
Natural History of Hazelnut Allergy and Current Approach to Its Diagnosis and Treatment
 , ,
, ,
Abstract
:1. Introduction
2. Natural History of Hazelnut Allergy
2.1. Prevalence of Hazelnut Allergy and First Manifestations
2.2. Cross-Sensitization with Tree Nuts
2.3. Association with Atopic Dermatitis
2.4. Association with Asthma
2.5. Natural Course of Hazelnut Allergy
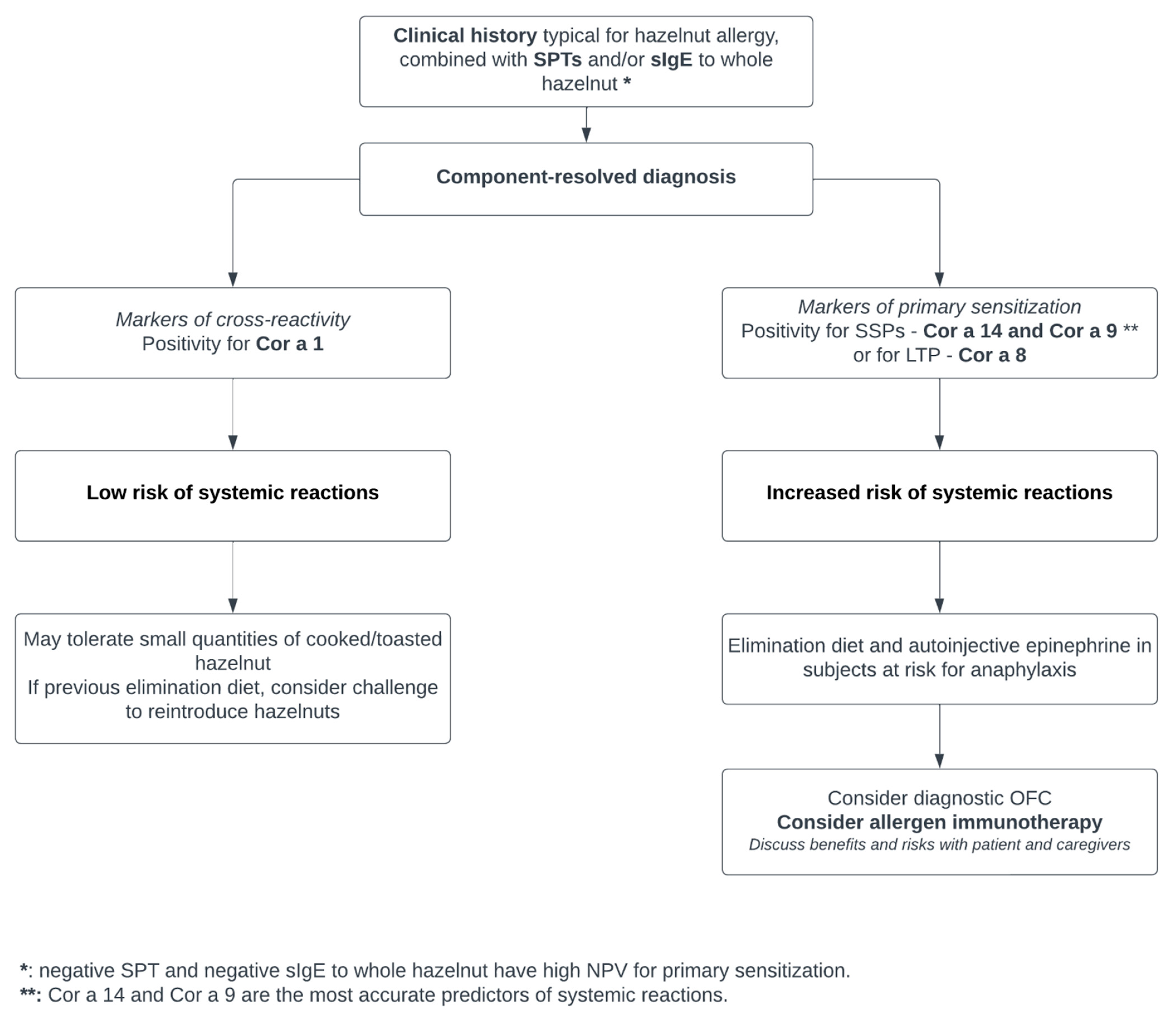
3. Diagnostic Considerations
3.1. Component Resolved Diagnosis
3.2. Basophil Activation Test
4. Prevention and Treatment
4.1. Can We Alter the Natural History of Hazelnut Allergy?
4.1.1. Allergen Immunotherapy
4.1.2. Other Approaches

{kind=link}
| Study, Year, Reference | Study Design | N° of Patients, Age | Intervention | Methods | Outcomes | Safety |
|---|---|---|---|---|---|---|
| Enrique, 2005 [90] | DBRCT | 12 active vs. 11 placebo, 18–60 yrs | SLIT with standardized hazelnut extract (unit masses of major allergens Cor a 1 and Cor a 8) vs. placebo | Buildup over 4 days (hospital), maintenance 5 months (at home). DBPCFC at baseline and after 3 months of maintenance. | Mean ED increased from 2.29 g to 11.56 g | Local reactions 7.4% (itching), systemic reactions 0.2% (only during buildup, no epinephrine required) |
| Enrique, 2008 [91] | Followup study | Same participants | All participants continued SLIT with standardized hazelnut extract on maintenance dose | DBPCFC at baseline and after 1 year on maintenance | ED threshold increase confirmed (mean 14.57 g) and lower sIgE to hazelnut and lower IL-10 | No systemic reactions. |
| Scurlock, 2017 [94] | Prospective cohort | 8, median age 9 yrs | Walnut OIT in patients with allergy to walnut and to another TN (including hazelnut) ** | OFC after 142 weeks of walnut OIT for both walnut and tree nuts. | 88% of desensitization to both walnut and tree nuts | Not reported |
| Elizur, 2019 [40] | Prospective cohort | 73 patients (55 active, 18 controls), median age 7.9 yrs | Walnut OIT in patients with or without co-allergy to pecan/hazelnut/cashew | Initial escalation of 4 days to establish the highest tolerated dose; buildup phase with monthly escalations in clinic, target 4000 mg walnut protein; after desensitization reached, maintenance with daily 1200 mg walnut protein. | Cross-desensitization to hazelnuts in 53% of patients co-allergic to hazelnuts. | 85% mild reactions during buildup in the clinic, 73% at home. 20% required epinephrine use in the clinic. No adverse reactions to hazelnuts consumption in patients who were successfully cross desensitized. |
| Moraly, 2020 [92] | Retrospective | 100, IQR 3–9 yrs | OIT with ground hazelnuts | Monthly buildup from 1/10th ED up to 50% ED. For those not desensitized at 6 mo, new dose buildup scheme. Maintenance with 416 mg hazelnut protein. OFC was performed after 6 mo on OIT and tolerance of 1635 mg of hazelnut protein defined desensitization. | 6 mo: 34% desensitized | No severe reactions |
| Sabouraud, 2022 [93] | Retrospective | 70, median age 10 years (IQR 6–13 yrs) | OIT with cooked hazelnuts | Buildup phase: individual dose definition based on OFC if possible. Daily dose of 10% of target, with progressive dose buildup over 6 mo. Maintenance dose was defined individually. | 12 mo: 51% desensitized | 51% mild, 2.9% severe reactions, 24% hazelnut aversion |
| Fiocchi, 2019 [98] | Real-life efficacy study (observational) | 1, 9 years * | Omalizumab 0.016 mg/kg/IgE every 2 to 4 weeks for 4 months | OFC after 4 months of treatment | ED threshold increase from 13.8 mg to 35′328 mg, measurable (PedsQL questionnaire) improvement in HR-QoL | Well tolerated |
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- McWilliam, V.; Koplin, J.; Lodge, C.; Tang, M.; Dharmage, S.; Allen, K. The Prevalence of Tree Nut Allergy: A Systematic Review. Curr. Allergy Asthma Rep. 2015, 15, 54. [Google Scholar] [CrossRef] [PubMed]
