1. Introduction
Down syndrome (DS) is a genetic condition caused by the tripling of chromosome 21 (T21) and is characterized by a wide range of physical and neurodevelopmental disabilities [
1]. Researchers are interested in DS since it is the most frequent genetic mutation [
2].
DS children are more likely to develop multiorgan comorbidities [
3]. Congenital cardiac disease is frequent in DS children, with ventricular septal defects being the most prevalent type [
4]. A common cardiac deformity in DS patients, atrioventricular septal defect (AVSD), accounts for up to 5% of all congenital heart problems [
5]. Total AVSD, the most common form in the DS group, has a worse prognosis than partial AVSD [
5]. Infant mortality before surgery is high despite the postoperative mortality being low [
5]. For the treatment of managing and lowering morbidity and mortality in DS children, early diagnosis of congenital heart disease and other comorbidities is advised [
3,
4]. DS children also have a higher probability of epilepsy, autoimmune diseases, celiac disease, arthropathy, thyroid dysfunction, diabetes mellitus, dermatological changes, auditory and visual abnormalities, and autistic spectrum disorder [
3].
All patients with cardiovascular diseases are recommended to engage in controlled physical activity and exercise, which are regarded as the gold standard of cardiac rehabilitation [
6] and offers a direct impact on morbidity and mortality, as well as in improving quality of life [
7]. Exercises such as whole-body vibration exercise (WBVE), a type of moderate-intensity physical activity, can improve health [
8,
9]. Among the main effects of the WBVE are increased peripheral blood circulation [
10,
11] and lymph [
12], decrease of pain [
13,
14], spasticity [
15], positive effects on the neuromuscular system [
16], and improvements of cognitive functions. [
17].
WBVE can be a helpful alternative for monotonous activities performed during cardiac rehabilitation [
18]. WBVE occurs when the individual is exposed to mechanical vibrations generated in a vibrating platform at a specific frequency and amplitude, adapted to each individual and their clinical condition [
19] during the systemic vibratory therapy [
20,
21]. WBVE compared to no training [
22,
23,
24] or as an adjunct to exercise, [
25,
26] has shown positive short-term effects on static balance within children and adolescents with DS, [
22] on lower limb muscle strength in DS children [
25,
26], and subtotal bone mineral density and subtotal bone mineral content in DS adolescents [
24]. There have been no short-term effects due to the WBVE that been represented in the body fat of DS children [
26] or the body fat and lean body mass in DS adolescents [
23].
Eid et al. [
25] investigated if the WBVE could improve standing balance and muscle strength in 30 DS children (8–10 years old). The control group received a designed physical therapy program, whereas the study group received the same program given to the control group, in addition to WBVE. Both groups received the treatment sessions three times per week for six successive months. Significant improvements in stability indices and muscle strength after treatment were demonstrated in each group, with significantly greater improvements seen in the study group when compared with the control group (
p < 0.05), suggesting that WBVE may be a useful intervention modality to improve balance and muscle strength in DS children.
Considering an increased prevalence of obesity and muscle weakness in DS children, Emara et al. [
26] examined the effects of a 12-week WBVE on the body composition and muscle strength of 31 DS children (10–12 years old) divided randomly into 2 groups, regarding the higher prevalence of obesity and muscle weakness in DS children. The trial group received WBVE in addition to the physical therapy program that was offered to the control group. For three months in a row, there were three treatment sessions every week. The results revealed that there was a significant increase in lower limb strength in both groups (pre and post treatment). Comparison concerning post treatment results revealed more increase in the lower limb strength in the WBVE group, suggesting that this modality may improve lower extremities muscular strength in obese DS children.
Finally, a study proposed by Eid et al. [
27] investigated the effects of isokinetic training on muscle strength and postural balance in 31 DS children (9 to 12 years old), divided randomly into 2 groups. The study group had isokinetic training 3 days per week for a period of 12 weeks, in addition to the same physical treatment as the control group underwent. Both groups had significant improvements in postural balance and the peak torque of their knee flexors and extensors (
p < 0.05), with the study group experiencing significantly greater improvements than the control group (
p < 0.05). These outcomes indicated that participation in the isokinetic training program induced greater improvements in muscle strength and postural balance in DS children. Therefore, the WBVE can be suggested for this population as an effective training modality.
3. Results
For the analysis of quantitative data, the mean and standard deviation of the collected data were used, and for the analysis of qualitative data, a comparison was made between the collected data.
