
Pediatric Glaucoma—From Screening, Early Detection to Management

Abstract
:1. Introduction
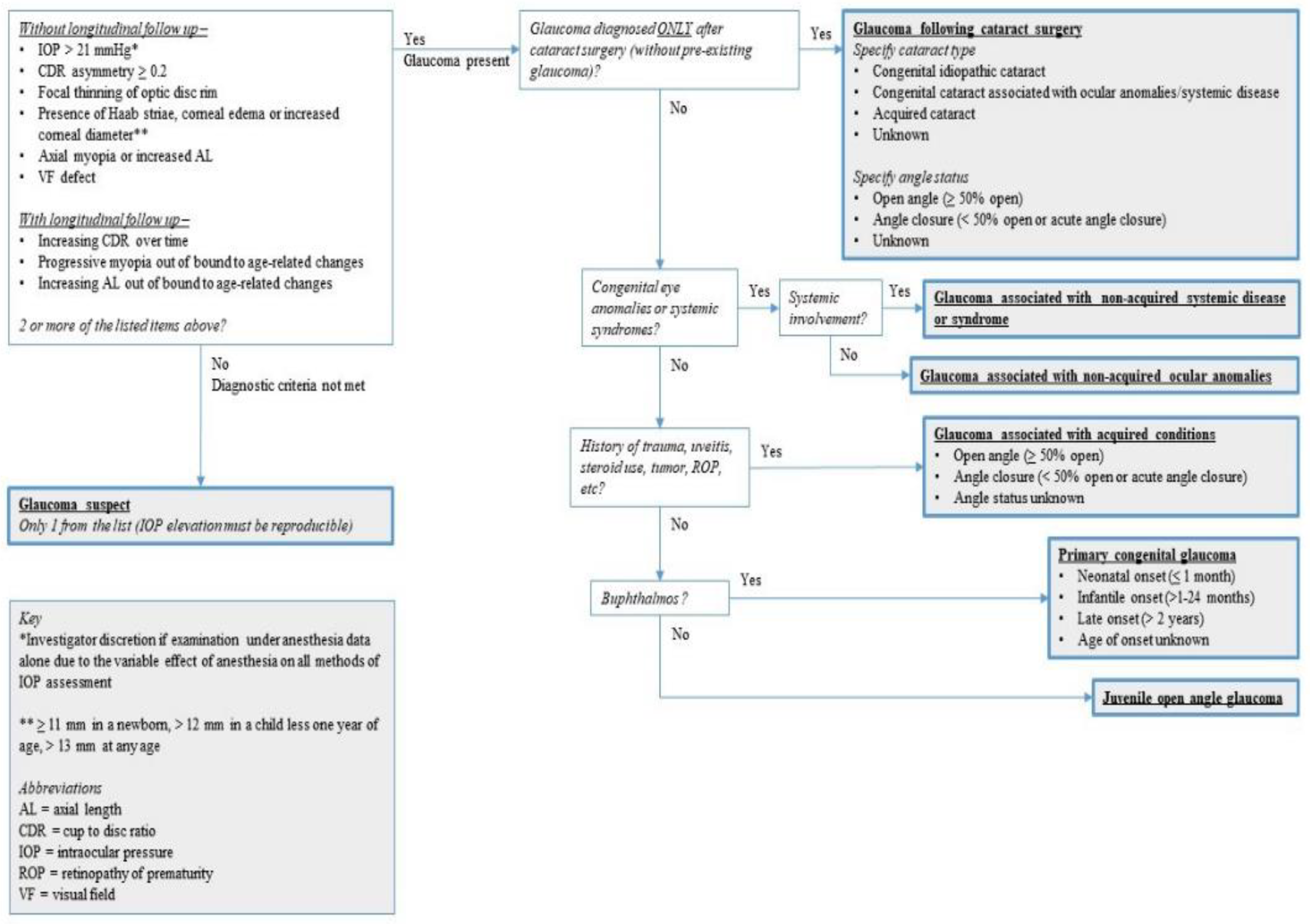
2. Classification and Diagnosis
3. Etiology
4. Screening
4.1. Importance of Awareness of Caregivers and Clinicians
4.2. Patterns of Referral
5. Clinical Characteristics
5.1. Anterior Segment Abnormalities
5.2. Posterior Segment Changes
5.3. Change in Axial Length and Refraction
5.4. Characteristics of Secondary Glaucomas
6. Examinations
6.1. IOP Measurement
6.2. Coreanl Diameter Measurement
6.3. Anterior Segment Imaging
6.4. Optical Coherence Tomography (OCT) Assessment
6.5. Retinal Imaging
7. General Principles of Management
8. Surgical Treatments
8.1. Angle Surgeries
8.1.1. Goniotomy
8.1.2. Trabeculotomy
8.1.3. Improvement of Conventional Angle Surgeries
8.2. Filtering Surgeries
8.2.1. Trabeculectomy
8.2.2. Glaucoma Drainage Device (GDD) Surgery
8.3. Minimally Invasive Glaucoma Surgery (MIGS)
8.4. Cyclophotocoagulation
8.5. Deep Sclerectomy
9. Medications in Pediatric Glaucoma
Developments and Challenges in Medical Treatments
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saavedra, C.; Rios, H.A.; Belalcazar, S.; Rosenstiehl, S.M. Characteristics of Pediatric Glaucoma in a Latin American Reference Center. J. Curr. Glaucoma Pract. 2020, 14, 10–15. [Google Scholar] [CrossRef]
- World Glaucoma Association. Childhood Glaucoma: The 9th Concensus Report of the World Glaucoma Association; Weinreb, R.N., Grajewski, A.L., Papadopoulos, M., Grigg, J., Freedman, S.E., Eds.; Kugler Publications: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Dada, T.; Aggarwal, A.; Bali, S.J.; Wadhwani, M.; Tinwala, S.; Sagar, R. Caregiver burden assessment in primary congenital glaucoma. Eur. J. Ophthalmol. 2013, 23, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Gao, J.; Li, X.; Yang, Q.; Lian, Y.; Xiao, H.; Huang, W. Burden, Positive Aspects, and Predictive Variables of Caregiving: A Study of Caregivers of Patients with Pediatric Glaucoma. J. Ophthalmol. 2019, 2019, 6980208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baig, N.B.; Chan, J.J.; Ho, J.C.; Tang, G.C.; Tsang, S.; Wan, K.H.; Yip, W.W.; Tham, C.C. Paediatric glaucoma in Hong Kong: A multicentre retrospective analysis of epidemiology, presentation, clinical interventions, and outcomes. Hong Kong Med. J. 2021, 27, 18–26. [Google Scholar] [CrossRef]
- Aponte, E.P.; Diehl, N.; Mohney, B.G. Incidence and clinical characteristics of childhood glaucoma: A population-based study. JAMA Ophthalmol. 2010, 128, 478–482. [Google Scholar] [CrossRef]
- Genĉík, A. Epidemiology and genetics of primary congenital glaucoma in Slovakia. Description of a form of primary congenital glaucoma in gypsies with autosomal-recessive inheritance and complete penetrance. Dev. Ophthalmol. 1989, 16, 76–115. [Google Scholar] [PubMed]
- Bejjani, B.A.; Stockton, D.W.; Lewis, R.A.; Tomey, K.F.; Dueker, D.K.; Jabak, M.; Astle, W.F.; Lupski, J.R. Multiple CYP1B1 mutations and incomplete penetrance in an inbred population segregating primary congenital glaucoma suggest frequent de novo events and a dominant modifier locus. Hum. Mol. Genet. 2000, 9, 367–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thau, A.; Lloyd, M.; Freedman, S.; Beck, A.; Grajewski, A.; Levin, A.V. New classification system for pediatric glaucoma: Implications for clinical care and a research registry. Curr. Opin. Ophthalmol. 2018, 29, 385–394. [Google Scholar] [CrossRef]
- Hoguet, A.; Grajewski, A.; Hodapp, E.; Chang, T.C. A retrospective survey of childhood glaucoma prevalence according to Childhood Glaucoma Research Network classification. Indian J. Ophthalmol. 2016, 64, 118–123. [Google Scholar] [CrossRef]
- Lopes, N.L.; Gracitelli, C.P.B.; Rolim-de-Moura, C. Childhood Glaucoma Profile in a Brazilian Tertiary Care Center Using Childhood Glaucoma Research Network Classification. J. Glaucoma 2021, 30, 129–133. [Google Scholar] [CrossRef]
- Mdala, S.; Zungu, T.; Manda, C.; Namate, C.; Fernando, E.; Twabi, H.S.; Msukwa, G.; Kayange, P.C. Profile of primary childhood glaucoma at a child eye health tertiary facility in Malawi. BMC Ophthalmol. 2022, 22, 45. [Google Scholar] [CrossRef] [PubMed]
- Tam, E.K.; Elhusseiny, A.M.; Shah, A.S.; Mantagos, I.S.; VanderVeen, D.K. Etiology and outcomes of childhood glaucoma at a tertiary referral center. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2022, 26, e111–e117. [Google Scholar] [CrossRef]
- Rauf, B.; Irum, B.; Kabir, F.; Firasat, S.; Naeem, M.A.; Khan, S.N.; Husnain, T.; Riazuddin, S.; Akram, J.; Riazuddin, S.A. A spectrum of CYP1B1 mutations associated with primary congenital glaucoma in families of Pakistani descent. Hum. Genome Var. 2016, 3, 16021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haddad, A.; Ait Boujmia, O.K.; El Maaloum, L.; Dehbi, H. Meta-analysis of CYP1B1 gene mutations in primary congenital glaucoma patients. Eur. J. Ophthalmol. 2021, 31, 2796–2807. [Google Scholar] [CrossRef]
- Tehreem, R.; Arooj, A.; Siddiqui, S.N.; Naz, S.; Afshan, K.; Firasat, S. Mutation screening of the CYP1B1 gene reveals thirteen novel disease-causing variants in consanguineous Pakistani families causing primary congenital glaucoma. PLoS ONE 2022, 17, e0274335. [Google Scholar] [CrossRef]
- Firasat, S.; Kaul, H.; Ashfaq, U.A.; Idrees, S. In silico analysis of five missense mutations in CYP1B1 gene in Pakistani families affected with primary congenital glaucoma. Int. Ophthalmol 2018, 38, 807–814. [Google Scholar] [CrossRef] [PubMed]
- Micheal, S.; Ayub, H.; Zafar, S.N.; Bakker, B.; Ali, M.; Akhtar, F.; Islam, F.; Khan, M.I.; Qamar, R.; den Hollander, A.I. Identification of novel CYP1B1 gene mutations in patients with primary congenital and primary open-angle glaucoma. Clin. Exp. Ophthalmol. 2015, 43, 31–39. [Google Scholar] [CrossRef]
- López-Garrido, M.P.; Medina-Trillo, C.; Morales-Fernandez, L.; Garcia-Feijoo, J.; Martínez-de-la-Casa, J.M.; García-Antón, M.; Escribano, J. Null CYP1B1 genotypes in primary congenital and nondominant juvenile glaucoma. Ophthalmology 2013, 120, 716–723. [Google Scholar] [CrossRef]
- Coêlho, R.E.A.; Sena, D.R.; Santa Cruz, F.; Moura, B.; Han, C.C.; Andrade, F.N.; Lira, R.P.C. CYP1B1 Gene and Phenotypic Correlation in Patients From Northeastern Brazil with Primary Congenital Glaucoma. J. Glaucoma 2019, 28, 161–164. [Google Scholar] [CrossRef]
- Geyer, O.; Wolf, A.; Levinger, E.; Harari-Shacham, A.; Walton, D.S.; Shochat, C.; Korem, S.; Bercovich, D. Genotype/phenotype correlation in primary congenital glaucoma patients from different ethnic groups of the Israeli population. Am. J. Ophthalmol. 2011, 151, 263–271.e1. [Google Scholar] [CrossRef]
- Abu-Amero, K.K.; Osman, E.A.; Mousa, A.; Wheeler, J.; Whigham, B.; Allingham, R.R.; Hauser, M.A.; Al-Obeidan, S.A. Screening of CYP1B1 and LTBP2 genes in Saudi families with primary congenital glaucoma: Genotype-phenotype correlation. Mol. Vis. 2011, 17, 2911–2919. [Google Scholar]
