
Validation and Determination of Physical Activity Intensity GT3X+ Cut-Points in Children and Adolescents with Physical Disabilities: Preliminary Results in a Cerebral Palsy Population
 , , ,
, , ,  , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Participants
2.3. Study Procedure
2.4. Outcomes Measures
2.4.1. Accelerometer
2.4.2. Portable Indirect Calorimeter
2.5. Data Reduction
2.6. Data Analysis
2.6.1. Study Objective (i): To Analyze the Accuracy of Evenson Cut-Points Estimating MVPA and SB in Children and Adolescents with Heterogeneous Disabilities Who Can Walk with or without Devices
2.6.2. Study Objective (ii): To Define New Equations to Estimate EE with the GT3X+ in Children and Adolescents with Heterogeneous Disabilities or CP Who Can Walk with or without Devices
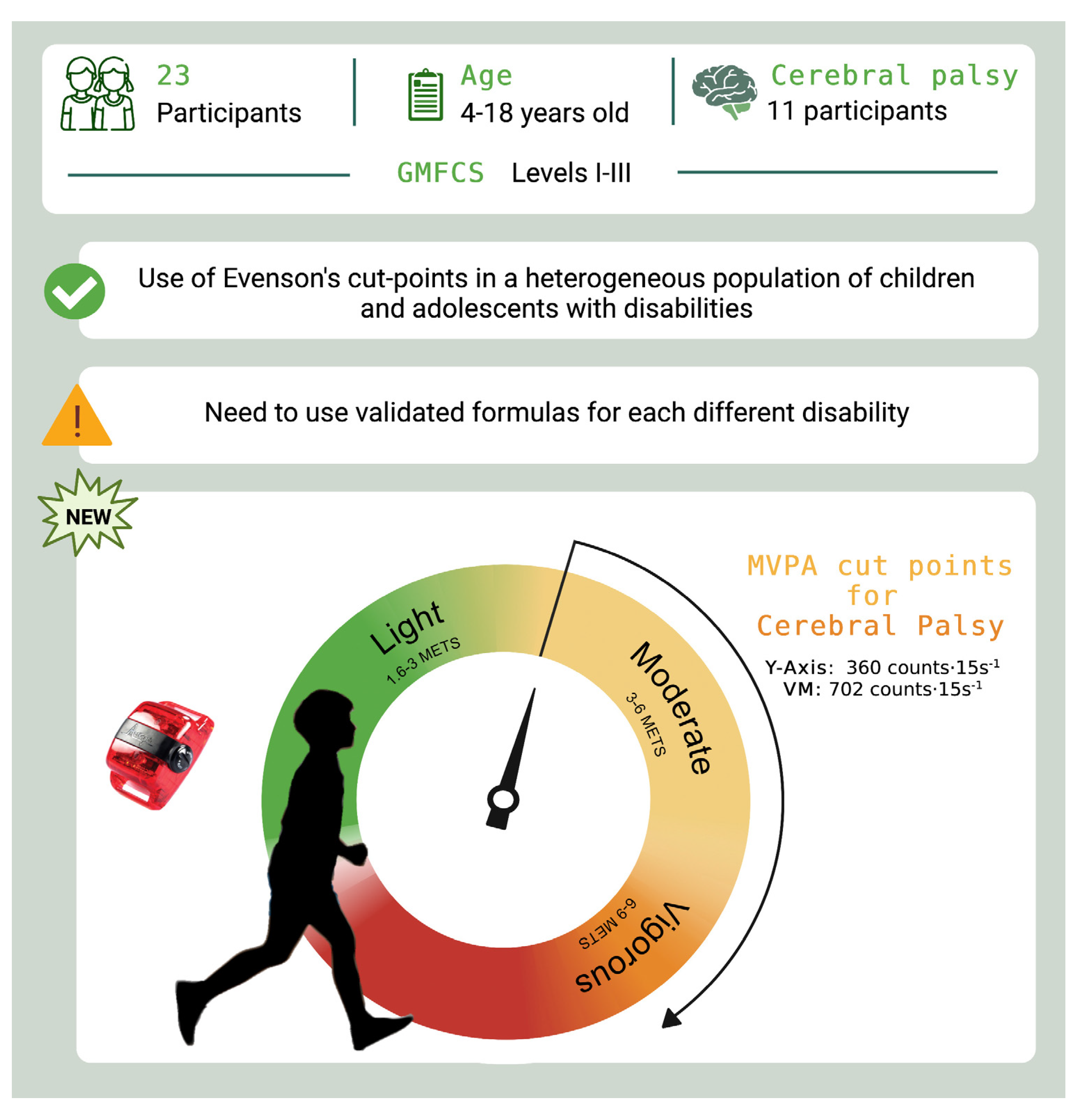
2.6.3. Study Objective (iii): To Define GT3X+ Cut-Points to Estimate MVPA in Children and Adolescents with CP
3. Results
3.1. Study Participants
3.2. Study Objective (i): To Analyze the Accuracy of Evenson Cut-Points Estimating MVPA and SB in Children and Adolescents with Heterogeneous Disabilities Who Can Walk with or without Devices
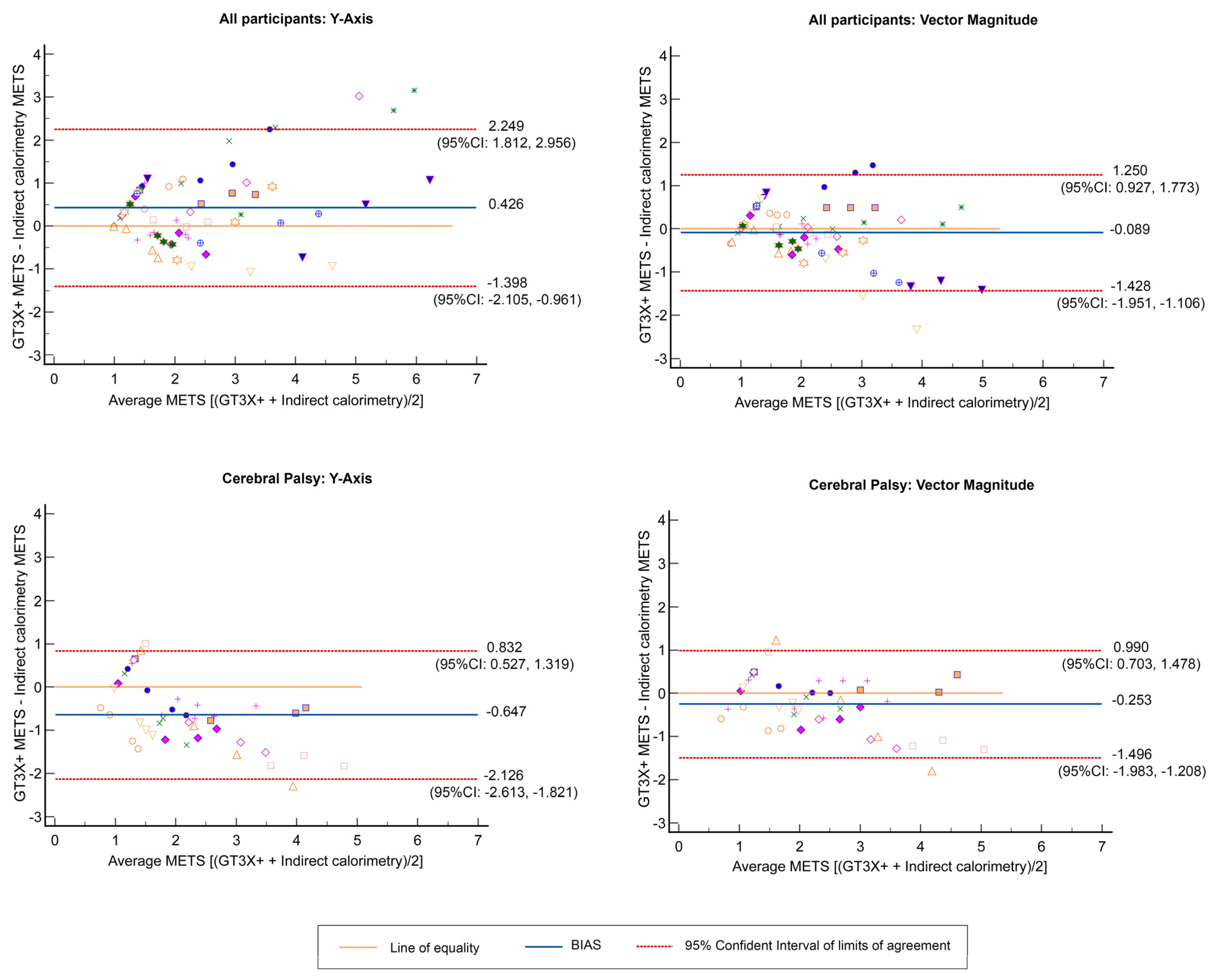
3.3. Study Objective (ii): To Define New Equations to Estimate EE with the GT3X+ in Children and Adolescents with Heterogeneous Disabilities or CP Who Can Walk with or without Devices
3.4. Study Objective (iii): To Define GT3X+ Cut-Points to Estimate MVPA in Children and Adolescents with CP
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chaput, J.P.; Willumsen, J.; Bull, F.; Chou, R.; Ekelund, U.; Firth, J.; Jago, R.; Ortega, F.B.; Katzmarzyk, P.T. 2020 WHO guidelines on physical activity and sedentary behaviour for children and adolescents aged 5–17 years: Summary of the evidence. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 141. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Physical Activity. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 17 June 2022).
- Jung, J.; Leung, W.; Schram, B.M.; Yun, J. Meta-Analysis of Physical Activity Levels in Youth With and Without Disabilities. Adapt. Phys. Activ. Q. 2018, 35, 381–402. [Google Scholar] [CrossRef] [PubMed]