3.1. Clinical Parameters
Data collected before WBVE 1 were to BP, 104 × 63, 108 × 71, 114 × 68 mmHg; to HR, 79, 93, 74 bpm; RR 15, 15, 14 ipm; and to SatO
2, 99%. After the WBVE 1 were to BP, 114 × 60, 101 × 62, 122 × 54 mmHg; to HR, 80, 77, 71 bpm; RR 16, 14, 15 ipm; and to SatO
2, 99%. The mean and standard deviation of these findings are shown in
Table 1.
Before the WBVE 2, the BP was 110 × 64, 109 × 51, 111 × 56 mmHg; HR 74, 78, 74 bpm; RR was 15, 15, 14 ipm; and SatO
2 was 99%. After the WBVE 2, the BP was 107 × 57, 134 × 86, 114 × 56 mmHg; HR 73, 51, 77 bpm; the RR 15, 15, 15 ipm; and SatO
2 was 99%. The mean and standard deviation of these findings are shown in
Table 2.
When comparing the data, it is possible to qualitatively confirm that systolic pressure increased post WBVE 1 compared to pre WBVE 1, and that systolic and diastolic pressure increased post WBVE 2 compared to pre WBVE 2. This shows that, as would be expected after performing physical exercise, WBVE had a clinical impact on cardiovascular function. However, the changed parameters did not approach alarming levels.
There was a reduction in HR post WBVE 1 compared to pre WBVE 1, as well as in the HR post WBVE 2 compared to pre WBVE 2. The RR remained the same in pre WBVE 1 and post WBVE 1, as well as in pre WBVE 2 and post WBVE 2 and Sat02 remained the same in all collections.
3.2. Infrared Thermography
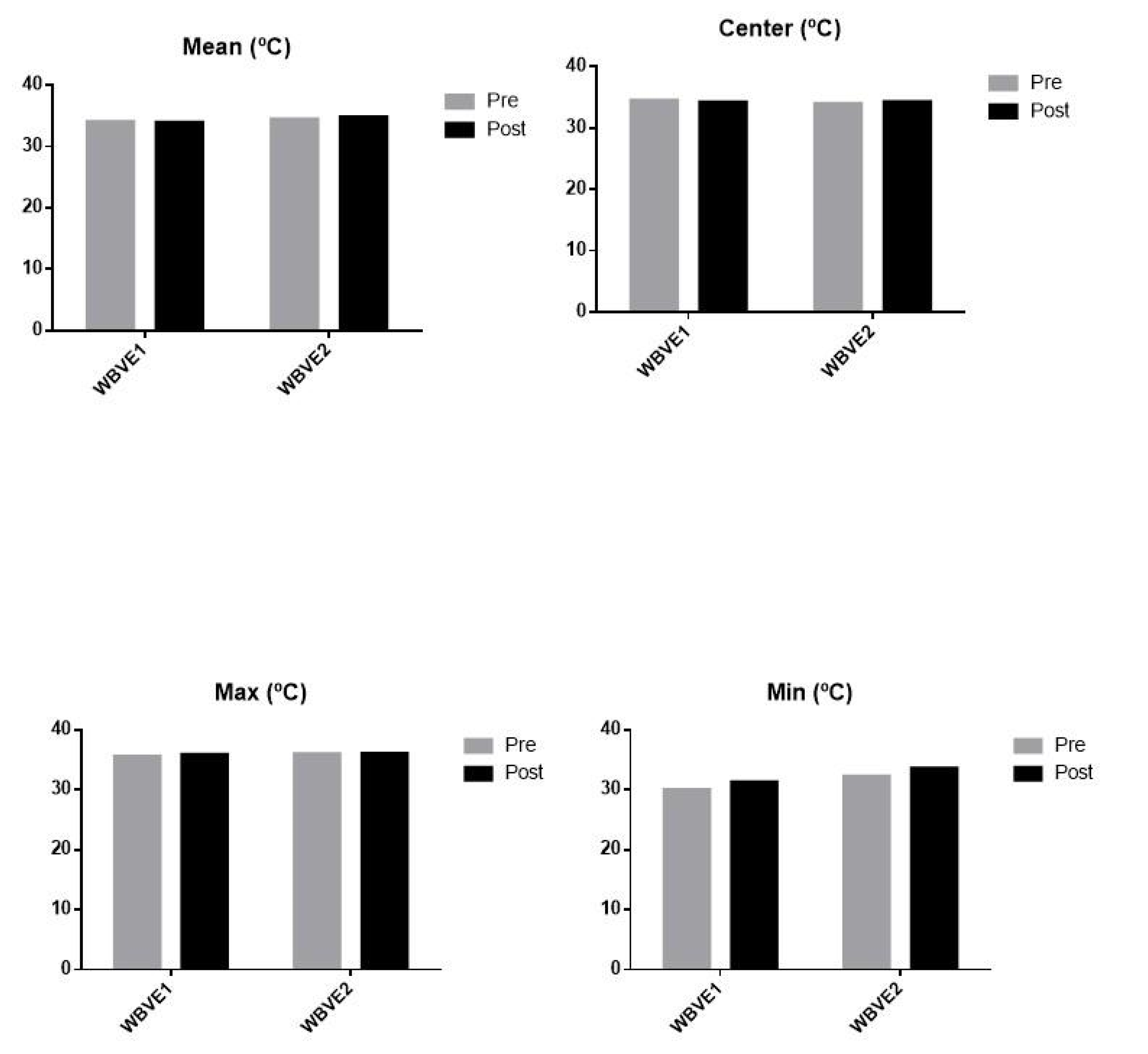
Before the first IT analysis, the anterior region of the neck showed a mean temperature of 34 °C, with a center temperature of 34.5 °C, a maximum temperature of 35.6 °C, and a minimum temperature of 30 °C. After WBVE 1, the IT analysis of the anterior region of the neck showed a mean temperature of 33.9 °C, a center temperature of 34.2 °C, a maximum temperature of 35.9 °C, and a minimum temperature of 31.3 °C. Before the WBVE 2, the IT analysis showed a mean temperature of 34.4 °C, a center temperature of 34.0 °C, a maximum temperature of 36.0 °C, and a minimum temperature of 32.3 °C. After WBVE 2, the IT analysis of the anterior region of the neck showed a mean temperature of 34.8 °C, a center temperature of 34.3 °C, a maximum temperature of 36.1 °C, and a minimum temperature of 33.6 °C.
