
Medication Intake as a Factor for Non-Initiation and Cessation of Breastfeeding: A Prospective Cohort Study in Greece during the COVID-19 Pandemic

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Considerations
- General and Maternity Hospital “HELENA VENIZELOU” (24285/29 October 2019)
- “ATTIKON” General University Hospital (570/1 October 2019)
- “ALEXANDRA” General Hospital (511/20 July 2020)
- “IASO” General Maternity and Gynecology Clinic (30 May 2019)
- “LETO” General, Maternity and Gynecology Clinic (174a/5 June 2019)
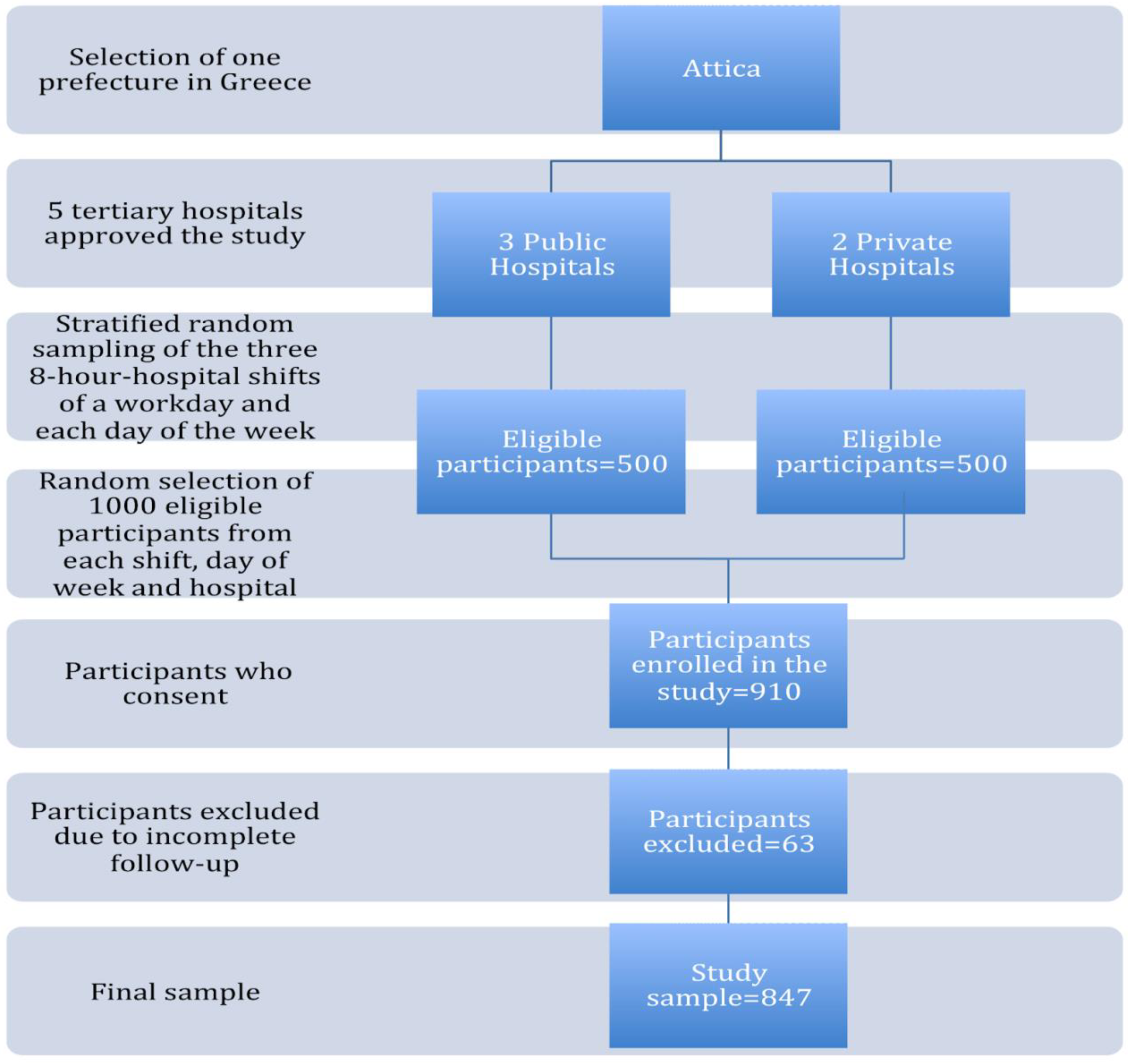
2.2. Sample and Setting
2.3. Data Collection
2.4. Measurements
2.5. Drug Classification
- Lactmed 1 includes the categories: “Compatible”; “Limited Data (LD). Compatible”;
- Lactmed 2 includes the categories: “Probably Compatible”; “Limited Data (LD). Probably Compatible”; “Probably Compatible. May reduce milk supply”;
- Lactmed 3 includes the categories: “Limited Data (LD). Use alternative drugs”; “No Data (ND). Use alternative drugs”; “Use alternative drugs. May suppress lactation”;
- Lactmed 4 includes the categories: “No Data (ND). Use with caution. Avoid during lactation”; “Avoid during lactation. Potential toxicity to the infant”.
