

Clinical Congenital Anophthalmos and Microphthalmos—Experiences of Patients and Their Parents after More than 10 Years of Treatment
 and
and
Abstract
:1. Introduction
2. Materials and Methods
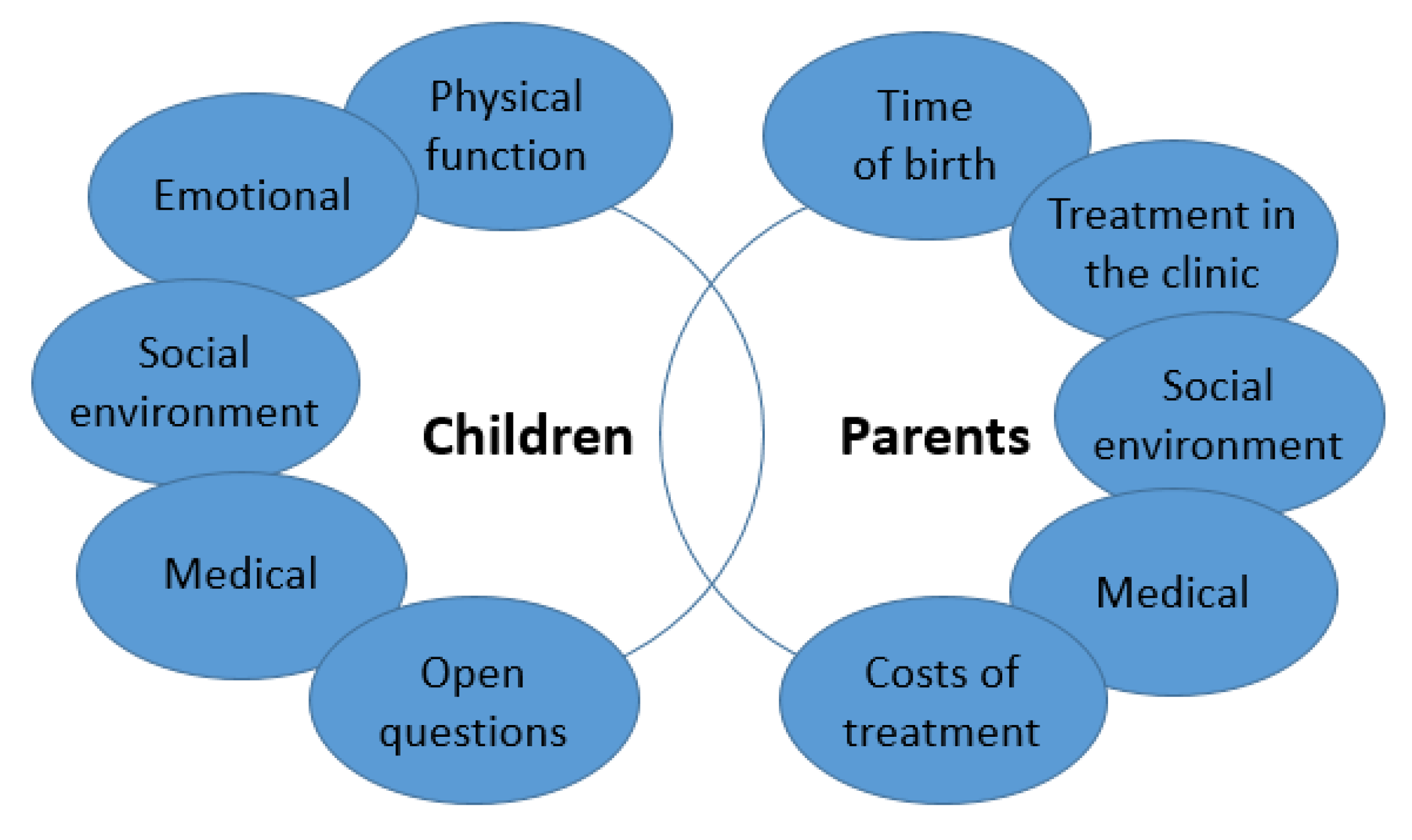
2.1. Development of an Anophthalmic/Microphthalmic Questionnaire for Parents and Patients
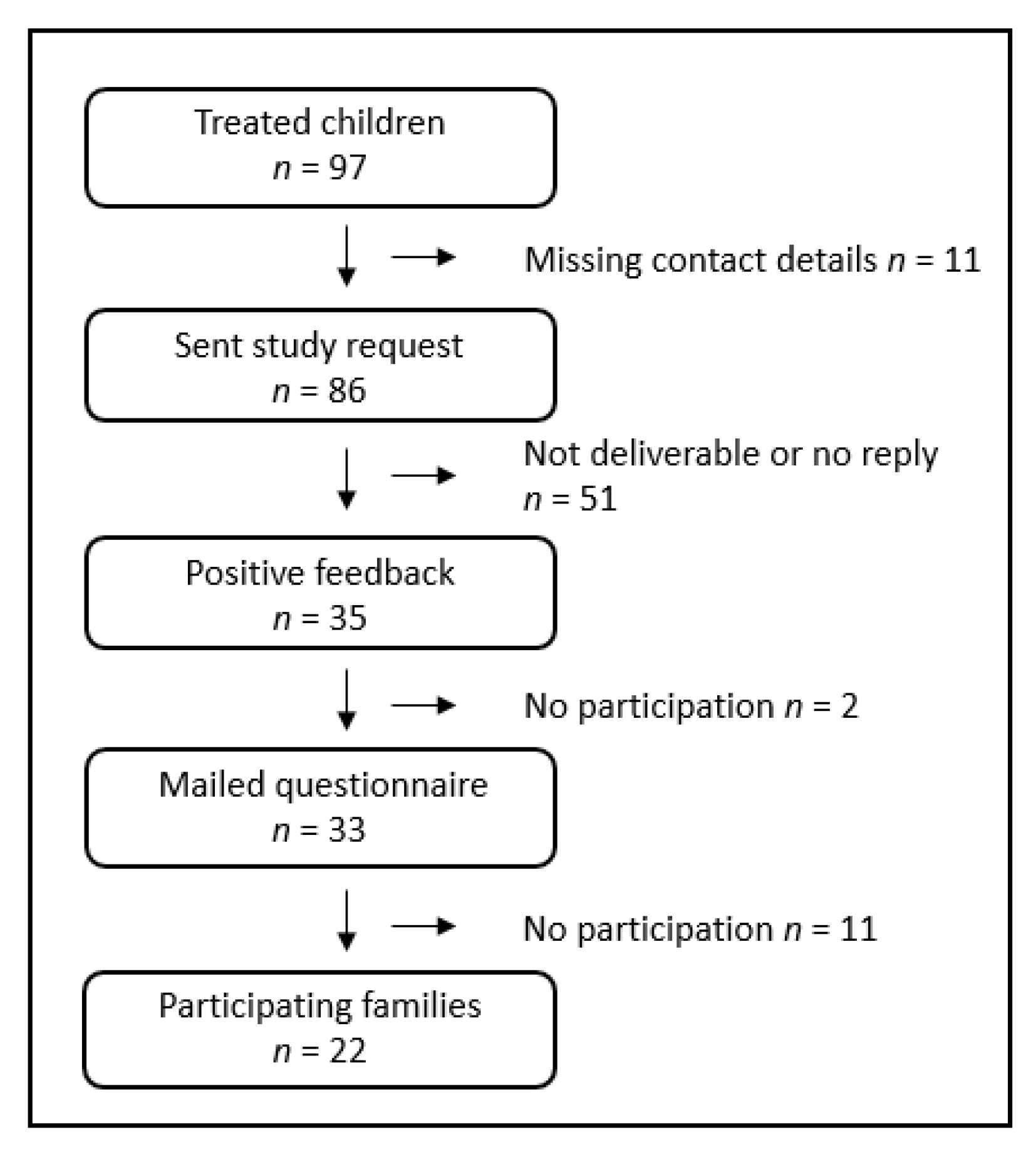
2.2. Study Design and Study Population
3. Results
3.1. Study Population
3.2. Unilateral Clinical Anophthalmos and Blind Microphthalmos with Sighted Eye
3.3. Bilateral Clinical Anophthalmos
3.4. Parental Statements of Patients with Unilateral and Bilateral Clinical Anophthalmos or Blind Microphthalmos
3.4.1. Around the Time of Birth
3.4.2. Treatment at the University Eye Hospital Rostock
3.4.3. Costs of Surgical and Conservative Treatments
3.4.4. Social Environment of Patients
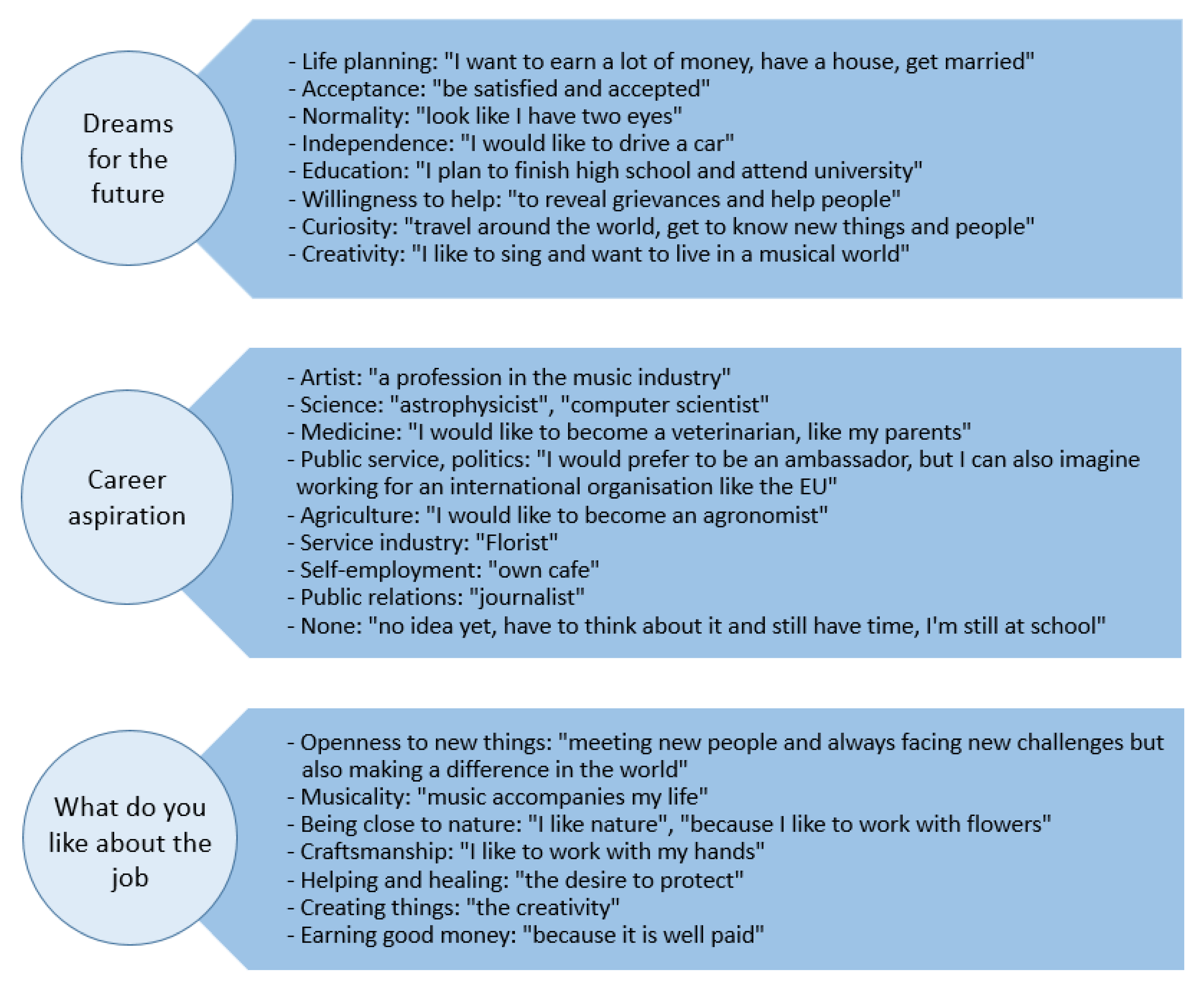
3.5. Open Question Section of Unilateral and Bilateral Patients with Clinical Anophthalmos or Blind Microphthalmos
4. Discussion
4.1. Prenatal Diagnosis, Birth and Initial Treatment in the Eye Clinic Rostock
4.2. Social Environment and Emotional Aspects of Life with Ocular Prosthesis in Young Patients with Congenital Clinical Anophthalmos or Blind Microphthalmos
4.3. Factors That Positively and Negatively Influence the Well-Being of Anophthalmic Patients
4.4. Medical Aspects of Ocular Protheses
4.5. Self-Perception and Perception by Others
4.6. Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Verma, A.S.; Fitzpatrick, D.R. Anophthalmia and microphthalmia. Orphanet J. Rare Dis. 2007, 2, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Handler, L.F.; Heher, K.L.; Katowitz, J.A. Congenital and acquired anophthalmia. Curr. Opin. Ophthalmol. 1994, 5, 89. [Google Scholar] [CrossRef]
- Schittkowski, M.P.; Gundlach, K.K.H.; Guthoff, R.F. Kongenitaler klinischer Anophthalmus und funktionsloser Mikrophthalmus. Vergleichende Betrachtungen zu unterschiedlichen Therapiekonzepten. Ophthalmologe 2003, 100, 507–517. [Google Scholar] [CrossRef] [PubMed]
- Duke-Elder, S. (Ed.) System of Ophthalmology Volume III Normal And Abnormal Development Part 2 Congenital Deformities: Part 2. In Academic Medicine; LWW: Philadelphia, PA, USA, 1963; pp. 416–428. [Google Scholar]
