

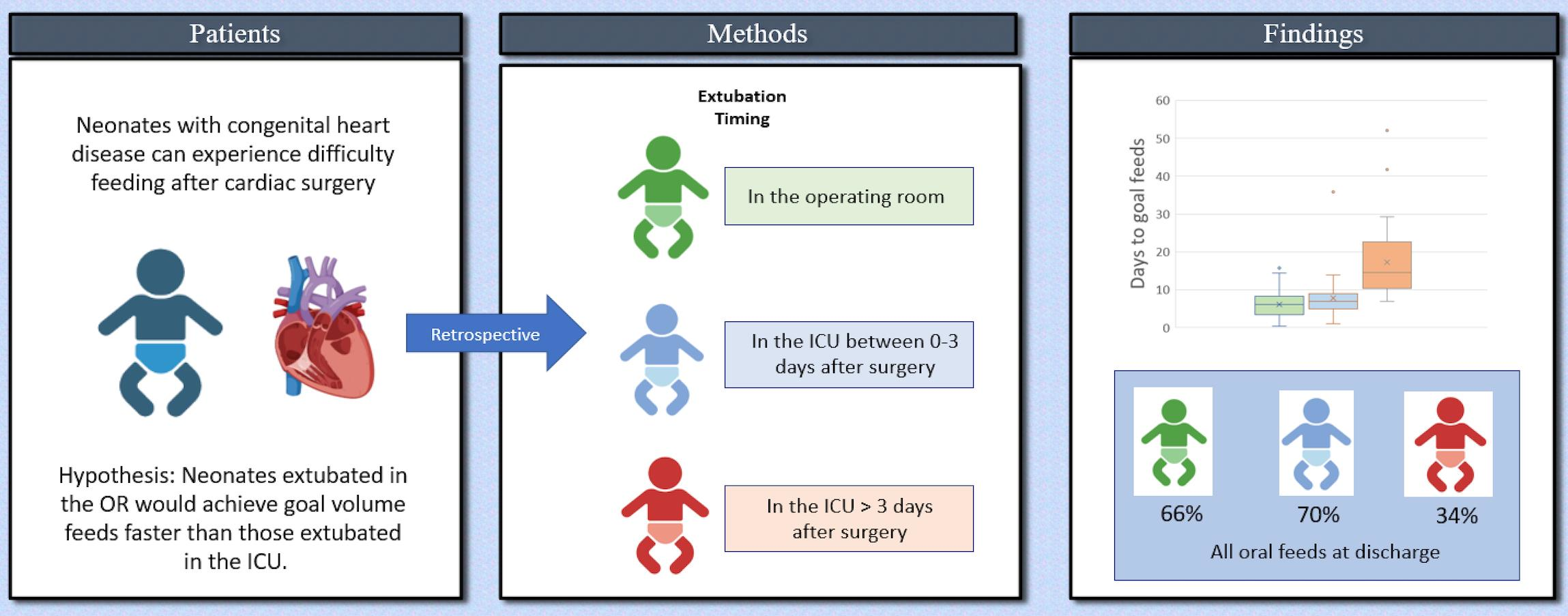
Impact of Extubation Time on Feeding Outcomes after Neonatal Cardiac Surgery: A Single-Center Study

Abstract
:
1. Introduction
2. Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tirotta, C.F.; Alcos, S.; Lagueruela, R.G.; Salyakina, D.; Wang, W.; Hughes, J.; Irizarry, M.; Burke, R.P. Three-Year Experience with Immediate Extubation in Pediatric Patients after Congenital Cardiac Surgery. J. Cardiothorac. Surg. 2020, 15, 1. [Google Scholar] [CrossRef] [PubMed]
- Neirotti, R.A.; Jones, D.; Hackbarth, R.; Paxson Fosse, G. Early Extubation in Congenital Heart Surgery. Heart Lung Circ. 2002, 11, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Harrison, A.M.; Cox, A.C.; Davis, S.; Piedmonte, M.; Drummond-Webb, J.; Mee, R.B.B. Failed Extubation after Cardiac Surgery in Young Children: Prevalence, Pathogenesis, and Risk Factors. Pediatr. Crit. Care Med. 2002, 3, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Mittnacht, A.J.C.; Thanjan, M.; Srivastava, S.; Joashi, U.; Bodian, C.; Hossain, S.; Kin, N.; Hollinger, I.; Nguyen, K. Extubation in the Operating Room after Congenital Heart Surgery in Children. J. Thorac. Cardiovasc. Surg. 2008, 136, 88–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahle, W.T.; Jacobs, J.P.; Jacobs, M.L.; Kim, S.; Kirshbom, P.M.; Pasquali, S.K.; Austin, E.H.; Kanter, K.R.; Nicolson, S.C.; Hill, K.D. Early Extubation After Repair of Tetralogy of Fallot and the Fontan Procedure: An Analysis of The Society of Thoracic Surgeons Congenital Heart Surgery Database. Ann. Thorac. Surg. 2016, 102, 