- Grabenhenrich, L.B.; Dölle, S.; Moneret-Vautrin, A.; Köhli, A.; Lange, L.; Spindler, T.; Ruëff, F.; Nemat, K.; Maris, I.; Roumpedaki, E.; et al. Anaphylaxis in children and adolescents: The European Anaphylaxis Registry. J. Allergy Clin. Immunol. 2016, 137, 1128–1137.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calvani, M.; Cardinale, F.; Martelli, A.; Muraro, A.; Pucci, N.; Savino, F.; Zappalà, D.; Panetta, V.; Alamazza, A.; Alessandri, C.; et al. Risk factors for severe pediatric food anaphylaxis in Italy. Pediatr. Allergy Immunol. 2011, 22, 813–819. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Ros, E.; Singh, A.; O’keefe, J.H. Nuts: Natural Pleiotropic Nutraceuticals. Nutrients 2021, 13, 3269. [Google Scholar] [CrossRef]
- Uotila, R.; Kukkonen, A.K.; Pelkonen, A.S.; Mäkelä, M.J. Cross-sensitization profiles of edible nuts in a birch-endemic area. Allergy 2016, 71, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, F.; Mastrorilli, C.; Tripodi, S.; Ricci, G.; Perna, S.; Panetta, V.; Asero, R.; Dondi, A.; Bianchi, A.; Maiello, N.; et al. Diagnostic relevance of IgE sensitization profiles to eight recombinant Phleum pratense molecules. Allergy 2018, 73, 673–682. [Google Scholar] [CrossRef] [PubMed]
- Masthoff, L.J.; Hoff, R.; Verhoeckx, K.C.M.; van Os-Medendorp, H.; Michelsen-Huisman, A.; Baumert, J.L.; Pasmans, S.G.; Meijer, Y.; Knulst, A.C. A systematic review of the effect of thermal processing on the allergenicity of tree nuts. Allergy 2013, 68, 983–993. [Google Scholar] [CrossRef] [Green Version]
- Lyons, S.A.; Clausen, M.; Knulst, A.C.; Ballmer-Weber, B.K.; Fernandez-Rivas, M.; Barreales, L.; Bieli, C.; Dubakiene, R.; Fernandez-Perez, C.; Jedrzejczak-Czechowicz, M.; et al. Prevalence of Food Sensitization and Food Allergy in Children across Europe. J. Allergy Clin. Immunol. Pract. 2020, 8, 2736–2746.e9. [Google Scholar] [CrossRef]
- Datema, M.R.; Zuidmeer-Jongejan, L.; Asero, R.; Barreales, L.; Belohlavkova, S.; de Blay, F.; Bures, P.; Clausen, M.; Dubakiene, R.; Gislason, D.; et al. Hazelnut allergy across Europe dissected molecularly: A EuroPrevall outpatient clinic survey. J. Allergy Clin. Immunol. 2015, 136, 382–391. [Google Scholar] [CrossRef] [Green Version]
- Lyons, S.A.; Burney, P.G.J.; Ballmer-Weber, B.K.; Fernandez-Rivas, M.; Barreales, L.; Clausen, M.; Dubakiene, R.; Fernandez-Perez, C.; Fritsche, P.; Jedrzejczak-Czechowicz, M.; et al. Food Allergy in Adults: Substantial Variation in Prevalence and Causative Foods Across Europe. J. Allergy Clin. Immunol. Pract. 2019, 7, 1920–1928.e11. [Google Scholar] [CrossRef]
- Kuźmiński, A.; Przybyszewski, M.; Przybyszewska, J.; Ukleja-Sokołowska, N.; Pałgan, K.; Bartuzi, Z. Tree nut allergy. Adv. Dermatol. Allergol. 2021, 38, 358–363. [Google Scholar] [CrossRef]
- Fleischer, D.M. The natural history of peanut and tree nut allergy. Curr. Allergy Asthma Rep. 2007, 7, 175–181. [Google Scholar] [CrossRef]
- Stensgaard, A.; Bindslev-Jensen, C.; Nielsen, D.; Munch, M.; DunnGalvin, A. Quality of life in childhood, adolescence and adult food allergy: Patient and parent perspectives. Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 2017, 47, 530–539. [Google Scholar] [CrossRef] [PubMed]
- Flokstra-De Blok, B.M.J.; Dubois, A.E.J.; Vlieg-Boerstra, B.J.; Oude Elberink, J.N.G.; Raat, H.; Dunngalvin, A.; Hourihane, J.O.B.; Duiverman, E.J. Health-related quality of life of food allergic patients: Comparison with the general population and other diseases. Allergy 2010, 65, 238–244. [Google Scholar] [CrossRef]
- van der Valk, J.P.M.; van Wijk, R.G.; Vergouwe, Y.; de Jong, N.W. Failure of introduction of food allergens after negative oral food challenge tests in children. Eur. J. Pediatr. 2015, 174, 1093–1099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grabenhenrich, L.; Trendelenburg, V.; Bellach, J.; Yürek, S.; Reich, A.; Fiandor, A.; Rivero, D.; Sigurdardottir, S.; Clausen, M.; Papadopoulos, N.G.; et al. Frequency of food allergy in school-aged children in eight European countries—The EuroPrevall-iFAAM birth cohort. Allergy 2020, 75, 2294–2308. [Google Scholar] [CrossRef]
- Tagliati, S.; Barni, S.; Giovannini, M.; Liccioli, G.; Sarti, L.; Alicandro, T.; Paladini, E.; Perferi, G.; Azzari, C.; Novembre, E.; et al. Nut Allergy: Clinical and Allergological Features in Italian Children. Nutrients 2021, 13, 4076. [Google Scholar] [CrossRef] [PubMed]