- Quaranta-Leoni, F.M. Congenital anophthalmia: Current concepts in management. Curr. Opin. Ophthalmol. 2011, 22, 380–384. [Google Scholar] [CrossRef] [PubMed]
- Schittkowski, M.P.; Guthoff, R.F. Systemic and ophthalmological anomalies in congenital anophthalmic or microphthalmic patients. Br. J. Ophthalmol. 2010, 94, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Ragge, N.K.; Subak-Sharpe, I.D.; Collin, J.R.O. A practical guide to the management of anophthalmia and microphthalmia. Eye 2007, 21, 1290–1300. [Google Scholar] [CrossRef] [Green Version]
- Gerth-Kahlert, C.; Williamson, K.; Ansari, M.; Rainger, J.K.; Hingst, V.; Zimmermann, T.; Tech, S.; Guthoff, R.F.; van Heyningen, V.; Fitzpatrick, D.R. Clinical and mutation analysis of 51 probands with anophthalmia and/or severe microphthalmia from a single center. Mol. Genet. Genom. Med. 2013, 1, 15–31. [Google Scholar] [CrossRef]
- Ohuchi, H.; Sato, K.; Habuta, M.; Fujita, H.; Bando, T. Congenital eye anomalies: More mosaic than thought? Congenit. Anom. 2019, 59, 56–73. [Google Scholar] [CrossRef]
- Roos, L.; Jensen, H.; Grønskov, K.; Holst, R.; Tümer, Z. Congenital Microphthalmia, Anophthalmia and Coloboma among Live Births in Denmark. Ophthalmic Epidemiol. 2016, 23, 324–330. [Google Scholar] [CrossRef]
- Stallings, E.B.; Isenburg, J.L.; Mai, C.T.; Liberman, R.F.; Moore, C.A.; Canfield, M.A.; Salemi, J.L.; Kirby, R.S.; Short, T.D.; Nembhard, W.N.; et al. Population-based birth defects data in the United States, 2011–2015: A focus on eye and ear defects. Birth Defects Res. 2018, 110, 1478–1486. [Google Scholar] [CrossRef]
- Changal, N.; Khandekar, R.B. Eye Conformers as Socket Expanders in Children: Experience at a Tertiary Eye Hospital in Central Saudi Arabia. Cureus 2021, 13, e13465. [Google Scholar] [CrossRef] [PubMed]
- Parker, S.E.; Mai, C.T.; Canfield, M.A.; Rickard, R.; Wang, Y.; Meyer, R.E.; Anderson, P.; Mason, C.A.; Collins, J.S.; Kirby, R.S.; et al. Updated National Birth Prevalence estimates for selected birth defects in the United States, 2004–2006. Birth Defects Res. A Clin. Mol. Teratol. 2010, 88, 1008–1016. [Google Scholar] [CrossRef] [PubMed]
- Bermejo, E.; Martínez-Frías, M.L. Congenital eye malformations: Clinical-epidemiological analysis of 1,124,654 consecutive births in Spain. Am. J. Med. Genet. 1998, 75, 497–504. [Google Scholar] [CrossRef]
