
The Effectiveness of Influenza Vaccination on Chronic Obstructive Pulmonary Disease with Different Severities of Airflow Obstruction

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
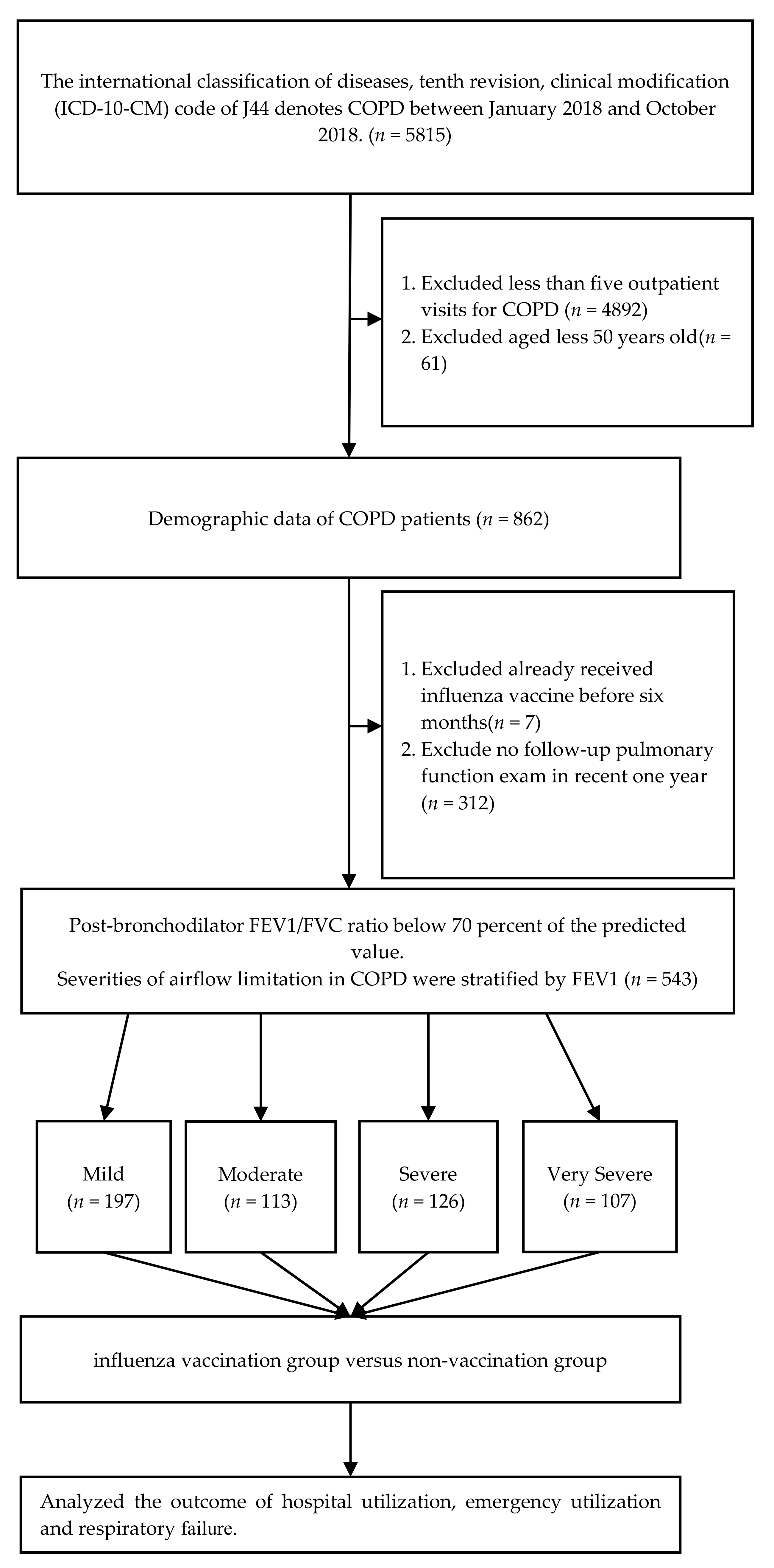
2.1. Design
2.2. Study Participants
2.3. Influenza Vaccines
2.4. Clinial Variables
2.5. Statistics
3. Results
3.1. Patients’ Characteristics
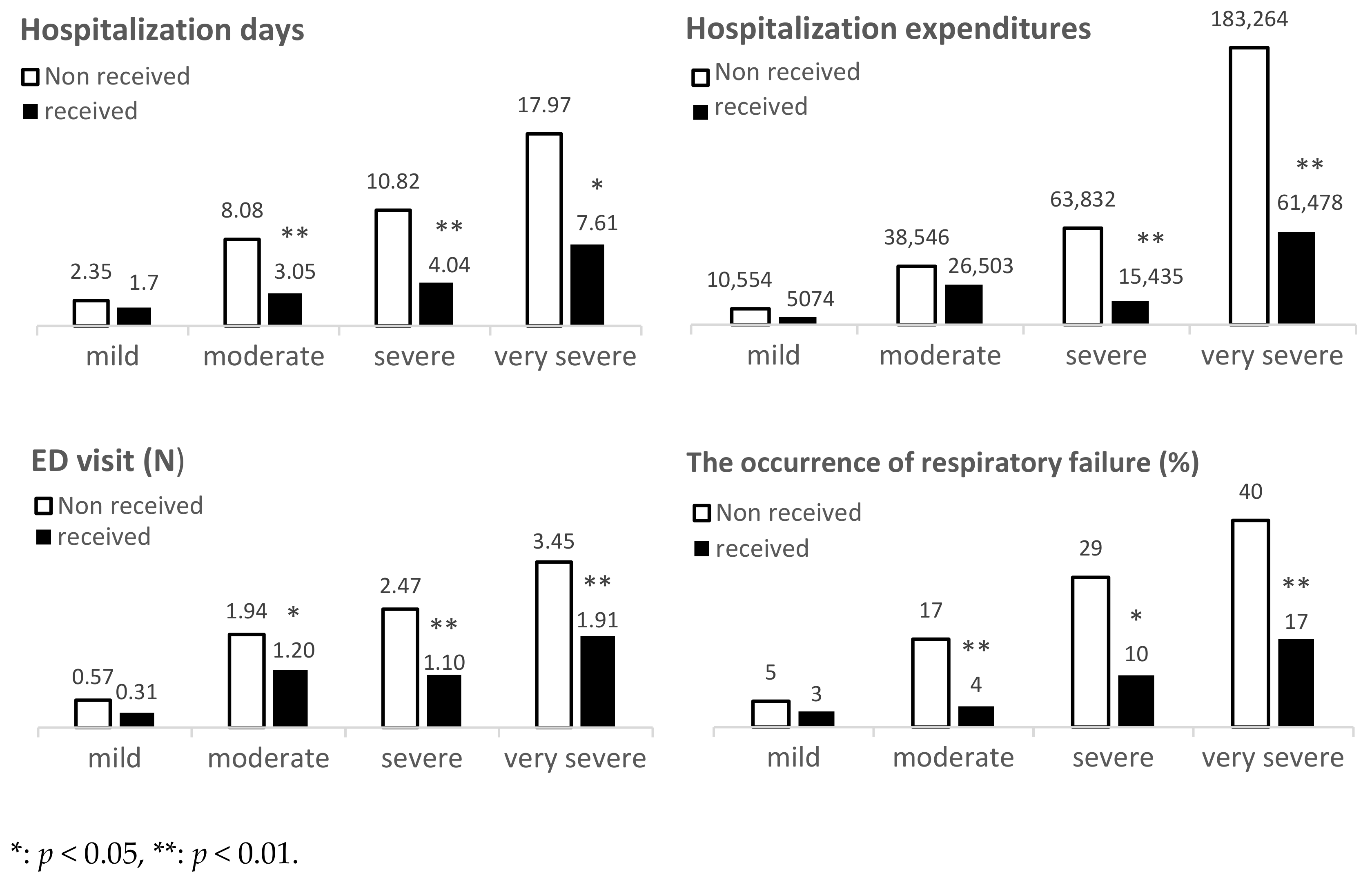
3.2. Effectiveness of Influenza Vaccination Measured by Hospital Utilization, Hospitalization Days, and Hospitalization Expenditure for COPD Patients with Different Severities of Airflow Obstruction