- Haroun-Díaz, E.; Azofra, J.; González-Mancebo, E.; de Las Heras, M.; Pastor-Vargas, C.; Esteban, V.; Villalba, M.; Díaz-Perales, A.; Cuesta-Herranz, J. Nut Allergy in Two Different Areas of Spain: Differences in Clinical and Molecular Pattern. Nutrients 2017, 9, 909. [Google Scholar] [CrossRef] [Green Version]
- Mastrorilli, C.; Cardinale, F.; Giannetti, A.; Caffarelli, C. Pollen-Food Allergy Syndrome: A not so Rare Disease in Childhood. Medicina 2019, 55, 641. [Google Scholar] [CrossRef] [Green Version]
- Valcour, A.; Lidholm, J.; Borres, M.P.; Hamilton, R.G. Sensitization profiles to hazelnut allergens across the United States. Ann. Allergy Asthma Immunol. 2019, 122, 111–116.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanc, F.; Bernard, H.; Ah-Leung, S.; Przybylski-Nicaise, L.; Skov, P.S.; Purohit, A.; de Blay, F.; Ballmer-Weber, B.; Fritsche, P.; Rivas, M.F.; et al. Further studies on the biological activity of hazelnut allergens. Clin. Transl. Allergy 2015, 5, 26. [Google Scholar] [CrossRef] [Green Version]
- Masthoff, L.J.; van Hoffen, E.; de Reus, A.; Boonacker, C.W.; Bruijnzeel-Koomen, C.A.; Pasmans, S.G.; Knulst, A.C. Hazelnut allergy differs between children and adults in frequency of severity, aetiology and relevance of diagnostic parameters. Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 2014, 44, 1539–1545. [Google Scholar] [CrossRef]
- Erhard, S.M.; Bellach, J.; Yürek, S.; Tschirner, S.; Trendelenburg, V.; Grabenhenrich, L.B.; Fernandez-Rivas, M.; van Ree, R.; Keil, T.; Beyer, K. Primary and pollen-associated hazelnut allergy in school-aged children in Germany: A birth cohort study. Allergol. Int. 2021, 70, 463–470. [Google Scholar] [CrossRef]
- Johnson, J.; Malinovschi, A.; Alving, K.; Lidholm, J.; Borres, M.P.; Nordvall, L. Ten-year review reveals changing trends and severity of allergic reactions to nuts and other foods. Acta Paediatr. 2014, 103, 862–867. [Google Scholar] [CrossRef] [PubMed]
- Worm, M.; Scherer, K.; Köhli-Wiesner, A.; Ruëff, F.; Mahler, V.; Lange, L.; Treudler, R.; Rietschel, E.; Szepfalusi, Z.; Lang, R.; et al. Food-induced anaphylaxis and cofactors—Data from the anaphylaxis registry. Allergol. Sel. 2017, 1, 21–27. [Google Scholar] [CrossRef]
- Povesi Dascola, C.; Caffarelli, C. Exercise-induced anaphylaxis: A clinical view. Ital. J. Pediatr. 2012, 38, 43. [Google Scholar] [CrossRef] [Green Version]
- Matias, J.; Gaspar, A.; Sokolova, A.; Borrego, L.M.; Piedade, S.; Pires, G.; Arede, C.; Sampaio, G.; Morais Almeida, M. Tree nuts anaphylaxis in preschool age children. Eur. Ann. Allergy Clin. Immunol. 2020, 52, 182–186. [Google Scholar] [CrossRef] [Green Version]
- Weinberger, T.; Sicherer, S. Current perspectives on tree nut allergy: A review. J. Asthma Allergy 2018, 11, 41–51. [Google Scholar] [CrossRef] [Green Version]
- Cetinkaya, P.G.; Buyuktiryaki, B.; Soyer, O.; Sahiner, U.M.; Sackesen, C.; Sekerel, B.E. Phenotypical characterization of tree nuts and peanut allergies in east Mediterranean children. Allergol. Immunopathol. 2020, 48, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.T.; Ewan, P.W. The development and progression of allergy to multiple nuts at different ages. Pediatr. Allergy Immunol. 2005, 16, 507–511. [Google Scholar] [CrossRef] [PubMed]
- Sicherer, S.H.; Burks, A.W.; Sampson, H.A. Clinical Features of Acute Allergic Reactions to Peanut and Tree Nuts in Children. Pediatrics 1998, 102, e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sicherer, S.H.; Furlong, T.J.; Muñoz-Furlong, A.; Burks, A.W.; Sampson, H.A. A voluntary registry for peanut and tree nut allergy: Characteristics of the first 5149 registrants. J. Allergy Clin. Immunol. 2001, 108, 128–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Midun, E.; Radulovic, S.; Brough, H.; Caubet, J.C. Recent advances in the management of nut allergy. World Allergy Organ. J. 2021, 14, 100491. [Google Scholar] [CrossRef] [PubMed]