- Chambers, T.M.; Agopian, A.J.; Lewis, R.A.; Langlois, P.H.; Danysh, H.E.; Weber, K.A.; Shaw, G.M.; Mitchell, L.E.; Lupo, P.J. Epidemiology of anophthalmia and microphthalmia: Prevalence and patterns in Texas, 1999–2009. Am. J. Med. Genet. A 2018, 176, 1810–1818. [Google Scholar] [CrossRef]
- Forrester, M.B.; Merz, R.D. Descriptive epidemiology of anophthalmia and microphthalmia, Hawaii, 1986–2001. Birth Defects Res. A Clin. Mol. Teratol. 2006, 76, 187–192. [Google Scholar] [CrossRef]
- Ferreira, C.R. The burden of rare diseases. Am. J. Med. Genet. A 2019, 179, 885–892. [Google Scholar] [CrossRef]
- Gundlach, K.K.H.; Guthoff, R.F.; Hingst, V.H.M.; Schittkowski, M.P.; Bier, U.C. Expansion of the socket and orbit for congenital clinical anophthalmia. Plast. Reconstr. Surg. 2005, 116, 1214–1222. [Google Scholar] [CrossRef]
- Schittkowski, M.P.; Guthoff, R.F. Results of lacrimal assessment in patients with congenital clinical anophthalmos or blind microphthalmos. Br. J. Ophthalmol. 2007, 91, 1624–1626. [Google Scholar] [CrossRef] [Green Version]
- Schittkowski, M.P. Therapiemöglichkeiten bei funktionslosem Mikrophthalmus und klinischem Anophthalmus. Ophthalmologe 2012, 109, 1122–1126. [Google Scholar] [CrossRef]
- Casslén, B.; Jugård, Y.; Taha Najim, R.; Odersjö, M.; Topa, A.; Andersson Grönlund, M. Visual function and quality of life in children and adolescents with anophthalmia and microphthalmia treated with ocular prosthesis. Acta Ophthalmol. 2020, 98, 662–670. [Google Scholar] [CrossRef]
- Dahlmann-Noor, A.; Tailor, V.; Abou-Rayyah, Y.; Adams, G.; Brookes, J.; Khaw, P.T.; Bunce, C.; Papadopoulos, M. Functional vision and quality of life in children with microphthalmia/anophthalmia/coloboma-a cross-sectional study. J. AAPOS 2018, 22, 281–285.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolleck, A.; Sauter, A. Aktueller Stand und Entwicklungen der Pränataldiagnostik; Büro für Technikfolgen-Abschätzung beim Deutschen Bundestag (TAB): Berlin, Germany, 2019; Volume 2019. [Google Scholar]
- Ondeck, C.L.; Pretorius, D.; McCaulley, J.; Kinori, M.; Maloney, T.; Hull, A.; Robbins, S.L. Ultrasonographic prenatal imaging of fetal ocular and orbital abnormalities. Surv. Ophthalmol. 2018, 63, 745–753. [Google Scholar] [CrossRef] [PubMed]
