
Vulvar and Vaginal Melanomas—The Darker Shades of Gynecological Cancers


 , , and
, , and
Abstract
:1. Introduction
2. Risk Factors
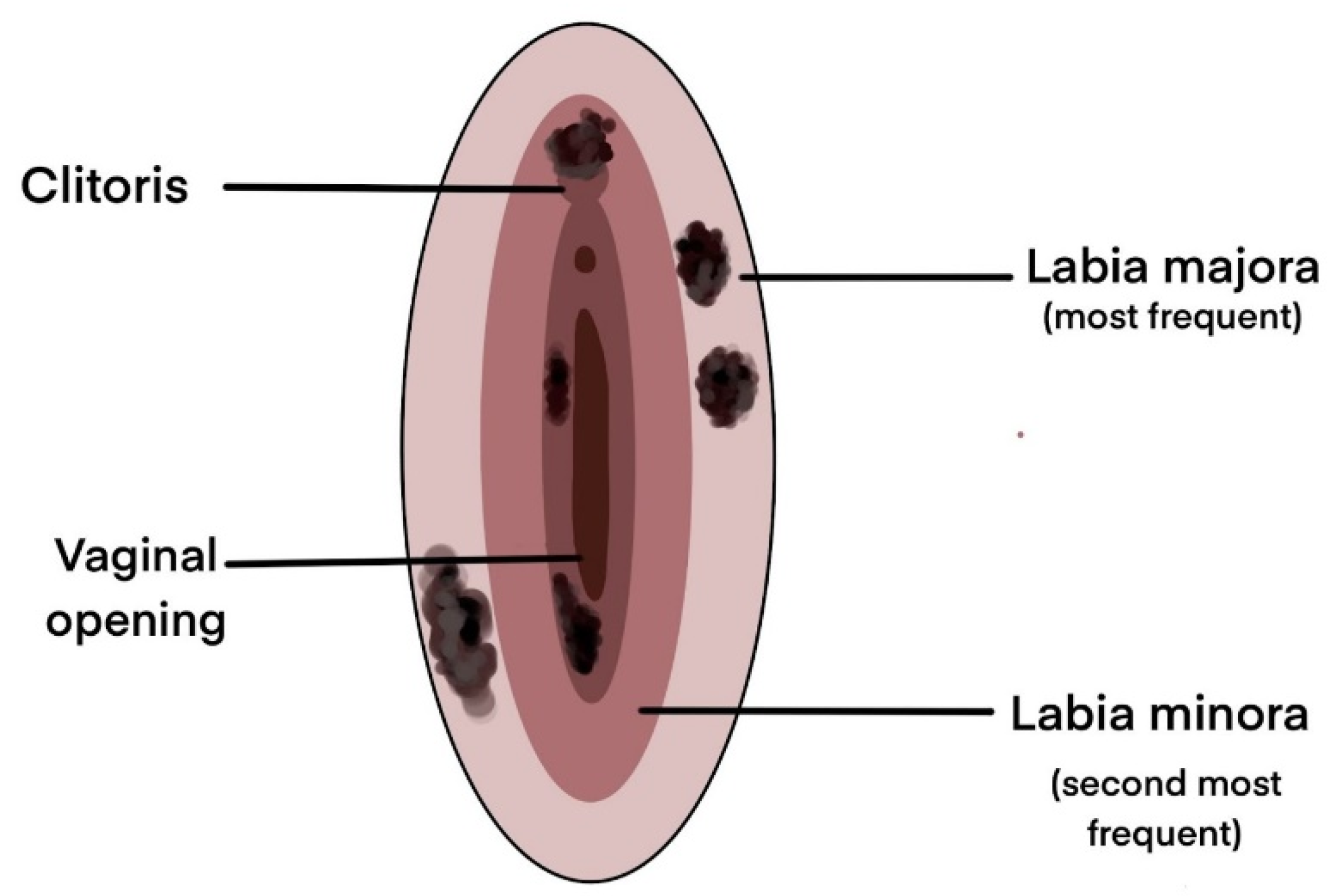
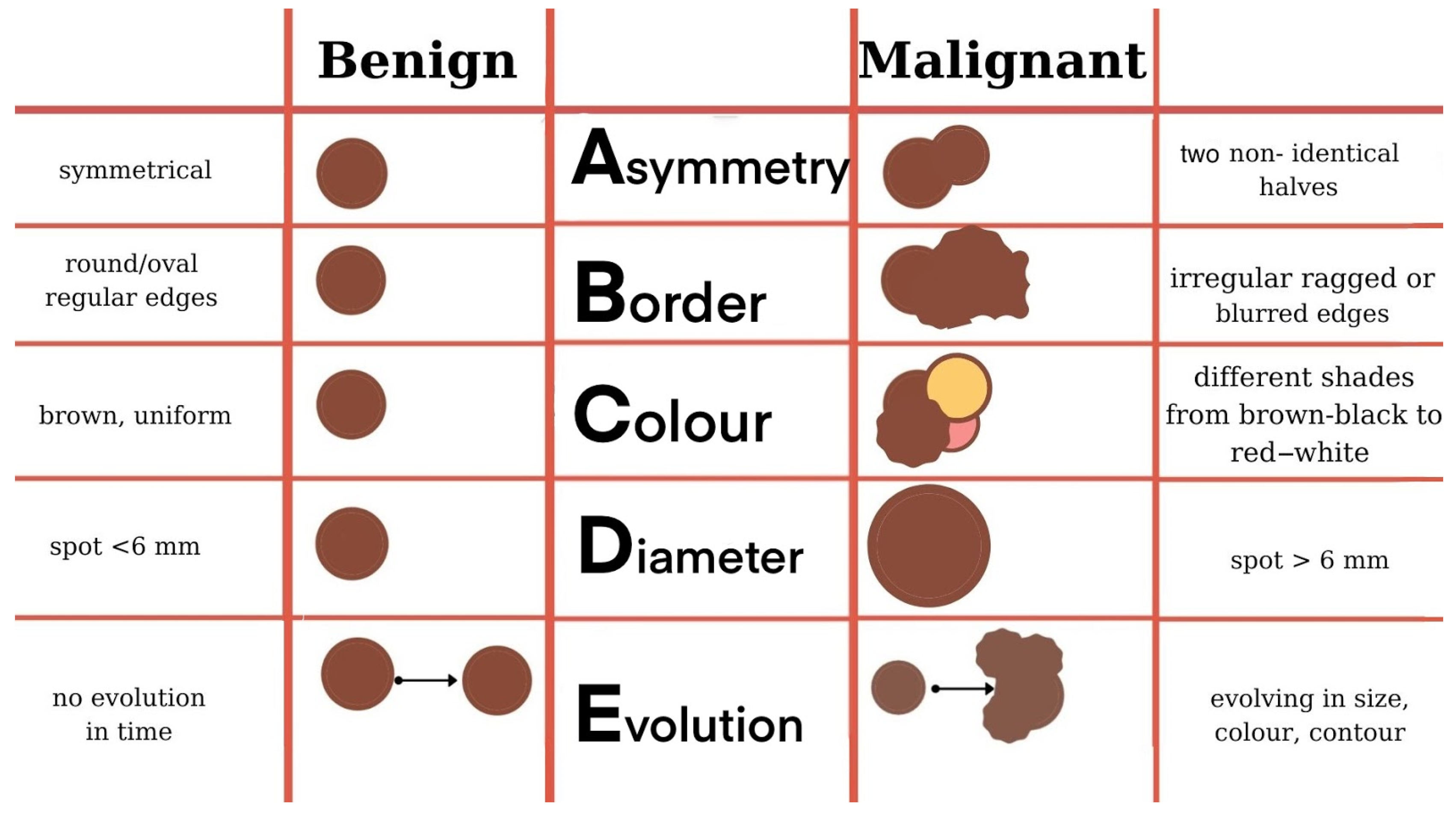
3. Clinical Manifestations

4. Histological Aspects
4.1. Macroscopic Examination
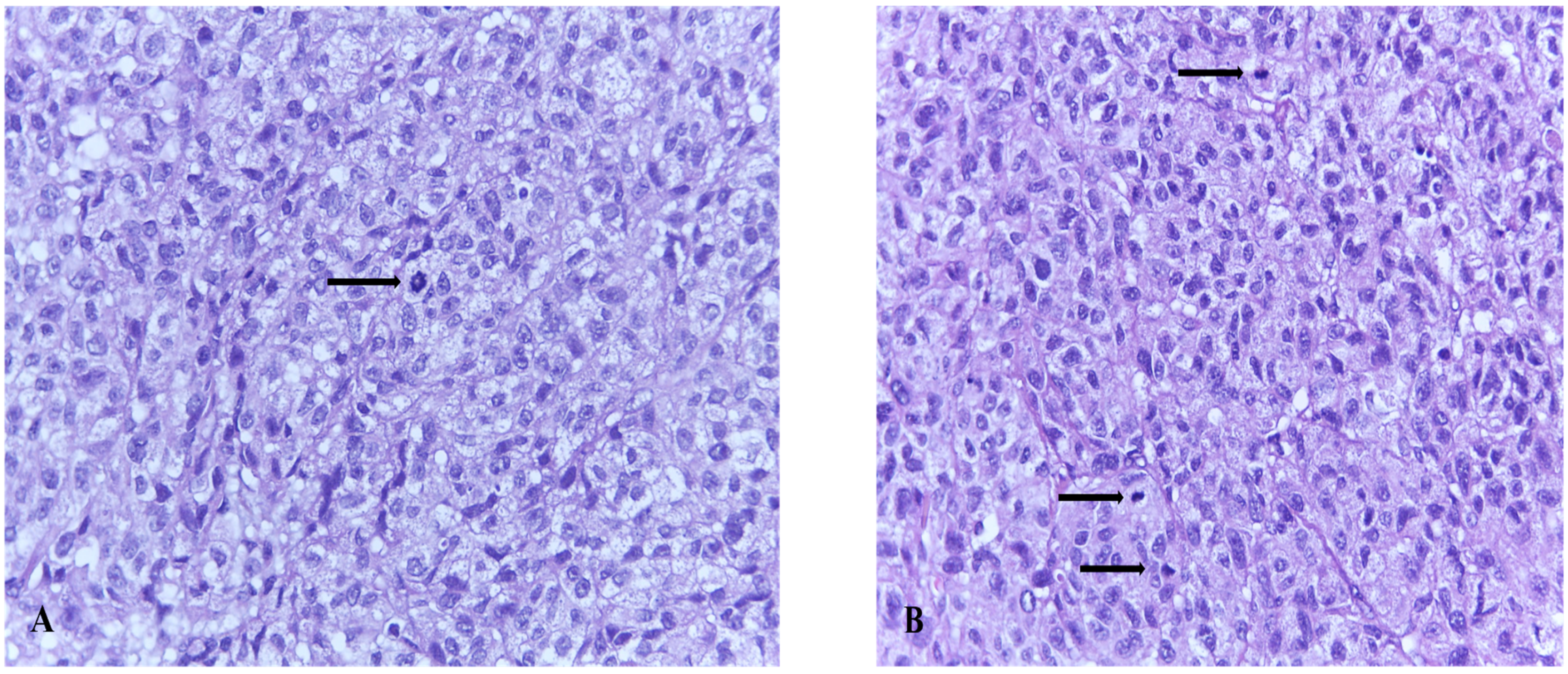
4.2. Microscopic Examination
4.3. Histological Subtypes of Melanoma
5. Immuno(cyto)histochemistry in the Diagnosis of Melanoma
6. Molecular Characterization

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mutated Gene | Percentage of Mutation (%) | Details |
|---|---|---|
| NRAS | 12/67—17.9% |
|
| BRAF | 11/67—16.4% |
|
| NF1 | 11/67—16.4% | |
| KIT | 10/67—14.9% |
|
| SF3B1 | 8/67—11.9% |
|
| TP53 | 6/67—8.9% |
|
| SPRED1 | 5/67—7.4% |
|
| ATRX | 4/67—5.9% |
|
| HLA-A | 4/67—5.9% | [93] |
| CHD8 | 3/67—4.4% | [93] |
7. Melanoma Stage Description
8. Therapeutic Approach
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Liu, Y.; Sheikh, M.S. Melanoma: Molecular Pathogenesis and Therapeutic Management. Mol. Cell. Pharmacol. 2014, 6, 228. [Google Scholar] [PubMed]
- Mort, R.L.; Jackson, I.J.; Patton, E.E. The Melanocyte Lineage in Development and Disease. Development 2015, 142, 620–632. [Google Scholar] [CrossRef] [Green Version]
- Ali, S.A.; Naaz, I. Current Challenges in Understanding the Story of Skin Pigmentation—Bridging the Morpho-Anatomical and Functional Aspects of Mammalian Melanocytes. In Muscle Cell and Tissue; Sakuma, K., Ed.; InTech: London, UK, 2015. [Google Scholar]
- Skin Cancer Statistics. Available online: https://www.wcrf.org/dietandcancer/cancer-trends/skin-cancer-statistics (accessed on 25 April 2021).