850–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, K.C.; Holowachuk, S.; Pitfield, S.; Sanatani, S.; Froese, N.; Potts, J.E.; Gandhi, S.K. Should Early Extubation Be the Goal for Children after Congenital Cardiac Surgery? J. Thorac. Cardiovasc. Surg. 2014, 148, 2642–2647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varghese, J.; Kutty, S.; Abdullah, I.; Hall, S.; Shostrom, V.; Hammel, J.M. Preoperative and Intraoperative Predictive Factors of Immediate Extubation After Neonatal Cardiac Surgery. Ann. Thorac. Surg. 2016, 102, 1588–1595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heinle, J.S.; Fox, L.S.; Diaz, L.K. Early Extubation after Cardiac Operations in Neonates and Young Infants. J. Thorac. Cardiovasc. Surg. 1997, 114, 413–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, S.; Worley, S.; Mee, R.B.; Harrison, A.M. Factors Associated with Early Extubation after Cardiac Surgery in Young Children. Pediatr. Crit. Care Med. 2004, 5, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Mahle, W.; Nicolson, S.; Hollenbeck-Pringle, D. Utilizing a Collaborative Learning Model to Promote Early Extubation Following Infant Heart Surgery: Erratum. Pediatr. Crit. Care Med. 2018, 19, 386–387. [Google Scholar] [CrossRef] [PubMed]
- Yu, A.-L.; Cai, X.-Z.; Gao, X.-J.; Zhang, Z.-W.; Ma, Z.-S.; Ma, L.-L.; Wang, L.-X. Determinants of Immediate Extubation in the Operating Room after Total Thoracoscopic Closure of Congenital Heart Defects. Med. Princ. Pract. 2013, 22, 234–238. [Google Scholar] [CrossRef] [PubMed]