- Yazdani, S.; Miraftabi, A.; Pakravan, M.; Ghahari, E.; Tousi, B.K.; Sedigh, M.; Yaseri, M.; Elahi, E. Phenotype and Genotype Correlation in Iranian Primary Congenital Glaucoma Patients. J. Glaucoma 2016, 25, 33–38. [Google Scholar] [CrossRef]
- Cardoso, M.S.; Anjos, R.; Vieira, L.; Ferreira, C.; Xavier, A.; Brito, C. CYP1B1 gene analysis and phenotypic correlation in Portuguese children with primary congenital glaucoma. Eur. J. Ophthalmol. 2015, 25, 474–477. [Google Scholar] [CrossRef]
- Berraho, A.; Serrou, A.; Fritez, N.; El Annas, A.; Bencherifa, F.; Gaboun, F.; Hilal, L. Genotype-phenotype correlation in Moroccan patients with primary congenital glaucoma. J. Glaucoma 2015, 24, 297–305. [Google Scholar] [CrossRef]
- Shipley, J.M.; Mecham, R.P.; Maus, E.; Bonadio, J.; Rosenbloom, J.; McCarthy, R.T.; Baumann, M.L.; Frankfater, C.; Segade, F.; Shapiro, S.D. Developmental expression of latent transforming growth factor beta binding protein 2 and its requirement early in mouse development. Mol. Cell. Biol. 2000, 20, 4879–4887. [Google Scholar] [CrossRef] [Green Version]
- Rauf, B.; Irum, B.; Khan, S.Y.; Kabir, F.; Naeem, M.A.; Riazuddin, S.; Ayyagari, R.; Riazuddin, S.A. Novel mutations in LTBP2 identified in familial cases of primary congenital glaucoma. Mol. Vis. 2020, 26, 14–25. [Google Scholar]
- Yang, Y.; Zhang, L.; Li, S.; Zhu, X.; Sundaresan, P. Candidate Gene Analysis Identifies Mutations in CYP1B1 and LTBP2 in Indian Families with Primary Congenital Glaucoma. Genet. Test. Mol. Biomarkers 2017, 21, 252–258. [Google Scholar] [CrossRef]
- Micheal, S.; Siddiqui, S.N.; Zafar, S.N.; Iqbal, A.; Khan, M.I.; den Hollander, A.I. Identification of Novel Variants in LTBP2 and PXDN Using Whole-Exome Sequencing in Developmental and Congenital Glaucoma. PLoS ONE 2016, 11, e0159259. [Google Scholar] [CrossRef] [Green Version]
- Svidnicki, P.V.; Braghini, C.A.; Costa, V.P.; Schimiti, R.B.; de Vasconcellos, J.P.C.; de Melo, M.B. Occurrence of MYOC and CYP1B1 variants in juvenile open angle glaucoma Brazilian patients. Ophthalmic Genet. 2018, 39, 717–724. [Google Scholar] [CrossRef]
- Qiao, Y.; Chen, Y.; Tan, C.; Sun, X.; Chen, X.; Chen, J. Screening and Functional Analysis of TEK Mutations in Chinese Children With Primary Congenital Glaucoma. Front. Genet. 2021, 12, 764509. [Google Scholar] [CrossRef]
- Siggs, O.M.; Souzeau, E.; Taranath, D.A.; Dubowsky, A.; Chappell, A.; Zhou, T.; Javadiyan, S.; Nicholl, J.; Kearns, L.S.; Staffieri, S.E.; et al. Biallelic CPAMD8 Variants Are a Frequent Cause of Childhood and Juvenile Open-Angle Glaucoma. Ophthalmology 2020, 127, 758–766. [Google Scholar] [CrossRef] [PubMed]
- Gupta, V.; Somarajan, B.I.; Kaur, G.; Gupta, S.; Singh, R.; Pradhan, D.; Singh, H.; Kaur, P.; Sharma, A.; Chawla, B.; et al. Exome sequencing identifies procollagen-lysine 2-oxoglutarate 5-dioxygenase 2 mutations in primary congenital and juvenile glaucoma. Indian J. Ophthalmol. 2021, 69, 2710–2716. [Google Scholar] [CrossRef] [PubMed]
- Ferre-Fernández, J.J.; Aroca-Aguilar, J.D.; Medina-Trillo, C.; Bonet-Fernández, J.M.; Méndez-Hernández, C.D.; Morales-Fernández, L.; Corton, M.; Cabañero-Valera, M.J.; Gut, M.; Tonda, R.; et al. Whole-Exome Sequencing of Congenital Glaucoma Patients Reveals Hypermorphic Variants in GPATCH3, a New Gene Involved in Ocular and Craniofacial Development. Sci. Rep. 2017, 7, 46175. [Google Scholar] [CrossRef] [Green Version]
- Labelle-Dumais, C.; Pyatla, G.; Paylakhi, S.; Tolman, N.G.; Hameed, S.; Seymens, Y.; Dang, E.; Mandal, A.K.; Senthil, S.; Khanna, R.C.; et al. Loss of PRSS56 function leads to ocular angle defects and increased susceptibility to high intraocular pressure. Dis. Model. Mech. 2020, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishimura, D.Y.; Swiderski, R.E.; Alward, W.L.; Searby, C.C.; Patil, S.R.; Bennet, S.R.; Kanis, A.B.; Gastier, J.M.; Stone, E.M.; Sheffield, V.C. The forkhead transcription factor gene FKHL7 is responsible for glaucoma phenotypes which map to 6p25. Nat. Genet. 1998, 19, 140–147. [Google Scholar] [CrossRef]
- Semina, E.V.; Reiter, R.; Leysens, N.J.; Alward, W.L.; Small, K.W.; Datson, N.A.; Siegel-Bartelt, J.; Bierke-Nelson, D.; Bitoun, P.; Zabel, B.U.; et al. Cloning and characterization of a novel bicoid-related homeobox transcription factor gene, RIEG, involved in Rieger syndrome. Nat. Genet. 1996, 14, 392–399. [Google Scholar] [CrossRef]
- Tzoulaki, I.; White, I.M.; Hanson, I.M. PAX6 mutations: Genotype-phenotype correlations. BMC Genet. 2005, 6, 27. [Google Scholar] [CrossRef] [Green Version]
- Stoilov, I.R.; Costa, V.P.; Vasconcellos, J.P.; Melo, M.B.; Betinjane, A.J.; Carani, J.C.; Oltrogge, E.V.; Sarfarazi, M. Molecular genetics of primary congenital glaucoma in Brazil. Investig. Ophthalmol. Vis. Sci. 2002, 43, 1820–1827. [Google Scholar]
- Kakiuchi-Matsumoto, T.; Isashiki, Y.; Ohba, N.; Kimura, K.; Sonoda, S.; Unoki, K. Cytochrome P450 1B1 gene mutations in Japanese patients with primary congenital glaucoma. Am. J. Ophthalmol. 2001, 131, 345–350. [Google Scholar] [CrossRef]
- Haddad, M.A.; Sei, M.; Sampaio, M.W.; Kara-Jose, N. Causes of visual impairment in children: A study of 3210 cases. J. Pediatr. Ophthalmol. Strabismus 2007, 44, 232–240. [Google Scholar] [CrossRef]
- Dandona, L.; Williams, J.D.; Williams, B.C.; Rao, G.N. Population-based assessment of childhood blindness in southern India. Arch. Ophthalmol. 1998, 116, 545–546. [Google Scholar] [PubMed]
- Mandal, A.K.; Sulthana, S.S.; Gothwal, V.K. Primary Congenital Glaucoma: Trends in Presentation Over 3 Decades at a Tertiary Eye Care Center in India. J. Glaucoma 2020, 29, 1095–1100. [Google Scholar] [CrossRef] [PubMed]
- Leite, A.; Rolim-de-Moura, C. Referral reasons for evaluating childhood glaucoma in a tertiary service. Arq. Bras. Oftalmol. 2022, 85. [Google Scholar] [CrossRef]
- Chu, B.S. Weill-Marchesani syndrome and secondary glaucoma associated with ectopia lentis. Clin. Exp. Optom. 2006, 89, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Vu, D.M.; Stoler, J.; Rothman, A.L.; Chang, T.C. A Service Coverage Analysis of Primary Congenital Glaucoma Care Across the United States. Am. J. Ophthalmol. 2021, 224, 112–119. [Google Scholar] [CrossRef]
- Patil, B.; Tandon, R.; Sharma, N.; Verma, M.; Upadhyay, A.D.; Gupta, V.; Sihota, R. Corneal changes in childhood glaucoma. Ophthalmology 2015, 122, 87–92. [Google Scholar] [CrossRef]
- Alshigari, R.; Freidi, A.; Souru, C.; Edward, D.P.; Malik, R. Risk Factors for Blindness in Children With Primary Congenital Glaucoma-Follow-up of a Registry Cohort. Am. J. Ophthalmol. 2021, 224, 238–245. [Google Scholar] [CrossRef]
- Hu, Y.; Fang, L.; Guo, X.; Yang, X.; Chen, W.; Ding, X.; Liu, X.; He, M. Corneal Configurations and High-order Aberrations in Primary Congenital Glaucoma. J. Glaucoma 2018, 27, 1112–1118. [Google Scholar] [CrossRef]