- Durstine, J.L.; Gordon, B.; Wang, Z.; Luo, X. Chronic disease and the link to physical activity. J. Sport Health Sci. 2013, 2, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Torpy, J.M.; Campbell, A.; Glass, R.M. JAMA patient page. Chronic diseases of children. JAMA 2010, 303, 682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evenson, K.R.; Catellier, D.J.; Gill, K.; Ondrak, K.S.; McMurray, R.G. Calibration of two objective measures of physical activity for children. J. Sports Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef]
- Romanzini, M.; Petroski, E.L.; Ohara, D.; Dourado, A.C.; Reichert, F.F. Calibration of ActiGraph GT3X, Actical and RT3 accelerometers in adolescents. Eur. J. Sport Sci. 2014, 14, 91–99. [Google Scholar] [CrossRef]
- Trost, S.G. State of the Art Reviews: Measurement of Physical Activity in Children and Adolescents. Am. J. Lifestyle Med. 2007, 1, 299–314. [Google Scholar] [CrossRef]
- Lyden, K.; Kozey, S.L.; Staudenmeyer, J.W.; Freedson, P.S. A comprehensive evaluation of commonly used accelerometer energy expenditure and MET prediction equations. Eur. J. Appl. Physiol. 2011, 111, 187–201. [Google Scholar] [CrossRef]
- Wijndaele, K.; Westgate, K.; Stephens, S.K.; Blair, S.N.; Bull, F.C.; Chastin, S.F.; Dunstan, D.W.; Ekelund, U.; Esliger, D.W.; Freedson, P.S.; et al. Utilization and Harmonization of Adult Accelerometry Data: Review and Expert Consensus. Med. Sci. Sports Exerc. 2015, 47, 2129–2139. [Google Scholar] [CrossRef] [Green Version]
- Norton, K.; Norton, L.; Sadgrove, D. Position statement on physical activity and exercise intensity terminology. J. Sci. Med. Sport 2010, 13, 496–502. [Google Scholar] [CrossRef]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A.; et al. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1081–1093. [Google Scholar] [CrossRef] [Green Version]
- Santos-Lozano, A.; Santin-Medeiros, F.; Cardon, G.; Torres-Luque, G.; Bailon, R.; Bergmeir, C.; Ruiz, J.R.; Lucia, A.; Garatachea, N. Actigraph GT3X: Validation and determination of physical activity intensity cut points. Int. J. Sports Med. 2013, 34, 975–982. [Google Scholar] [CrossRef]
- Wright, A.; Roberts, R.; Bowman, G.; Crettenden, A. Barriers and facilitators to physical activity participation for children with physical disability: Comparing and contrasting the views of children, young people, and their clinicians. Disabil. Rehabil. 2019, 41, 1499–1507. [Google Scholar] [CrossRef]