- Melanoma Skin Cancer Statistics. Available online: https://www.cancer.org/cancer/melanoma-skin-cancer/about/key-statistics.html (accessed on 25 April 2021).
- Weir, H.K.; Marrett, L.D.; Cokkinides, V.; Barnholtz-Sloan, J.; Patel, P.; Tai, E.; Jemal, A.; Li, J.; Kim, J.; Ekwueme, D.U. Melanoma in Adolescents and Young Adults (Ages 15–39 Years): United States, 1999–2006. J. Am. Acad. Dermatol. 2011, 65, S38–S49. [Google Scholar] [CrossRef] [Green Version]
- Olsen, C.M.; Thompson, J.F.; Pandeya, N.; Whiteman, D.C. Evaluation of Sex-Specific Incidence of Melanoma. JAMA Dermatol. 2020, 156, 553–560. [Google Scholar] [CrossRef]
- Paulson, K.G.; Gupta, D.; Kim, T.S.; Veatch, J.R.; Byrd, D.R.; Bhatia, S.; Wojcik, K.; Chapuis, A.G.; Thompson, J.A.; Madeleine, M.M.; et al. Age-Specific Incidence of Melanoma in the United States. JAMA Dermatol. 2020, 156, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Davis, L.E.; Shalin, S.C.; Tackett, A.J. Current State of Melanoma Diagnosis and Treatment. Cancer Biol. Ther. 2019, 20, 1366–1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthews, N.H.; Li, W.-Q.; Qureshi, A.A.; Weinstock, M.A.; Cho, E. Cutaneous Melanoma: Etiology and Therapy. Codon Publ. 2017. [Google Scholar] [CrossRef]
- Corona, R.; Mele, A.; Amini, M.; De Rosa, G.; Coppola, G.; Piccardi, P.; Fucci, M.; Pasquini, P.; Faraggiana, T. Interobserver Variability on the Histopathologic Diagnosis of Cutaneous Melanoma and Other Pigmented Skin Lesions. J. Clin. Oncol. 1996, 14, 1218–1223. [Google Scholar] [CrossRef]
- Troxel, D.B. Pitfalls in the Diagnosis of Malignant Melanoma: Findings of a Risk Management Panel Study. Am. J. Surg. Pathol. 2003, 27, 1278–1283. [Google Scholar] [CrossRef]
