 2007, 39, 567–574. [Google Scholar] [CrossRef] [Green Version]
- Behrman, A.L.; Nair, P.M.; Bowden, M.G.; Dauser, R.C.; Herget, B.R.; Martin, J.B.; Phadke, C.P.; Reier, P.J.; Senesac, C.R.; Thompson, F.J.; et al. Locomotor training restores walking in a nonambulatory child with chronic, severe, incomplete cervical spinal cord injury. Phys. Ther. 2008, 88, 580–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Day, K.V.; Kautz, S.A.; Wu, S.S.; Suter, S.P.; Behrman, A.L. Foot placement variability as a walking balance mechanism post-spinal cord injury. Clin. Biomech. 2012, 27, 145–150. [Google Scholar] [CrossRef] [Green Version]
- Prosser, L.A. Locomotor training within an inpatient rehabilitation program after pediatric incomplete spinal cord injury. Phys. Ther. 2007, 87, 1224–1232. [Google Scholar] [CrossRef] [Green Version]
- Fox, E.J.; Tester, N.J.; Phadke, C.P.; Nair, P.M.; Senesac, C.R.; Howland, D.R.; Behrman, A.L. Ongoing walking recovery 2 years after locomotor training in a child with severe incomplete spinal cord injury. Phys. Ther. 2010, 90, 793–802. [Google Scholar] [CrossRef] [Green Version]
- Arora, T.; Musselman, K.E.; Lanovaz, J.L.; Linassi, G.; Arnold, C.; Milosavljevic, S.; Oates, A. Walking Stability During Normal Walking and Its Association with Slip Intensity Among Individuals with Incomplete Spinal Cord Injury. PM R 2019, 11, 270–277. [Google Scholar] [CrossRef] [Green Version]
- Behrman, A.L.; Watson, E.; Fried, G.; D’Urso, K.; D’Urso, D.; Cavadini, N.; Brooks, M.; Kern, M.; Wenzel, L.; Taylor, H.; et al. Restorative rehabilitation entails a paradigm shift in pediatric incomplete spinal cord injury in adolescence: An illustrative case series. J. Pediatr. Rehabil. Med. 2012, 5, 245–259. [Google Scholar] [CrossRef]
- Bowden, M.G.; Hannold, E.M.; Nair, P.M.; Fuller, L.B.; Behrman, A.L. Beyond gait speed: A case report of a multidimensional approach to locomotor rehabilitation outcomes in incomplete spinal cord injury. J. Neurol. Phys. Ther. 2008, 32, 129–138. [Google Scholar] [CrossRef]
- Matsubara, J.H.; Wu, M.; Gordon, K.E. Metabolic cost of lateral stabilization during walking in people with incomplete spinal cord injury. Gait Posture 2015, 41, 646–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wirz, M.; van Hedel, H.J.A. Balance, gait, and falls in spinal cord injury. Handb. Clin. Neurol. 2018, 159, 367–384. [Google Scholar] [PubMed]
- Behrman, A.L.; Ardolino, E.M.; Harkema, S.J. Activity-Based Therapy: From Basic Science to Clinical Application for Recovery After Spinal Cord Injury. J. Neurol. Phys. Ther. 2017, 41 (Suppl. 3), S39–S45. [Google Scholar] [CrossRef]
- Dolbow, D.R.; Gorgey, A.S.; Recio, A.C.; Stiens, S.A.; Curry, A.C.; Sadowsky, C.L.; Gater, D.R.; Martin, R.; McDonald, J.W. Activity-Based Restorative Therapies after Spinal Cord Injury: Inter-institutional conceptions and perceptions. Aging Dis. 2015, 6, 254–261. [Google Scholar] [CrossRef] [Green Version]
- Sadowsky, C.L.; McDonald, J.W. Activity-based restorative therapies: Concepts and applications in spinal cord injury-related neurorehabilitation. Dev. Disabil. Res. Rev. 2009, 15, 112–116. [Google Scholar] [CrossRef]
- Harkema, S.J.; Behrman, A.L.; Barbeau, H. Locomotor Training: Principles and Practice; Oxford University Press, Inc.: New York, NY, USA, 2011. [Google Scholar]
- Roy, R.R.; Harkema, S.J.; Edgerton, V.R. Basic concepts of activity-based interventions for improved recovery of motor function after spinal cord injury. Arch. Phys. Med. Rehabil. 2012, 93, 1487–1497. [Google Scholar] [CrossRef] [PubMed]