- Arvidsson, D.; Fridolfsson, J.; Borjesson, M. Measurement of physical activity in clinical practice using accelerometers. J. Intern. Med. 2019, 286, 137–153. [Google Scholar] [CrossRef] [Green Version]
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Delisle Nystrom, C.; Mora-Gonzalez, J.; Lof, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer Data Collection and Processing Criteria to Assess Physical Activity and Other Outcomes: A Systematic Review and Practical Considerations. Sports Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef]
- Ried-Larsen, M.; Brond, J.C.; Brage, S.; Hansen, B.H.; Grydeland, M.; Andersen, L.B.; Moller, N.C. Mechanical and free living comparisons of four generations of the Actigraph activity monitor. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 113. [Google Scholar] [CrossRef] [Green Version]
- Novak, I.; Morgan, C.; Adde, L.; Blackman, J.; Boyd, R.N.; Brunstrom-Hernandez, J.; Cioni, G.; Damiano, D.; Darrah, J.; Eliasson, A.C.; et al. Early, Accurate Diagnosis and Early Intervention in Cerebral Palsy: Advances in Diagnosis and Treatment. JAMA Pediatr. 2017, 171, 897–907. [Google Scholar] [CrossRef]
- Xing, R.; Huang, W.Y.; Sit, C.H. Validity of accelerometry for predicting physical activity and sedentary time in ambulatory children and young adults with cerebral palsy. J. Exerc. Sci. Fit. 2021, 19, 19–24. [Google Scholar] [CrossRef]
- Palisano, R.; Rosenbaum, P.; Walter, S.; Russell, D.; Wood, E.; Galuppi, B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev. Med. Child Neurol. 1997, 39, 214–223. [Google Scholar] [CrossRef]
- Palisano, R.J.; Rosenbaum, P.; Bartlett, D.; Livingston, M.H. Content validity of the expanded and revised Gross Motor Function Classification System. Dev. Med. Child Neurol. 2008, 50, 744–750. [Google Scholar] [CrossRef]
- Goodlich, B.I.; Armstrong, E.L.; Horan, S.A.; Baque, E.; Carty, C.P.; Ahmadi, M.N.; Trost, S.G. Machine learning to quantify habitual physical activity in children with cerebral palsy. Dev. Med. Child Neurol. 2020, 62, 1054–1060. [Google Scholar] [CrossRef]