- Level 1 (L1): compatible;
- Level 2 (L2): probably compatible: Drug that has been studied in a limited number of breastfeeding women, without an increase in adverse effects in the infant. And/or the evidence of a demonstrated risk which is likely to follow the use of this medication in a breastfeeding woman is remote;
- Level 3 (L3): probably compatible: There are no control studies in breastfeeding women; however, the risk of untoward effects to a breastfed infant is possible, or controlled studies show only minimal non-threatening adverse effects. Drugs should be given only if the potential benefit justifies the potential risk to the infant. (New medications that have absolutely no published data are automatically categorized in this category, regardless of how safe they are);
- Level 4 (L4): potentially hazardous: There is positive evidence of risk to a breastfed infant or to breast milk production, but the benefits of use in breastfeeding mothers may be acceptable despite the risk to the infant;
- Level 5 (L5): hazardous.
- Lactmed 1, Lactmed 2, L1 (Hale) and L2 (Hale);
- Lactmed 3, L3 (Hale);
- Lactmed 4, L4 (Hale) and L5 (Hale).
2.6. Data Analysis
3. Results
3.1. Basic Sample Characteristics
3.2. Maternal Medication Intake during Postpartum Period
3.2.1. Compatibility with Breastfeeding
3.2.2. Medication Intake as a Reason for Breastfeeding Cessation
3.2.3. Factors Associated with Breastfeeding Cessation due to Medication Intake
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shamir, R. The Benefits of Breast Feeding. Nestle Nutr. Inst. Workshop Ser. 2016, 86, 67–76. [Google Scholar] [CrossRef] [Green Version]
- Al-Sawalha, N.A.; Tahaineh, L.; Sawalha, A.; Almomani, B.A. Medication Use in Breastfeeding Women: A National Study. Breastfeed Med. 2016, 11, 386–391. [Google Scholar] [CrossRef]
- Tigka, M.; Metallinou, D.; Pardali, L.; Lykeridou, K. Shared decision-making about medication intake during lactation: A prospective longitudinal study in Greece. Eur. J. Midwifery 2022, 6, 48. [Google Scholar] [CrossRef] [PubMed]
- Hanley, L. Medication Use During Lactation: Either a Potential Contributor to Premature Weaning or Evidence-based Support of the Mother/Child Couplet. Clin. Ther. 2020, 42, 393–400. [Google Scholar] [CrossRef]
- Odom, E.C.; Li, R.; Scanlon, K.S.; Perrine, C.G.; Grummer-Strawn, L. Reasons for earlier than desired cessation of breastfeeding. Pediatrics 2013, 131, e726–e732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saha, M.R.; Ryan, K.; Amir, L.H. Postpartum women’s use of medicines and breastfeeding practices: A systematic review. Int. Breastfeed J. 2015, 10, 28. [Google Scholar] [CrossRef] [PubMed]
- Verstegen, R.H.J.; Ito, S. Drugs in lactation. J. Obs. Gynaecol. Res. 2019, 45, 522–531. [Google Scholar] [CrossRef]
- Byrne, J.J.; Saucedo, A.M.; Spong, C.Y. Evaluation of Drug Labels Following the 2015 Pregnancy and Lactation Labeling Rule. JAMA Netw. Open 2020, 3, e2015094. [Google Scholar] [CrossRef]
- European Medicines Agency. Guideline on Good Pharmacovigilance Practices (GVP). Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/draft-guideline-good-pharmacovigilance-practices-product-population-specific-considerations-iii_en.pdf (accessed on 24 January 2023).