- Butler, P.; Saavedra, M.S.; Sofranac, M.M.; Jarvis, M.S.; Woollacott, M. Refinement, reliability, and validity of the segmental assessment of trunk control. Pediatr. Phys. Ther. 2010, 22, 246–257. [Google Scholar] [CrossRef] [Green Version]
- Arsh, A.; Darain, H.; Rahman, M.U.; Ullah, I.; Shakil-Ur-Rehman, S. Reliability of modified functional reach test in the assessment of balance function in people with spinal cord injury: A systematic review. J. Pak. Med. Assoc. 2021, 71, 2040–2044. [Google Scholar] [PubMed]
- Behrman, A.L.; Argetsinger, L.C.; Roberts, M.T.; Stout, D.; Thompson, J.; Ugiliweneza, B.; Trimble, S.A. Activity-Based Therapy Targeting Neuromuscular Capacity After Pediatric-Onset Spinal Cord Injury. Top. Spinal Cord Inj. Rehabil. 2019, 25, 132–149. [Google Scholar] [CrossRef] [PubMed]
- de Baptista, C.R.; Vicente, A.M.; Souza, M.A.; Cardoso, J.; Ramalho, V.M.; Mattiello-Sverzut, A.C. Methods of 10-Meter Walk Test and Repercussions for Reliability Obtained in Typically Developing Children. Rehabil. Res. Pract. 2020, 2020, 4209812. [Google Scholar] [CrossRef]
- van Hedel, H.J.; Wirz, M.; Dietz, V. Assessing walking ability in subjects with spinal cord injury: Validity and reliability of 3 walking tests. Arch. Phys. Med. Rehabil. 2005, 86, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Witherspoon, J.W.; Vasavada, R.; Logaraj, R.H.; Waite, M.; Collins, J.; Shieh, C.; Meilleur, K.; Bönnemann, C.; Jain, M. Two-minute versus 6-minute walk distances during 6-minute walk test in neuromuscular disease: Is the 2-minute walk test an effective alternative to a 6-minute walk test? Eur. J. Paediatr. Neurol. 2019, 23, 165–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Argetsinger, L.C.; Trimble, S.A.; Roberts, M.T.; Thompson, J.E.; Ugiliweneza, B.; Behrman, A.L. Sensitivity to change and responsiveness of the Segmental Assessment of Trunk Control (SATCo) in children with spinal cord injury. Dev. Neurorehabil. 2019, 22, 260–271. [Google Scholar] [CrossRef]
- Bartlett, D.; Birmingham, T. Validity and reliability of a pediatric reach test. Pediatr. Phys. Ther. 2003, 15, 84–92. [Google Scholar] [CrossRef]
- Franjoine, M.R.; Gunther, J.S.; Taylor, M.J. Pediatric balance scale: A modified version of the berg balance scale for the school-age child with mild to moderate motor impairment. Pediatr. Phys. Ther. 2003, 15, 114–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Field-Fote, E.C.; Fluet, G.G.; Schafer, S.D.; Schneider, E.M.; Smith, R.; Downey, P.A.; Ruhl, C.D. The Spinal Cord Injury Functional Ambulation Inventory (SCI-FAI). J. Rehabil. Med. 2001, 33, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Norris, R.A.; Wilder, E.; Norton, J. The functional reach test in 3- to 5-year-old children without disabilities. Pediatr. Phys. Ther. 2008, 20, 47–52. [Google Scholar] [CrossRef]
- Voss, S.; Joyce, J.; Biskis, A.; Parulekar, M.; Armijo, N.; Zampieri, C.; Tracy, R.; Palmer, A.S.; Fefferman, M.; Ouyang, B.; et al. Normative database of spatiotemporal gait parameters using inertial sensors in typically developing children and young adults. Gait Posture 2020, 80, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Brazg, G.; Fahey, M.; Holleran, C.L.; Connolly, M.; Woodward, J.; Hennessy, P.W.; Schmit, B.D.; Hornby, T.G. Effects of Training Intensity on Locomotor Performance in Individuals With Chronic Spinal Cord Injury: A Randomized Crossover Study. Neurorehabil. Neural Repair 2017, 31, 944–954. [Google Scholar] [CrossRef] [Green Version]