- Trost, S.G.; Fragala-Pinkham, M.; Lennon, N.; O’Neil, M.E. Decision Trees for Detection of Activity Intensity in Youth with Cerebral Palsy. Med. Sci. Sports Exerc. 2016, 48, 958–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clanchy, K.M.; Tweedy, S.M.; Boyd, R.N.; Trost, S.G. Validity of accelerometry in ambulatory children and adolescents with cerebral palsy. Eur. J. Appl. Physiol. 2011, 111, 2951–2959. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, M.E.; Fragala-Pinkham, M.A.; Forman, J.L.; Trost, S.G. Measuring reliability and validity of the ActiGraph GT3X accelerometer for children with cerebral palsy: A feasibility study. J. Pediatr. Rehabil. Med. 2014, 7, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Antonsson, E.K.; Mann, R.W. The frequency content of gait. J. Biomech. 1985, 18, 39–47. [Google Scholar] [CrossRef]
- ActiGraph. GT3X+ and wGT3X+ Device Manual; ActiGraph: Pensacola, FL, USA, 2018. [Google Scholar]
- Brond, J.C.; Arvidsson, D. Sampling frequency affects the processing of Actigraph raw acceleration data to activity counts. J. Appl. Physiol. (1985) 2016, 120, 362–369. [Google Scholar] [CrossRef] [Green Version]
- Cortex. Operator’s Manual MetaLyzer® 3B Version ML3B 2.1; Cortex: Leipzig, Germany, 2022. [Google Scholar]
- Lamarra, N.; Whipp, B.J.; Ward, S.A.; Wasserman, K. Effect of interbreath fluctuations on characterizing exercise gas exchange kinetics. J. Appl. Physiol. (1985) 1987, 62, 2003–2012. [Google Scholar] [CrossRef]
- Corry, I.S.; Duffy, C.M.; Cosgrave, A.P.; Graham, H.K. Measurement of oxygen consumption in disabled children by the Cosmed K2 portable telemetry system. Dev. Med. Child Neurol. 1996, 38, 585–593. [Google Scholar] [CrossRef]
- Hanggi, J.M.; Phillips, L.R.; Rowlands, A.V. Validation of the GT3X ActiGraph in children and comparison with the GT1M ActiGraph. J. Sci. Med. Sport 2013, 16, 40–44. [Google Scholar] [CrossRef]
- Zweig, M.H.; Campbell, G. Receiver-operating characteristic (ROC) plots: A fundamental evaluation tool in clinical medicine. Clin. Chem. 1993, 39, 561–577. [Google Scholar] [CrossRef]
- Trost, S.G.; Fees, B.S.; Haar, S.J.; Murray, A.D.; Crowe, L.K. Identification and validity of accelerometer cut-points for toddlers. Obesity (Silver Spring). 2012, 20, 2317–2319. [Google Scholar] [CrossRef]