3.3. Effectiveness of Influenza Vaccination Measured by Emergency Department Utilization and Number of Visits in COPD Patients with Different Severities of Airflow Obstruction
3.4. Effectiveness of Influenza Vaccination Measured by Occurrence of Respiratory Failure in COPD Patients with Different Severities of Airflow Obstruction
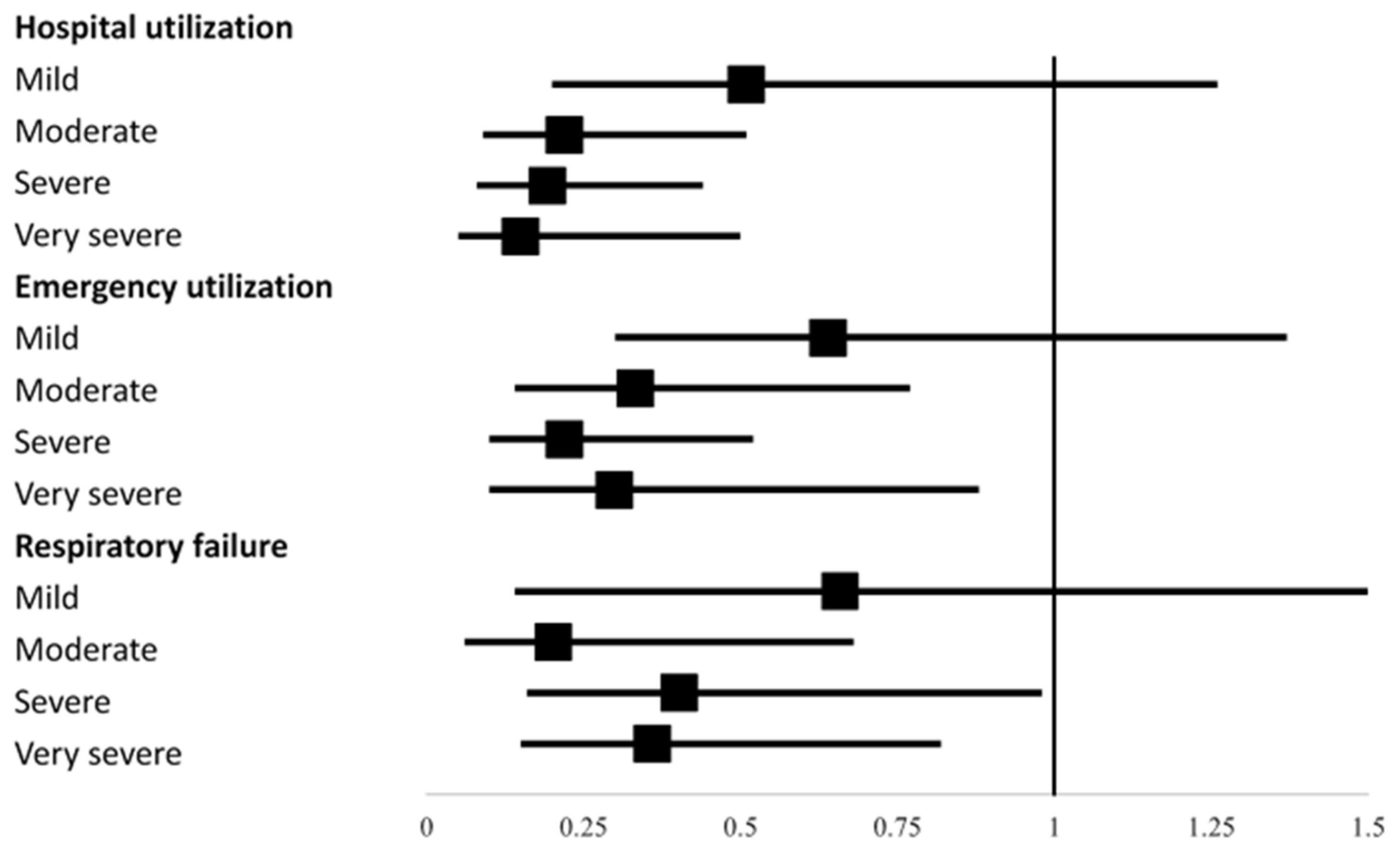
3.5. Adjusted Odds Ratio of Medical Utilization According to Influenza Vaccination Status among COPD Patients with Different Severities of Airflow Obstruction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| COPD | Chronic Obstructive Pulmonary Disease |
| GOLD | Global Initiative for Chronic Obstructive Lung Disease |
| FEV1 | Forced expiratory volume during the first second |
| FVC | Forced Vital Capacity |
References
- Ratiu, I.A.; Ligor, T.; Bocos-Bintintan, V.; Mayhew, C.A.; Buszewski, B. Volatile Organic Compounds in Exhaled Breath as Fingerprints of Lung Cancer, Asthma and COPD. J. Clin. Med. 2020, 10, 32. [Google Scholar] [CrossRef]
- 2021 Global Strategy for Prevention, Diagnosis and Management of Copd. Available online: https://goldcopd.org/ (accessed on 20 June 2021).