- EU Project on Promotion of Breastfeeding in Europe. Protection, Promotion and Support Of Breastfeeding in Europe: A Blueprint for Action (Revised). European Commission, Directorate Public Health and Risk Assessment, Luxembourg. 2008. Available online: https://www.aeped.es/sites/default/files/6-newblueprintprinter.pdf (accessed on 23 February 2023).
- Institute of Child Health. National Breastfeeding Promotion Initiative “Alkyoni”. Website in Greek. Available online: https://epilegothilasmo.gr/ (accessed on 23 February 2023).
- Elena Venizelou. Special Breastfeeding Promotion Unit—Milk Bank. Website in Greek. Available online: https://www.hospital-elena.gr/medical-services/eidikes-ypiresies/trapeza-galaktos-mitrikos-thilasmos (accessed on 23 February 2023).
- WHO. Director-General Opening Remarks at the Media Briefing on COVID-19-11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 25 February 2023).
- Bode, L. COVID-19 and Human Milk: Are We Prepared for the Next Pandemic? Proceedings 2023, 84, 8. [Google Scholar]
- Wei, S.Q.; Bilodeau-Bertrand, M.; Liu, S.; Auger, N. The impact of COVID-19 on pregnancy outcomes: A systematic review and meta-analysis. CMAJ 2021, 193, E540–E548. [Google Scholar] [CrossRef]
- Ceulemans, M.; Foulon, V.; Panchaud, A.; Winterfeld, U.; Pomar, L.; Lambelet, V.; Cleary, B.; O’Shaughnessy, F.; Passier, A.; Richardson, J.L.; et al. Self-Reported Medication Use among Pregnant and Breastfeeding Women during the COVID-19 Pandemic: A Cross-Sectional Study in Five European Countries. Int. J. Env. Res. Public Health 2022, 19, 1389. [Google Scholar] [CrossRef]
- Tigka, M.; Metallinou, D.; Nanou, C.; Iliodromiti, Z.; Lykeridou, K. Frequency and Determinants of Breastfeeding in Greece: A Prospective Cohort Study during the COVID-19 Pandemic. Children 2022, 9, 43. [Google Scholar] [CrossRef] [PubMed]
- Pallavi, P.P.; Rajesh, K.; Purushothama, R.K.; Ravindra, R.K.; Rama, D.V. Drug use pattern among lactating women in a tertiary care teaching hospital. J. Glob. Trends Pharm. Sci. 2013, 4, 1138–1143. [Google Scholar]
- Schirm, E.; Schwagermann, M.P.; Tobi, H.; de Jong-van den Berg, L.T. Drug use during breastfeeding. A survey from the Netherlands. Eur. J. Clin. Nutr. 2004, 58, 386–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 24 January 2023).
- Drugs and Lactation Database (LactMed). Available online: https://www.ncbi.nlm.nih.gov/books/NBK501922/ (accessed on 24 January 2023).