- Treuth, M.S.; Schmitz, K.; Catellier, D.J.; McMurray, R.G.; Murray, D.M.; Almeida, M.J.; Going, S.; Norman, J.E.; Pate, R. Defining accelerometer thresholds for activity intensities in adolescent girls. Med. Sci. Sports Exerc. 2004, 36, 1259–1266. [Google Scholar]
- Myles, P.S.; Cui, J. Using the Bland-Altman method to measure agreement with repeated measures. Br. J. Anaesth. 2007, 99, 309–311. [Google Scholar] [CrossRef] [Green Version]
- Zou, G.Y. Confidence interval estimation for the Bland-Altman limits of agreement with multiple observations per individual. Stat. Methods Med. Res. 2013, 22, 630–642. [Google Scholar] [CrossRef]
- Atkinson, G.; Davison, R.C.; Nevill, A.M. Performance characteristics of gas analysis systems: What we know and what we need to know. Int. J. Sports Med. 2005, 26 (Suppl. 1), S2–S10. [Google Scholar] [CrossRef]
- Steene-Johannessen, J.; Hansen, B.H.; Dalene, K.E.; Kolle, E.; Northstone, K.; Moller, N.C.; Grontved, A.; Wedderkopp, N.; Kriemler, S.; Page, A.S.; et al. Variations in accelerometry measured physical activity and sedentary time across Europe—Harmonized analyses of 47,497 children and adolescents. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 38. [Google Scholar] [CrossRef] [Green Version]
- Stephens, S.; Takken, T.; Esliger, D.W.; Pullenayegum, E.; Beyene, J.; Tremblay, M.; Schneiderman, J.; Biggar, D.; Longmuir, P.; McCrindle, B.; et al. Validation of Accelerometer Prediction Equations in Children with Chronic Disease. Pediatr. Exerc. Sci. 2016, 28, 117–132. [Google Scholar] [CrossRef] [Green Version]
- Keawutan, P.; Bell, K.L.; Oftedal, S.; Davies, P.S.; Boyd, R.N. Validation of Accelerometer Cut-Points in Children With Cerebral Palsy Aged 4 to 5 Years. Pediatr. Phys. Ther. 2016, 28, 427–434. [Google Scholar] [CrossRef]
- Oftedal, S.; Bell, K.L.; Davies, P.S.; Ware, R.S.; Boyd, R.N. Validation of accelerometer cut points in toddlers with and without cerebral palsy. Med. Sci. Sports Exerc. 2014, 46, 1808–1815. [Google Scholar] [CrossRef] [Green Version]
- Trost, S.G.; O’Neil, M. Clinical use of objective measures of physical activity. Br. J. Sports Med. 2014, 48, 178–181. [Google Scholar] [CrossRef]
- Welk, G.J. Principles of design and analyses for the calibration of accelerometry-based activity monitors. Med. Sci. Sports Exerc. 2005, 37 (Suppl. 11), S501–S511. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Outcome | All (n = 23) | Cerebral Palsy (n = 11) |
