
Methylation Dynamics on 5′-UTR of DAT1 Gene as a Bio-Marker to Recognize Therapy Success in ADHD Children
 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Recruitment of the Sample
2.2. Building Up of Two Subgroups
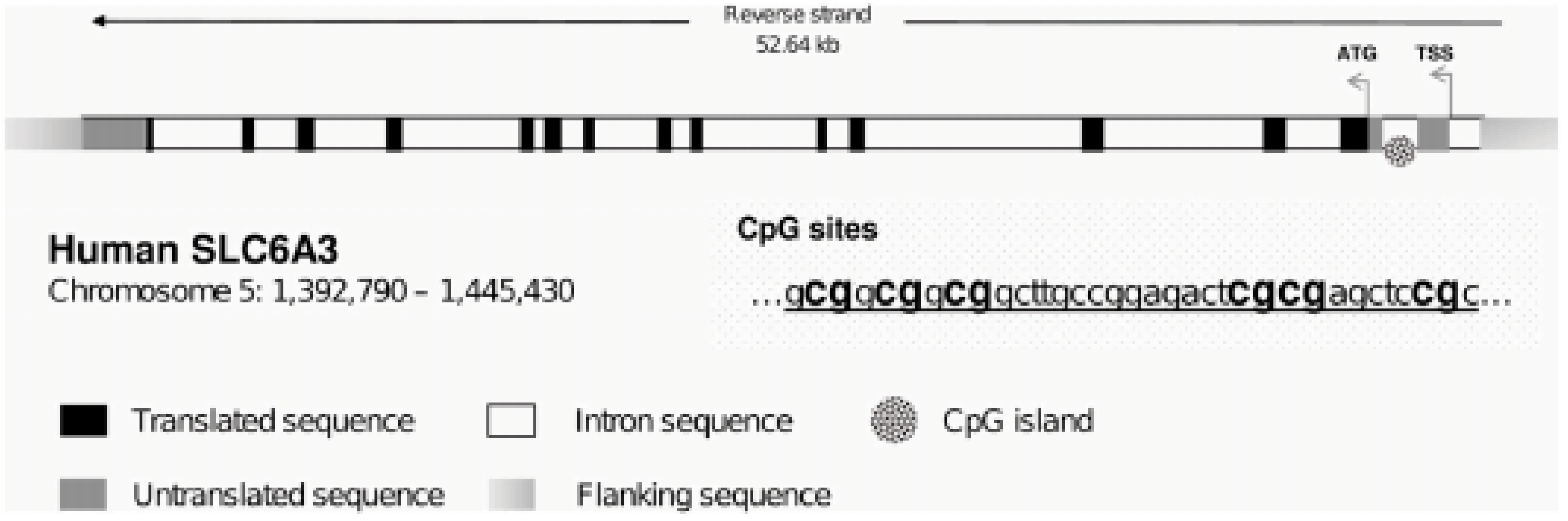
2.3. Measurement of 5′-UTR CpG’s Methylation Level
2.4. Linear Correlation between CpGs: Patterns of Methylation
3. Results
4. Discussion
4.1. Limitations
4.2. Future Perspective
4.3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, TX, USA, 2013; pp. 59–65. [Google Scholar]
- Posner, J.; Polanczyk, G.V.; Sonuga-Barke, E. Attention-deficit hyperactivity disorder. Lancet 2020, 395, 450–462. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Weibman, D.; Halperin, J.M.; Li, X. A Review of Heterogeneity in Attention Deficit/Hyperactivity Disorder (ADHD). Front. Hum. Neurosci. 2019, 13, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swanson, J.M.; Kinsbourne, M.; Nigg, J.; Lanphear, B.; Stefanatos, G.A.; Volkow, N.; Taylor, E.; Casey, B.J.; Castellanos, F.X.; Wadhwa, P.D. Etiologic subtypes of attention-deficit/hyperactivity disorder: Brain imaging, molecular genetic and environmental factors and the dopamine hypothesis. Neuropsychol. Rev. 2007, 17, 39–59. [Google Scholar] [CrossRef] [PubMed]
- Posner, J. The Role of Precision Medicine in Child Psychiatry: What Can We Expect and When? J. Am. Acad. Child Adolesc. Psychiatry 2018, 57, 813–817. [Google Scholar] [CrossRef]
- Posner, J.; Rauh, V.; Gruber, A.; Gat, I.; Wang, Z.; Peterson, B.S. Dissociable attentional and affective circuits in medication-naïve children with attention-deficit/hyperactivity disorder. Psychiatry Res. 2013, 213, 24–30. [Google Scholar] [CrossRef] [Green Version]
- van Mil, N.H.; Steegers-Theunissen, R.P.; Bouwland-Both, M.I.; Verbiest, M.M.; Rijlaarsdam, J.; Hofman, A.; Steegers, E.A.; Heijmans, B.T.; Jaddoe, V.W.; Verhulst, F.C.; et al. DNA methylation profiles at birth and child ADHD symptoms. J. Psychiatr. Res. 2014, 49, 51–59. [Google Scholar] [CrossRef] [Green Version]
- Walton, E.; Pingault, J.B.; Cecil, C.A.; Gaunt, T.R.; Relton, C.L.; Mill, J.; Barker, E.D. Epigenetic profiling of ADHD symptoms trajectories: A prospective, methylome-wide study. Mol. Psychiatry 2017, 22, 250–256. [Google Scholar] [CrossRef] [Green Version]
- Ding, K.; Yang, J.; Reynolds, G.P.; Chen, B.; Shao, J.; Liu, R.; Qian, Q.; Liu, H.; Yang, R.; Wen, J.; et al. DAT1 methylation is associated with methylphenidate response on oppositional and hyperactive-impulsive symptoms in children and adolescents with ADHD. World J. Biol. Psychiatry 2017, 18, 291–299. [Google Scholar] [CrossRef]