- Kogon, B.E.; Ramaswamy, V.; Todd, K.; Plattner, C.; Kirshbom, P.M.; Kanter, K.R.; Simsic, J. Feeding Difficulty in Newborns Following Congenital Heart Surgery. Congenit. Heart Dis. 2007, 2, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Jadcherla, S.R.; Vijayapal, A.S.; Leuthner, S. Feeding Abilities in Neonates with Congenital Heart Disease: A Retrospective Study. J. Perinatol. 2009, 29, 112–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Einarson, K.; Arthur, H. Predictors of Oral Feeding Difficulty in Cardiac Surgical Infants. Pediatr. Nurs. 2003, 29, 315–319. [Google Scholar] [PubMed]
- Tabib, A.; Abrishami, S.E.; Mahdavi, M.; Mortezaeian, H.; Totonchi, Z. Predictors of Prolonged Mechanical Ventilation in Pediatric Patients After Cardiac Surgery for Congenital Heart Disease. Res. Cardiovasc. Med. 2016, 5, e30391. [Google Scholar] [CrossRef] [PubMed]
- Shi, S.; Zhao, Z.; Liu, X.; Shu, Q.; Tan, L.; Lin, R.; Shi, Z.; Fang, X. Perioperative Risk Factors for Prolonged Mechanical Ventilation Following Cardiac Surgery in Neonates and Young Infants. Chest 2008, 134, 768–774. [Google Scholar] [CrossRef] [PubMed]
- Ip, P.; Chiu, C.S.W.; Cheung, Y.F. Risk Factors Prolonging Ventilation in Young Children after Cardiac Surgery: Impact of Noninfectious Pulmonary Complications. Pediatr. Crit. Care Med. 2002, 3, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Rooney, S.R.; Mastropietro, C.W.; Benneyworth, B.; Graham, E.M.; Klugman, D.; Costello, J.; Ghanayem, N.; Zhang, W.; Banerjee, M.; Gaies, M. Influence of Early Extubation Location on Outcomes Following Pediatric Cardiac Surgery. Pediatr. Crit. Care Med. 2020, 21, e915–e921. [Google Scholar] [CrossRef] [PubMed]