|---|---|---|
| Age (yr), mean (SD) | 10 ± 3 (5–18) | 11 ± 4 (5–18) |
| Gender, n females (%) | 10 (44%) | 4 (36%) |
| Height (cm), mean (SD) | 129.2 ± 19.9 | 135.5 ± 17.9 |
| Weight (kg), mean (SD) | 33.2 ± 12.5 | 34.6 ± 12.3 |
| GMFCS, n (%) | ||
| Level I | 13 (57%) | 5 (46%) |
| Level II | 4 (17%) | 1 (9%) |
| Level II | 6 (26%) | 5 (46%) |
| Coginitive, n (%) | ||
| Average | 12 (57%) | 7 (33%) |
| Mild impairment | 7 (33%) | 2 (18%) |
| Moderate impairment | 4 (19%) | 2 (18%) |
| School type, n (%) | ||
| Main stream (included) | 19 (90%) | 9 (82%) |
| Main stream (self-contained) | 2 (10%) | 1 (9%) |
| Special school | 2 (10%) | 1 (9%) |
| Clinical diagnosis, n (%) | ||
| Cerebral palsy | 11 (48%) | 11 (100%) |
| Prader–Willi syndrome | 3 (13%) | - |
| Williams syndrome | 1 (4%) | - |
| Spina bifida | 1 (4%) | - |
| Diencephalic brain tumor | 1 (4%) | - |
| Autism spectrum disorder | 1 (4%) | - |
| Achondroplasia | 1 (4%) | - |
| Metabolic disease | 2 (9%) | - |
| Congenital malformation of upper limbs | 1 (4%) | - |
| Condition | Speed (km·h−1) | HR (bpm) | VO2 (L·min−1) | METs | Axis Y Counts·15s−1 | VM Counts·15s−1 | |
|---|---|---|---|---|---|---|---|
| All (n = 23) | Rest | − | 91 ± 12 | 0.26 ± 0.05 | 1.0 ± 0.0 | 2 ± 5 | 12 ± 13 |
| Comfortable paced walking | 1.8 ± 0.6 | 121 ± 3 | 0.51 ± 0.19 | 2.0 ± 0.7 | 160 ± 130 | 500 ± 233 | |
| Brisk paced walking | 2.7 ± 0.8 | 128 ± 4 | 0.60 ± 0.26 | 2.4 ± 0.9 | 381 ± 304 | 754 ± 350 | |
| Fast paced walking | 3.4 ± 1.0 | 134 ± 4 | 0.71 ± 0.31 | 2.8 ± 1.0 | 578 ± 414 | 989 ± 451 | |
| Cerebral palsy (n = 11) | Rest | − | 90 ± 14 | 0.24 ± 0.05 | 1.0 ± 0.0 | 2 ± 3 | 11 ± 10 |
| Comfortable paced walking | 1.7 ± 06 | 127 ± 17 | 0.58 ± 0.23 | 2.4 ± 0.9 | 150 ± 148 | 477 ± 297 | |
| Brisk paced walking | 2.7 ± 0.8 | 138 ± 19 | 0.74 ± 0.24 | 3.0 ± 1.0 | 440 ± 390 | 804 ± 450 | |
| Fast paced walking | 3.2 ± 0.9 | 146 ± 18 | 0.86 ± 0.3 | 3.5 ± 1.2 | 647 ± 507 | 1087 ± 544 |
| Group | Variable | Sensitivity (%) | Specificity (%) | AUC | Correctly Classified (%) | SE |
|---|---|---|---|---|---|---|
| Sedentary (<25 counts·15 s−1) | Y | 75 | 90 | 0.825 | 85 | 0.0435 |