- Hornby, T.G.; Reisman, D.S.; Ward, I.G.; Scheets, P.L.; Miller, A.; Haddad, D.; Fox, E.J.; Fritz, N.E.; Hawkins, K.; Henderson, C.E.; et al. Clinical Practice Guideline to Improve Locomotor Function Following Chronic Stroke, Incomplete Spinal Cord Injury, and Brain Injury. J. Neurol. Phys. Ther. 2020, 44, 49–100. [Google Scholar] [CrossRef]
- Harkema, S.J.; Schmidt-Read, M.; Lorenz, D.J.; Edgerton, V.R.; Behrman, A.L. Balance and ambulation improvements in individuals with chronic incomplete spinal cord injury using locomotor training-based rehabilitation. Arch. Phys. Med. Rehabil. 2012, 93, 1508–1517. [Google Scholar] [CrossRef] [PubMed]
- Howland, D.R.; Trimble, S.A.; Fox, E.J.; Tester, N.J.; Spiess, M.R.; Senesac, C.R.; Kleim, J.A.; Spierre, L.Z.; Rose, D.K.; Johns, J.S.; et al. Recovery of walking in nonambulatory children with chronic spinal cord injuries: Case series. J. Neurosci. Res. 2023. [Google Scholar] [CrossRef] [PubMed]
- Morris, P.J. Physical activity recommendations for children and adolescents with chronic disease. Curr. Sports Med. Rep. 2008, 7, 353–358. [Google Scholar] [CrossRef] [Green Version]
- Calhoun, C.L.; Schottler, J.; Vogel, L.C. Recommendations for mobility in children with spinal cord injury. Top. Spinal Cord Inj. Rehabil. 2013, 19, 142–151. [Google Scholar] [CrossRef] [Green Version]
- Jefferies, P.; Ungar, M.; Aubertin, P.; Kriellaars, D. Physical Literacy and Resilience in Children and Youth. Front. Public Health 2019, 7, 346. [Google Scholar] [CrossRef] [Green Version]
- Rowland, E.; Knibbe, T.J.; English, K.; Lindsay, S.; McPherson, A.C. “Oh I try, but it’s so hard”: Parental experiences of health promotion in children with disabilities. Disabil. Rehabil. 2022, 44, 5133–5140. [Google Scholar] [CrossRef]
- Keller, A.; Singh, G.; Sommerfeld, J.H.; King, M.; Parikh, P.; Ugiliweneza, B.; D’Amico, J.; Gerasimenko, Y.; Behrman, A.L. Noninvasive spinal stimulation safely enables upright posture in children with spinal cord injury. Nat. Commun. 2021, 12, 5850. [Google Scholar] [CrossRef]
- Gill, M.L.; Grahn, P.J.; Calvert, J.S.; Linde, M.B.; Lavrov, I.A.; Strommen, J.A.; Beck, L.A.; Sayenko, D.G.; Van Straaten, M.G.; Drubach, D.I.; et al. Neuromodulation of lumbosacral spinal networks enables independent stepping after complete paraplegia. Nat. Med. 2018, 24, 1677–1682. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.; Lucas, K.; Keller, A.; Martin, O.R.; Behrman, A.; Vissarionov, S.; Gerasimenko, Y.P. Transcutaneous Spinal Stimulation From Adults to Children: A Review. Top. Spinal Cord Inj. Rehabil. 2023, 29, 16–32. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leon Machado, L.; Lucas, K.; Behrman, A.L. Activity-Based Restorative Therapy Promotes Progression from Asymmetry to Symmetry in Posture and Gait in a Child with Chronic, Incomplete Spinal Cord Injury. Children 2023, 10, 594. https://doi.org/10.3390/children10030594
Leon Machado L, Lucas K, Behrman AL. Activity-Based Restorative Therapy Promotes Progression from Asymmetry to Symmetry in Posture and Gait in a Child with Chronic, Incomplete Spinal Cord Injury. Children. 2023; 10(3):594. https://doi.org/10.3390/children10030594
Chicago/Turabian StyleLeon Machado, Laura, Kathryn Lucas, and Andrea L. Behrman. 2023. "Activity-Based Restorative Therapy Promotes Progression from Asymmetry to Symmetry in Posture and Gait in a Child with Chronic, Incomplete Spinal Cord Injury" Children 10, no. 3: 594. https://doi.org/10.3390/children10030594