- Adriani, W.; Romano, E.; Pucci, M.; Pascale, E.; Cerniglia, L.; Cimino, S.; Tambelli, R.; Curatolo, P.; Granstrem, O.; Maccarrone, M.; et al. Potential for diagnosis versus therapy monitoring of attention deficit hyperactivity disorder: A new epigenetic biomarker interacting with both genotype and auto-immunity. Eur. Child Adolesc. Psychiatry 2018, 27, 241–252. [Google Scholar] [CrossRef]
- Carpentieri, V.; Cerniglia, L.; Cimino, S.; Pucci, M.; Pascale, E.; D’Addario, C.; Adriani, W. Epigenetic regulation of DAT gene promoter modulates the risk of externalizing and internalizing behaviors on a normative population: An explorative study. Behav. Brain Res. 2021, 406, 113246. [Google Scholar] [CrossRef]
- Chmielowiec, J.; Chmielowiec, K.; Strońska-Pluta, A.; Suchanecka, A.; Humińska-Lisowska, K.; Lachowicz, M.; Niewczas, M.; Białecka, M.; Śmiarowska, M.; Grzywacz, A. Methylation in the Promoter Region of the Dopamine Transporter DAT1 Gene in People Addicted to Nicotine. Int. J. Environ. Res. Public Health 2022, 19, 8602. [Google Scholar] [CrossRef]
- Arpón, A.; Milagro, F.I.; Laja, A.; Segura, V.; de Pipaón, M.S.; Riezu-Boj, J.I.; Alfredo Martínez, J. Methylation changes and pathways affected in preterm birth: A role for SLC6A3 in neurodevelopment. Epigenomics 2018, 10, 91–103. [Google Scholar] [CrossRef]
- Lambacher, G.; Pascale, E.; Pucci, M.; Mangiapelo, S.; D’Addario, C.; Adriani, W. Search for an epigenetic biomarker in ADHD diagnosis, based on the DAT1 gene 5′-UTR methylation: A new possible approach. Psychiatry Res. 2020, 291, 113154. [Google Scholar] [CrossRef]
- Carpentieri, V.; Pascale, E.; Cerniglia, L.; Pucci, M.; D’Addario, C.; Laviola, G.; Adriani, W.; Cimino, S. Methylation patterns within 5′-UTR of DAT1 gene as a function of allelic 3′-UTR variants and their maternal or paternal origin: May these affect the psychopathological phenotypes in children? An explorative study. Neurosci. Lett. 2022, 791, 136916. [Google Scholar] [CrossRef]
- Klein, R.G.; Abikoff, H. Behavior therapy and methylphenidate in the treatment of children with ADHD. J. Atten. Disord. 1997, 2, 89–114. [Google Scholar] [CrossRef]
- Evans, S.W.; Pelham, W.E.; Smith, B.H.; Bukstein, O.; Gnagy, E.M.; Greiner, A.R.; Baron-Myak, C. Dose-response effects of methylphenidate on ecologically valid measures of academic performance and classroom behavior in adolescents with ADHD. Exp. Clin. Psychopharmacol. 2001, 9, 163. [Google Scholar] [CrossRef]
- Pan, M.R.; Huang, F.; Zhao, M.J.; Wang, Y.F.; Wang, Y.F.; Qian, Q.J. A comparison of efficacy between cognitive behavioral therapy (CBT) and CBT combined with medication in adults with attention-deficit/hyperactivity disorder (ADHD). Psychiatry Res. 2019, 279, 23–33. [Google Scholar] [CrossRef]
