
Associations between Chronic Pain and Attention-Deficit Hyperactivity Disorder (ADHD) in Youth: A Scoping Review

Abstract
:1. Introduction
Chronic Pain and ADHD
2. Aim 1: Scoping Review of the Literature
2.1. Methods
2.1.1. Eligibility Criteria
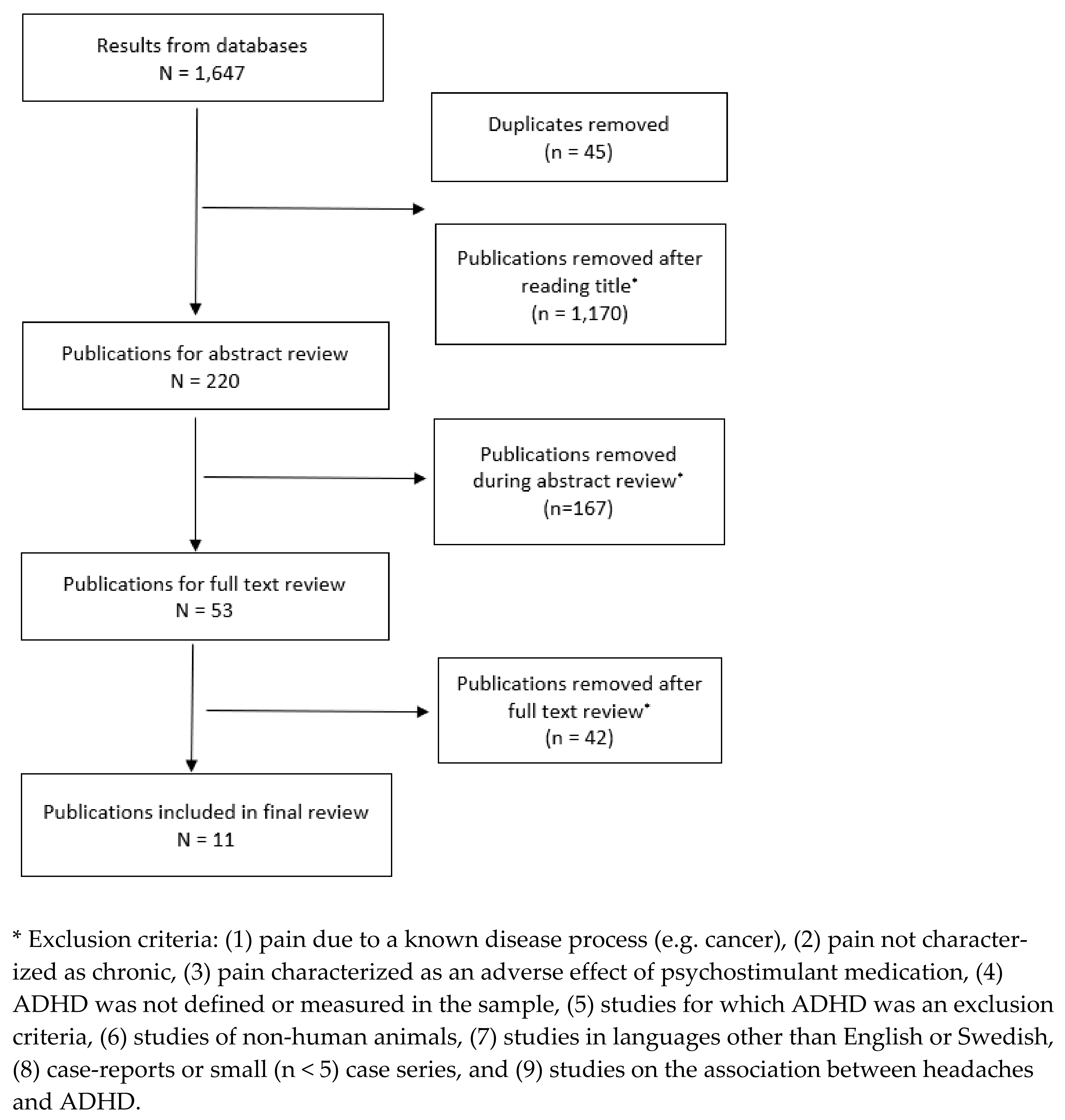
2.1.2. Study Selection
2.2. Results
2.2.1. Characteristics of Included Studies
2.2.2. ADHD Prevalence in Samples of Youth with Chronic Pain
2.2.3. Chronic Pain Prevalence in Samples of Youth with ADHD
2.2.4. Additional Relevant Studies of Pain Symptomatology and ADHD That Did Not Meet Identified Criteria for Standard Definitions of Chronic Pain
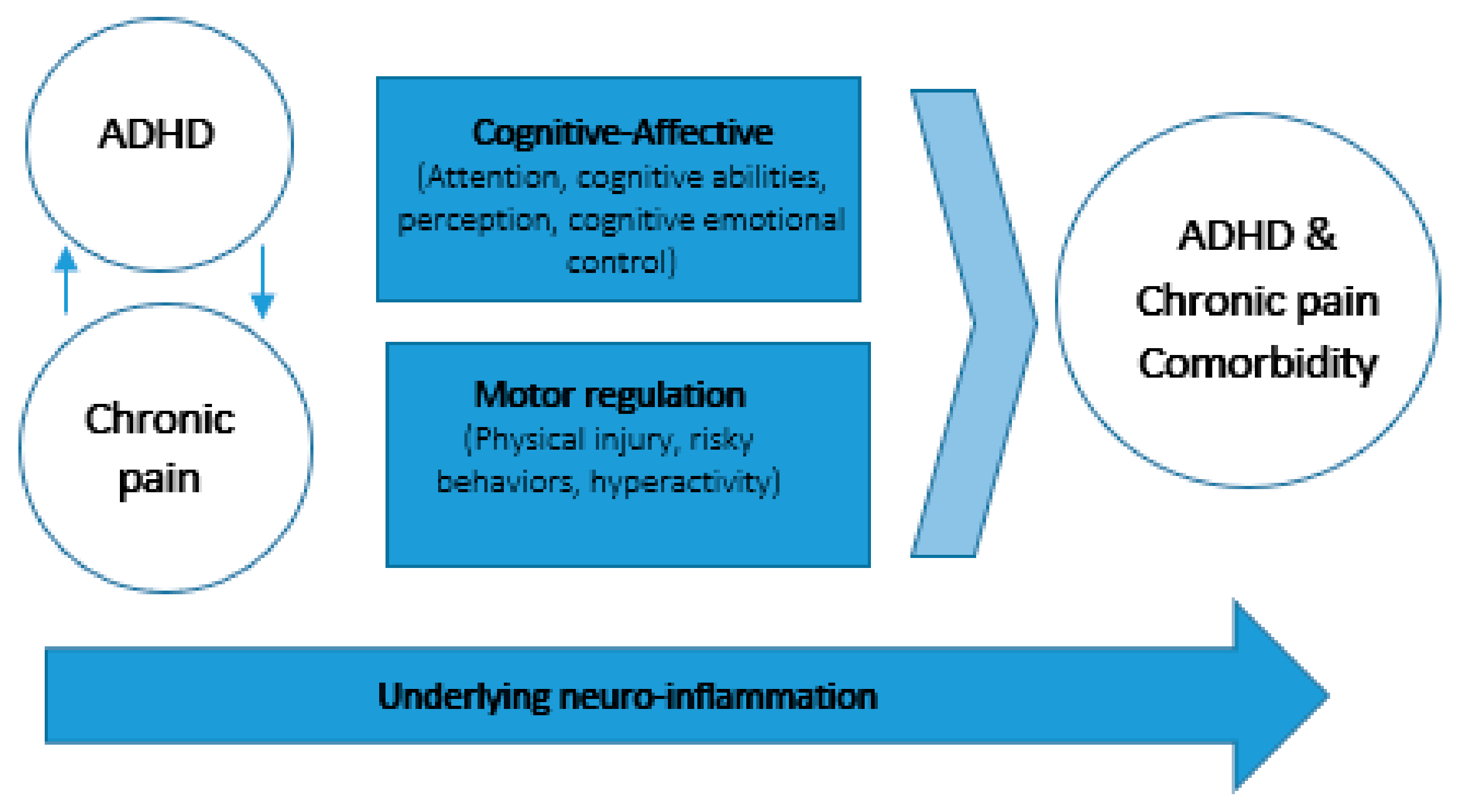
3. Aim 2: Potential Associations between Chronic Pain and ADHD over Time
3.1. Cognitive–Affective Models of Pain Highlight the Role of Attention
3.2. Motor Regulation, Injury and Pain
3.3. Neuroinflammation
4. Discussion and Future Directions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Classification of chronic pain. Descriptions of chronic pain syndromes and definitions of pain terms. Prepared by the International Association for the Study of Pain, Subcommittee on Taxonomy. Pain Suppl. 1986, 3, S1.
- King, S.; Chambers, C.T.; Huguet, A.; MacNevin, R.C.; McGrath, P.J.; Parker, L.; Macdonald, A.J. The epidemiology of chronic pain in children and adolescents revisited: A systematic review. Pain 2011, 152, 2729–2738. [Google Scholar] [CrossRef] [PubMed]
- Groenewald, C.B.; Wright, D.R.; Palermo, T.M. Health care expenditures associated with pediatric pain-related conditions in the United States. Pain 2015, 156, 951–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simon, L.S. RELIEVING PAIN IN AMERICA: A BLUEPRINT FOR TRANSFORMING PREVENTION, CARE, EDUCATION, AND RESEARCH. J. Pain Palliat. Care Pharmacother. 2012, 26, 197–198. [Google Scholar] [CrossRef]
- Holley, A.L.; Wilson, A.C.; Cho, E.; Palermo, T.M. Clinical Phenotyping of Youth With New-Onset Musculoskeletal Pain. Clin. J. Pain 2017, 33, 28–36. [Google Scholar] [CrossRef] [Green Version]
- Becker, A.J.; Heathcote, L.C.; Timmers, I.; Simons, L.E. Precipitating events in child and adolescent chronic musculoskeletal pain. Pain Rep. 2018, 3, e665. [Google Scholar] [CrossRef]
- Murray, C.B.; Groenewald, C.B.; de la Vega, R.; Palermo, T.M. Long-term impact of adolescent chronic pain on young adult educational, vocational, and social outcomes. Pain 2020, 161, 439–445. [Google Scholar] [CrossRef]
- Forgeron, P.A.; King, S.; Stinson, J.N.; McGrath, P.J.; Macdonald, A.J.; Chambers, C.T. Social Functioning and Peer Relationships in Children and Adolescents with Chronic Pain: A Systematic Review. Pain Res. Manag. 2010, 15, 27–41. [Google Scholar] [CrossRef] [Green Version]
- Cordts, K.P.; Stone, A.L.; Beveridge, J.K.; Wilson, A.C.; Noel, M. The (Parental) Whole Is Greater Than the Sum of Its Parts: A Multifactorial Model of Parent Factors in Pediatric Chronic Pain. J. Pain 2019, 20, 786–795. [Google Scholar] [CrossRef]
- Holley, A.L.; Wilson, A.C.; Palermo, T.M. Predictors of the transition from acute to persistent musculoskeletal pain in children and adolescents: A prospective study. Pain 2017, 158, 794–801. [Google Scholar] [CrossRef]
- Holley, A.; Wilson, A.; Noel, M.; Palermo, T. Post-traumatic stress symptoms in children and adolescents with chronic pain: A topical review of the literature and a proposed framework for future research. Eur. J. Pain 2016, 20, 1371–1383. [Google Scholar] [CrossRef]
- The American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders DSM-5TM, 5th ed.; The American Psychiatric Association Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Erskine, H.E.; Ferrari, A.; Nelson, P.; Polanczyk, G.V.; Flaxman, A.D.; Vos, T.; Whiteford, H.; Scott, J. Research Review: Epidemiological modelling of attention-deficit/hyperactivity disorder and conduct disorder for the Global Burden of Disease Study. J. Child Psychol. Psychiatry 2013, 54, 1263–1274. [Google Scholar] [CrossRef]