- Gatzioufas, Z.; Labiris, G.; Stachs, O.; Hovakimyan, M.; Schnaidt, A.; Viestenz, A.; Käsmann-Kellner, B.; Seitz, B. Biomechanical profile of the cornea in primary congenital glaucoma. Acta Ophthalmol. 2013, 91, e29–e34. [Google Scholar] [CrossRef]
- Perucho-González, L.; Martínez de la Casa, J.M.; Morales-Fernández, L.; Bañeros-Rojas, P.; Saenz-Francés, F.; García-Feijoó, J. Intraocular pressure and biomechanical corneal properties measure by ocular response analyser in patients with primary congenital glaucoma. Acta Ophthalmol. 2016, 94, e293–e297. [Google Scholar] [CrossRef] [Green Version]
- Mahelková, G.; Filous, A.; Odehnal, M.; Cendelín, J. Corneal changes assessed using confocal microscopy in patients with unilateral buphthalmos. Investig. Ophthalmol. Vis. Sci. 2013, 54, 4048–4053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, S.; Chaurasia, A.K.; Sen, S.; Bhardwaj, M.; Mandal, S.; Titiyal, J.S.; Gupta, V. The Descemet Membrane in Primary Congenital Glaucoma. Cornea 2021, 40, 172–178. [Google Scholar] [CrossRef]
- Chan, J.Y.Y.; Choy, B.N.; Ng, A.L.; Shum, J.W. Review on the Management of Primary Congenital Glaucoma. J. Curr. Glaucoma Pract. 2015, 9, 92–99. [Google Scholar] [CrossRef]
- Al Nosair, G.; Khandekar, R.; Al-Shamrani, M.; Edward, D.P. Ciliary body location in eyes with and without primary congenital glaucoma. Can. J. Ophthalmol. 2017, 52, 578–582. [Google Scholar] [CrossRef] [PubMed]
- Senthil, S.; Ali, M.J.; Chary, R.; Mandal, A.K. Co-existing lacrimal drainage anomalies in eyes with congenital Glaucoma. Eur. J. Ophthalmol. 2022, 32, 2683–2687. [Google Scholar] [CrossRef] [PubMed]
- Harju, M.; Saari, J.; Kurvinen, L.; Vesti, E. Reversal of optic disc cupping in glaucoma. Br. J. Ophthalmol. 2008, 92, 901–905. [Google Scholar] [CrossRef]
- Ely, A.L.; El-Dairi, M.A.; Freedman, S.F. Cupping reversal in pediatric glaucoma—Evaluation of the retinal nerve fiber layer and visual field. Am. J. Ophthalmol. 2014, 158, 905–915. [Google Scholar] [CrossRef]
- El-Dairi, M.A.; Holgado, S.; Asrani, S.G.; Enyedi, L.B.; Freedman, S.F. Correlation between optical coherence tomography and glaucomatous optic nerve head damage in children. Brit. J. Ophthalmol. 2009, 93, 1325–1330. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.; You, Q.S.; Xu, X.; Gao, F.; Zhang, Z.; Li, B.; Jonas, J.B. Scleral and choroidal thickness in secondary high axial myopia. Retina 2016, 36, 1579–1585. [Google Scholar] [CrossRef]
- Milla, E.; Leszczynska, A.; Rey, A.; Navarro, M.; Larena, C. Novel FBN1 mutation causes Marfan syndrome with bilateral ectopia lentis and refractory glaucoma. Eur. J. Ophthalmol. 2012, 22, 667–669. [Google Scholar] [CrossRef]
- Ha, A.; Kim, J.S.; Baek, S.U.; Park, Y.J.; Jeoung, J.W.; Park, K.H.; Kim, Y.K. Facial Port-Wine Stain Phenotypes Associated with Glaucoma Risk in Neonates. Am. J. Ophthalmol. 2020, 220, 183–190. [Google Scholar] [CrossRef]
- Khaier, A.; Nischal, K.K.; Espinosa, M.; Manoj, B. Periocular port wine stain: The great ormond street hospital experience. Ophthalmology 2011, 118, 2274–2278.e1. [Google Scholar] [CrossRef]
- Kaushik, S.; Choudhary, S.; Dhingra, D.; Singh, M.P.; Gupta, G.; Arora, A.; Thattaruthody, F.; Pandav, S.S. Newborn Glaucoma: A Neglected Manifestation of Congenital Rubella Syndrome. Ophthalmol. Glaucoma 2022, 5, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Mikhail, M.; Sabri, K.; Levin, A.V. Effect of anesthesia on intraocular pressure measurement in children. Surv. Ophthalmol. 2017, 62, 648–658. [Google Scholar] [CrossRef] [PubMed]
- Senthil, S.; Nakka, M.; Rout, U.; Ali, H.; Choudhari, N.; Badakere, S.; Garudadri, C. Changes in intraocular pressures associated with inhalational and mixed anesthetic agents currently used in ophthalmic surgery. Indian J. Ophthalmol. 2021, 69, 1808–1814. [Google Scholar] [CrossRef] [PubMed]
- Nagdeve, N.G.; Yaddanapudi, S.; Pandav, S.S. The effect of different doses of ketamine on intraocular pressure in anesthetized children. J. Pediatr. Ophthalmol. Strabismus 2006, 43, 219–223. [Google Scholar] [CrossRef]
- McCarthy, D. The effect of nitrous oxide on intra-ocular pressure. Anaesthesia 2012, 67, 680–681. [Google Scholar] [CrossRef]
- Feng, C.S.; Jin, K.W.; Yi, K.; Choi, D.G. Comparison of Intraocular Pressure Measurements Obtained by Rebound, Noncontact, and Goldmann Applanation Tonometry in Children. Am. J. Ophthalmol. 2015, 160, 937–943.e1. [Google Scholar] [CrossRef] [PubMed]
- Flemmons, M.S.; Hsiao, Y.C.; Dzau, J.; Asrani, S.; Jones, S.; Freedman, S.F. Icare rebound tonometry in children with known and suspected glaucoma. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2011, 15, 153–157. [Google Scholar] [CrossRef]
- Vodenčarević, A.N.; Jusufović, V.; Terzić, S.; Halilbašić, M. Comparison of Intraocular Pressure Measurements Obtained by Rebound, Noncontact, and Goldmann Applanation Tonometry in Children. Am. J. Ophthalmol. 2016, 163, 192. [Google Scholar] [CrossRef]
- Chan, W.H.; Lloyd, I.C.; Symes, R.J.; Ashworth, J.L.; Cosgrove, E.; Pilling, R.; Biswas, S. Accuracy of Intraocular Pressure Measurement with the Icare Tonometer in Children. Asia Pac. J. Ophthalmol. 2015, 4, 357–359. [Google Scholar] [CrossRef] [PubMed]
- Lambert, S.R.; Melia, M.; Buffenn, A.N.; Chiang, M.F.; Simpson, J.L.; Yang, M.B. Rebound tonometry in children: A report by the American Academy of Ophthalmology. Ophthalmology 2013, 120, e21–e27. [Google Scholar] [CrossRef] [PubMed]
- Dahlmann-Noor, A.H.; Puertas, R.; Tabasa-Lim, S.; El-Karmouty, A.; Kadhim, M.; Wride, N.K.; Lewis, A.; Grosvenor, D.; Rai, P.; Papadopoulos, M.; et al. Comparison of handheld rebound tonometry with Goldmann applanation tonometry in children with glaucoma: A cohort study. BMJ Open 2013, 3, e001788. [Google Scholar] [CrossRef] [PubMed]
- Angmo, D.; Ramesh, P.; Mahalingam, K.; Azmira, K.; Pandey, S.; Gupta, V.; Sihota, R.; Dada, T. Comparative Evaluation of Rebound and Perkins Tonometers in Pediatric Glaucoma With Varied Corneal Characteristics. J. Glaucoma 2021, 30, 312–316. [Google Scholar] [CrossRef]
- Serafino, M.; Villani, E.; Lembo, A.; Rabbiolo, G.; Specchia, C.; Trivedi, R.H.; Nucci, P. A comparison of Icare PRO and Perkins tonometers in anesthetized children. Int. Ophthalmol. 2020, 40, 19–29. [Google Scholar] [CrossRef]
- Esmael, A.; Ismail, Y.M.; Elhusseiny, A.M.; Fayed, A.E.; Elhilali, H.M. Agreement profiles for rebound and applanation tonometry in normal and glaucomatous children. Eur. J. Ophthalmol. 2019, 29, 379–385. [Google Scholar] [CrossRef]
- AlHarkan, D.H.; Al-Shamlan, F.T.; Edward, D.P.; Khan, A.O. A Comparison of Rebound to Indentation Tonometry in Supine Sedated Children with Glaucoma. Middle East Afr. J. Ophthalmol. 2016, 23, 183–186. [Google Scholar] [CrossRef]
- McKee, E.C.; Ely, A.L.; Duncan, J.E.; Dosunmu, E.O.; Freedman, S.F. A comparison of Icare PRO and Tono-Pen XL tonometers in anesthetized children. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2015, 19, 332–337. [Google Scholar] [CrossRef]