- Trimble, E.L. Melanomas of the Vulva and Vagina. Oncol. Williston Park 1996, 10, 1017–1023. [Google Scholar]
- Qurrat ul Ain, Q.; Rao, B. A Rare Case Report: Malignant Vulvar Melanoma. Indian J. Gynecol. Oncol. 2020, 18. [Google Scholar] [CrossRef] [Green Version]
- Boer, F.L.; Ten Eikelder, M.L.G.; Kapiteijn, E.H.; Creutzberg, C.L.; Galaal, K.; van Poelgeest, M.I.E. Vulvar Malignant Melanoma: Pathogenesis, Clinical Behaviour and Management: Review of the Literature. Cancer Treat. Rev. 2019, 73, 91–103. [Google Scholar] [CrossRef] [PubMed]
- Ragnarsson-Olding, B.K. Primary Malignant Melanoma of the Vulva—An Aggressive Tumor for Modeling the Genesis of Non-UV Light-Associated Melanomas. Acta Oncol. 2004, 43, 421–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heinzelmann-Schwarz, V.A.; Nixdorf, S.; Valadan, M.; Diczbalis, M.; Olivier, J.; Otton, G.; Fedier, A.; Hacker, N.F.; Scurry, J.P. A Clinicopathological Review of 33 Patients with Vulvar Melanoma Identifies C-KIT as a Prognostic Marker. Int. J. Mol. Med. 2014, 33, 784–794. [Google Scholar] [CrossRef] [Green Version]
- Wohlmuth, C.; Wohlmuth-Wieser, I. Vulvar Malignancies: An Interdisciplinary Perspective. J. Dtsch. Dermatol. Ges. 2019, 17, 1257–1276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jamaer, E.; Liang, Z.; Stagg, B. Primary Malignant Melanoma of the Vagina. BMJ Case Rep. 2020, 13, e232200. [Google Scholar] [CrossRef] [Green Version]
- Kalampokas, E.; Kalampokas, T.; Damaskos, C. Primary Vaginal Melanoma, A Rare and Aggressive Entity. A Case Report and Review of the Literature. In Vivo 2017, 31, 133–139. [Google Scholar] [CrossRef]