| VM | 59 | 100 | 0.797 | 86 | 0.0441 | |
| Moderate-to-vigorous (≥574 counts·15 s−1) | Y | 67 | 91 | 0.790 | 88 | 0.0728 |
| VM | 92 | 59 | 0.758 | 63 | 0.0500 |
| Group | Axis | Equation | RMSE | p-Value |
|---|---|---|---|---|
| All participants (n = 23; 10 girls) | Y | METS = 0.383 + 0.001 · Y-Axis AC + 0.020 · BM + 0.263 · GMFCS | 0.62 | <0.001 |
| VM | METS = 0.014 + 0.0004 · VM AC + 0.026 · BM + 0.206 · GMFCS | 0.60 | <0.001 | |
| Cerebral palsy (n = 11, 4 girls) | Y | METS = −0.309 + 0.0004 · Y-Axis AC + 0.034· BM + 0.245 · GMFCS | 0.61 | <0.001 |
| VM | METS = 2.535 + 0.0004 · VM AC + 0.144 · A − 0.033 · H + 0.037 · BM + 0.190 · GMFCS | 0.57 | <0.001 |
| Variable | Cerebral Palsy (n = 11) | |||||
|---|---|---|---|---|---|---|
| Cut-Point (Counts·15 s−1) | Sensitivity (%) | Specificity (%) | AUC (Mean ± Standard Error) | p-Value | ||
| 3 METS (MVPA) | Axis Y | 360 | 92 | 84 | 0.907 ± 0.036 | <0.001 |
| VM | 702 | 93 | 83 | 0.900 ± 0.056 | <0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matey-Rodríguez, C.; López-Ortiz, S.; Peñín-Grandes, S.; Pinto-Fraga, J.; Valenzuela, P.L.; Pico, M.; Fiuza-Luces, C.; Lista, S.; Lucia, A.; Santos-Lozano, A. Validation and Determination of Physical Activity Intensity GT3X+ Cut-Points in Children and Adolescents with Physical Disabilities: Preliminary Results in a Cerebral Palsy Population. Children 2023, 10, 475. https://doi.org/10.3390/children10030475
Matey-Rodríguez C, López-Ortiz S, Peñín-Grandes S, Pinto-Fraga J, Valenzuela PL, Pico M, Fiuza-Luces C, Lista S, Lucia A, Santos-Lozano A. Validation and Determination of Physical Activity Intensity GT3X+ Cut-Points in Children and Adolescents with Physical Disabilities: Preliminary Results in a Cerebral Palsy Population. Children. 2023; 10(3):475. https://doi.org/10.3390/children10030475
Chicago/Turabian StyleMatey-Rodríguez, Carmen, Susana López-Ortiz, Saúl Peñín-Grandes, José Pinto-Fraga, Pedro L. Valenzuela, Mónica Pico, Carmen Fiuza-Luces, Simone Lista, Alejandro Lucia, and Alejandro Santos-Lozano. 2023. "Validation and Determination of Physical Activity Intensity GT3X+ Cut-Points in Children and Adolescents with Physical Disabilities: Preliminary Results in a Cerebral Palsy Population" Children 10, no. 3: 475. https://doi.org/10.3390/children10030475