- Sehrawat, P.; Beri, S.; Garg, R.; Datta, V.; Shandil, A. Central corneal thickness and corneal diameter in preterm and term newborns and preterm neonates at term. Indian J. Ophthalmol. 2019, 67, 1575–1578. [Google Scholar] [CrossRef]
- Kun, L.; Szigeti, A.; Bausz, M.; Nagy, Z.Z.; Maka, E. Preoperative biometry data of eyes with unilateral congenital cataract. J. Cataract. Refract. Surg. 2018, 44, 1198–1202. [Google Scholar] [CrossRef]
- Bafna, R.K.; Mahalingam, K.; Rakheja, V.; Sharma, N.; Gupta, S.; Daniel, R.A.; Gupta, V. Validating the use of U-tool as a novel method for measuring the corneal diameter in infants screened for congenital glaucoma. Indian J. Ophthalmol. 2022, 70, 143–146. [Google Scholar] [CrossRef]
- Tandon, A.; Watson, C.; Ayyala, R. Ultrasound biomicroscopy measurement of Schlemm’s canal in pediatric patients with and without glaucoma. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2017, 21, 234–237. [Google Scholar] [CrossRef] [PubMed]
- Janssens, R.; van Rijn, L.J.; Eggink, C.A.; Jansonius, N.M.; Janssen, S.F. Ultrasound biomicroscopy of the anterior segment in patients with primary congenital glaucoma: A review of the literature. Acta Ophthalmol. 2022, 100, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Alexander, J.L.; Maripudi, S.; Kannan, K.; Drechsler, J.; Levin, M.R.; Saeedi, O.J.; Kaleem, M.; Bazemore, M.; Karwoski, B.; Martinez, C.; et al. Semiautomated Assessment of Anterior Segment Structures in Pediatric Glaucoma Using Quantitative Ultrasound Biomicroscopy. J. Glaucoma 2021, 30, e222–e226. [Google Scholar] [CrossRef]
- Gupta, V.; Chaurasia, A.K.; Gupta, S.; Gorimanipalli, B.; Sharma, A.; Gupta, A. In Vivo Analysis of Angle Dysgenesis in Primary Congenital, Juvenile, and Adult-Onset Open Angle Glaucoma. Investig. Ophthalmol. Vis. Sci. 2017, 58, 6000–6005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Posarelli, C.; Sartini, F.; Casini, G.; Passani, A.; Toro, M.D.; Vella, G.; Figus, M. What Is the Impact of Intraoperative Microscope-Integrated OCT in Ophthalmic Surgery? Relevant Applications and Outcomes. A Systematic Review. J. Clin. Med. 2020, 9, 1682. [Google Scholar] [CrossRef] [PubMed]
- Ghasia, F.F.; El-Dairi, M.; Freedman, S.F.; Rajani, A.; Asrani, S. Reproducibility of spectral-domain optical coherence tomography measurements in adult and pediatric glaucoma. J. Glaucoma 2015, 24, 55–63. [Google Scholar] [CrossRef]
- Prakalapakorn, S.G.; Freedman, S.F.; Lokhnygina, Y.; Gandhi, N.G.; Holgado, S.; Chen, B.B.; El-Dairi, M.A. Longitudinal reproducibility of optical coherence tomography measurements in children. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2012, 16, 523–528. [Google Scholar] [CrossRef] [Green Version]
- Xu, L.; Freedman, S.F.; Silverstein, E.; Muir, K.; El-Dairi, M. Longitudinal reproducibility of spectral domain optical coherence tomography in children with physiologic cupping and stable glaucoma. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2019, 23, 262.e1–262.e6. [Google Scholar] [CrossRef]
- Lever, M.; Halfwassen, C.; Unterlauft, J.D.; Bechrakis, N.E.; Manthey, A.; Böhm, M.R.R. The Paediatric Glaucoma Diagnostic Ability of Optical Coherence Tomography: A Comparison of Macular Segmentation and Peripapillary Retinal Nerve Fibre Layer Thickness. Biology 2021, 10, 260. [Google Scholar] [CrossRef]
- Shoji, T.; Sato, H.; Ishida, M.; Takeuchi, M.; Chihara, E. Assessment of glaucomatous changes in subjects with high myopia using spectral domain optical coherence tomography. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1098–1102. [Google Scholar] [CrossRef] [Green Version]
- Rao, A.; Sahoo, B.; Kumar, M.; Varshney, G.; Kumar, R. Retinal nerve fiber layer thickness in children < 18 years by spectral-domain optical coherence tomography. Semin. Ophthalmol. 2013, 28, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Goh, J.P.; Koh, V.; Chan, Y.H.; Ngo, C. Macular Ganglion Cell and Retinal Nerve Fiber Layer Thickness in Children with Refractive Errors-An Optical Coherence Tomography Study. J. Glaucoma 2017, 26, 619–625. [Google Scholar] [CrossRef]
- Shah, S.D.; Haq, A.; Toufeeq, S.; Tu, Z.; Edawaji, B.; Abbott, J.; Gottlob, I.; Proudlock, F.A. Reliability and Recommended Settings for Pediatric Circumpapillary Retinal Nerve Fiber Layer Imaging Using Hand-Held Optical Coherence Tomography. Transl. Vis. Sci. Technol. 2020, 9, 43. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Purohit, R.; Patel, A.; Papageorgiou, E.; Sheth, V.; Maconachie, G.; Pilat, A.; McLean, R.J.; Proudlock, F.A.; Gottlob, I. In Vivo Foveal Development Using Optical Coherence Tomography. Investig. Ophthalmol. Vis. Sci. 2015, 56, 4537–4545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Go, M.S.; Barman, N.R.; Kelly, M.P.; House, R.J.; Rotruck, J.C.; El-Dairi, M.A.; Freedman, S.F. Overhead Mounted Optical Coherence Tomography in Childhood Glaucoma Evaluation. J. Glaucoma 2020, 29, 742–749. [Google Scholar] [CrossRef]
- Pilat, A.V.; Shah, S.; Sheth, V.; Purohit, R.; Proudlock, F.A.; Abbott, J.; Gottlob, I. Detection and characterisation of optic nerve and retinal changes in primary congenital glaucoma using hand-held optical coherence tomography. BMJ Open Ophthalmol. 2019, 4, e000194. [Google Scholar] [CrossRef] [Green Version]
- Erraguntla, V.; MacKeen, L.D.; Atenafu, E.; Stephens, D.; Buncic, J.R.; Budning, A.S.; Levin, A.V. Assessment of change of optic nerve head cupping in pediatric glaucoma using the RetCam 120. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2006, 10, 528–533. [Google Scholar] [CrossRef]
- Kaur, R.; Singh, H.; Samria, S.; Kumar, N.; Parachuri, N.; Sharma, R.; Bandello, F.; Loewenstein, A.; Bilong, Y.; Hafeez Faridi, M.; et al. MII RetCam assisted smartphone-based fundus imaging (MSFI)—A boon for paediatric retinal imaging. Eye 2020, 34, 1307–1309. [Google Scholar] [CrossRef]
- Sharma, A.; Goyal, A.; Bilong, Y.; Shah, P.; Banker, A.; Kumar, N.; Sharma, R.; Kuppermann, B.D.; Bandello, F. Comparison of a Smartphone-Based Photography Method with Indirect Ophthalmoscopic Assessment in Referable Retinopathy of Prematurity: A Smart Retinopathy of Prematurity Model Pilot Study. Ophthalmol. Retin. 2019, 3, 911–912. [Google Scholar] [CrossRef]
- Goyal, A.; Gopalakrishnan, M.; Anantharaman, G.; Chandrashekharan, D.P.; Thachil, T.; Sharma, A. Smartphone guided wide-field imaging for retinopathy of prematurity in neonatal intensive care unit—A Smart ROP (SROP) initiative. Indian J. Ophthalmol. 2019, 67, 840–845. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, S.D.; Netland, P.A. Trabeculectomy versus combined trabeculotomy-trabeculectomy in pediatric glaucoma. J. Pediatr. Ophthalmol. Strabismus 2012, 49, 359–365. [Google Scholar] [CrossRef]
- Eldaly, M.A. Pneumatic trabecular bypass versus trabeculotomy in the management of primary congenital glaucoma. Graefe’s Arch Clin. Exp. Ophthalmol. 2014, 252, 989–994. [Google Scholar] [CrossRef] [PubMed]