- Miravitlles, M.; Worth, H.; Cataluña, J.J.S.; Price, D.; De Benedetto, F.; Roche, N.; Godtfredsen, N.S.; van Der Molen, T.; Löfdahl, C.G.; Padullés, L.; et al. Observational study to characterise 24-hour COPD symptoms and their relationship with patient-reported outcomes: Results from the ASSESS study. Respir. Res. 2014, 15, 122. [Google Scholar] [CrossRef]
- Kessler, R.; Partridge, M.R.; Miravitlles, M.; Cazzola, M.; Vogelmeier, C.; Leynaud, D.; Ostinelli, J. Symptom variability in patients with severe COPD: A pan-European cross-sectional study. Eur. Respir. J. 2011, 372, 264–272. [Google Scholar] [CrossRef] [Green Version]
- Woodhead, M.; Blasi, F.; Ewig, S.; Huchon, G.; Ieven, M.; Ortqvist, A.; Schaberg, T.; Torres, A.; van der Heijden, G.; Verheijet, T.J. Guidelines for the management of adult lower respiratory tract infections. Eur. Respir. J. 2005, 26, 1138–1180. [Google Scholar] [CrossRef] [PubMed]
- Mallia, P.; Johnston, S.L. Influenza infection and COPD. Int. J. Chronic Obstr. Pulm. Dis. 2007, 2, 55–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerke, A.; Tang, F.; Yang, M.; Foster, E.; Cavanaugh, J.; Polgreen, P. Predicting chronic obstructive pulmonary disease hospitalizations based on concurrent influenza activity. COPD 2013, 10, 573–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santa-Olalla Peralta, P.; Cortes-Garcia, M.; Vicente-Herrero, M.; Castrillo-Villamandos, C.; Arias-Bohigas, P.; Pachon-Del Amo, I. Risk factors for disease severity among hospitalised patients with 2009 pandemic influenza A (H1N1) in Spain, April–December 2009. Eurosurveillance 2010, 15, 19667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, Y.H.; You, S.H.; Lin, Y.J.; Chen, S.C.; Chen, W.Y.; Chou, W.C.; Hsieh, N.H.; Liao, C.M. Mathematical modeling of postcoinfection with influenza A virus and Streptococcus pneumoniae, with implications for pneumonia and COPD-risk assessment. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 1973–1988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seki, M.; Kosai, K.; Yanagihara, K.; Higashiyama, Y.; Kurihara, S.; Izumikawa, K.; Miyazaki, Y.; Hirakata, Y.; Tashiro, T.; Kohno, S. Disease Severity in Patients with Simultaneous Influenza and Bacterial Pneumonia. Intern. Med. 2007, 46, 953–958. [Google Scholar] [CrossRef] [Green Version]
- Edwards, K.M.; Dupont, W.D.; Westrich, M.K.; Plummer, W.D., Jr.; Palmer, P.S.; Wright, P.F. A randomized controlled trial of cold- adapted and inactivated vaccines for the prevention of influenza A disease. J. Infect. Dis. 1994, 169, 68–76. [Google Scholar] [CrossRef]
- Gross, P.A.; Hermogenes, A.W.; Sacks, H.S.; Lau, J.; Levandowski, R.A. The efficacy of influenza vaccine in elderly persons: A meta-analysis and review of the literature. Ann. Intern. Med. 1995, 123, 518–527. [Google Scholar] [CrossRef] [PubMed]
- Montserrat-Capdevila, J.; Godoy, P.; Marsal, J.-R.; Cruz, I.; Solanes, M. Effectiveness of influenza vaccination in preventing hospital admission due to exacerbations of chronic obstructive pulmonary disease. Enferm. Infecc. Y Microbiol. Clin. 2014, 32, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Bekkat-Berkani, R.; Wilkinson, T.; Buchy, P.; Dos Santos, G.; Stefanidis, D.; Devaster, J.-M.; Meyer, N. Seasonal influenza vaccination in patients with COPD: A systematic literature review. BMC Pulm. Med. 2017, 17, 79. [Google Scholar] [CrossRef] [Green Version]