Figure 1 shows the data obtained with IF.
It is possible to verify that the maximum and minimum temperatures, as well as the mean temperature, were slightly increased post WBVE 1 compared to pre WBVE 1. Pre and post the WBVE 2, the center temperature remained stable.
3.3. Tone
Before WBVE 1, palpation of the muscles showed bilateral hypotonia of the deltoid, bilateral biceps brachii (BB), bilateral triceps brachii (TB), bilateral abdominals, bilateral hamstrings, and left triceps surae (TS); as well as normal tone of the bilateral pectorals, bilateral abdominal obliques (BO), bilateral quadriceps, and right TS. In passive joint movements, the girl presented hypotonia of bilateral shoulder flexors (SF) and shoulder extensors (SE), bilateral wrist extensors (WE), bilateral hip flexors (HF), bilateral hip adductors (HA), bilateral knee flexors (KF), bilateral ankle dorsiflexors (AD), and bilateral ankle plantar flexors (AP); as well as normal tone of bilateral elbow flexors (EF), bilateral elbow extensors (EE), and wrist flexors (WF).
After WBVE 1, the palpation of the muscles showed hypotonia in the bilateral deltoid muscles, bilateral BB, bilateral TB, and left TS; as well as normal tone of the other groups. In the joints, he presented hypotonia in the bilateral SF, bilateral SE, bilateral WE, bilateral HA, bilateral KF, bilateral AD, and bilateral AP; as well as normal tone of bilateral EF, bilateral EE, bilateral WF, and bilateral HF.
After WBVE 2, muscle tone was hypotonic in the bilateral deltoid, bilateral BB, bilateral TB, bilateral pectoral, bilateral TS, and bilateral hamstrings; as well as normal tone in the abdominals, bilateral obliques, and bilateral quadriceps. Joint tone was hypotonic in the bilateral SF, bilateral SE, bilateral EF, bilateral WE, bilateral HF, bilateral HA, bilateral KF, left AD, and left AP; as well as normal in the bilateral EE, bilateral WF, right AD, and right AP.
Table 3 shows the tonus data collected in muscle palpation and
Table 4 shows the tonus data collected through passive joint movement.