- Polanczyk, G.V.; Willcutt, E.G.; Salum, G.A.; Kieling, C.; Rohde, L.A. ADHD prevalence estimates across three decades: An updated systematic review and meta-regression analysis. Int. J. Epidemiol. 2014, 43, 434–442. [Google Scholar] [CrossRef]
- Kerekes, N.; Sanchéz-Pérez, A.M.; Landry, M. Neuroinflammation as a possible link between attention-deficit/hyperactivity disorder (ADHD) and pain. Med. Hypotheses 2021, 157, 110717. [Google Scholar] [CrossRef]
- Nigg, J.T. Attention-deficit/hyperactivity disorder and adverse health outcomes. Clin. Psychol. Rev. 2013, 33, 215–228. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, S.; Rajendran, K.; Mahbubani, S.M.; Halperin, J.M. Preschool Predictors of ADHD Symptoms and Impairment During Childhood and Adolescence. Curr. Psychiatry Rep. 2017, 19, 95. [Google Scholar] [CrossRef]
- Merrill, B.M.; Molina, B.S.G.; Coxe, S.; Gnagy, E.M.; Altszuler, A.R.; Macphee, F.L.; Morrow, A.S.; Trucco, E.M.; Pelham, W.E. Functional Outcomes of Young Adults with Childhood ADHD: A Latent Profile Analysis. J. Clin. Child Adolesc. Psychol. 2020, 49, 215–228. [Google Scholar] [CrossRef]
- Asherson, P.; Akehurst, R.; Kooij, J.J.S.; Huss, M.; Beusterien, K.; Sasané, R.; Gholizadeh, S.; Hodgkins, P. Under Diagnosis of Adult ADHD. J. Atten. Disord. 2012, 16, 20S–38S. [Google Scholar] [CrossRef]
- Doshi, J.A.; Hodgkins, P.; Kahle, J.; Sikirica, V.; Cangelosi, M.J.; Setyawan, J.; Erder, M.H.; Neumann, P.J. Economic Impact of Childhood and Adult Attention-Deficit/Hyperactivity Disorder in the United States. J. Am. Acad. Child Adolesc. Psychiatry 2012, 51, 990–1002. [Google Scholar] [CrossRef]
- Soltani, S.; Kopala-Sibley, D.C.; Noel, M. The Co-occurrence of Pediatric Chronic Pain and Depression: A Narrative Review and Conceptualization of Mutual Maintenance. Clin. J. Pain 2019, 35, 633–643. [Google Scholar] [CrossRef]
- Jastrowski Mano, K.E.; O’Bryan, E.M.; Gibler, R.C.; Beckmann, E. The Co-occurrence of Pediatric Chronic Pain and Anxiety: A Theoretical Review of a Developmentally Informed Shared Vulnerability Model. Clin. J. Pain 2019, 35, 989–1002. [Google Scholar] [CrossRef] [PubMed]
- Vinall, J.; Pavlova, M.; Asmundson, G.J.G.; Rasic, N.; Noel, M. Mental Health Comorbidities in Pediatric Chronic Pain: A Narrative Review of Epidemiology, Models, Neurobiological Mechanisms and Treatment. Children 2016, 3, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKillop, H.N.; Banez, G.A. A Broad Consideration of Risk Factors in Pediatric Chronic Pain: Where to Go from Here? Children 2016, 3, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Instanes, J.T.; Klungsøyr, K.; Halmøy, A.; Fasmer, O.B.; Haavik, J. Adult ADHD and Comorbid Somatic Disease: A Systematic Literature Review. J. Atten. Disord. 2016, 22, 203–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stray, L.L.; Kristensen, Ø.; Lomeland, M.; Skorstad, M.; Stray, T.; Tønnessen, F.E. Motor regulation problems and pain in adults diagnosed with ADHD. Behav. Brain Funct. 2013, 9, 18. [Google Scholar] [CrossRef] [Green Version]
- Lensing, M.B.; Zeiner, P.; Sandvik, L.; Opjordsmoen, S. Quality of Life in Adults Aged 50+ With ADHD. J. Atten. Disord. 2015, 19, 405–413. [Google Scholar] [CrossRef]
- Stickley, A.; Koyanagi, A.; Takahashi, H.; Kamio, Y. ADHD symptoms and pain among adults in England. Psychiatry Res. 2016, 246, 326–331. [Google Scholar] [CrossRef]
- Stickley, A.; Koyanagi, A.; Takahashi, H.; Ruchkin, V.; Inoue, Y.; Kamio, Y. Attention-deficit/hyperactivity disorder and physical multimorbidity: A population-based study. Eur. Psychiatry 2017, 45, 227–234. [Google Scholar] [CrossRef]