- Temkar, S.; Gupta, S.; Sihota, R.; Sharma, R.; Angmo, D.; Pujari, A.; Dada, T. Illuminated microcatheter circumferential trabeculotomy versus combined trabeculotomy-trabeculectomy for primary congenital glaucoma: A randomized controlled trial. Am. J. Ophthalmol. 2015, 159, 490–497.e2. [Google Scholar] [CrossRef]
- Lim, M.E.; Neely, D.E.; Wang, J.; Haider, K.M.; Smith, H.A.; Plager, D.A. Comparison of 360-degree versus traditional trabeculotomy in pediatric glaucoma. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2015, 19, 145–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shakrawal, J.; Bali, S.; Sidhu, T.; Verma, S.; Sihota, R.; Dada, T. Randomized Trial on Illuminated-Microcatheter Circumferential Trabeculotomy versus Conventional Trabeculotomy in Congenital Glaucoma. Am. J. Ophthalmol. 2017, 180, 158–164. [Google Scholar] [CrossRef]
- Abdelrahman, A.M.; El Sayed, Y.M. Micropulse Versus Continuous Wave Transscleral Cyclophotocoagulation in Refractory Pediatric Glaucoma. J. Glaucoma 2018, 27, 900–905. [Google Scholar] [CrossRef]
- El Sayed, Y.M.; Gawdat, G.I. Microcatheter-assisted Trabeculotomy versus 2-site Trabeculotomy with the Rigid Probe Trabeculotome in Primary Congenital Glaucoma. J. Glaucoma 2018, 27, 371–376. [Google Scholar] [CrossRef]
- Elwehidy, A.S.; Badawi, A.E.; Hagras, S.M.; Bayoumi, N.H.L. Ahmed Glaucoma Valve Revision versus Visco-Trabeculotomy after Failed Ahmed Glaucoma Valve in Refractory Pediatric Glaucoma. J. Glaucoma 2019, 28, 307–312. [Google Scholar] [CrossRef]
- Elhofi, A.; Helaly, H.A. Non-Penetrating Deep Sclerectomy versus Trabeculectomy in Primary Congenital Glaucoma. Clin. Ophthalmol. 2020, 14, 1277–1285. [Google Scholar] [CrossRef]
- Puthuran, G.V.; Wijesinghe, H.K.; Gedde, S.J.; Chiranjeevi, K.P.; Mani, I.; Krishnadas, S.R.; Lee Robin, A.; Palmberg, P. Surgical Outcomes of Superotemporal versus Inferonasal Placement of Aurolab Aqueous Drainage Implant in Refractory Pediatric Glaucoma. Am. J. Ophthalmol. 2021, 224, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Qiao, Y.; Tan, C.; Chen, X.; Sun, X.; Chen, J. Gonioscopy-assisted transluminal trabeculotomy versus goniotomy with Kahook dual blade in patients with uncontrolled juvenile open-angle glaucoma: A retrospective study. BMC Ophthalmol. 2021, 21, 395. [Google Scholar] [CrossRef]
- Elwehidy, A.S.; Bayoumi, N.H.L.; Abd Elfattah, D.; Hagras, S.M. Surgical Outcomes of Visco-Circumferential-Suture-Trabeculotomy versus Rigid Probe Trabeculotomy in Primary Congenital Glaucoma: A 3-Year Randomized Controlled Study. J. Glaucoma 2022, 31, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Barkan, O. Operation for congenital glaucoma. Am. J. Ophthalmol. 1942, 25, 552–568. [Google Scholar] [CrossRef]
- Scheie, H.G. Goniotomy in the treatment of congenital glaucoma. Trans. Am. Ophthalmol. Soc. 1949, 47, 115–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaushik, S.; Gupta, G.; Thattaruthody, F.; Dhingra, D.; Kumari, K.; Arora, A.; Snehi, S.; Raj, S.; Pandav, S.S. Goniotomy for initial and re-surgery for childhood glaucoma in Northern India. Indian J. Ophthalmol. 2021, 69, 2088–2094. [Google Scholar] [CrossRef]
- Bowman, R.J.; Dickerson, M.; Mwende, J.; Khaw, P.T. Outcomes of goniotomy for primary congenital glaucoma in East Africa. Ophthalmology 2011, 118, 236–240. [Google Scholar] [CrossRef]
- Mukkamala, L.; Fechtner, R.; Holland, B.; Khouri, A.S. Characteristics of Children with Primary Congenital Glaucoma Receiving Trabeculotomy and Goniotomy. J. Pediatr. Ophthalmol. Strabismus 2015, 52, 377–382. [Google Scholar] [CrossRef]
- Al-Hazmi, A.; Awad, A.; Zwaan, J.; Al-Mesfer, S.A.; Al-Jadaan, I.; Al-Mohammed, A. Correlation between surgical success rate and severity of congenital glaucoma. Br. J. Ophthalmol. 2005, 89, 449–453. [Google Scholar] [CrossRef] [Green Version]
- Freedman, S.F.; Rodriguez-Rosa, R.E.; Rojas, M.C.; Enyedi, L.B. Goniotomy for glaucoma secondary to chronic childhood uveitis. Am. J. Ophthalmol. 2002, 133, 617–621. [Google Scholar] [CrossRef]
- Hassanein, D.H.; Awadein, A.; Elhilali, H. Factors associated with early and late failure after goniotomy for primary pediatric glaucoma. Eur. J. Ophthalmol. 2020, 30, 162–167. [Google Scholar] [CrossRef]
- Martin, E.; Le Meur, G.; Orignac, I.; Weber, M.; Lebranchu, P.; Péchereau, A. Trabeculotomy as first-line surgical treatment in pediatric glaucoma: Surgical and visual outcomes from a 7-year retrospective study. J. Fr. Ophtalmol. 2014, 37, 707–716. [Google Scholar] [CrossRef]
- Demirok, G.; Özkan, G.; Kaderli, A.; Güvenç, U.; Yakın, M.; Ekşioğlu, Ü. Factors affecting the surgical success of trabeculectomy performed as the first surgery in primary pediatric glaucoma. Int. Ophthalmol. 2022, 42, 2511–2518. [Google Scholar] [CrossRef]
- Harms, H.; Dannheim, R. Epicritical consideration of 300 cases of trabeculotomy ‘ab externo’. Trans. Ophthalmol. Soc. UK 1970, 89, 491–499. [Google Scholar]
- Zagora, S.L.; Funnell, C.L.; Martin, F.J.; Smith, J.E.; Hing, S.; Billson, F.A.; Veillard, A.S.; Jamieson, R.V.; Grigg, J.R. Primary congenital glaucoma outcomes: Lessons from 23 years of follow-up. Am. J. Ophthalmol. 2015, 159, 788–796. [Google Scholar] [CrossRef]
- El Sayed, Y.; Esmael, A.; Mettias, N.; El Sanabary, Z.; Gawdat, G. Factors influencing the outcome of goniotomy and trabeculotomy in primary congenital glaucoma. Br. J. Ophthalmol. 2021, 105, 1250–1255. [Google Scholar] [CrossRef]
- Areaux, R.G., Jr.; Grajewski, A.L.; Balasubramaniam, S.; Brandt, J.D.; Jun, A.; Edmunds, B.; Shyne, M.T.; Bitrian, E. Trabeculotomy Ab Interno with the Trab360 Device for Childhood Glaucomas. Am. J. Ophthalmol. 2020, 209, 178–186. [Google Scholar] [CrossRef]
- Al Habash, A.; Otaif, W.; Edward, D.P.; Al Jadaan, I. Surgical Outcomes of Microcatheter-assisted Trabeculotomy as a Secondary Procedure in Patients with Primary Congenital Glaucoma. Middle East Afr. J. Ophthalmol. 2020, 27, 145–149. [Google Scholar] [CrossRef]
- Berger, O.; Mohamed-Noriega, J.; Low, S.; Daniel, M.C.; Petchyim, S.; Papadopoulos, M.; Brookes, J. From Conventional Angle Surgery to 360-Degree Trabeculotomy in Pediatric Glaucoma. Am. J. Ophthalmol. 2020, 219, 77–86. [Google Scholar] [CrossRef]
- Grover, D.S.; Godfrey, D.G.; Smith, O.; Feuer, W.J.; Montes de Oca, I.; Fellman, R.L. Gonioscopy-assisted transluminal trabeculotomy, ab interno trabeculotomy: Technique report and preliminary results. Ophthalmology 2014, 121, 855–861. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, H.; Han, Y.; Shi, Y.; Xin, C.; Yin, P.; Li, M.; Cao, K.; Wang, N. Outcomes of gonioscopy-assisted transluminal trabeculotomy in juvenile-onset primary open-angle glaucoma. Eye 2021, 35, 2848–2854. [Google Scholar] [CrossRef]
- Aktas, Z.; Ucgul, A.Y.; Atalay, H.T. Outcomes of Circumferential Trabeculotomy and Converted 180-Degree Traditional Trabeculotomy in Patients with Neonatal-onset Primary Congenital Glaucoma. J. Glaucoma 2020, 29, 813–818. [Google Scholar] [CrossRef]