- Brough, H.A.; Caubet, J.-C.; Mazon, A.; Haddad, D.; Bergmann, M.M.; Wassenberg, J.; Panetta, V.; Gourgey, R.; Radulovic, S.; Nieto, M.; et al. Defining challenge-proven coexistent nut and sesame seed allergy: A prospective multicenter European study. J. Allergy Clin. Immunol. 2020, 145, 1231–1239. [Google Scholar] [CrossRef] [PubMed]
- Elizur, A.; Appel, M.Y.; Nachshon, L.; Levy, M.B.; Epstein-Rigbi, N.; Golobov, K.; Goldberg, M.R. NUT Co Reactivity—ACquiring Knowledge for Elimination Recommendations (NUT CRACKER) study. Allergy 2018, 73, 593–601. [Google Scholar] [CrossRef]
- Bueno-Díaz, C.; Martín-Pedraza, L.; Parrón, J.; Cuesta-Herranz, J.; Cabanillas, B.; Pastor-Vargas, C.; Batanero, E.; Villalba, M. Characterization of Relevant Biomarkers for the Diagnosis of Food Allergies: An Overview of the 2S Albumin Family. Foods 2021, 10, 1235. [Google Scholar] [CrossRef]
- Dubiela, P.; Kabasser, S.; Smargiasso, N.; Geiselhart, S.; Bublin, M.; Hafner, C.; Mazzucchelli, G.; Hoffmann-Sommergruber, K. Jug r 6 is the allergenic vicilin present in walnut responsible for IgE cross-reactivities to other tree nuts and seeds. Sci. Rep. 2018, 8, 11366. [Google Scholar] [CrossRef] [Green Version]
- Villalta, D.; Scala, E.; Mistrello, G.; Amato, S.; Asero, R. Evidence of Cross-Reactivity between Different Seed Storage Proteins from Hazelnut (Corylus avellana) and Walnut (Juglans regia) Using Recombinant Allergen Proteins. Int. Arch. Allergy Immunol. 2019, 178, 89–92. [Google Scholar] [CrossRef]
- Elizur, A.; Appel, M.Y.; Nachshon, L.; Levy, M.B.; Epstein-Rigbi, N.; Pontoppidan, B.; Lidholm, J.; Goldberg, M.R. Walnut oral immunotherapy for desensitisation of walnut and additional tree nut allergies (Nut CRACKER): A single-centre, prospective cohort study. Lancet Child Adolesc. Health 2019, 3, 312–321. [Google Scholar] [CrossRef]
- Masthoff, L.J.; van Hoffen, E.; Mattsson, L.; Lidholm, J.; Andersson, K.; Zuidmeer-Jongejan, L.; Versteeg, S.A.; Bruijnzeel-Koomen, C.A.; Knulst, A.C.; Pasmans, S.G.; et al. Peanut allergy is common among hazelnut-sensitized subjects but is not primarily the result of IgE cross-reactivity. Allergy 2015, 70, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Bager, J.; Tedner, S.G.; Andersson, N.; Ballardini, N.; Borres, M.P.; Konradsen, J.R.; Nilsson, C.; Westman, M.; Kull, I.; Bergström, A.; et al. Prevalence and early-life risk factors for tree nut sensitization and allergy in young adults. Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 2021, 51, 1429–1437. [Google Scholar] [CrossRef] [PubMed]
- Grewling, L.; Jenerowicz, D.; Nowak, M.; Polańska, A.; Jackowiak, B.; Czarnecka-Operacz, M.; Smith, M. Clinical relevance of Corylus pollen in Poznań, western Poland. Ann. Agric. Environ. Med. 2014, 21, 64–69. [Google Scholar] [PubMed]
- Caffarelli, C.; Dondi, A.; Dascola, C.P.; Ricci, G. Skin prick test to foods in childhood atopic eczema: Pros and cons. Ital. J. Pediatr. 2013, 39, 48. [Google Scholar] [CrossRef] [Green Version]
- Astolfi, A.; Cipriani, F.; Messelodi, D.; De Luca, M.; Indio, V.; Di Chiara, C.; Giannetti, A.; Ricci, L.; Neri, I.; Patrizi, A.; et al. Filaggrin Loss-of-Function Mutations Are Risk Factors for Severe Food Allergy in Children with Atopic Dermatitis. J. Clin. Med. 2021, 10, 233. [Google Scholar] [CrossRef]
- Kalb, B.; Marenholz, I.; Jeanrenaud, A.C.S.N.; Meixner, L.; Arnau-Soler, A.; Rosillo-Salazar, O.D.; Ghauri, A.; Cibin, P.; Blümchen, K.; Schlags, R.; et al. Filaggrin loss-of-function mutations are associated with persistence of egg and milk allergy. J. Allergy Clin. Immunol. 2022, 150, 1125–1134. [Google Scholar] [CrossRef]
- Caffarelli, C.; Garrubba, M.; Greco, C.; Mastrorilli, C.; Dascola, C.P. Asthma and Food Allergy in Children: Is There a Connection or Interaction? Front. Pediatr. 2016, 4, 34. [Google Scholar] [CrossRef] [Green Version]
- Rentzos, G.; Johanson, L.; Sjölander, S.; Telemo, E.; Ekerljung, L. Self-reported adverse reactions and IgE sensitization to common foods in adults with asthma. Clin. Transl. Allergy 2015, 5, 25. [Google Scholar] [CrossRef] [Green Version]
- Johnson, J.; Malinovschi, A.; Lidholm, J.; Petersson, C.J.; Nordvall, L.; Janson, C.; Alving, K.; Borres, M.P. Sensitization to storage proteins in peanut and hazelnut is associated with higher levels of inflammatory markers in asthma. Clin. Mol. Allergy 2020, 18, 11. [Google Scholar] [CrossRef]