- Asztély, K.; Kopp, S.; Gillberg, C.; Waern, M.; Bergman, S. Chronic Pain And Health-Related Quality Of Life In Women With Autism And/Or ADHD: A Prospective Longitudinal Study. J. Pain Res. 2019, 12, 2925–2932. [Google Scholar] [CrossRef] [Green Version]
- Reyero, F.; Ponce, G.; Rodriguez-Jimenez, R.; Fernandez-Dapica, P.; Taboada, D.; Martin, V.; Navio, M.; Jiménez-Arriero, M.; Hoenicka, J.; Palomo, T. High frequency of childhood ADHD history in women with fibromyalgia. Eur. Psychiatry 2010, 26, 482–483. [Google Scholar] [CrossRef]
- Karaş, H.; Çetingök, H.; İlişer, R.; Çarpar, E.; Kaşer, M. Childhood and adult attention deficit hyperactivity disorder symptoms in fibromyalgia: Associations with depression, anxiety and disease impact. Int. J. Psychiatry Clin. Pract. 2020, 24, 257–263. [Google Scholar] [CrossRef]
- Moore, D.J.; Meints, S.M.; Lazaridou, A.; Johnson, D.; Franceschelli, O.; Cornelius, M.; Schreiber, K.; Edwards, R.R. The Effect of Induced and Chronic Pain on Attention. J. Pain 2019, 20, 1353–1361. [Google Scholar] [CrossRef]
- Petanidou, D.; Giannakopoulos, G.; Tzavara, C.; Dimitrakaki, C.; Kolaitis, G.; Tountas, Y. Adolescents’ multiple, recurrent subjective health complaints: Investigating associations with emotional/behavioural difficulties in a cross-sectional, school-based study. Child Adolesc. Psychiatry Ment. Health 2014, 8, 3. [Google Scholar] [CrossRef] [Green Version]
- Salem, H.; Vivas, D.; Cao, F.; Kazimi, I.F.; Teixeira, A.L.; Zeni, C.P. ADHD is associated with migraine: A systematic review and meta-analysis. Eur. Child Adolesc. Psychiatry 2017, 27, 267–277. [Google Scholar] [CrossRef]
- Jacobs, H.; Singhi, S.; Gladstein, J. Medical Comorbidities in Pediatric Headache. Semin. Pediatr. Neurol. 2016, 23, 60–67. [Google Scholar] [CrossRef]
- Shimizu, V.T.; Bueno, O.F.A.; Miranda, M.C. Sensory processing abilities of children with ADHD. Braz. J. Phys. Ther. 2014, 18, 343–352. [Google Scholar] [CrossRef] [Green Version]
- Merikangas, K.R.; Calkins, M.E.; Burstein, M.; He, J.-P.; Chiavacci, R.; Lateef, T.; Ruparel, K.; Gur, R.C.; Lehner, T.; Hakonarson, H.; et al. Comorbidity of Physical and Mental Disorders in the Neurodevelopmental Genomics Cohort Study. Pediatrics 2015, 135, e927–e938. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.D.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Évid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Sawyer, S.M.; Azzopardi, P.S.; Wickremarathne, D.; Patton, G.C. The age of adolescence. Lancet Child. Adolesc. Health 2018, 2, 223–228. [Google Scholar] [CrossRef]
- Celletti, C.; Mari, G.; Ghibellini, G.; Celli, M.; Castori, M.; Camerota, F. Phenotypic variability in developmental coordination disorder:Clustering of generalized joint hypermobility with attention deficit/hyperactivity disorder, atypical swallowing and narrative difficulties. Am. J. Med. Genet. C Semin. Med. Genet. 2015, 169, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Cruz, N.; O’Reilly, J.; Slomine, B.S.; Salorio, C.F. Emotional and Neuropsychological Profiles of Children With Complex Regional Pain Syndrome Type-I in an Inpatient Rehabilitation Setting. Clin. J. Pain 2011, 27, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Galli, F.; D’Antuono, G.; Tarantino, S.; Viviano, F.; Borrelli, O.; Chirumbolo, A.; Cucchiara, S.; Guidetti, V. Headache and Recurrent Abdominal Pain: A Controlled Study by the Means Of The Child Behaviour Checklist (CBCL). Cephalalgia 2007, 27, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Ghanizadeh, A.; Moaiedy, F.; Imanieh, M.H.; Askani, H.; Haghighat, M.; Dehbozorgi, G.; Dehghani, S.M. Psychiatric disorders and family functioning in children and adolescents with functional abdominal pain syndrome. J. Gastroenterol. Hepatol. 2008, 23, 1132–1136. [Google Scholar] [CrossRef] [PubMed]