- Searle, A.; Shetty, P.; Melov, S.J.; Alahakoon, T.I. Prenatal diagnosis and implications of microphthalmia and anophthalmia with a review of current ultrasound guidelines: Two case reports. J. Med. Case Rep. 2018, 12, 250. [Google Scholar] [CrossRef] [PubMed]
- Varejão, A.M.; Pestana, I. Prenatal diagnosis of isolated bilateral anophthalmia. BMJ Case Rep. 2021, 14, e244684. [Google Scholar] [CrossRef] [PubMed]
- Makrakis, L.R.; Araújo, C.B.; de Macedo, A.P.; Silva-Lovato, C.H. The Impact of an Ocular Prosthesis on the Quality of Life, Perceived Stress, and Clinical Adaptation of Anophthalmic Patients: A Clinical and Longitudinal Trial. J. Prosthodont. 2021, 30, 394–400. [Google Scholar] [CrossRef]
- Wang, K.J.; Li, S.S.; Wang, H.Y. Psychological symptoms in anophthalmic patients wearing ocular prosthesis and related factors. Medicine 2020, 99, e21338. [Google Scholar] [CrossRef]
- Avery, R.A.; Hardy, K.K. Vision specific quality of life in children with optic pathway gliomas. J. Neurooncol. 2014, 116, 341–347. [Google Scholar] [CrossRef]
- Chak, M.; Rahi, J.S. The health-related quality of life of children with congenital cataract: Findings of the British Congenital Cataract Study. Br. J. Ophthalmol. 2007, 91, 922–926. [Google Scholar] [CrossRef] [Green Version]
- Castañeda, Y.S.; Cheng-Patel, C.S.; Leske, D.A.; Wernimont, S.M.; Hatt, S.R.; Liebermann, L.; Birch, E.E.; Holmes, J.M. Quality of life and functional vision concerns of children with cataracts and their parents. Eye 2016, 30, 1251–1259. [Google Scholar] [CrossRef]
- Tailor, V.K.; Abou-Rayyah, Y.; Brookes, J.; Khaw, P.T.; Papadopoulos, M.; Adams, G.G.W.; Bunce, C.; Dahlmann-Noor, A. Quality of life and functional vision in children treated for cataract-a cross-sectional study. Eye 2017, 31, 856–864. [Google Scholar] [CrossRef]
- Dahlmann-Noor, A.; Tailor, V.; Bunce, C.; Abou-Rayyah, Y.; Adams, G.; Brookes, J.; Khaw, P.T.; Papadopoulos, M. Quality of Life and Functional Vision in Children with Glaucoma. Ophthalmology 2017, 124, 1048–1055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goiato, M.C.; dos Santos, D.M.; Bannwart, L.C.; Moreno, A.; Pesqueira, A.A.; Haddad, M.F.; dos Santos, E.G. Psychosocial impact on anophthalmic patients wearing ocular prosthesis. Int. J. Oral Maxillofac. Surg. 2013, 42, 113–119. [Google Scholar] [CrossRef]