- Wood, R.A. The Natural History of Food Allergy. In Food Allergy; John Wiley & Sons Ltd.: Chichester, UK, 2014; pp. 464–474. ISBN 9781118744185. [Google Scholar]
- Stiefel, G.; Anagnostou, K.; Boyle, R.J.; Brathwaite, N.; Ewan, P.; Fox, A.T.; Huber, P.; Luyt, D.; Till, S.J.; Venter, C.; et al. BSACI guideline for the diagnosis and management of peanut and tree nut allergy. Clin. Exp. Allergy 2017, 47, 719–739. [Google Scholar] [CrossRef] [Green Version]
- Caffarelli, C.; Ricò, S.; Rinaldi, L.; Povesi Dascola, C.; Terzi, C.; Bernasconi, S. Blood pressure monitoring in children undergoing food challenge: Association with anaphylaxis. Ann. Allergy Asthma Immunol. 2012, 108, 285–286. [Google Scholar] [CrossRef]
- Eller, E.; Mortz, C.G.; Bindslev-Jensen, C. Cor a 14 is the superior serological marker for hazelnut allergy in children, independent of concomitant peanut allergy. Allergy 2016, 71, 556–562. [Google Scholar] [CrossRef]
- Ho, M.H.K.; Heine, R.G.; Wong, W.; Hill, D.J. Diagnostic accuracy of skin prick testing in children with tree nut allergy. J. Allergy Clin. Immunol. 2006, 117, 1506–1508. [Google Scholar] [CrossRef]
- Buyuktiryaki, B.; Cavkaytar, O.; Sahiner, U.M.; Yilmaz, E.A.; Yavuz, S.T.; Soyer, O.; Sekerel, B.E.; Tuncer, A.; Sackesen, C. Cor a 14, Hazelnut-Specific IgE, and SPT as a Reliable Tool in Hazelnut Allergy Diagnosis in Eastern Mediterranean Children. J. Allergy Clin. Immunol. Pract. 2016, 4, 265–272.e3. [Google Scholar] [CrossRef]
- Masthoff, L.J.; Pasmans, S.G.; Van Hoffen, E.; Knol, M.J.; Bruijnzeel-Koomen, C.A.; Flinterman, A.E.; Kentie, P.; Knulst, A.C.; Meijer, Y. Diagnostic value of hazelnut allergy tests including rCor a 1 spiking in double-blind challenged children. Allergy 2012, 67, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Brettig, T.; Dang, T.; McWilliam, V.; Peters, R.L.; Koplin, J.J.; Perrett, K.P. The Accuracy of Diagnostic Testing in Determining Tree Nut Allergy: A Systematic Review. J. Allergy Clin. Immunol. Pract. 2021, 9, 2028–2049.e2. [Google Scholar] [CrossRef] [PubMed]
- Ortolani, C.; Ballmer-Weber, B.K.; Hansen, K.S.; Ispano, M.; Wüthrich, B.; Bindslev-Jensen, C.; Ansaloni, R.; Vannucci, L.; Pravettoni, V.; Scibilia, J.; et al. Hazelnut allergy: A double-blind, placebo-controlled food challenge multicenter study. J. Allergy Clin. Immunol. 2000, 105, 577–581. [Google Scholar] [CrossRef]
- Beyer, K.; Grabenhenrich, L.; Härtl, M.; Beder, A.; Kalb, B.; Ziegert, M.; Finger, A.; Harandi, N.; Schlags, R.; Gappa, M.; et al. Predictive values of component-specific IgE for the outcome of peanut and hazelnut food challenges in children. Allergy 2015, 70, 90–98. [Google Scholar] [CrossRef]
- Inoue, Y.; Sato, S.; Takahashi, K.; Yanagida, N.; Yamamoto, H.; Shimizu, N.; Ebisawa, M. Component-resolved diagnostics can be useful for identifying hazelnut allergy in Japanese children. Allergol. Int. 2020, 69, 239–245. [Google Scholar] [CrossRef]
- Grabenhenrich, L.; Lange, L.; Härtl, M.; Kalb, B.; Ziegert, M.; Finger, A.; Harandi, N.; Schlags, R.; Gappa, M.; Puzzo, L.; et al. The component-specific to total IgE ratios do not improve peanut and hazelnut allergy diagnoses. J. Allergy Clin. Immunol. 2016, 137, 1751–1760.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, J.; Mafra, I.; Carrapatoso, I.; Oliveira, M.B.P.P. Hazelnut allergens: Molecular characterization, detection, and clinical relevance. Crit. Rev. Food Sci. Nutr. 2016, 56, 2579–2605. [Google Scholar] [CrossRef] [Green Version]
- Pfeifer, S.; Bublin, M.; Dubiela, P.; Hummel, K.; Wortmann, J.; Hofer, G.; Keller, W.; Radauer, C.; Hoffmann-Sommergruber, K. Cor a 14, the allergenic 2S albumin from hazelnut, is highly thermostable and resistant to gastrointestinal digestion. Mol. Nutr. Food Res. 2015, 59, 2077–2086. [Google Scholar] [CrossRef] [Green Version]
- Caffarelli, C.; Mastrorilli, C.; Santoro, A.; Criscione, M.; Procaccianti, M. Component-Resolved Diagnosis of Hazelnut Allergy in Children. Nutrients 2021, 13, 640. [Google Scholar] [CrossRef] [PubMed]