- Chan, E.; Fogler, J.M.; Hammerness, P.G. Treatment of Attention-Deficit/Hyperactivity Disorder in Adolescents: A Systematic Review. JAMA 2016, 315, 1997–2008. [Google Scholar] [CrossRef]
- American Psychiatric Association. Quick Reference to the Diagnostic Criteria from DSM-IV-TR; American Psychiatric Association: Washington, DC, USA, 2000; p. 370. [Google Scholar]
- Kaufman, J.; Birmaher, B.; Brent, D.; Rao, U.; Flynn, C.; Moreci, P.; Williamson, D.; Ryan, N. Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL): Initial reliability and validity data. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 980–988. [Google Scholar] [CrossRef]
- Shaffer, D.; Gould, M.S.; Brasic, J.; Ambrosini, P.; Fisher, P.; Bird, H.; Aluwahlia, S. A children’s global assessment scale (CGAS). Arch. Gen. Psychiatry 1983, 40, 1228–1231. [Google Scholar] [CrossRef]
- Conners, C.K. Conners’ Parent Rating Scale—Revised (S); Multi-Health Systems: North Tonawanda, NY, USA, 1997. [Google Scholar]
- Braun, P.R.; Han, S.; Hing, B.; Nagahama, Y.; Gaul, L.N.; Heinzman, J.T.; Grossbach, A.J.; Close, L.; Dlouhy, B.J.; Howard, M.A., 3rd; et al. Genome-wide DNA methylation comparison between live human brain and peripheral tissues within individuals. Transl. Psychiatry 2019, 9, 47. [Google Scholar] [CrossRef] [Green Version]
- Smith, A.K.; Kilaru, V.; Klengel, T.; Mercer, K.B.; Bradley, B.; Conneely, K.N.; Ressler, K.J.; Binder, E.B. DNA extracted from saliva for methylation studies of psychiatric traits: Evidence tissue specificity and relatedness to brain. Am. J. Med. Genet. Part B Neuropsychiatr. Genet. 2015, 168B, 36–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdolmaleky, H.M.; Pajouhanfar, S.; Faghankhani, M.; Joghataei, M.T.; Mostafavi, A.; Thiagalingam, S. Antipsychotic drugs attenuate aberrant DNA methylation of DTNBP1 (dysbindin) promoter in saliva and post-mortem brain of patients with schizophrenia and Psychotic bipolar disorder. Am. J. Med. Genet. Part B Neuropsychiatr. Genet. 2015, 168, 687–696. [Google Scholar] [CrossRef] [PubMed]
- Nohesara, S.; Ghadirivasfi, M.; Mostafavi, S.; Eskandari, M.R.; Ahmadkhaniha, H.; Thiagalingam, S.; Abdolmaleky, H.M. DNA hypomethylation of MB-COMT promoter in the DNA derived from saliva in schizophrenia and bipolar disorder. J. Psychiatr. Res. 2011, 45, 1432–1438. [Google Scholar] [CrossRef] [PubMed]
- Issa, A.M. Personalized medicine and the practice of medicine in the 21st century. McGill J. Med. MJM 2007, 10, 53–57. [Google Scholar] [CrossRef]
- Erskine, H.E.; Norman, R.E.; Ferrari, A.J.; Chan, G.C.; Copeland, W.E.; Whiteford, H.A.; Scott, J.G. Long-Term Outcomes of Attention-Deficit/Hyperactivity Disorder and Conduct Disorder: A Systematic Review and Meta-Analysis. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 841–850. [Google Scholar] [CrossRef]