- Pine, K.; Sloan, B.; Stewart, J.; Jacobs, R.J. Concerns of anophthalmic patients wearing artificial eyes. Clin. Exp. Ophthalmol. 2011, 39, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Rokohl, A.C.; Koch, K.R.; Trester, M.; Trester, W.; Pine, K.R.; Heindl, L.M. Concerns of Anophthalmic Patients Wearing Cryolite Glass Prosthetic Eyes. Ophthalmic Plast. Reconstr. Surg. 2018, 34, 369–374. [Google Scholar] [CrossRef]
- Ruiters, S.; Jong, S.; de Mombaerts, I. Measuring quality of care and life in patients with an ocular prosthesis. Graefes Arch. Clin. Exp. Ophthalmol. 2021, 259, 2017–2025. [Google Scholar] [CrossRef]
- Ahn, J.M.; Lee, S.Y.; Yoon, J.S. Health-related quality of life and emotional status of anophthalmic patients in Korea. Am. J. Ophthalmol. 2010, 149, 1005–1011.e1. [Google Scholar] [CrossRef]
- Goiato, M.C.; Caxias, F.P.; de dos Santos, D.M. Quality of life living with ocular prosthesis. Expert Rev. Ophthalmol. 2018, 13, 187–189. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Zhang, H.; Chen, W.; Li, G. The psychosocial benefits of secondary hydroxyapatite orbital implant insertion and prosthesis wearing for patients with anophthalmia. Ophthalmic Plast. Reconstr. Surg. 2012, 28, 324–327. [Google Scholar] [CrossRef]
- Song, J.-S.; Oh, J.; Baek, S.H. A survey of satisfaction in anophthalmic patients wearing ocular prosthesis. Graefes Arch. Clin. Exp. Ophthalmol. 2006, 244, 330–335. [Google Scholar] [CrossRef]
- Rasmussen, M.L.R. The eye amputated—Consequences of eye amputation with emphasis on clinical aspects, phantom eye syndrome and quality of life. Acta Ophthalmol. 2010, 88, 1–26. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Unilateral Congenital Clinical Anophthalmos | Bilateral Congenital Clinical Anophthalmos | Unilateral Blind Microphthalmos | Total (%) | |
|---|---|---|---|---|
| Male | 7 | 2 | 3 | 12 (54) |
| Female | 7 | 2 | 1 | 10 (46) |
| Total | 14 | 4 | 4 | 22 (100) |
| Physical Function | Yes | To Some Extent | No |
|---|---|---|---|
| I don’t feel restricted by seeing with just one eye | 11 | 3 | 1 |
| When I look in the mirror, I don’t see a big difference between the prothesis and my eye | 4 | 3 | 7 |
| I see everything I need in the booklet and on the blackboard at school/at the training place | 11 | 2 | 2 |