- Kindgren, E.; Perez, A.Q.; Knez, R. Prevalence of ADHD and Autism Spectrum Disorder in Children with Hypermobility Spectrum Disorders or Hypermobile Ehlers-Danlos Syndrome: A Retrospective Study. Neuropsychiatr. Dis. Treat. 2021, 17, 379–388. [Google Scholar] [CrossRef]
- Lipsker, C.W.; Bölte, S.; Hirvikoski, T.; Lekander, M.; Holmström, L.; Wicksell, R.K. Prevalence of autism traits and attention-deficit hyperactivity disorder symptoms in a clinical sample of children and adolescents with chronic pain. J. Pain Res. 2018, 11, 2827–2836. [Google Scholar] [CrossRef] [Green Version]
- Kapalu, C.M.L.; Hall, J.J.; Wallace, D.P. Neuropsychological Functioning of Youth Receiving Intensive Interdisciplinary Pain Treatment. J. Pediatr. Psychol. 2018, 43, 870–881. [Google Scholar] [CrossRef] [Green Version]
- Mangerud, W.L.; Bjerkeset, O.; Lydersen, S.; Indredavik, M.S. Chronic pain and pain-related disability across psychiatric disorders in a clinical adolescent sample. BMC Psychiatry 2013, 13, 272. [Google Scholar] [CrossRef] [Green Version]
- Wolff, N.; Rubia, K.; Knopf, H.; Hölling, H.; Martini, J.; Ehrlich, S.; Roessner, V. Reduced pain perception in children and adolescents with ADHD is normalized by methylphenidate. Child Adolesc. Psychiatry Ment. Health 2016, 10, 24. [Google Scholar] [CrossRef] [Green Version]
- Woodbury, M.M. Recurrent Abdominal Pain in Child Patients Seen at a Pediatric Gastroenterology Clinic: Observations of 50 Children and Their Families. Psychosomatics 1993, 34, 485–493. [Google Scholar] [CrossRef]
- Holmberg, K.; Hjern, A. Health complaints in children with attention-deficit/hyperactivity disorder. Acta Paediatr. 2006, 95, 664–670. [Google Scholar] [CrossRef]
- Kaplan, B.J.; McNICOL, J.; Conte, R.A.; Moghadam, H.K. Physical Signs and Symptoms in Preschool-Age Hyperactive and Normal Children. J. Dev. Behav. Pediatr. 1987, 8, 305–310. [Google Scholar] [CrossRef]
- Egger, H.L.; Costello, E.J.; Erkanli, A.; Angold, A. Somatic Complaints and Psychopathology in Children and Adolescents: Stomach Aches, Musculoskeletal Pains, and Headaches. J. Am. Acad. Child Adolesc. Psychiatry 1999, 38, 852–860. [Google Scholar] [CrossRef]
- Yeh, Y.-C.; Huang, M.-F.; Wu, Y.-Y.; Hu, H.-F.; Yen, C.-F. Pain, Bullying Involvement, and Mental Health Problems Among Children and Adolescents With ADHD in Taiwan. J. Atten. Disord. 2019, 23, 809–816. [Google Scholar] [CrossRef]
- Akmatov, M.K.; Ermakova, T.; Bätzing, J. Psychiatric and Nonpsychiatric Comorbidities Among Children With ADHD: An Exploratory Analysis of Nationwide Claims Data in Germany. J. Atten. Disord. 2021, 25, 874–884. [Google Scholar] [CrossRef]
- Klassen, A.F.; Miller, A.; Fine, S. Health-Related Quality of Life in Children and Adolescents Who Have a Diagnosis of Attention-Deficit/Hyperactivity Disorder. Pediatrics 2004, 114, e541–e547. [Google Scholar] [CrossRef] [Green Version]
- Kenar, A.; Örün, U.A.; Yoldaş, T.; Kayalı, Ş.; Bodur, Ş.; Karademir, S. Anxiety, depression, and behavioural rating scales in children with non-cardiac chest pain. Cardiol. Young 2019, 29, 1268–1271. [Google Scholar] [CrossRef]
- Simons, L.E.; Elman, I.; Borsook, D. Psychological processing in chronic pain: A neural systems approach. Neurosci. Biobehav. Rev. 2014, 39, 61–78. [Google Scholar] [CrossRef] [Green Version]
- Eccleston, C.; Crombez, G. Pain demands attention: A cognitive–affective model of the interruptive function of pain. Psychol. Bull. 1999, 125, 356–366. [Google Scholar] [CrossRef]
- Ho, G.H.Y.; Bennett, S.M.; Cox, D.; Poole, G. Brief Report: Cognitive Functioning and Academic Achievement in Children and Adolescents with Chronic Pain. J. Pediatr. Psychol. 2009, 34, 311–316. [Google Scholar] [CrossRef] [Green Version]