- Swanson, J.M.; Arnold, L.E.; Molina, B.; Sibley, M.H.; Hechtman, L.T.; Hinshaw, S.P.; Abikoff, H.B.; Stehli, A.; Owens, E.B.; Mitchell, J.T.; et al. Young adult outcomes in the follow-up of the multimodal treatment study of attention-deficit/hyperactivity disorder: Symptom persistence, source discrepancy, and height suppression. J. Child Psychol. Psychiatry Allied Discip. 2017, 58, 663–678. [Google Scholar] [CrossRef]
- Luciano, M.; Sampogna, G.; Mancuso, E.; Simonetti, A.; De Fazio, P.; Di Nicola, M.; Di Lorenzo, G.; Pepe, M.; Sambataro, F.; Signorelli, M.S.; et al. Trait-Related Impulsivity, Affective Temperaments and Mood Disorders: Results from a Real-World Multicentric Study. Brain Sci. 2022, 12, 1554. [Google Scholar] [CrossRef]
- Jahan, A.B.; Tanev, K. Neurobiological Mechanisms of Depression Following Traumatic Brain Injury. Brain Inj. 2022, advance online publication. [Google Scholar] [CrossRef]
- Shen, J.; Wang, J.; Hao, Q.; Ji, W.; Peng, H.; Wu, Y.; Zhao, R.; Qiu, X.; Wang, W.; Yang, J.; et al. Transformable Nanotheranostics Capable of Sensoring Nucleic Acid Drugs’ Spatiotemporal Behaviors. Adv. Funct. Mater. 2022, 33, 2209749. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (a) Severe Subjects | |
|---|---|
| M3 M1M5 | 0.97 |
| M5 M1M3 | 0.91 |
| M3 D2M5 | 0.95 |
| M5 D2M3 | 0.97 |
| M3 D6M5 | 0.97 |
| M5 D6M3 | 0.97 |
| M1 D2M5 | 0.86 |
| M5 D2M1 | 0.83 |
| M1 D2M3 | 0.93 |
| M3 D2M1 | 0.88 |
| M1 D6M3 | 0.92 |
| M3 D6M5 | 0.9 |
| p < 0.05 | |
| (b) Improving Subjects | |
| M3 M5D1 | 0.82 |
| M3 M5M2 | 0.85 |
| M3 M5M6 | 0.87 |
| M3 M2M6 | 0.85 |
| p < 0.05 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carpentieri, V.; Lambacher, G.; Troianiello, M.; Pucci, M.; Di Pietro, D.; Laviola, G.; D’Addario, C.; Pascale, E.; Adriani, W. Methylation Dynamics on 5′-UTR of DAT1 Gene as a Bio-Marker to Recognize Therapy Success in ADHD Children. Children 2023, 10, 584. https://doi.org/10.3390/children10030584
Carpentieri V, Lambacher G, Troianiello M, Pucci M, Di Pietro D, Laviola G, D’Addario C, Pascale E, Adriani W. Methylation Dynamics on 5′-UTR of DAT1 Gene as a Bio-Marker to Recognize Therapy Success in ADHD Children. Children. 2023; 10(3):584. https://doi.org/10.3390/children10030584
Chicago/Turabian StyleCarpentieri, Valentina, Gabriella Lambacher, Miriam Troianiello, Mariangela Pucci, Diana Di Pietro, Giovanni Laviola, Claudio D’Addario, Esterina Pascale, and Walter Adriani. 2023. "Methylation Dynamics on 5′-UTR of DAT1 Gene as a Bio-Marker to Recognize Therapy Success in ADHD Children" Children 10, no. 3: 584. https://doi.org/10.3390/children10030584