- Hale, W.T. Hale’s Medication and Mothers’ Milk. A Manual of Lactational Pharmacology, 19th ed.; Springer Publishing: New York, NY, USA, 2021; pp. 20–686. [Google Scholar]
- Silveira, M.P.T.; Possignollo, J.; Miranda, V.I.A.; Silveira, M.F.D.; Pizzol, T.D.S.D.; Serrate, S.; Bertoldi, A.D. Breastfeeding and risk classification of medications used during hospitalization for delivery: 2015 Pelotas Birth Cohort. Rev. Bras. Epidemiol. 2020, 23, e200026. [Google Scholar] [CrossRef]
- Lutz, B.H.; Bassani, D.G.; Miranda, V.I.A.; Silveira, M.P.T.; Mengue, S.S.; Dal Pizzol, T.D.S.; da Silveira, M.F.; Bertoldi, A.D. Use of Medications by Breastfeeding Women in the 2015 Pelotas (Brazil) Birth Cohort Study. Int. J. Env. Res. Public Health 2020, 17, 568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaves, R.M.; Lamounier, J.A.; César, G.C. Association between duration of breastfeeding and drug therapy. Asian Pac. J. Trop. Dis. 2011, 1, 216–221. [Google Scholar] [CrossRef]
- Olesen, C.; Sørensen, H.T.; de Jong-van den Berg, L.; Olsen, J.; Steffensen, F.H. The Euromap Group. Prescribing during pregnancy and lactation with reference to the Swedish classification system. A population-based study among Danish women. Acta Obs. Gynecol. Scand. 1999, 78, 686–692. [Google Scholar] [CrossRef]
- Fomina, Y.Y.; Byrne, J.J.; Spong, C.Y. Evaluating strength of recommendations for commonly administered medications in lactating women. J. Matern. Fetal. Neonatal. Med. 2023, 36, e2163626. [Google Scholar] [CrossRef]
- de Waard, M.; Blomjous, B.S.; Hol, M.L.F.; Sie, S.D.; Corpeleijn, W.E.; van Goudoever, J.H.B.; van Weissenbruch, M.M. Medication Use During Pregnancy and Lactation in a Dutch Population. J. Hum. Lact. 2019, 35, 154–164. [Google Scholar] [CrossRef]
- Spiesser-Robelet, L.; Brunie, V.; de Andrade, V.; Gagnayre, R. Knowledge, Representations, Attitudes, and Behaviors of Women Faced with Taking Medications While Breastfeeding. J. Hum. Lact. 2017, 33, 98–114. [Google Scholar] [CrossRef]
- Brown, A.; Shenker, N. Experiences of breastfeeding during COVID-19: Lessons for future practical and emotional support. Matern. Child Nutr. 2021, 17, e13088. [Google Scholar] [CrossRef] [PubMed]
- Ceulemans, M.; Verbakel, J.Y.; Van Calsteren, K.; Eerdekens, A.; Allegaert, K.; Foulon, V. SARS-CoV-2 Infections and Impact of the COVID-19 Pandemic in Pregnancy and Breastfeeding: Results from an Observational Study in Primary Care in Belgium. Int. J. Env. Res. Public Health 2020, 17, 6766. [Google Scholar] [CrossRef]
- Scime, N.V.; Metcalfe, A.; Nettel-Aguirre, A.; Tough, S.C.; Chaput, K.H. Association of postpartum medication practices with early breastfeeding cessation among mothers with chronic conditions: A prospective cohort study [published online ahead of print, 2023 Jan 27]. Acta Obstet. Gynecol. Scand. 2023, 102, 420–429. [Google Scholar] [CrossRef] [PubMed]
- Chooniedass, R.; Tarrant, M.; Turner, S.; Lok Fan, H.S.; Del Buono, K.; Masina, S.; Becker, A.B.; Mandhane, P.; Turvey, S.E.; Moraes, T.; et al. Factors associated with breast-feeding initiation and continuation in Canadian-born and non-Canadian-born women: A multi-centre study. Public Health Nutr. 2022, 25, 2822–2833. [Google Scholar] [CrossRef]
- Cohen, S.S.; Alexander, D.D.; Krebs, N.F.; Young, B.E.; Cabana, M.D.; Erdmann, P.; Hays, N.P.; Bezold, C.P.; Levin-Sparenberg, E.; Turini, M.; et al. Factors Associated with Breastfeeding Initiation and Continuation: A Meta-Analysis. J. Pediatr. 2018, 203, 190–196.e21. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.; Moretti, M.E.; Collantes, A.; Chong, D.; Mazzotta, P.; Koren, G.; Merchant, S.S.; Ito, S. Choice of breastfeeding and physicians’ advice: A cohort study of women receiving propylthiouracil. Pediatrics 2000, 106, 27–30. [Google Scholar] [CrossRef]