- Wohlmuth, C.; Wohlmuth-Wieser, I.; May, T.; Vicus, D.; Gien, L.T.; Laframboise, S. Malignant Melanoma of the Vulva and Vagina: A US Population-Based Study of 1863 Patients. Am. J. Clin. Dermatol. 2020, 217, 285–295. [Google Scholar] [CrossRef] [Green Version]
- Hu, D.-N.; Yu, G.-P.; McCormick, S.A. Population-Based Incidence of Vulvar and Vaginal Melanoma in Various Races and Ethnic Groups with Comparisons to Other Site-Specific Melanomas. Melanoma Res. 2010, 20, 153–158. [Google Scholar] [CrossRef]
- Riker, A.I.; Zea, N.; Trinh, T. The Epidemiology, Prevention, and Detection of Melanoma. Ochsner J. 2010, 10, 56–65. [Google Scholar]
- Scheistrøen, M.; Tropé, C.; Kaern, J.; Abeler, V.M.; Pettersen, E.O.; Kristensen, G.B. Malignant Melanoma of the Vulva FIGO Stage I: Evaluation of Prognostic Factors in 43 Patients with Emphasis on DNA Ploidy and Surgical Treatment. Gynecol. Oncol. 1996, 61, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Harting, M.S.; Kim, K.B. Biochemotherapy in Patients with Advanced Vulvovaginal Mucosal Melanoma. Melanoma Res. 2004, 14, 517–520. [Google Scholar] [CrossRef] [PubMed]
- Baiocchi, G.; Duprat, J.P.; Neves, R.I.; Fukazawa, E.M.; Landman, G.; Guimarães, G.C.; Valadares, L.J. Vulvar Melanoma: Report on Eleven Cases and Review of the Literature. Sao Paulo Med. J. 2010, 128, 38–41. [Google Scholar] [CrossRef] [Green Version]
- You, J.S.; Jones, P.A. Cancer Genetics and Epigenetics: Two Sides of the Same Coin? Cancer Cell 2012, 22, 9–20. [Google Scholar] [CrossRef] [Green Version]
- Rastrelli, M.; Tropea, S.; Rossi, C.R.; Alaibac, M. Melanoma: Epidemiology, Risk Factors, Pathogenesis, Diagnosis and Classification. In Vivo 2014, 28, 1005–1011. [Google Scholar]