- Mulpuru, S.; Li, L.; Ye, L.; Hatchette, T.; Andrew, M.K.; Ambrose, A.; Boivin, G.; Bowie, W.; Chit, A.; Dos Santos, G.J.C. Effectiveness of influenza vaccination on hospitalizations and risk factors for severe outcomes in hospitalized patients with COPD. Chest 2019, 155, 69–78. [Google Scholar] [CrossRef]
- Huang, H.-H.; Chen, S.-J.; Chao, T.-F.; Liu, C.-J.; Chen, T.-J.; Chou, P.; Wang, F.-D. Influenza vaccination and risk of respiratory failure in patients with chronic obstructive pulmonary disease: A nationwide population-based case-cohort study. J. Microbiol. Immunol. Infect. 2019, 52, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Fell, P.J.; Watson, N.P.; O’Donnell, H.F.; Simmons, R.L.; Hasell, S.K. Longer term effects of influenza vaccine in patients with chronic pulmonary disease. Lancet 1977, 309, 1282–1284. [Google Scholar] [CrossRef]
- Gross, P.A.; Patriaco, D.; McGuire, K.; Weksler, M.E.; Setia, U.; Douglas, R.G., Jr. Relation of chronic disease and immune response to influenza vaccine in the elderly. Vaccine 1989, 7, 303–308. [Google Scholar] [CrossRef]
- Wongsurakiat, P.; Maranetra, K.N.; Wasi, C.; Kositanont, U.; Dejsomritrutai, W.; Charoenratanakul, S. Acute respiratory illness in patients with COPD and the effectiveness of influenza vaccination: A randomized controlled study. Chest 2004, 125, 2011–2020. [Google Scholar] [CrossRef] [Green Version]
- Rhee, C.K.; Kim, K.; Yoon, H.K.; Kim, J.A.; Kim, S.H.; Lee, S.H.; Park, Y.B.; Jung, K.S.; Yoo, K.H.; Hwang, Y.I. Natural course of early COPD. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 663. [Google Scholar] [CrossRef] [Green Version]
- Anzueto, A. Impact of exacerbations on COPD. Eur. Respir. Rev. 2010, 19, 113–118. [Google Scholar] [CrossRef] [PubMed]
- White, A.J.; Gompertz, S.; Stockley, R.A. Chronic obstructive pulmonary disease. 6: The aetiology of exacerbations of chronic obstructive pulmonary disease. Thorax 2003, 58, 73–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, L.; Cai, Y.; Barratt, B.; Lyu, B.; Chan, Q.; Hansell, A.L.; Xie, W.; Zhang, D.; Kelly, F.J.; Tong, Z. Associations between daily air quality and hospitalisations for acute exacerbation of chronic obstructive pulmonary disease in Beijing, 2013–2017: An ecological analysis. Lancet Planet Health 2019, 3, e270–e279. [Google Scholar] [CrossRef] [Green Version]
- Wedzicha, J.A.; Donaldson, G.C. Exacerbations of chronic obstructive pulmonary disease. Respir. Care 2003, 48, 1204–1213. [Google Scholar] [PubMed]
- Morris, D.E.; Cleary, D.W.; Clarke, S.C. Secondary bacterial infections associated with influenza pandemics. Front. Microbiol. 2017, 8, 1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Anthony, D.; Selemidis, S.; Vlahos, R.; Bozinovski, S. Resolving viral-induced secondary bacterial infection in COPD: A concise review. Front. Immunol. 2018, 9, 2345. [Google Scholar] [CrossRef] [Green Version]
- Van der Sluijs, K.F.; van Elden, L.J.; Nijhuis, M.; Schuurman, R.; Pater, J.M.; Florquin, S.; Goldman, M.; Jansen, H.M.; Lutter, R.; van der Poll, T. IL-10 is an important mediator of the enhanced susceptibility to pneumococcal pneumonia after influenza infection. J. Immunol. 2004, 172, 7603–7609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCullers, J.A.; Iverson, A.R.; McKeon, R.; Murray, P.J. The platelet activating factor receptor is not required for exacerbation of bacterial pneumonia following influenza. Scand. J. Infect. Dis. 2008, 40, 11–17. [Google Scholar] [CrossRef]