- Lagatta, J.M.; Uhing, M.; Acharya, K.; Lavoie, J.; Rholl, E.; Malin, K.; Malnory, M.; Leuthner, J.; Brousseau, D.C. Actual and Potential Impact of a Home Nasogastric Tube Feeding Program for Infants Whose Neonatal Intensive Care Unit Discharge Is Affected by Delayed Oral Feedings. J. Pediatr. 2021, 234, 38. [Google Scholar] [CrossRef] [PubMed]
- Gaies, M.; Pasquali, S.K.; Nicolson, S.C.; Shekerdemian, L.; Witte, M.; Wolf, M.; Zhang, W.; Donohue, J.E.; Mahle, W.T. Sustainability of Infant Cardiac Surgery Early Extubation Practices After Implementation and Study. Ann. Thorac. Surg. 2019, 107, 1427–1433. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Variable | Immediate Extubation n = 32 | Early Extubation n = 43 | Delayed Extubation n = 44 | p-Value |
|---|---|---|---|---|
| Age, days | 5.0 (3.0–6.5) | 4.0 (3.0–6.0) | 5.5 (4.0–7.0) | 0.117 |
| Gestational age | 39.0 (37.6–39.2) | 39.0 (38.0–39.2) | 38.4 (37.3–39.0) | 0.049 |
| Weight, kg | 3.3 (2.9–3.6) | 3.3 (3.1–3.8) | 3.2 (2.7–3.6) | 0.121 |
| Sex (male) | 16 (50%) | 31 (72%) | 26 (59%) | 0.14 |
| Lesion | 0.295 | |||
| Aortic arch hypoplasia/coarctation | 9 (27%) | 13 (30%) | 11 (25%) | |
| Hypoplastic left heart | 4 (13%) | 2 (5%) | 9 (20%) | |
| Interrupted aortic arch | 1 (3%) | 1 (2%) | 3 (7%) | |
| Other two ventricles | 3 (9%) | 2 (5%) | 3 (7%) | |
| Other single ventricle | 1 (3%) | 2 (5%) | 2 (5%) | |
| Pulmonary atresia/IVS 1 | 1 (3%) | 4 (9%) | 2 (5%) | |
| Pulmonary atresia/VSD 2 | 2 (6%) | 0 | 3 (7%) | |
| TAPVR 3 | 2 (6%) | 4 (9%) | 4 (9%) | |
| TGA 4 | 9 (28%) | 13 (30%) | 3 (7%) | |