- Dragosloveanu, C.D.M.; Celea, C.G.; Dragosloveanu, Ş. Comparison of 360° circumferential trabeculotomy and conventional trabeculotomy in primary pediatric glaucoma surgery: Complications, reinterventions and preoperative predictive risk factors. Int. Ophthalmol. 2020, 40, 3547–3554. [Google Scholar] [CrossRef]
- Rojas, C.; Bohnsack, B.L. Rate of Complete Catheterization of Schlemm’s Canal and Trabeculotomy Success in Primary and Secondary Childhood Glaucomas. Am. J. Ophthalmol. 2020, 212, 69–78. [Google Scholar] [CrossRef]
- Panigrahi, A.; Huang, A.S.; Arora, M.; Kumari, S.; Mahalingam, K.; Gupta, V.; Gupta, S. Indocyanine Green Aided Schlemm Canal Identification during Gonioscopic Assisted Transluminal Trabeculotomy. J. Glaucoma 2022, 31, e69–e71. [Google Scholar] [CrossRef]
- Gupta, S.; Panigrahi, A.; Mahalingam, K.; Kumari, S.; Gupta, V. External Jugular Vein Compression Aided Gonioscopy Assisted Transluminal Trabeculotomy in Eyes with Congenital Glaucoma. J. Glaucoma 2022, 31, e43–e45. [Google Scholar] [CrossRef]
- Stürmer, J.; Broadway, D.C.; Hitchings, R.A. Young patient trabeculectomy. Assessment of risk factors for failure. Ophthalmology 1993, 100, 928–939. [Google Scholar] [CrossRef]
- Gurney, S.P.; Ahmad, M.; Makanjuola, T.; Ramm, L.; Parulekar, M.V. Long-term Efficacy of Mitomycin C Augmented Trabeculectomy in a Mixed Pediatric Glaucoma Cohort. J. Glaucoma 2021, 30, 357–361. [Google Scholar] [CrossRef]
- Jayaram, H.; Scawn, R.; Pooley, F.; Chiang, M.; Bunce, C.; Strouthidis, N.G.; Khaw, P.T.; Papadopoulos, M. Long-Term Outcomes of Trabeculectomy Augmented with Mitomycin C Undertaken within the First 2 Years of Life. Ophthalmology 2015, 122, 2216–2222. [Google Scholar] [CrossRef] [Green Version]
- Tsai, A.S.; Boey, P.Y.; Htoon, H.M.; Wong, T.T. Bleb needling outcomes for failed trabeculectomy blebs in Asian eyes: A 2-year follow up. Int. J. Ophthalmol. 2015, 8, 748–753. [Google Scholar] [CrossRef] [Green Version]
- Shah, C.; Sen, P.; Mohan, A.; Sen, A.; Sood, D.; Jain, E. Outcome of Bleb Needling with 5-Fluorouracil in Failed Filtering Procedures in Pediatric Glaucoma. J. Pediatr. Ophthalmol. Strabismus 2021, 58, 118–125. [Google Scholar] [CrossRef]
- Shah, C.; Sen, P.; Mohan, A.; Peeush, P.; Jain, E.; Prasad, K.; Sen, A.; Tripathi, S. Outcomes and risk factors for failure of trabeculectomy with mitomycin C in children with traumatic glaucoma—A retrospective study. Indian J. Ophthalmol. 2022, 70, 590–596. [Google Scholar] [CrossRef]
- Brandt, J.D. Use of a Novel Microshunt in Refractory Childhood Glaucoma: Initial Experience in a Compassionate Use/Early Access Cohort. Am. J. Ophthalmol. 2022, 239, 223–229. [Google Scholar] [CrossRef]
- Glaser, T.S.; Meekins, L.C.; Freedman, S.F. Outcomes and lessons learned from two decades’ experience with glaucoma drainage device implantation for refractory Sturge Weber-associated childhood glaucoma. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2021, 25, 332.e1–332.e6. [Google Scholar] [CrossRef]
- Gedde, S.J.; Singh, K.; Schiffman, J.C.; Feuer, W.J. The Tube Versus Trabeculectomy Study: Interpretation of results and application to clinical practice. Curr. Opin. Ophthalmol. 2012, 23, 118–126. [Google Scholar] [CrossRef]
- Senthil, S.; Rai, M.; Mohamed, A.; Bagga, B.; Ramappa, M. Outcomes of Ahmed Glaucoma Valve Implantation in Eyes with Pediatric Keratoplasty. Ophthalmol. Glaucoma 2022, 5, 94–100. [Google Scholar] [CrossRef]
- Pakravan, M.; Esfandiari, H.; Yazdani, S.; Doozandeh, A.; Dastborhan, Z.; Gerami, E.; Kheiri, B.; Pakravan, P.; Yaseri, M.; Hassanpour, K. Clinical outcomes of Ahmed glaucoma valve implantation in pediatric glaucoma. Eur. J. Ophthalmol. 2019, 29, 44–51. [Google Scholar] [CrossRef]
- Geyer, O.; Segal, A.; Melamud, A.; Wolf, A. Clinical Outcomes after Ahmed Glaucoma Valve Implantation for Pediatric Glaucoma after Congenital Cataract Surgery. J. Glaucoma 2021, 30, 78–82. [Google Scholar] [CrossRef]
- Promelle, V.; Lyons, C.J. Long-term Results of Ahmed Valve Implantation with Mitomycin-C in Pediatric Glaucoma. J. Glaucoma 2021, 30, 596–605. [Google Scholar] [CrossRef]
- Dawodu, O.; Levin, A.V. Spontaneous disconnection of glaucoma tube shunt extenders. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2010, 14, 361–363. [Google Scholar] [CrossRef] [Green Version]
- Porter, A.; Lee, G.A.; Shah, P.; Todd, B. Glaucoma drainage device tube extension without the need for a tube extender device or angiocatheter. Clin. Exp. Ophthalmol. 2017, 45, 308–310. [Google Scholar] [CrossRef] [PubMed]
- Sarkisian, S.R.; Netland, P.A. Tube extender for revision of glaucoma drainage implants. J. Glaucoma 2007, 16, 637–639. [Google Scholar] [CrossRef] [PubMed]
- Merrill, K.D.; Suhr, A.W.; Lim, M.C. Long-term success in the correction of exposed glaucoma drainage tubes with a tube extender. Am. J. Ophthalmol. 2007, 144, 136–137. [Google Scholar] [CrossRef]
- Smith, M.F.; Doyle, J.W. Results of another modality for extending glaucoma drainage tubes. J. Glaucoma 1999, 8, 310–314. [Google Scholar] [CrossRef]
- Sternfeld, A.; Dotan, G.; Bohra, L.; Roarty, J. Ahmed Valve Tube Extension in Pediatric Glaucoma. J. Glaucoma 2020, 29, 276–279. [Google Scholar] [CrossRef]
- Chen, A.; Yu, F.; Law, S.K.; Giaconi, J.A.; Coleman, A.L.; Caprioli, J. Valved Glaucoma Drainage Devices in Pediatric Glaucoma: Retrospective Long-term Outcomes. JAMA Ophthalmol. 2015, 133, 1030–1035. [Google Scholar] [CrossRef] [Green Version]
- Ou, Y.; Yu, F.; Law, S.K.; Coleman, A.L.; Caprioli, J. Outcomes of Ahmed glaucoma valve implantation in children with primary congenital glaucoma. Arch Ophthalmol. 2009, 127, 1436–1441. [Google Scholar] [CrossRef] [Green Version]
- Almobarak, F.; Khan, A.O. Complications and 2-year valve survival following Ahmed valve implantation during the first 2 years of life. Br. J. Ophthalmol. 2009, 93, 795–798. [Google Scholar] [CrossRef]
- Daniel, M.C.; Mohamed-Noriega, J.; Petchyim, S.; Brookes, J. Childhood Glaucoma: Long-Term Outcomes of Glaucoma Drainage Device Implantation within the First 2 Years of Life. J. Glaucoma 2019, 28, 878–883. [Google Scholar] [CrossRef]
- Nassiri, N.; Nouri-Mahdavi, K.; Coleman, A.L. Ahmed glaucoma valve in children: A review. Saudi J. Ophthalmol. 2011, 25, 317–327. [Google Scholar] [CrossRef] [Green Version]
- Jomar, D.E.; Al-Shahwan, S.; Al-Beishri, A.S.; Freidi, A.; Malik, R. Risk factors for glaucoma drainage device exposure in children: A case-control study. Am. J. Ophthalmol. 2022, 245, 174–183. [Google Scholar] [CrossRef]
- Jacobson, A.; Bohnsack, B.L. Ologen augmentation of Ahmed valves in pediatric glaucomas. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2022, 26, 122.e1–122.e6. [Google Scholar] [CrossRef]
- Elwehidy, A.S.; Bayoumi, N.H.L.; Hagras, S.M.; Elshaer, S. Ahmed glaucoma valve implantation with and without Ologen adjuvant in pediatric glaucoma. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2022, 26, 238.e1–238.e6. [Google Scholar] [CrossRef]