- Beckmann, E.; Jastrowski Mano, K.E. Advancing the Measurement of Executive Functioning in Pediatric Chronic Pain. Children 2021, 8, 630. [Google Scholar] [CrossRef] [PubMed]
- Demers, M.M.; McNevin, N.; Azar, N.R. ADHD and Motor Control: A Review of the Motor Control Deficiencies Associated With Attention Deficit/Hyperactivity Disorder and Current Treatment Options. Crit. Rev. Phys. Rehabilit. Med. 2013, 25, 231–239. [Google Scholar] [CrossRef]
- Fliers, E.A.; Franke, B.; Lambregts-Rommelse, N.N.; Altink, M.E.; Buschgens, C.J.; der Sanden, M.W.N.-V.; Sergeant, J.A.; Faraone, S.V.; Buitelaar, J.K. Undertreatment of Motor Problems in Children with ADHD. Child Adolesc. Ment. Health 2010, 15, 85–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neto, F.R.; Goulardins, J.B.; Rigoli, D.; Piek, J.P.; de Oliveira, J.A. Motor development of children with attention deficit hyperactivity disorder. Rev. Bras. de Psiquiatr. 2015, 37, 228–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allan, C.C.; DeShazer, M.; Staggs, V.S.; Nadler, C.; Crawford, T.P.; Moody, S.; Chacko, A. Accidental Injuries in Preschoolers: Are We Missing an Opportunity for Early Assessment and Intervention? J. Pediatr. Psychol. 2021, 46, 835–843. [Google Scholar] [CrossRef]
- Brunkhorst-Kanaan, N.; Libutzki, B.; Reif, A.; Larsson, H.; McNeill, R.V.; Kittel-Schneider, S. ADHD and accidents over the life span–A systematic review. Neurosci. Biobehav. Rev. 2021, 125, 582–591. [Google Scholar] [CrossRef]
- Dahan, A.; Ryder, C.H.; Reiner, M. Components of Motor Deficiencies in ADHD and Possible Interventions. Neuroscience 2016, 378, 34–53. [Google Scholar] [CrossRef]
- Sil, S.; Thomas, S.; DiCesare, C.; Strotman, D.; Ting, T.V.; Myer, G.; Kashikar-Zuck, S. Preliminary Evidence of Altered Biomechanics in Adolescents With Juvenile Fibromyalgia. Arthritis Care Res. 2015, 67, 102–111. [Google Scholar] [CrossRef] [Green Version]
- Matsuda, M.; Huh, Y.; Ji, R.-R. Roles of inflammation, neurogenic inflammation, and neuroinflammation in pain. J. Anesthesia 2018, 33, 131–139. [Google Scholar] [CrossRef]
- Ji, R.-R.; Nackley, A.; Huh, B.Y.; Terrando, N.; Maixner, D.W. Neuroinflammation and Central Sensitization in Chronic and Widespread Pain. Anesthesiology 2018, 129, 343–366. [Google Scholar] [CrossRef]
- Dunn, G.A.; Nigg, J.T.; Sullivan, E.L. Neuroinflammation as a risk factor for attention deficit hyperactivity disorder. Pharmacol. Biochem. Behav. 2019, 182, 22–34. [Google Scholar] [CrossRef]
- Gustafsson, H.C.; Sullivan, E.L.; Battison, E.A.; Holton, K.F.; Graham, A.M.; Karalunas, S.L.; Fair, D.A.; Loftis, J.M.; Nigg, J.T. Evaluation of maternal inflammation as a marker of future offspring ADHD symptoms: A prospective investigation. Brain Behav. Immun. 2020, 89, 350–356. [Google Scholar] [CrossRef]
- Leffa, D.T.; Torres, I.L.; Rohde, L.A. A Review on the Role of Inflammation in Attention-Deficit/Hyperactivity Disorder. Neuroimmunomodulation 2019, 25, 328–333. [Google Scholar] [CrossRef]
- Boerner, K.; Eccleston, C.; Chambers, C.; Keogh, E. Sex differences in the efficacy of psychological therapies for the management of chronic and recurrent pain in children and adolescents: A systematic review and meta-analysis. Pain 2017, 158, 569–582. [Google Scholar] [CrossRef] [Green Version]
- May, T.; Adesina, I.; McGillivray, J.; Rinehart, N.J. Sex differences in neurodevelopmental disorders. Curr. Opin. Neurol. 2019, 32, 622–626. [Google Scholar] [CrossRef]
- Carbonneau, M.L.; Demers, M.; Bigras, M.; Guay, M.-C. Meta-Analysis of Sex Differences in ADHD Symptoms and Associated Cognitive Deficits. J. Atten. Disord. 2021, 25, 1640–1656. [Google Scholar] [CrossRef]