- Damjanovic, D.; Lai, R.; Jeyanathan, M.; Hogaboam, C.M.; Xing, Z. Marked improvement of severe lung immunopathology by influenza-associated pneumococcal superinfection requires the control of both bacterial replication and host immune responses. Am. J. Pathol. 2013, 183, 868–880. [Google Scholar] [CrossRef]
- Bradley, B.T.; Bryan, A. Emerging respiratory Infections: The infectious disease pathology of SARS, MERS, pandemic influenza, and Legionella. Semin. Diagn. Pathol. 2019, 36, 152–159. [Google Scholar] [CrossRef]
- Voordouw, B.C.G.; Sturkenboom, M.C.J.M.; Dieleman, J.P.; Stijnen, T.; van der Lei, J.; Stricker, B.H.C. Annual influenza vaccination in community-dwelling elderly individuals and the risk of lower respiratory tract infections or pneumonia. Arch. Intern. Med. 2006, 166, 1980–1985. [Google Scholar] [CrossRef] [Green Version]
- Chow, E.J.; Rolfes, M.A.; Carrico, R.L.; Furmanek, S.; Ramirez, J.A.; Ferdinands, J.M.; Fry, A.M.; Patel, M.M. Vaccine Effectiveness Against Influenza-Associated Lower Respiratory Tract Infections in Hospitalized Adults, Louisville, Kentucky, 2010–2013. Open Forum Infect. Dis. 2020, 7, ofaa262. [Google Scholar] [CrossRef]
- Wilkinson, T.M.; Patel, I.S.; Wilks, M.; Donaldson, G.C.; Wedzicha, J.A. Airway bacterial load and FEV1 decline in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2003, 167, 1090–1095. [Google Scholar] [CrossRef]
- Viniol, C.; Vogelmeier, C.F. Exacerbations of COPD. Eur. Respir. Rev. 2018, 27, 170103. [Google Scholar] [CrossRef] [Green Version]
- Celli, B.R.; Cote, C.G.; Marin, J.M.; Casanova, C.; Montes de Oca, M.; Mendez, R.A.; Pinto Plata, V.; Cabral, H.J. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N. Engl. J. Med. 2004, 350, 1005–1012. [Google Scholar] [CrossRef] [Green Version]
- Müllerová, H.; Shukla, A.; Hawkins, A.; Quint, J. Risk factors for acute exacerbations of COPD in a primary care population: A retrospective observational cohort study. BMJ Open 2014, 4, e006171. [Google Scholar] [CrossRef] [Green Version]
- Clar, C.; Oseni, Z.; Flowers, N.; Keshtkar-Jahromi, M.; Rees, K. Influenza vaccines for preventing cardiovascular disease. Cochrane Database Syst. Rev. 2015, 5, CD005050. [Google Scholar]
- Yedlapati, S.H.; Khan, S.U.; Talluri, S.; Lone, A.N.; Khan, M.Z.; Khan, M.S.; Navar, A.M.; Gulati, M.; Johnson, H.; Baum, S.; et al. Effects of Influenza Vaccine on Mortality and Cardiovascular Outcomes in Patients With Cardiovascular Disease: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2021, 10, e019636. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Severity Variables | Mild | Moderate | Severe | Very Severe | ||||
|---|---|---|---|---|---|---|---|---|
| Observation | 197 | 113 | 126 | 107 | ||||
| Age | 71.37(8.47) | 71.18(8.50) | 70.73(9.29) | 72.08(10.07) | ||||
| Gender | ||||||||
| Male | 171 | 86.80% | 87 | 76.99% | 110 | 87.30% | 83 | 77.57% |
| Female | 26 | 13.20% | 26 | 23.01% | 16 | 12.70% | 24 | 22.43% |
| Vaccination | ||||||||
| Yes | 93 | 47.21% | 51 | 45.13% | 49 | 38.89% | 45 | 42.06% |