- Uotila, R.; Röntynen, P.; Pelkonen, A.S.; Voutilainen, H.; Kaarina Kukkonen, A.; Mäkelä, M.J. For hazelnut allergy, component testing of Cor a 9 and Cor a 14 is relevant also in birch-endemic areas. Allergy 2020, 75, 2977–2980. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, C.; Scheurer, S.; Rost, K.; Graulich, E.; Jamin, A.; Foetisch, K.; Saloga, J.; Vieths, S.; Steinbrink, K.; Adler, H.S. Cor a 1-reactive T cells and IgE are predominantly cross-reactive to Bet v 1 in patients with birch pollen-associated food allergy to hazelnut. J. Allergy Clin. Immunol. 2013, 131, 1384–1392.e6. [Google Scholar] [CrossRef] [PubMed]
- Offermann, L.R.; Bublin, M.; Perdue, M.L.; Pfeifer, S.; Dubiela, P.; Borowski, T.; Chruszcz, M.; Hoffmann-Sommergruber, K. Structural and Functional Characterization of the Hazelnut Allergen Cor a 8. J. Agric. Food Chem. 2015, 63, 9150–9158. [Google Scholar] [CrossRef] [PubMed]
- Le, T.M.; van Hoffen, E.; Lebens, A.F.M.; Bruijnzeel-Koomen, C.A.F.M.; Knulst, A.C. Anaphylactic versus mild reactions to hazelnut and apple in a birch-endemic area: Different sensitization profiles? Int. Arch. Allergy Immunol. 2013, 160, 56–62. [Google Scholar] [CrossRef]
- Geiselhart, S.; Hoffmann-Sommergruber, K.; Bublin, M. Tree nut allergens. Mol. Immunol. 2018, 100, 71–81. [Google Scholar] [CrossRef]
- Faber, M.A.; De Graag, M.; Van Der Heijden, C.; Sabato, V.; Hagendorens, M.M.; Bridts, C.H.; De Clerck, L.S.; Ebo, D.G. Cor a 14: Missing link in the molecular diagnosis of hazelnut allergy? Int. Arch. Allergy Immunol. 2014, 164, 200–206. [Google Scholar] [CrossRef]
- Kattan, J.D.; Sicherer, S.H.; Sampson, H.A. Clinical reactivity to hazelnut may be better identified by component testing than traditional testing methods. J. Allergy Clin. Immunol. Pract. 2014, 2, 633–634.e1. [Google Scholar] [CrossRef] [Green Version]
- Masthoff, L.J.N.; Mattsson, L.; Zuidmeer-Jongejan, L.; Lidholm, J.; Andersson, K.; Akkerdaas, J.H.; Versteeg, S.A.; Garino, C.; Meijer, Y.; Kentie, P.; et al. Sensitization to Cor a 9 and Cor a 14 is highly specific for a hazelnut allergy with objective symptoms in Dutch children and adults. J. Allergy Clin. Immunol. 2013, 132, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Masthoff, L.J.N.; Blom, W.M.; Rubingh, C.M.; Klemans, R.J.B.; Remington, B.C.; Bruijnzeel-Koomen, C.A.F.M.; van Hoffen, E.; Houben, G.F.; Meyer, Y.; Pasmans, S.G.M.A.; et al. Sensitization to Cor a 9 or Cor a 14 has a strong impact on the distribution of thresholds to hazelnut. J. Allergy Clin. Immunol. Pract. 2018, 6, 2112–2114.e1. [Google Scholar] [CrossRef] [PubMed]
- Giovannini, M.; Comberiati, P.; Piazza, M.; Chiesa, E.; Piacentini, G.L.; Boner, A.; Zanoni, G.; Peroni, D.G. Retrospective definition of reaction risk in Italian children with peanut, hazelnut and walnut allergy through component-resolved diagnosis. Allergol. Immunopathol. 2019, 47, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Nebbia, S.; Lamberti, C.; Cirrincione, S.; Acquadro, A.; Abbà, S.; Ciuffo, M.; Torello Marinoni, D.; Manfredi, M.; Marengo, E.; Calzedda, R.; et al. Oleosin Cor a 15 is a novel allergen for Italian hazelnut allergic children. Pediatr. Allergy Immunol. 2021, 32, 1743–1755. [Google Scholar] [CrossRef]
- Santos, A.F.; Bergmann, M.; Brough, H.A.; Couto-Francisco, N.; Kwok, M.; Panetta, V.; Haddad, D.; Lack, G.; Eigenmann, P.; Caubet, J.-C. Basophil Activation Test Reduces Oral Food Challenges to Nuts and Sesame. J. Allergy Clin. Immunol. Pract. 2021, 9, 2016–2027.e6. [Google Scholar] [CrossRef]
- Duan, L.; Celik, A.; Hoang, J.A.; Schmidthaler, K.; So, D.; Yin, X.; Ditlof, C.M.; Ponce, M.; Upton, J.E.M.; Lee, J.-S.; et al. Basophil activation test shows high accuracy in the diagnosis of peanut and tree nut allergy: The Markers of Nut Allergy Study. Allergy 2021, 76, 1800–1812. [Google Scholar] [CrossRef] [PubMed]
- Brandström, J.; Nopp, A.; Johansson, S.G.O.; Lilja, G.; Sundqvist, A.-C.; Borres, M.P.; Nilsson, C. Basophil allergen threshold sensitivity and component-resolved diagnostics improve hazelnut allergy diagnosis. Clin. Exp. Allergy 2015, 45, 1412–1418. [Google Scholar] [CrossRef]