| Emotional | Yes | To Some Extent | No |
| The fact that I can only see with one eye makes me: | |||
| Sad | 2 | 3 | 10 |
| Angry | 1 | 2 | 12 |
| Worried | 3 | 1 | 11 |
| Afraid or anxious | 1 | 1 | 13 |
| I got used to it | 12 | 3 | 0 |
| I am afraid that my only eyesight could fade in the future | 7 | 4 | 4 |
| Social Environment | Yes | To Some Extent | No |
| I feel/felt accepted as I am | 11 | 3 | 0 |
| I’m often asked about my appearance | 2 | 7 | 5 |
| I am playing/played just like other seeing children | 10 | 3 | 1 |
| I’m afraid of making new contacts because of my blindness | 1 | 2 | 12 |
| Other people don’t even notice the malformation of the eye | 2 | 7 | 6 |
| The malformation of the eye is a frequent topic of conversation | 1 | 8 | 6 |
| I have contact with other children who also wear one or two eye prostheses | 1 | 1 | 13 |
| Medical | Yes | To Some Extent | No |
| I have to see an ophthalmologist more than twice a year | 2 | 0 | 13 |
| I am afraid of visiting an ophthalmologist or ocularist | 1 | 1 | 13 |
| The side with the prosthesis often hurts | 0 | 0 | 0 |
| The side with the prosthesis sometimes hurts | 6 | 0 | 0 |
| The side with the prosthesis never hurts | 8 | 0 | 0 |
| The position of the prostheses must be corrected more than once a year | 2 | 0 | 10 |
| I have other diseases | 5 | 0 | 9 |
| Physical Function | Yes | To Some Extent | No |
|---|---|---|---|
| My blindness restricts me so much that I need personal help | 3 | 0 | 1 |
| In the school for the blind I am/was taught all skills to be able to act independently | 1 | 2 | 1 |
| Since I’m blind, I’m only in familiar places | 2 | 0 | 2 |
| Emotional | Yes | To Some Extent | No |
| The fact that I can’t see makes me: | |||
| Sad | 1 | 0 | 0 |
| Angry | 0 | 0 | 0 |
| Worries | 1 | 0 | 0 |
| Afraid or anxious | 1 | 0 | 0 |
| I got used to it | 3 | 1 | 0 |
| I am afraid that as a blind person I will not be able to cope alone in the future | 1 | 2 | 1 |
| Social Environment | Yes | To Some Extent | No |
| I feel/felt accepted as I am | 4 | 0 | 0 |
| I’m afraid of making new contacts because of my blindness | 0 | 0 | 4 |
| I’m often asked about my appearance. | 0 | 2 | 2 |
| Other people don’t even notice the malformation of the eyes | 1 | 2 | 1 |