- Glandorf, K.; Lommatzsch, C.; Heinz, C.; Koch, J.M. Trabeculectomy with Ologen® implant and bevacizumab. Ophthalmologe 2020, 117, 445–451. [Google Scholar] [CrossRef]
- Kaushik, S.; Kataria, P.; Raj, S.; Pandav, S.S.; Ram, J. Safety and efficacy of a low-cost glaucoma drainage device for refractory childhood glaucoma. Br. J. Ophthalmol. 2017, 101, 1623–1627. [Google Scholar] [CrossRef]
- Rathi, S.G.; Seth, N.G.; Kaur, S.; Thattaruthody, F.; Kaushik, S.; Raj, S.; Pandav, S.S.; Ram, J. A prospective randomized controlled study of Aurolab aqueous drainage implant versus Ahmed glaucoma valve in refractory glaucoma: A pilot study. Indian J. Ophthalmol. 2018, 66, 1580–1585. [Google Scholar] [CrossRef]
- Wijesinghe, H.K.; Puthuran, G.V.; Gedde, S.J.; Pradhan, C.; Uduman, M.S.; Krishnadas, S.R.; Kannan, N.B.; Robin, A.L.; Palmberg, P. Incidence and Outcomes of Suprachoroidal Hemorrhage following Aurolab Aqueous Drainage Implant in Adult and Pediatric Glaucoma. J. Glaucoma 2021, 30, 497–501. [Google Scholar] [CrossRef]
- Jacobson, A.; Besirli, C.G.; Bohnsack, B.L. Outcomes of combined endoscopic vitrectomy and posteriorly placed glaucoma drainage devices in pediatric patients. BMC Ophthalmol. 2022, 22, 149. [Google Scholar] [CrossRef]
- Schlenker, M.B.; Durr, G.M.; Michaelov, E.; Ahmed, I.I.K. Intermediate Outcomes of a Novel Standalone Ab Externo SIBS Microshunt with Mitomycin C. Am. J. Ophthalmol. 2020, 215, 141–153. [Google Scholar] [CrossRef]
- Silber, S.; Colombo, A.; Banning, A.P.; Hauptmann, K.; Drzewiecki, J.; Grube, E.; Dudek, D.; Baim, D.S. Final 5-year results of the TAXUS II trial: A randomized study to assess the effectiveness of slow-and moderate-release polymer-based paclitaxel-eluting stents for de novo coronary artery lesions. Circulation 2009, 120, 1498–1504. [Google Scholar] [CrossRef] [Green Version]
- Pinchuk, L.; Wilson, G.J.; Barry, J.J.; Schoephoerster, R.T.; Parel, J.-M.; Kennedy, J.P. Medical applications of poly(styrene-block-isobutylene-block-styrene) (“SIBS”). Biomaterials 2008, 29, 448–460. [Google Scholar] [CrossRef]
- Acosta, A.C.; Espana, E.M.; Yamamoto, H.; Davis, S.; Pinchuk, L.; Weber, B.A.; Orozco, M.; Dubovy, S.; Fantes, F.; Parel, J.M. A newly designed glaucoma drainage implant made of poly(styrene-b-isobutylene-b-styrene): Biocompatibility and function in normal rabbit eyes. Arch Ophthalmol 2006, 124, 1742–1749. [Google Scholar] [CrossRef] [Green Version]
- Ruparelia, S.; Berco, E.; Lichtinger, A.; Shoham-Hazon, N. Multiple XEN Gel Stents for Refractory Pediatric Glaucoma. J. Pediatr. Ophthalmol. Strabismus 2022, 59, e11–e14. [Google Scholar] [CrossRef]
- D’Alessandro, E.; Guidotti, J.M.; Mansouri, K.; Mermoud, A. XEN-augmented Baerveldt: A New Surgical Technique for Refractory Glaucoma. J. Glaucoma 2017, 26, e90–e92. [Google Scholar] [CrossRef]
- Arad, T.; Hoffmann, E.M.; Prokosch-Willing, V.; Pfeiffer, N.; Grehn, F. XEN-augmented Baerveldt Implantation for Refractory Childhood Glaucoma: A Retrospective Case Series. J. Glaucoma 2019, 28, 1015–1018. [Google Scholar] [CrossRef]
- José, P.; Pinto, L.A.; Teixeira, F.J. XEN-augmented Baerveldt Failure: Three Different Revision Approaches for Pediatric Patients. J. Curr. Glaucoma Pract. 2021, 15, 96–98. [Google Scholar] [CrossRef]
- Chen, M.F.; Kim, C.H.; Coleman, A.L. Cyclodestructive procedures for refractory glaucoma. Cochrane Database Syst. Rev. 2019, 2019, Cd012223. [Google Scholar] [CrossRef]
- Al Owaifeer, A.M.; Almutairi, A.T.; Schargel, K. The outcomes of trans-scleral cyclophotocoagulation in pediatric glaucoma secondary to Sturge-Weber syndrome. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2022, 26, 78.e1–78.e5. [Google Scholar] [CrossRef]
- Fieß, A.; Shah, P.; Sii, F.; Godfrey, F.; Abbott, J.; Bowman, R.; Bauer, J.; Dithmar, S.; Philippin, H. Trabeculectomy or Transscleral Cyclophotocoagulation as Initial Treatment of Secondary Childhood Glaucoma in Northern Tanzania. J. Glaucoma 2017, 26, 657–660. [Google Scholar] [CrossRef]
- Elhefney, E.M.; Mokbel, T.H.; Hagras, S.M.; AlNagdy, A.A.; Ellayeh, A.A.; Mohsen, T.A.; Gaafar, W.M. Micropulsed diode laser cyclophotocoagulation in recurrent pediatric glaucoma. Eur. J. Ophthalmol. 2020, 30, 1149–1155. [Google Scholar] [CrossRef]
- Cantor, A.J.; Wang, J.; Li, S.; Neely, D.E.; Plager, D.A. Long-term efficacy of endoscopic cyclophotocoagulation in the management of glaucoma following cataract surgery in children. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2018, 22, 188–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feusier, M.; Roy, S.; Mermoud, A. Deep sclerectomy combined with trabeculectomy in pediatric glaucoma. Ophthalmology 2009, 116, 30–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bayoumi, N.H. Deep sclerectomy in pediatric glaucoma filtering surgery. Eye 2012, 26, 1548–1553. [Google Scholar] [CrossRef] [PubMed]
- Al-Obeidan, S.A.; Osman Eel, D.; Dewedar, A.S.; Kestelyn, P.; Mousa, A. Efficacy and safety of deep sclerectomy in childhood glaucoma in Saudi Arabia. Acta Ophthalmol. 2014, 92, 65–70. [Google Scholar] [CrossRef]
- Al-Shahwan, S.; Al-Torbak, A.A.; Turkmani, S.; Al-Omran, M.; Al-Jadaan, I.; Edward, D.P. Side-effect profile of brimonidine tartrate in children. Ophthalmology 2005, 112, 2143. [Google Scholar] [CrossRef]
- Quaranta, L.; Biagioli, E.; Riva, I.; Galli, F.; Poli, D.; Rulli, E.; Katsanos, A.; Longo, A.; Uva, M.G.; Torri, V.; et al. The Glaucoma Italian Pediatric Study (GIPSy): 1-Year Results. J. Glaucoma 2017, 26, 987–994. [Google Scholar] [CrossRef]
- Enyedi, L.B.; Freedman, S.F. Latanoprost for the treatment of pediatric glaucoma. Surv. Ophthalmol. 2002, 47 (Suppl. S1), S129–S132. [Google Scholar] [CrossRef]
- Enyedi, L.B.; Freedman, S.F.; Buckley, E.G. The effectiveness of latanoprost for the treatment of pediatric glaucoma. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 1999, 3, 33–39. [Google Scholar] [CrossRef]
- Dixon, E.R.; Landry, T.; Venkataraman, S.; Gustafson, N.; Salem, C.; Bradfield, Y.; Aljasim, L.A.; Feldman, R. A 3-month safety and efficacy study of travoprost 0.004% ophthalmic solution compared with timolol in pediatric patients with glaucoma or ocular hypertension. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2017, 21, 370–374.e1. [Google Scholar] [CrossRef] [Green Version]
- Sit, A.J.; Gupta, D.; Kazemi, A.; McKee, H.; Challa, P.; Liu, K.C.; Lopez, J.; Kopczynski, C.; Heah, T. Netarsudil Improves Trabecular Outflow Facility in Patients with Primary Open Angle Glaucoma or Ocular Hypertension: A Phase 2 Study. Am. J. Ophthalmol. 2021, 226, 262–269. [Google Scholar] [CrossRef]
- Araie, M.; Sugiyama, K.; Aso, K.; Kanemoto, K.; Kothapalli, K.; Kopczynski, C.; Senchyna, M.; Hollander, D.A. Phase 2 Randomized Clinical Study of Netarsudil Ophthalmic Solution in Japanese Patients with Primary Open-Angle Glaucoma or Ocular Hypertension. Adv. Ther. 2021, 38, 1757–1775. [Google Scholar] [CrossRef] [PubMed]