- Gandini, S.; Sera, F.; Cattaruzza, M.S.; Pasquini, P.; Picconi, O.; Boyle, P.; Melchi, C.F. Meta-Analysis of Risk Factors for Cutaneous Melanoma: II. Sun Exposure. Eur. J. Cancer 2005, 41, 45–60. [Google Scholar] [CrossRef] [PubMed]
- Bevona, C.; Goggins, W.; Quinn, T.; Fullerton, J.; Tsao, H. Cutaneous Melanomas Associated with Nevi. Arch. Dermatol. 2003, 139, 1620–1624. [Google Scholar] [CrossRef]
- Stern, R.S.; PUVA Follow up Study. The Risk of Melanoma in Association with Long-Term Exposure to PUVA. J. Am. Acad. Dermatol. 2001, 44, 755–761. [Google Scholar] [CrossRef]
- Mihajlovic, M.; Vlajkovic, S.; Jovanovic, P.; Stefanovic, V. Primary Mucosal Melanomas: A Comprehensive Review. Int. J. Clin. Exp. Pathol. 2012, 5, 739–753. [Google Scholar]
- Rapi, V.; Dogan, A.; Schultheis, B.; Hartmann, F.; Rezniczek, G.A.; Tempfer, C.B. Melanoma of the Vagina: Case Report and Systematic Review of the Literature. Anticancer Res. 2017, 37, 6911–6920. [Google Scholar]
- Stang, A.; Streller, B.; Eisinger, B.; Jöckel, K.H. Population-Based Incidence Rates of Malignant Melanoma of the Vulva in Germany. Gynecol. Oncol. 2005, 96, 216–221. [Google Scholar] [CrossRef]
- Tasseron, E.W.; van der Esch, E.P.; Hart, A.A.; Brutel de la Rivière, G.; Aartsen, E.J. A Clinicopathological Study of 30 Melanomas of the Vulva. Gynecol. Oncol. 1992, 46, 170–175. [Google Scholar] [CrossRef]
- Wechter, M.E.; Gruber, S.B.; Haefner, H.K.; Lowe, L.; Schwartz, J.L.; Reynolds, K.R.; Johnston, C.M.; Johnson, T.M. Vulvar Melanoma: A Report of 20 Cases and Review of the Literature. J. Am. Acad. Dermatol. 2004, 50, 554–562. [Google Scholar] [CrossRef] [PubMed]