After WBVE 1 and WBVE 2, it is possible to verify that there were slight alterations in the muscle tone. The changes in tone observed on the palpation of the muscle belly included: bilateral pectoral and abdominal from normal to hypotonic after the second intervention; bilateral hamstring from hypotonic to normal after WBVE 1; and right triceps surae from normal to hypotonic after WBVE 2. As for the tone verified through passive joint movement, it is possible to verify the changes: flexion of the left elbow from normal to hypotonic after WBVE 2; bilateral elbow extension from normal to hypotonic after WBVE 2; bilateral hip flexion from hypotonic to normal after the first intervention; and change in dorsiflexion and plantarflexion of the right ankle from hypotonic to normal after WBVE 2.
3.4. WBVE Results in Body Composition
Before WBVE 1, the body composition (BC) was 118.5 cm of height, 26 kg of body mass, 18.1 kg of lean mass, 19.1 kg of fat-free mass, 1.02 kg of bone mass, 14.2 kg of water total body, 3.7 kg of protein (normal), 1.23 kg of minerals (normal), 6.9 kg of body fat (excessive), 9.2 kg of muscle mass, body mass index of 18.5 kg/m2 (normal), body fat percentage of 26.5% (much higher), and a waist-to-hip ratio 0.76 (normal). After WBVE 2, the BC showed 119 cm of height, 25 kg of body mass, 18.4 kg of lean mass, 19.4 kg of fat-free mass, 1.03 kg of bone mass, 14.4 kg of body water total, 3.8 kg of protein (normal), 1.23 kg of minerals (normal), 5.6 kg of body fat (normal), 9.4 kg of muscle mass, body mass index of 17.6 kg /m2 (normal), body fat percentage of 22.2% (above), and a waist-to-hip ratio 0.76 (normal) (
Table 5).
Height, lean mass, fat-free mass, bone mass, total body water, proteins, and muscle mass all increased after WBVE, according to data collected pre WBVE 1 and post WBVE 2. Post WBVE 2, body weight, body fat, body mass index, and fat percentage all decreased. Minerals and the waist-hip ratio remained stable.
3.5. WBVE Results in Sleep Disorder
3.5.1. QRL
Post the WBVE 2 session, a new round of QRL responses was collected. Only five questions changed, suggesting that the sleep pattern had improved. After two sessions of WBVE, the child under investigation stopped urinating during naps, woke up in the morning in less than 15 min, did not arrive late to school from oversleeping despite family members waking up, did not have any trouble staying awake at school in the mornings, and had no need or desire to sleep longer.
3.5.2. DSDC
In the DSDC performed before WBVE 1, the total score (TS) was 45; sleep initiation and maintenance disorder (SIMD) 15; sleep breathing disorders (SBD) 5; arousal disorders (AD) 6; sleep-wake transition disorders (SWTD) 6; excessive daytime sleepiness (EDS) 11; sleep hyperhidrosis (SH) 2. In the DSDC performed after WBVE 2, the TS was 43; SIMD 14; SBD 5; AD 3; SWTD 10; EDS 9; SH 2. These findings are also in
Table 6.
Comparing the results before WBVE 1 and after WBVE 2, it is possible to verify that, qualitatively, there was a decrease in TS, SIMD, AD, and EDS as well as an increase in SWTD after WBVE 2. The SBD and SH did not change.
4. Discussion
The current case report shows that the WBVE can be used in DS children who have undergone surgery to correct a total AVSD. In the current case report, even for the child performing only two interventions, the WBVE provided benefits and positive outcomes of quick and easy execution.
WBVE is a potential intervention for improving motor function and bone growth in children with disabilities, although most of the evidence comes from adult trials. It is crucial to understand the mechanisms of both disabled and non-disabled children. WBVE appears to be a safe intervention and the protocol should be appropriate for both disabled and non-disabled children, considering the biomechanical parameters of each patient [
39]. The outcomes of the current study support the findings of Saquetto et al. [
40], that in a systematic review it is suggested that WBVE has positive effects on body composition, bone mineral density, and balance in DS children and DS adolescents. Additionally, Gusso et al. [
41] performed vibratory training in 14 DS adolescents. On the base of the platform, the teenagers stood with their feet apart and their knees slightly bent. Each participant began their training with three series of 1-min sessions at a frequency of 12 Hz. The duration and intensity were gradually lengthened. For 20 weeks, there were 4 sessions every week. After the fourth week, all participants completed 3 sets of 3 min each at 20 Hz, 1 mm of amplitude, and 3 min of rest in between each set. A greater distance was traveled throughout the six minute walk test as a result, and muscle strength also increased.