| Truncus arteriosus | 0 | 2 (5%) | 4 (9%) | |
| Pre-operative feeds | 0.093 | |||
| Oral | 22 (69%) | 23 (53%) | 16 (36%) | |
| Nasogastric | 3 (9%) | 5 (12%) | 12 (27%) | |
| Oral + nasogastric | 0 | 1 (2%) | 2 (5%) | |
| None | 7 (22%) | 14 (33%) | 14 (32%) | |
| Post-operative cyanosis | 14 (42%) | 16 (37%) | 31 (70%) | 0.005 |
| Surgery | 0.058 | |||
| Arch reconstruction | 10 (31%) | 11 (40%) | 16 (36%) | |
| Arterial switch | 8 (25%) | 12 (28%) | 2 (5%) | |
| BTT shunt | 1 (3%) | 4 (9%) | 0 | |
| Norwood + Sano | 4 (13%) | 2 (5%) | 7 (16%) | |
| Other two ventricle repair | 6 (19%) | 2 (5%) | 9 (20%) | |
| Other single-ventricle palliation | 1 (3%) | 1 (2%) | 2 (5%) | |
| TAPVR repair | 1 (3%) | 4 (9%) | 4 (9%) | |
| Truncus arteriosus repair | 1 (3%) | 1 (2%) | 4 (9%) | |
| STAT 5 category | <0.0001 | |||
| 1 | 8 (26%) | 1 (2%) | 2 (5%) | |
| 2 | 1 (3%) | 2 (5%) | 4 (10%) | |
| 3 | 7 (23%) | 11 (26%) | 5 (12%) | |
| 4 | 11 (36%) | 27 (63%) | 23 (55%) | |
| 5 | 4 (13%) | 2 (5%) | 8 (19%) | |
| Cardiopulmonary bypass time, minutes | 83 (53–119) | 86 (61–100) | 120 (83–155) | 0.0004 |
| Cross clamp time, minutes | 39 (15–48) | 36 (19–52) | 58 (39–77) | 0.0004 |
| Variable | Immediate Extubation n = 32 | Early Extubation n = 43 | Delayed Extubation n = 44 | p-Value |
|---|---|---|---|---|
| Time to extubation, days | 0 | 1.6 (0.9–2.1) | 5.2 (4.2–10.6) | <0.0001 |
| Time to first enteral feed, days | 1.3 (1–3.4) | 2.3 (1.1–3.3) | 3.5 (2.2–5.1) | 0.0009 |
| Time to first oral feed, days | 2.0 (1.1–4.5) | 3.1 (1.8–4.4) | 8.4 (5.3–15.6) | <0.0001 |
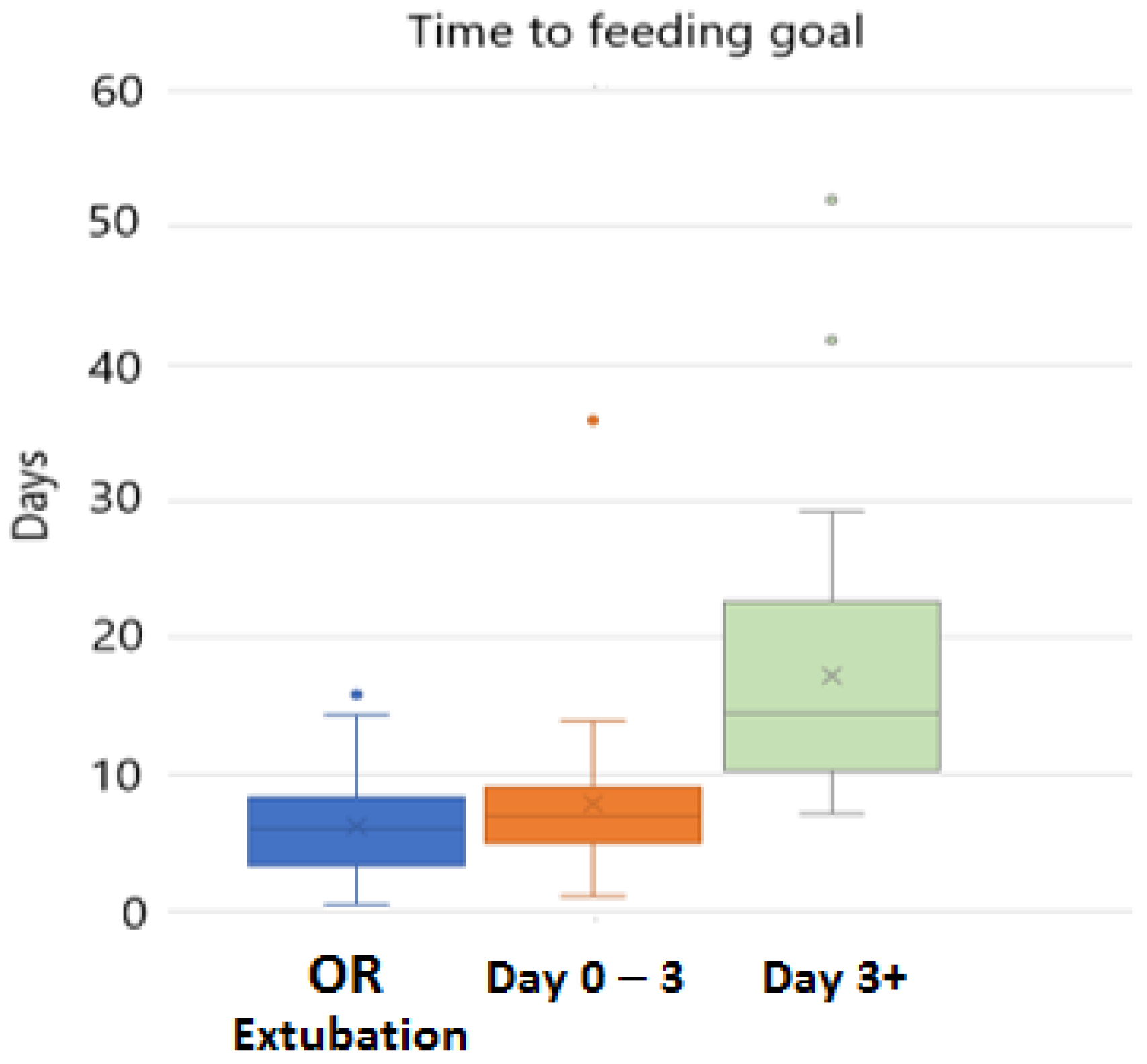