- Mert, I.; Semaan, A.; Winer, I.; Morris, R.T.; Ali-Fehmi, R. Vulvar/Vaginal Melanoma: An Updated Surveillance Epidemiology and End Results Database Review, Comparison with Cutaneous Melanoma and Significance of Racial Disparities. Int. J. Gynecol. Cancer 2013, 23, 1118–1126. [Google Scholar] [CrossRef] [PubMed]
- Hassanein, A.M.; Mrstik, M.E.; Hardt, N.S.; Morgan, L.A.; Wilkinson, E.J. Malignant Melanoma Associated with Lichen Sclerosus in the Vulva of a 10-Year-Old. Pediatr. Dermatol. 2004, 21, 473–476. [Google Scholar] [CrossRef]
- Hieta, N.; Kurki, S.; Rintala, M.; Söderlund, J.; Hietanen, S.; Orte, K. Association of Vulvar Melanoma with Lichen Sclerosus. Acta Derm. Venereol. 2019, 99, 339–340. [Google Scholar] [CrossRef] [Green Version]
- Zekan, J.; Sirotkovic-Skerlev, M.; Skerlev, M. Oncogenic Aspects of HPV Infections of the Female Genital Tract. In DNA Replication-Current Advances; Seligmann, H., Ed.; InTech: London, UK, 2011. [Google Scholar]
- Münger, K.; Baldwin, A.; Edwards, K.M.; Hayakawa, H.; Nguyen, C.L.; Owens, M.; Grace, M.; Huh, K. Mechanisms of Human Papillomavirus-Induced Oncogenesis. J. Virol. 2004, 78, 11451–11460. [Google Scholar] [CrossRef] [Green Version]
- Crum, C.P.; McLachlin, C.M.; Tate, J.E.; Mutter, G.L. Pathobiology of Vulvar Squamous Neoplasia. Curr. Opin. Obstet. Gynecol. 1997, 9, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Swetter, S.M.; Tsao, H.; Bichakjian, C.K.; Curiel-Lewandrowski, C.; Elder, D.E.; Gershenwald, J.E.; Guild, V.; Grant-Kels, J.M.; Halpern, A.C.; Johnson, T.M.; et al. Guidelines of Care for the Management of Primary Cutaneous Melanoma. J. Am. Acad. Dermatol. 2019, 80, 208–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, L. Pigmented Vulvar Lesions: Pigmented Vulvar Lesions. Dermatol. Ther. 2010, 23, 449–457. [Google Scholar] [CrossRef]