- Khouri, A.S.; Serle, J.B.; Bacharach, J.; Usner, D.W.; Lewis, R.A.; Braswell, P.; Kopczynski, C.C.; Heah, T. Once-Daily Netarsudil versus Twice-Daily Timolol in Patients with Elevated Intraocular Pressure: The Randomized Phase 3 ROCKET-4 Study. Am. J. Ophthalmol. 2019, 204, 97–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rapuano, P.B.; Levin, A.V.; Price, J.M.; Myers, J.S.; Lee, D.; Shukla, A.G. Early Experience with Netarsudil in Pediatric Patients: A Retrospective Case Series. Ophthalmol. Glaucoma 2021, 4, 232–234. [Google Scholar] [CrossRef]
- Sacchi, M.; Lizzio, R.A.U.; Villani, E.; Monsellato, G.; Lucentini, S.; Cremonesi, E.; Luccarelli, S.; Serafino, M.; Nucci, P. Medical management of pediatric glaucoma: Lessons learned from randomized clinical trials. Graefes Arch Clin. Exp. Ophthalmol. 2020, 258, 1579–1586. [Google Scholar] [CrossRef]
- Al-Dawood, A.; Ahmad, K.; Al-Salman, S.; Al Hussan, F.; Al Houssien, A.; Al-Shahwan, S.; Khandekar, R.; Edward, D.P. Barriers and adherence to glaucoma medication in a paediatric glaucoma population: A cross-sectional survey in central Saudi Arabia. Eur. J. Ophthalmol. 2022, 32, 3451–3460. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.B.; Neustein, R.F.; Jones, S.K.; Robin, A.L.; Muir, K.W. Pediatric glaucoma medical therapy: Who more accurately reports medication adherence, the caregiver or the child? Clin. Ophthalmol. 2015, 9, 2209–2212. [Google Scholar] [CrossRef] [Green Version]
- Kaur, S.; Dhiman, I.; Kaushik, S.; Raj, S.; Pandav, S.S. Outcome of Ocular Steroid Hypertensive Response in Children. J. Glaucoma 2016, 25, 343–347. [Google Scholar] [CrossRef]
- Ozturk, T.; Durmaz Engin, C.; Koksaldi, S.; Arikan, G. The short-term effects of intranasal steroids on intraocular pressure in pediatric population. Int. Ophthalmol. 2022, 42, 3821–3827. [Google Scholar] [CrossRef]
- Bello, N.R.; LaMattina, K.C.; Minor, J.M.; Utz, V.M.; Dong, K.; Levin, A.V. The risk of uveitis due to prostaglandin analogs in pediatric glaucoma. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2022, 26, 126.e1–126.e5. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| First Author (Year) | Glaucoma Type | Study Design | Surgical Treatments | Sample Size | Main Results |
|---|---|---|---|---|---|
| Lawrence et al. (2012) [103] | PG | Retrospective, comparative | Group 1: Trabeculectomy Group 2: Combined trabeculotomy-trabeculectomy | 40 eyes in 33 patients. Group 1: 17 eyes Group 2: 23 eyes | Group 2 had greater long-term success. |
| Eldaly et al. (2014) [104] | PCG | Prospective, comparative | Group 1: Pneumatic trabecular bypass (PTB) Group 2: Conventional trabeculotomy | 42 eyes of 42 patients. Group 1: 17 eyes Group 2: 25 eyes | PTB had a greater total cumulative chance for success than group 2 (88.2% vs. 56% respectively). |
| Temkar et al. (2015) [105] | PCG | Prospective, randomized | Group 1: Illuminated microcatheter-assisted circumferential trabeculotomy Group 2: Combined mitomycin C-augmented trabeculotomy-trabeculectomy | 60 eyes of 30 patients with bilateral PCG aged ≤ 2 years. Group 1: 30 eyes Group 2: 30 eyes | The two groups achieved comparable surgical outcomes. |
| Lim et al. (2015) [106] | PG | Retrospective, comparative | Group 1: 360-degree circumferential trabeculotomy Group 2: Traditional trabeculotomy (<360 degrees or partial) | 91 eyes of 66 patients. Group 1: 14 eyes Group 2: 77 eyes | Group 1 had a higher surgical success rate than group 2 at 1-year (85.71% vs. 58.44%, respectively). |
| Shakrawal et al. (2017) [107] | PCG | Prospective, randomized | Group 1: Illuminated-Microcatheter Circumferential Trabeculotomy Group 2: Conventional partial trabeculotomy | 40 eyes of 31 patients aged ≤ 2 years. Group 1: 20 eyes Group 2: 20 eyes | Group 1 performed better than group 2 at 1 year follow-up. |
| Abdelrahman et al. (2018) [108] | Refractory glaucoma | Prospective, comparative | Group 1: Micropulse cyclophotocoagulation Group 2: Transscleral continuous wave cyclophotocoagulation | 45 eyes of 36 patients. Group 1: 17 eyes Group 2: 28 eyes | Group 1 had a higher success rate was higher (71% vs. 46% in group 2) although the difference was not significant (p = 0.1). Group 1 had lower rate of complications, pain, and inflammation. |
| El Sayed et al. (2018) [109] | PCG | Retrospective, comparative | Group 1: Microcatheter-assisted trabeculotomy Group 2: 2-site circumferential trabeculotomy using the rigid probe trabeculotome | 92 eyes of 92 patients. Group 1: 33 eyes Group 2: 59 eyes | The two groups had comparable results. However, the added cost of the microcatheter in group 1 should be considered. |
| Elwehidy (2019) [110] | Refractory Glaucoma with failed AGV | Prospective, randomized | Group 1: Ahmed glaucoma valve revision Group 2: Visco-trabeculotomy (VT) | 41 eyes of 41 patients. Group 1: 19 eyes Group 2: 22 eyes | VT had a higher success rate and a decrease in IOP-lowering medication use. |
| Elhofi (2020) [111] | PCG | Retrospective, comparative | Group 1: Non-penetrating deep sclerectomy Group 2: Trabeculectomy | 80 eyes of 80 patients aged < 3 years. Group 1: 40 eyes Group 2: 40 eyes | Group 1 had fewer postoperative complications with a comparative postoperative IOP reduction and overall success rates. |
| Puthuran (2021) [112] | Refractory glaucoma | Retrospective, comparative | Group 1: Aurolab aqueous drainage implant (AADI) placed in the superotemporal quadrant Group 2: AADI placed in the inferonasal quadrant | 144 eyes of 144 patients. Group 1: 96 eyes Group 2: 48 eyes | Group 1 had better IOP-related outcomes and is a safer surgical option in pediatric eyes. |
| Qiao (2021) [113] | Uncontrolled JOAG | Retrospective, comparative | Group 1: Gonioscopy-assisted transluminal trabeculotomy (GATT) Group 2: Kahook dual blade excisional goniotomy | 46 eyes of 43 patients. Group 1: 36 eyes Group 2: 10 eyes | GATT was preferred in medical uncontrolled surgery-naïve JOAG eyes. |
| Elwehidy (2022) [114] | PCG | Prospective, randomized | Group 1: Visco-circumferential-suture-trabeculotomy (VCST) Group 2: Rigid probe visco-trabeculotomy | 84 eyes of 49 patients Group 1: 40 eyes Group 2: 44 eyes | Group 1 provided a marginal advantage over group 2. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shen, R.; Li, V.S.W.; Wong, M.O.M.; Chan, P.P.M. Pediatric Glaucoma—From Screening, Early Detection to Management. Children 2023, 10, 181. https://doi.org/10.3390/children10020181
Shen R, Li VSW, Wong MOM, Chan PPM. Pediatric Glaucoma—From Screening, Early Detection to Management. Children. 2023; 10(2):181. https://doi.org/10.3390/children10020181
Chicago/Turabian StyleShen, Ruyue, Venice S. W. Li, Mandy O. M. Wong, and Poemen P. M. Chan. 2023. "Pediatric Glaucoma—From Screening, Early Detection to Management" Children 10, no. 2: 181. https://doi.org/10.3390/children10020181