| No | 104 | 52.79% | 62 | 54.87% | 77 | 61.11% | 62 | 57.94% |
| Smoking Status | ||||||||
| Ex-smoker | 123 | 62.44% | 71 | 62.83% | 96 | 76.19% | 67 | 62.62% |
| Non-smoker | 74 | 37.56% | 42 | 37.17% | 30 | 23.81% | 40 | 37.38% |
| Successful smoking Cessation | ||||||||
| Yes | 57 | 46.34% | 44 | 61.97% | 51 | 53.13% | 48 | 71.64% |
| No | 66 | 53.66% | 27 | 28.03% | 45 | 46.88% | 19 | 28.36% |
| Charlson comorbidity index | ||||||||
| 0 | 56 | 28.43 | 20 | 17.70 | 21 | 16.67 | 18 | 16.82 |
| 1 | 49 | 24.87 | 24 | 21.24 | 41 | 32.54 | 15 | 14.02 |
| ≥2 | 92 | 46.70 | 69 | 61.06 | 64 | 50.79 | 74 | 69.16 |
| Severity Variables | Mild | Moderate | Severe | Very Severe | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Influenza Vaccination | Non-Received | Received | p Value | Non-Received | Received | p Value | Non-Received | Received | p Value | Non-Received | Received | p Value |
| Hospital utilization (%) | 18.27 | 10.75 | 0.137 | 75.81 | 41.18 | <0.001 | 79.22 | 40.82 | <0.001 | 88.71 | 62.22 | 0.001 |
| Hospitalization, days (SD) | 2.35 (8.42) | 1.70 (8.00) | 0.582 | 8.08 (7.86) | 3.05 (4.40) | <0.001 | 10.82 (14.32) | 4.04 (5.99) | 0.002 | 17.97 (23.19) | 7.61 (11.69) | 0.017 |
| Hospitalizations expenditures mean ± SD | 10,554 (51,737) | 5074 (19,650) | 0.338 | 38,546 (56,437) | 26,503 (104,248) | 0.440 | 63,832 (100,230) | 15,435 (24,015) | 0.001 | 183,264 (282,776) | 61,478 (75,215) | 0.006 |
| ED utilization (%) | 23.08 | 18.28 | 0.408 | 77.42 | 52.94 | 0.006 | 77.92 | 46.94 | <0.001 | 88.71 | 71.11 | 0.021 |
| ED visit, N (%) | 0.57 (1.80) | 0.31 (1.00) | 0.210 | 1.94 (2.25) | 1.20 (1.56) | 0.049 | 2.47 (3.37) | 1.10 (1.61) | 0.009 | 3.45 (3.13) | 1.91 (1.93) | 0.004 |
| Respiratory failure occur (%) | 4.81 | 3.23 | 0.574 | 27.42 | 7.84 | 0.008 | 37.66 | 20.41 | 0.041 | 64.52 | 37.38 | 0.006 |
| Hospital Utilization | Emergency Utilization | Respiratory Failure | ||||
|---|---|---|---|---|---|---|
| OR(95%CI) | p value | OR(95%CI) | p value | OR(95%CI) | p value | |
| Mild | 0.51(0.2–1.26) | 0.133 | 0.64(0.30–1.37) | 0.407 | 0.66(0.14–3.20) | 0.571 |
| Moderate | 0.22(0.09–0.51) | 0.000 * | 0.33(0.14–0.77) | 0.006 | 0.20(0.06–0.68) | 0.006 |
| Severe | 0.19(0.08–0.44) | 0.000 * | 0.22(0.10–0.52) | 0.000 * | 0.40(0.16–0.98) | 0.037 |
| Very severe | 0.15(0.05–0.5) | 0.001 | 0.30(0.10–0.88) | 0.022 | 0.36(0.15–0.82) | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, H.-C.; Liu, S.-F.; Li, Y.-C.; Kuo, H.-C.; Tsai, Y.-C.; Chen, M.-H. The Effectiveness of Influenza Vaccination on Chronic Obstructive Pulmonary Disease with Different Severities of Airflow Obstruction. Biomedicines 2021, 9, 1175. https://doi.org/10.3390/biomedicines9091175
Chang H-C, Liu S-F, Li Y-C, Kuo H-C, Tsai Y-C, Chen M-H. The Effectiveness of Influenza Vaccination on Chronic Obstructive Pulmonary Disease with Different Severities of Airflow Obstruction. Biomedicines. 2021; 9(9):1175. https://doi.org/10.3390/biomedicines9091175
Chicago/Turabian StyleChang, Hui-Chuan, Shih-Feng Liu, Ying-Chun Li, Ho-Chang Kuo, Yun-Chyn Tsai, and Min-Hui Chen. 2021. "The Effectiveness of Influenza Vaccination on Chronic Obstructive Pulmonary Disease with Different Severities of Airflow Obstruction" Biomedicines 9, no. 9: 1175. https://doi.org/10.3390/biomedicines9091175