- Acevedo, M.; Pretini, J.; Micelli, M.; Sequeira, G.; Kerzberg, E. Breastfeeding initiation, duration, and reasons for weaning in patients with systemic lupus erythematosus. Rheumatol. Int. 2017, 37, 1183–1186. [Google Scholar] [CrossRef]
- Schaefer, C.; Peters, P.; Miller, R.K. Drugs During Pregnancy and Lactation, 2nd ed.; Elsevier: Oxford, UK, 2007; pp. 644–730. [Google Scholar]
- Tigka, M.; Vivilaki, V.; Metallinou, D.; Nanou, C.; Lykeridou, A. The value of midwifery counseling during lactation as a key factor of pharmacovigilance. Eur. J. Midwifery 2022, 6, 65. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| BF Cessation due to Medication Intake | OR (95% CI) | p-Value |
|---|---|---|
| Qualitative variables | ||
| Physician’s recommendation for BF cessation due to medication intake On physician’s recommendation Women without recommendation by a physician to discontinue BF | 93.9 (45.6–193.4) Ref | <0.001 |
| Medication intake for chronic disease Women who received medication for chronic diseases Women who did not receive medication for chronic diseases | 4.6 (2.6–8.2) Ref | <0.001 |
| Mode of delivery Cesarean section Vaginal delivery | 2.8 (1.4–5.8) Ref | 0.005 |
| Non-employment at 6 months after delivery Not employed Maternity leave Work suspension due to COVID-19 pandemic Teleworking due to COVID-19 pandemic Mothers working at 6 months postpartum | 0.54 (0.27–1.06) 0.10 (0.02–0.40) 0.08 (0.01–0.62) 0.17 (0.05–0.54) Ref | <0.001 |
| Educational level College University Postgraduate studies Women with education up to High School | 0.7 (0.3–1.6) 0.6 (0.3–1.1) 0.2 (0.1–0.6) Ref | 0.034 |
| Nationality Greek Others | Ref | 0.467 |
| Employment before pregnancy Women working before pregnancy Women not working before pregnancy | Ref | 0.727 |
| Quantitative variables | ||
| Previous BF experience (days) | 0.994 (0.992–0.997) | <0.001 |
| Maternal age | 0.444 | |
| Parity | 0.601 | |
| BF Cessation due to Medication Intake | OR (95% CI) | p-Value |
|---|---|---|
| Physician’s recommendation for BF cessation due to medication intake On physician’s recommendation Women without recommendation by a physician to discontinue BF | 171.44 (67.401–436.075) Ref | <0.001 |
| Mode of delivery Cesarean section Vaginal delivery | 6.097 (2.062–18.025) Ref | 0.001 |
| Type of hospital Private Public | 2.261 (0.981–5.209) Ref | 0.055 |
| Smoking before pregnancy (cigarettes/day) | 1.103 (1.059–1.149) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tigka, M.; Metallinou, D.; Nanou, C.; Iliodromiti, Z.; Gryparis, A.; Lykeridou, K. Medication Intake as a Factor for Non-Initiation and Cessation of Breastfeeding: A Prospective Cohort Study in Greece during the COVID-19 Pandemic. Children 2023, 10, 586. https://doi.org/10.3390/children10030586
Tigka M, Metallinou D, Nanou C, Iliodromiti Z, Gryparis A, Lykeridou K. Medication Intake as a Factor for Non-Initiation and Cessation of Breastfeeding: A Prospective Cohort Study in Greece during the COVID-19 Pandemic. Children. 2023; 10(3):586. https://doi.org/10.3390/children10030586
Chicago/Turabian StyleTigka, Maria, Dimitra Metallinou, Christina Nanou, Zoi Iliodromiti, Alexandros Gryparis, and Katerina Lykeridou. 2023. "Medication Intake as a Factor for Non-Initiation and Cessation of Breastfeeding: A Prospective Cohort Study in Greece during the COVID-19 Pandemic" Children 10, no. 3: 586. https://doi.org/10.3390/children10030586