Partial AVSD is more common in non-chromosomal cases, while total AVSD is more common in DS people [
42]. The AVSD is the most prevalent type of congenital heart malformation lesion [
43]. All patients with cardiovascular disorders should engage in appropriate and controlled physical activity and exercise, which is considered the gold standard of cardiac rehabilitation [
6] and has a considerable impact on quality of life, morbidity, and mortality [
17].
Thermoregulatory mechanisms are responsible for maintaining the optimal temperature of the body. Exercise speeds up oxygen transport and blood circulation, which raises metabolism and, ultimately, body temperature [
44]. Dębiec-Bąk et al. [
28], examined 36 people of both sexes, 18 DS individuals and 18 individuals without DS. All performed 45 min of identical training, with the necessary adaptations, twice a week for a period of 30 days. Before exercise, the temperature in all body regions was lower in DS individuals. After 5 min of training, the temperature decreased in all parts of the body in both groups, with the greatest decrease in the DS group. However, 15 min after training, the group without DS had body temperatures similar to the initial measurement, while the DS group temperatures did not return to baseline values. The findings presented in
Figure 1 agree with the results reported by Dębiec-Bąk et al. [
28].
Hypotonia is the primary cause of balance and postural control disorders in DS children and adolescents [
45]. Skeletal disorders such as hip and patellar dislocation, as well as flat feet, are also common [
46]. Hernandez-Reif et al. [
47], conducted a study in DS children to evaluate the effect of massage therapy on motricity and muscle tone. When compared to the control group, the massage therapy group showed greater gains in fine and gross motor function, as well as alterations in hypotonicity. The findings suggest that including massage therapy in an early intervention program can improve motor functioning and modulate muscle tone in DS children. Song et al. [
48] evaluated the effects of WBVE on trunk and lower limb muscle tone and activation, balance, and gait in a child with spastic diplegia cerebral palsy. WBVE decreased muscular tone in the hip extensor and plantar flexor of the right ankle; increased muscle activation in the bilateral erector spinae, rectus abdominis, rectus femoris, tibialis anterior, and gastrocnemius; and improved gait speed and balance. As a result, the authors concluded that WBVE can be used to safely and effectively maintain and increase physical performance and can be included in rehabilitation programs. Small changes in muscular tone were seen in this case study. However, considering the evidence assessed, it was agreed that the modulation of the aspect of hypotonia in DS could not be determined in only two WBVE sessions.
Weight gain and growth are measures of overall health in DS people. Obesity affects 25% of DS children and 50% of DS adults, exacerbating a range of issues such as obstructive sleep apnea, diabetes, and cardiopulmonary conditions. Obesity diagnosis and early intervention to encourage healthy diet and exercise routines are essential for managing weight gains [
46]. González-Agüero et al. [
23], investigated how the 20-week WBVE affected the body composition of DS young people. Thirty DS adolescents were allocated into the control and WBVE groups. The WBVE group showed a greater reduction in body fat in the upper limbs and a tendency to increase the percentage of total lean body mass, which may be useful to improve body composition in this population. The increase in height, lean mass, fat-free mass and bone mass, proteins, total body water and muscle mass was observed in this case study. The decrease in body mass was also identified. This is consistent with research findings that suggest a positive effect of systemic vibratory therapy on the BC of DS children.
Sleep difficulties are another prevalent issue among DS children. Choi et al. [
49] conducted a study in which 88 caregivers of Korean DS children aged 5 to 17 years old completed the Children’s Sleep Habits Questionnaire (CSHQ) to analyze the sleep characteristics of these children. The result showed that 83% of children with DS had sleep disorders. In this case study, an improvement in sleep initiation and maintenance, sleep agitation, and excessive sleep during the day was observed after the proposed protocol. There is presently no data in the literature describing WBVE protocols developed for DS children and analyzing sleep disorders.
The limitations of the present study are related to the quantity of interventions and any potential bias in the method used to measure muscle tone. Additionally, if other biomechanical factors and various WBVE protocols had been considered, the outcomes might have been different.
Another limitation of this case report that should be highlighted is the assessment of cognitive function. Although there is an understanding of the importance of identifying the cognitive potential of DS children, this ability was not considered as a criterion for participation in this protocol, because this evaluation and consideration of its consequences in the development of DS children requires qualified professionals.
The strength of this case study is that this is the first one to consider the effect of WBVE on a DS child who underwent total AVSD correction regarding CP, BT, muscle tone, BC, and sleep quality. This case report helps to fill part of the gap in the research field related to the effects of WBVE on CP, BT, tone, BC and sleep quality in DS children.

 ,
, 





{kind=link}