- Perkin, M.R.; Logan, K.; Tseng, A.; Raji, B.; Ayis, S.; Peacock, J.; Brough, H.; Marrs, T.; Radulovic, S.; Craven, J.; et al. Randomized Trial of Introduction of Allergenic Foods in Breast-Fed Infants. N. Engl. J. Med. 2016, 374, 1733–1743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du Toit, G.; Roberts, G.; Sayre, P.H.; Bahnson, H.T.; Radulovic, S.; Santos, A.F.; Brough, H.A.; Phippard, D.; Basting, M.; Feeney, M.; et al. Randomized Trial of Peanut Consumption in Infants at Risk for Peanut Allergy. N. Engl. J. Med. 2015, 372, 803–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalb, B.; Meixner, L.; Trendelenburg, V.; Unterleider, N.; Dobbertin-Welsch, J.; Heller, S.; Dölle-Bierke, S.; Roll, S.; Lau, S.; Lee, Y.-A.A.; et al. Tolerance induction through early feeding to prevent food allergy in infants with eczema (TEFFA): Rationale, study design, and methods of a randomized controlled trial. Trials 2022, 23, 210. [Google Scholar] [CrossRef]
- NCT04801823 The TreEat Study—Can Early Introduction of Tree Nuts Prevent Tree Nut Allergy in Infants with Peanut Allergy. Available online: https://clinicaltrials.gov/show/NCT04801823 (accessed on 10 January 2023).
- Fleischer, D.M.; Perry, T.T.; Atkins, D.; Wood, R.A.; Burks, A.W.; Jones, S.M.; Henning, A.K.; Stablein, D.; Sampson, H.A.; Sicherer, S.H. Allergic Reactions to Foods in Preschool-Aged Children in a Prospective Observational Food Allergy Study. Pediatrics 2012, 130, e25–e32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardona, V.; Ansotegui, I.J.; Ebisawa, M.; El-Gamal, Y.; Fernandez Rivas, M.; Fineman, S.; Geller, M.; Gonzalez-Estrada, A.; Greenberger, P.A.; Sanchez Borges, M.; et al. World allergy organization anaphylaxis guidance 2020. World Allergy Organ. J. 2020, 13, 100472. [Google Scholar] [CrossRef] [PubMed]
- Durham, S.R.; Shamji, M.H. Allergen immunotherapy: Past, present and future. Nat. Rev. Immunol. 2022, 1–12. [Google Scholar] [CrossRef]
- PALISADE Group of Clinical Investigators. AR101 Oral Immunotherapy for Peanut Allergy. N. Engl. J. Med. 2018, 379, 1991–2001. [Google Scholar] [CrossRef] [PubMed]
- Bégin, P.; Chan, E.S.; Kim, H.; Wagner, M.; Cellier, M.S.; Favron-Godbout, C.; Abrams, E.M.; Ben-Shoshan, M.; Cameron, S.B.; Carr, S.; et al. CSACI guidelines for the ethical, evidence-based and patient-oriented clinical practice of oral immunotherapy in IgE-mediated food allergy. Allergy Asthma Clin. Immunol. 2020, 16, 20. [Google Scholar] [CrossRef] [Green Version]
- Pajno, G.B.; Fernandez-Rivas, M.; Arasi, S.; Roberts, G.; Akdis, C.A.; Alvaro-Lozano, M.; Beyer, K.; Bindslev-Jensen, C.; Burks, W.; Ebisawa, M.; et al. EAACI Guidelines on allergen immunotherapy: IgE-mediated food allergy. Allergy 2018, 73, 799–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nachshon, L.; Schwartz, N.; Levy, M.B.; Goldberg, M.R.; Epstein-Rigbi, N.; Katz, Y.; Elizur, A. Factors Associated with Home Epinephrine-Treated Reactions During Peanuts and Tree-nuts Oral Immunotherapy. Ann. Allergy Asthma Immunol. 2023, 130, 340–346. [Google Scholar] [CrossRef]
- Enrique, E.; Pineda, F.; Malek, T.; Bartra, J.; Basagaña, M.; Tella, R.; Castelló, J.V.; Alonso, R.; De Mateo, J.A.; Cerdá-Trias, T.; et al. Sublingual immunotherapy for hazelnut food allergy: A randomized, double-blind, placebo-controlled study with a standardized hazelnut extract. J. Allergy Clin. Immunol. 2005, 116, 1073–1079. [Google Scholar] [CrossRef]
- Enrique, E.; Malek, T.; Pineda, F.; Palacios, R.; Bartra, J.; Tella, R.; Basagaña, M.; Alonso, R.; Cisteró-Bahíma, A. Sublingual immunotherapy for hazelnut food allergy: A follow-up study. Ann. Allergy Asthma Immunol. 2008, 100, 283–284. [Google Scholar] [CrossRef]
- Moraly, T.; Pelletier de Chambure, D.; Verdun, S.; Preda, C.; Seynave, M.; Vilain, A.C.; Chenivesse, C.; Delebarre-Sauvage, C. Oral Immunotherapy for Hazelnut Allergy: A Single-Center Retrospective Study on 100 Patients. J. Allergy Clin. Immunol. Pract. 2020, 8, 704–709.e4. [Google Scholar] [CrossRef]