| The malformation of the eyes is a frequent topic of conversation | 1 | 1 | 2 |
| I have contact with other children who also wear one or two eye prostheses | 2 | 1 | 1 |
| Medical | Yes | To Some Extent | No |
| I have to see an ophthalmologist more than twice a year | 1 | 1 | 2 |
| I am afraid of visiting an ophthalmologist or ocularist | 0 | 0 | 4 |
| The prostheses often hurt | 0 | 0 | 0 |
| The prostheses sometimes hurt | 0 | 0 | 0 |
| The prostheses never hurt | 4 | 0 | 0 |
| The position of the prosthesis must be corrected more than once a year | 2 | 0 | 2 |
| I have other diseases | 1 | 1 | 2 |
| At the Time of Your Child’s Birth | Yes | To Some Extent | No | |
|---|---|---|---|---|
| Already during the ultrasound examination during pregnancy, a possible physical change or malformation was detected in our child | Uni | 0 | 1 | 14 |
| Bi | 2 | 0 | 4 | |
| We were affected when we first saw our child at birth. | Uni | 8 | 3 | 4 |
| Bi | 3 | 2 | 1 | |
| The gynaecologist and the paediatrician were able to explain the change to us. | Uni | 3 | 4 | 8 |
| Bi | 1 | 3 | 2 | |
| We had to inform ourselves through books and the internet to understand what change it is. | Uni | 8 | 5 | 2 |
| Bi | 1 | 3 | 0 | |
| Treatment at the University Eye Hospital | Yes | To Some Extent | No | |
| The gynaecologist and the paediatrician referred us to the Eye Clinic Rostock | Uni | 2 | 2 | 10 |
| Bi | 4 | 0 | 2 | |
| Only by own research we got to the Eye Clinic Rostock | Uni | 9 | 3 | 3 |
| Bi | 2 | 0 | 3 | |
| The team of doctors, nurses and ocularists answered our questions, fears and worries | Uni | 12 | 1 | 2 |
| Bi | 6 | 0 | 0 | |
| We were able to see the success of the operation after the first operation | Uni | 11 | 2 | 2 |
| Bi | 3 | 3 | 0 | |
| Costs of Treatments | Yes | To Some Extent | No | |
| Our health insurance company of the statutory health insurance or private insurance company paid all costs such as travel, stays, operations, in full | Uni | 7 | 5 | 3 |
| Bi | 5 | 1 | 0 | |
| Our own costs accounted for more than 35% of the treatment costs | Uni | 3 | 0 | 12 |
| Bi | 0 | 2 | 4 | |
| There is concern about new costs in the course of further treatments | Uni | 2 | 3 | 10 |
| Bi | 2 | 0 | 4 | |
| Social Environment | Yes | To Some Extent | No | |
| Our child gets/got along well in kindergarten | Uni | 13 | 0 | 0 |