- Baeza-Velasco, C. Neurodevelopmental atypisms in the context of joint hypermobility, hypermobility spectrum disorders, and Ehlers–Danlos syndromes. Am. J. Med. Genet. C Semin. Med. Genet. 2021, 187, 491–499. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author, Year, Country | Aims | Study Design | Study Population | Measured Variables (ADHD; Pain) | Main Findings |
|---|---|---|---|---|---|
| Asztely et al. (2019); Sweden [30] | To investigate the prevalence of chronic pain in women with a diagnosis of ADHD in childhood. | 16–19 year follow-up of cohort of 100 females who were initially referred to a neuropsychiatric clinic; 46% of participants had ADHD at the baseline assessment. Analysis was limited to those not lost to follow-up with a primary or secondary diagnosis of ADHD (n = 74). | 74 females aged 3–18 at time of ADHD diagnosis. Follow-up was conducted at ages 19–37 (Mage = 27.2, SD= 4.2). | ADHD: Semi-structured interview by an experienced clinician based on DSM-IV criteria. Pain: Chronic widespread pain (CWP): >3 months of musculoskeletal pain, above and below the waist, on both sides of the body and involving the axial skeleton; >3 months of pain in the head or abdominal regions. | - Participants with a primary diagnosis of ADHD (n = 41), 39.0% reported CWP at follow-up. 31.7% reported chronic abdominal pain and 31.7% reported chronic headache. - Participants with ADHD treated with stimulants (24/74, 32.4%) had a statistically significantly lower prevalence of CWP than those with untreated ADHD (16.7% vs. 42.0%). |
| Celletti et al. (2015); Italy [42] | To assess the prevalence of generalized joint hypermobility (gJHM) in a group of 41 Italian children with development coordination disorder (DCD). | Compared groups of children with DCD who did and did not meet criteria for gJHM. Linear regressions were performed to assess for associations with ADHD. | 41 children (Mage = 8; 31 males, 10 females) from specialty clinics. | ADHD: Assessed using DSM-IV criteria by investigators. Pain: Physicians used Beighton scores to diagnose generalized Joint Hypermobility Syndrome, questionnaires asked about symptoms related to gJHM. | - Statistically significant higher proportion of gJHM group with frequent falls, bruising and prolonged bleeding, motor impersistence, arthralgias and myalgias, intestinal constipation, sore hands from writing, and ADHD. - Beighton score was positively associated with ADHD. |
| Cruz et al. (2011); USA [43] | To describe neuropsychological profiles of children with Type 1 Complex Regional Pain Syndrome (CRPS-I) receiving inpatient rehabilitation. | Children admitted to an inpatient rehabilitation facility completed comprehensive neuropsychological assessments. Performances on neuropsychological measures were compared with age-based norms. | 17 female children ages 9–18 (mean not calculated) with CRPS-I admitted to a neurorehabilitation unit. | ADHD: Attention problems subscale of the parent report version of Behavior Assessment System for Children (BASC) and BASC-2, prior ADHD diagnosis, Continuous Performance Test (CPT-II), Brief Test of Attention. Pain: CRPS-I diagnosis by physician, Numerical Rating Scale (NRS; 0–10). | - 4 of 17 patients (23.5%) had previously diagnosed ADHD. - Mean BASC score was within normal limits. - Overall mean standard score on the Brief Test of Attention was at-risk/impaired (M = 82.67, SD = 15.19, n = 6). |