- Sabouraud, M.; Biermé, P.; André-Gomez, S.-A.; Villard-Truc, F.; Payot, F.; Corréard, A.-K.; Garnier, L.; Braun, C. Real-life experience with hazelnut oral immunotherapy. Ann. Allergy Asthma Immunol. 2022, 128, 432–438. [Google Scholar] [CrossRef]
- Scurlock, A.M.; Rettiganti, M.; Hiegel, A.M.; Gibson, E.D.; Beckwith, S.; House, S.E.; Sikes, J.D.; Chervinskiy, S.K.; Pesek, R.; Perry, T.T.; et al. Long-term Walnut Oral Immunotherapy Induces Clinically Relevant Treatment Responses in Tree Nut Allergic Children. J. Allergy Clin. Immunol. 2017, 139, AB175. [Google Scholar] [CrossRef]
- Babu, K.S.; Polosa, R.; Morjaria, J.B. Anti-IgE—Emerging opportunities for Omalizumab. Expert Opin. Biol. Ther. 2013, 13, 765–777. [Google Scholar] [CrossRef] [PubMed]
- Dantzer, J.A.; Wood, R.A. Update on omalizumab in allergen immunotherapy. Curr. Opin. Allergy Clin. Immunol. 2021, 21, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Dantzer, J.A.; Wood, R.A. The use of omalizumab in allergen immunotherapy. Clin. Exp. Allergy 2018, 48, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Fiocchi, A.; Artesani, M.C.; Riccardi, C.; Mennini, M.; Pecora, V.; Fierro, V.; Calandrelli, V.; Dahdah, L.; Valluzzi, R.L. Impact of Omalizumab on Food Allergy in Patients Treated for Asthma: A Real-Life Study. J. Allergy Clin. Immunol. Pract. 2019, 7, 1901–1909.e5. [Google Scholar] [CrossRef]
- Rial, M.J.; Barroso, B.; Sastre, J. Dupilumab for treatment of food allergy. J. Allergy Clin. Immunol. Pract. 2019, 7, 673–674. [Google Scholar] [CrossRef]
- Spekhorst, L.S.; van der Rijst, L.P.; de Graaf, M.; van Megen, M.; Zuithoff, N.P.A.; Knulst, A.C.; de Bruin-Weller, M.S.; Le, T.M. Dupilumab has a profound effect on specific-IgE levels of several food allergens in atopic dermatitis patients. Allergy 2022, 78, 875–878. [Google Scholar] [CrossRef]
- Sicherer, S.H.; Sampson, H.A. Food allergy: A review and update on epidemiology, pathogenesis, diagnosis, prevention, and management. J. Allergy Clin. Immunol. 2018, 141, 41–58. [Google Scholar] [CrossRef] [Green Version]

| Study, Year, Reference | Design | Countries | N° of Patients | Age of 1st Reaction | Severity |
|---|---|---|---|---|---|
| Tagliati, 2021 [18] | Retrospective | Italy | 113 with confirmed nut allergy, 43 HA | 3.7 ± 3.2 years | 48% anaphylaxis * |
| Matias, 2020 [28] | Retrospective | Portugal | 25 TN allergy (2 HA) | Mean age 3.1 years ** | This study focused on TN anaphylaxis in preschoolers. There were no fatal events. 16% presented life-threatening glottis edema. |
| Cetinkaya, 2020 [30] | Prospective observational | Turkey | 227 with TN and/or peanut allergy (63.9% HA) | Median age 9 mo. (range 6–12 mo.) | 41.4% anaphylactic reactions after consumption of any TN or peanut |
| Clark, 2005 [31] | Prospective cross-sectional | United Kingdom | 784 peanut or nut allergy, 319 HA | Median 2 years | 28% moderately severe reaction (airway narrowing), 8% severe reactions |
| Sicherer, 2001 [33] | Voluntary registry | USA (5146), Canada (2), United Kingdom (1) | 5149 registrants with peanut or TN allergy (<5% HA) | Median 36 mo., mean 77 mo. | 1st reaction to TN was severe in ca. 30% of cases and a higher proportion of subsequent reactions was severe |
| Sicherer, 1998 [32] | Prospective observational | USA | 122 (54 TN allergy, >5% HA) | Median age 62 mo. (range 10–264 mo.) | 21.6% required epinephrine |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giannetti, A.; Ruggi, A.; Ricci, G.; Giannì, G.; Caffarelli, C. Natural History of Hazelnut Allergy and Current Approach to Its Diagnosis and Treatment. Children 2023, 10, 585. https://doi.org/10.3390/children10030585
Giannetti A, Ruggi A, Ricci G, Giannì G, Caffarelli C. Natural History of Hazelnut Allergy and Current Approach to Its Diagnosis and Treatment. Children. 2023; 10(3):585. https://doi.org/10.3390/children10030585
Chicago/Turabian StyleGiannetti, Arianna, Alessandro Ruggi, Giampaolo Ricci, Giuliana Giannì, and Carlo Caffarelli. 2023. "Natural History of Hazelnut Allergy and Current Approach to Its Diagnosis and Treatment" Children 10, no. 3: 585. https://doi.org/10.3390/children10030585