| Bi | 3 | 2 | 1 | |
| Our child gets/got along well in the school (for the blind) | Uni | 8 | 2 | 2 |
| Bi | 3 | 2 | 1 | |
| Our child plays/played just like other children | Uni | 7 | 2 | 6 |
| Bi | 2 | 1 | 3 | |
| Our child is afraid to meet new children because of its own special appearance | Uni | 0 | 5 | 9 |
| Bi | 0 | 0 | 5 | |
| We are approached as parents about the appearance of our child. | Uni | 4 | 7 | 3 |
| Bi | 2 | 2 | 1 | |
| At first glance, others do not even notice the malformation. | Uni | 3 | 7 | 5 |
| Bi | 3 | 1 | 2 | |
| The malformation is a topic of conversation between us, the parents | Uni | 6 | 5 | 3 |
| Bi | 1 | 1 | 3 | |
| The malformation is a topic of conversation between us, the parents and our child | Uni | 6 | 6 | 2 |
| Bi | 3 | 0 | 2 | |
| The malformation is a topic of conversation between us, the parents and other parents | Uni | 2 | 4 | 9 |
| Bi | 2 | 2 | 2 | |
| The fact that our child can only see with one eye/is blind does not impact our social environment | Uni | 11 | 2 | 2 |
| Bi | 3 | 2 | 1 | |
| Our child has career plans | Uni | 8 | 0 | 1 |
| Bi | 1 | 1 | 4 | |
| We are in contact with other families and children in the same situation through a self-help group | Uni | 0 | 1 | 13 |
| Bi | 1 | 0 | 5 | |
| We are in private contact with other families and children who are in the same situation | Uni | 3 | 1 | 11 |
| Bi | 3 | 1 | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frech, S.; Schulze Schwering, M.; Schittkowski, M.P.; Guthoff, R.F. Clinical Congenital Anophthalmos and Microphthalmos—Experiences of Patients and Their Parents after More than 10 Years of Treatment. Children 2023, 10, 34. https://doi.org/10.3390/children10010034
Frech S, Schulze Schwering M, Schittkowski MP, Guthoff RF. Clinical Congenital Anophthalmos and Microphthalmos—Experiences of Patients and Their Parents after More than 10 Years of Treatment. Children. 2023; 10(1):34. https://doi.org/10.3390/children10010034
Chicago/Turabian StyleFrech, Stefanie, Markus Schulze Schwering, Michael P. Schittkowski, and Rudolf F. Guthoff. 2023. "Clinical Congenital Anophthalmos and Microphthalmos—Experiences of Patients and Their Parents after More than 10 Years of Treatment" Children 10, no. 1: 34. https://doi.org/10.3390/children10010034