| Galli et al. (2006); Italy [44] | To compare the prevalence of internalizing and externalizing disorders between children with recurrent abdominal pain (RAP), headache, and a control group. | Case-controlled study. ANOVA one-way analysis was used to compare Child Behavior Checklist 4–18 (CBCL) scales and subscales between groups. | 70 children with recurrent abdominal pain (Mage = 9, SD = 3.6) and 70 healthy controls (Mage = 11.6, SD = 4.6). | ADHD: CBCL, parent-report. Pain: Recurrent Abdominal Pain (RAP), clinical diagnosis according to Rome II criteria. | ANOVA showed a highly statistically significant difference between attention for children with RAP (4.03), headache (5.06) and controls (3.27), but pairwise differences between children with RAP and healthy controls were not significant. |
| Ghanizadeh et al. (2008); Iran [45] | To compare the prevalence of psychiatric disorders between youth with functional abdominal pain syndrome (FAPS), with organic abdominal pain, and without chronic pain. | Case-controlled study over 2 years at a pediatric gastroenterology clinic. Psychiatrists performed blinded interviews and ANOVAs were performed to compare groups. | 45 children with FAPS (ages 5–18, Mage = 10.8, SD = 3.6), 45 children with organic abdominal pain (ages 5–18, Mage = 11.8, SD = 3.3 children pain) and pain-free children (ages 5–18, Mage = 11.3, SD = 3.6). | ADHD: Semi-structured interview using the Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS). Pain: Functional abdominal pain syndrome (FAPS), clinical diagnosis according to Rome III criteria. | Prevalence of ADHD differed significantly among children with FAPS (15.6%), organic abdominal pain (2.2%), and pain-free controls (0%). |
| Kindgren et al. (2021); Sweden [46] | To establish the prevalence of ADHD and ASD among children with Hypermobility Spectrum Disorders (HSD) and hypermobile Ehlers–Danlos Syndrome (hEDS). | Retrospective study of children in the clinic since 2012 who received treatment for HSD or EDS. Chi-square and t-tests were used to compare groups. | 201 children ages 6–18 (Mage = 12); 113 females, 88 males treated at one pediatric and youth medicine clinic with diagnoses of HDS or hEDS. | ADHD: Prior diagnosis in medical record. Pain: Prior ICD-10 diagnosis of HDS or hEDS in medical record. Beighton hypermobility scale in medical record. | 16% of all subjects had a verified ADHD diagnosis and a further 7% were undergoing ADHD diagnostic investigation. Significantly more children with hEDS had ADHD compared to children with HSD. - |
| Lipsker et al. (2018); Sweden [47] | To examine (1) the clinically significant traits and symptoms of ASD and ADHD, (2) the proportion with previously diagnosed ADHD or ASD, and (3) differences in demographic and pain-related variables between the two groups. | Cross-sectional study examining parent–child dyads referred to a tertiary pain clinic. | 126 children and adolescents (ages = 8–17, M = 14.6) (70% female) consecutively referred for chronic pain to a specialized pain clinic. | ADHD: Conners-3 parent report Pain: Children completed the Lübeck Pain Questionnaire (LPQ). Co-occurrence of other chronic somatic disease is assessed in the LPQ using an open-ended write-in option. Intensity of pain was assessed with a visual analog scale (VAS). | Mean ADHD T-score was 55.42 (vs. population mean of 50) with 19.9% scoring as “clinically significant” (T ≥ 65). |
| Low Kapalu et al. (2018); USA [48] | To examine the cognitive or neuropsychological functioning of youth with chronic pain. | Case series of youth entering an intense interdisciplinary pain treatment program. | 94 youth with chronic pain (85.1% female, ages 10–18, Mage = 15.41, SD = 1.96) who were beginningintensive interdisciplinary pain treatment (IIPT). | ADHD: Wechsler Abbreviated Scale of Intelligence-II, Wechsler Intelligence Scale for Children-II; Processing Speed subtest (PSI), Grooved Pegboard Test, California Verbal Learning Test, Rey Complex Figure Test, WRAT-4, Conners Continuous Performance Test-II, Behavior Rating Inventory of Executive Functioning. Pain: 100 mm Visual Analogue Scale for pain. | -18% of participants had ADHD. -Youth with chronic pain had higher verbal comprehension and full-scale IQ scores than expected, below-average non-dominant hand dexterity, and difficulty with visual recall. -Performance on neuropsychological measures were generally not associated with pain intensity. |