| Time to goal feeds, days | 6.0 (3.2–8.3) | 6.9 (5.0–9.0) | 14.5 (10.4–22.3) | <0.0001 |
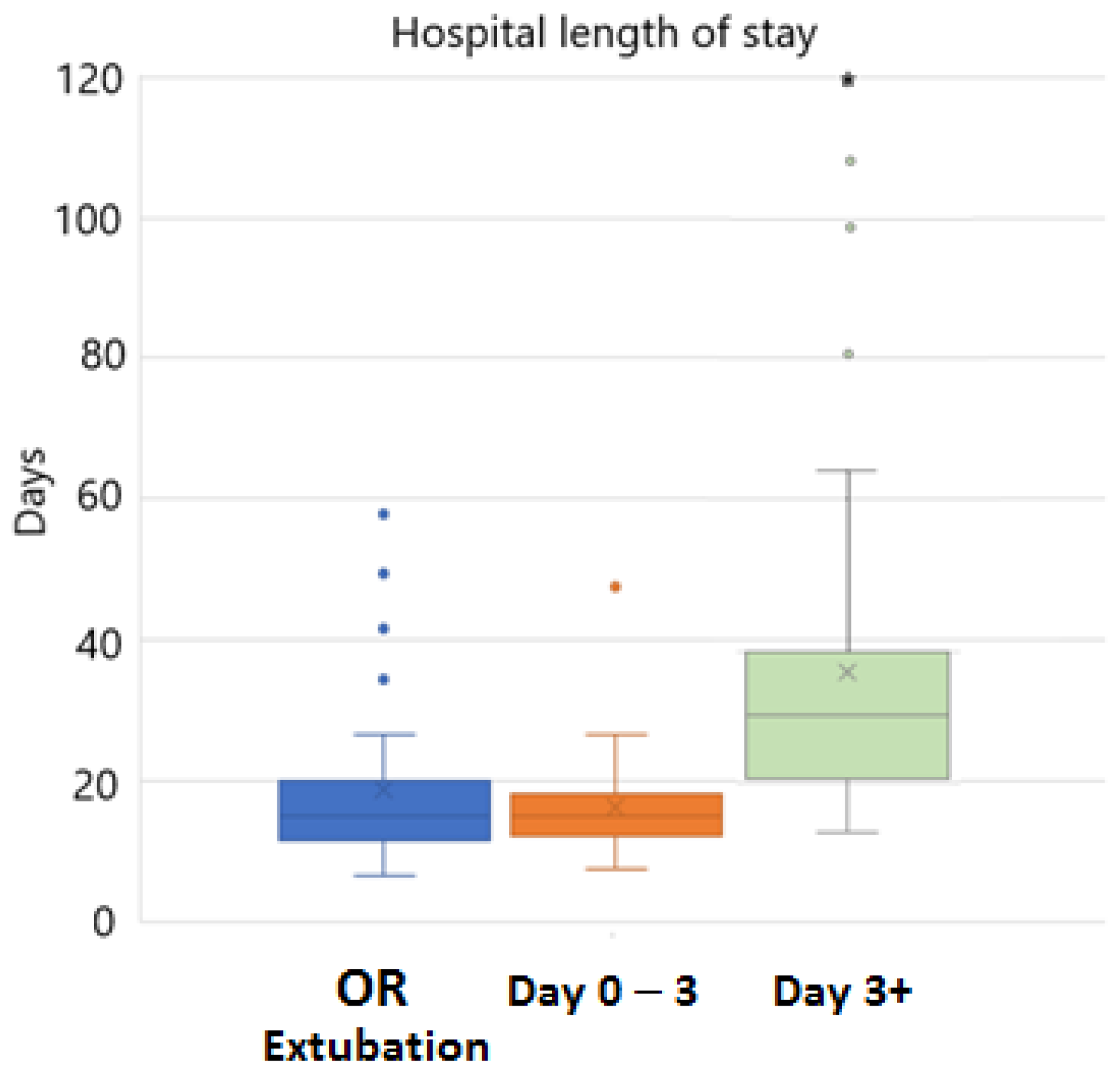
| Length of hospital stay, days | 15.1 (11.6–19.8) | 15.0 (12.3–18.2) | 32.5 (21.2–41.6) | <0.0001 |
| z-score change | −0.8 (−1.1–−0.48) | −1.0 (−1.3–−0.47) | −1.2 (−1.5- −0.74) | 0.057 |
| Type of first feeds post-op | 0.0001 | |||
| Oral | 17 (53%) | 22 (51%) | 5 (11%) | |
| Nasogastric bolus | 9 (28%) | 7 (16%) | 13 (30%) | |
| Nasogastric continuous | 6 (19%) | 14 (33%) | 26 (59%) | |
| Discharge feeds | 0.007 | |||
| All oral | 21 (66%) | 30 (70%) | 15 (34%) | |
| Oral + tube | 7 (22%) | 9 (21%) | 15 (34%) | |
| All tube | 4 (12%) | 4 (9%) | 14 (32%) | |
| Feeds at one year | 0.0002 | |||
| All oral | 24 (75%) | 41 (95%) | 27 (61%) | |
| Oral + tube | 3 (9%) | 1 (2%) | 3 (7%) | |
| All tube | 1 (3%) | 0 | 11 (25%) | |
| Missing data | 4 (13%) | 2 (5%) | 3 (7%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kepple, J.W.; Kendall, M.; Ortmann, L.A. Impact of Extubation Time on Feeding Outcomes after Neonatal Cardiac Surgery: A Single-Center Study. Children 2023, 10, 592. https://doi.org/10.3390/children10030592
Kepple JW, Kendall M, Ortmann LA. Impact of Extubation Time on Feeding Outcomes after Neonatal Cardiac Surgery: A Single-Center Study. Children. 2023; 10(3):592. https://doi.org/10.3390/children10030592
Chicago/Turabian StyleKepple, Jeffrey W., Meghan Kendall, and Laura A. Ortmann. 2023. "Impact of Extubation Time on Feeding Outcomes after Neonatal Cardiac Surgery: A Single-Center Study" Children 10, no. 3: 592. https://doi.org/10.3390/children10030592