| Mangerud et al. (2013); Norway [49] | To investigate frequency and location of chronic pain and pain-related disability among adolescent patients presenting to a psychiatric clinic. | Cross-sectional study that was part of a lager cohort study at a department of child and adolescent psychiatry. | 717 children seen by a Department of Child and Adolescent Psychiatry (43.5% of those eligible to participate, ages 13–18, Mage = 15.7, SD = 1.7). 30.1% had ADHD as their primary diagnosis. | ADHD: ICD-10 diagnosis of ADHD as the reason for presentation to the clinic. Pain: Chronic pain defined as weekly pain over the last 3 months not related to known disease or injury. Pain was considered musculoskeletal if present in the neck, shoulder, back, buttocks, chest or extremities. Pain in ≥3 sites was considered multi-site pain. | Prevalence of chronic pain was 65.9% among adolescents with ADHD, with 55.1% reporting musculoskeletal pain and 31.3% reporting multi-site pain. |
| Wolff et al. (2016); Germany [50] | To examine pain perception in children and adolescents with ADHD and the interaction between pain perception and the administration of methylphenidate (MPH). | Sample from “German Health Interview and Examination Survey for Children and Adolescents” (KiGGS) cohort. Examined parents’ assessments of children’s pain distribution and pain perception as well as differences in pain perception between subjects receiving and not receiving MPH. | 260 children and adolescents ages 3–17; 184 male, 76 female. 50% healthy controls, 25% ADHD not on MPH, 25% ADHD on MPH. | ADHD: Parent report of prior ADHD diagnosis (validated by Strengths and Difficulties Questionnaire (SDQ) Hyperactivity scale). Pain: Retrospective pain rating for past 3 month. Parent report for children aged 7–10 and self-report for children aged 11–17. | Children and adolescents diagnosed with ADHD without MPH treatment had significantly lower pain ratings compared to both healthy controls (HC) and those with ADHD treated with MPH. |
| Woodbury (1993); USA [51] | To investigate stressors, psychopathology, and biopsychosocial treatment of children with recurrent abdominal pain (RAP). | 50 children were referred to the authors with non-organic RAP, with persistent dysfunction despite diet changes. | 50 children (58% male, ages 4–20, Mage = 8) with nonorganic recurrent abdominal pain. | ADHD: Clinical interview based on the DSM-III, Conners-Teacher version. Unspecified psychological testing and/or neuropsychological testing completed for children presenting with learning problems only. Pain: Met clinical criteria for RAP | 18% of participants had ADHD. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Battison, E.A.J.; Brown, P.C.M.; Holley, A.L.; Wilson, A.C. Associations between Chronic Pain and Attention-Deficit Hyperactivity Disorder (ADHD) in Youth: A Scoping Review. Children 2023, 10, 142. https://doi.org/10.3390/children10010142
Battison EAJ, Brown PCM, Holley AL, Wilson AC. Associations between Chronic Pain and Attention-Deficit Hyperactivity Disorder (ADHD) in Youth: A Scoping Review. Children. 2023; 10(1):142. https://doi.org/10.3390/children10010142
Chicago/Turabian StyleBattison, Eleanor A. J., Patrick C. M. Brown, Amy L. Holley, and Anna C. Wilson. 2023. "Associations between Chronic Pain and Attention-Deficit Hyperactivity Disorder (ADHD) in Youth: A Scoping Review" Children 10, no. 1: 142. https://doi.org/10.3390/children10010142