- Resende, F.S.; Conforti, C.; Giuffrida, R.; de Barros, M.H.; Zalaudek, I. Raised Vulvar Lesions: Be Aware! Dermatol. Pract. Concept. 2018, 8, 158–161. [Google Scholar] [CrossRef] [Green Version]
- Sand, F.L.; Thomsen, S.F. Clinician’s Update on the Benign, Premalignant, and Malignant Skin Tumours of the Vulva: The Dermatologist’s View. Int. Sch. Res. Not. 2017, 2017, 2414569. [Google Scholar] [CrossRef] [Green Version]
- De Simone, P.; Silipo, V.; Buccini, P.; Mariani, G.; Marenda, S.; Eibenschutz, L.; Ferrari, A.; Catricalà, C. Vulvar Melanoma: A Report of 10 Cases and Review of the Literature. Melanoma Res. 2008, 18, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Genton, C.Y.; Kunz, J.; Schreiner, W.E. Primary Malignant Melanoma of the Vagina and Cervix Uteri: Report of a Case with Utrastructural Study. Virchows Arch. A Path. Anat. Histol. 1981, 393, 245–250. [Google Scholar]
- Hewitt, P. Sequel to a Case of Recurrent Melanosis of Both Groins and Back: The Disease Reappearing in the Brain, Heart, Pancreas, Liver and Other Organs. Lancet 1861, 77, 263. [Google Scholar]
- Panizzon, R.G. Vulvar Melanoma. Semin. Dermatol. 1996, 15, 67–70. [Google Scholar] [CrossRef]
- Pirlamarla, A.K.; Tang, J.; Amin, B.; Kabarriti, R. Vulvar Melanoma with Isolated Metastasis to the Extraocular Muscles: Case Report and Brief Literature Review. Anticancer Res. 2018, 38, 3763–3766. [Google Scholar] [CrossRef]
- Campaner, A.B.; Fernandes, G.L.; de Cardoso, F.A.; Veasey, J.V. Vulvar Melanoma: Relevant Aspects in Therapeutic Management. An. Bras. Dermatol. 2017, 92, 398–400. [Google Scholar] [CrossRef] [Green Version]
- Baderca, F.; Cojocaru, S.; Lazăr, E.; Lăzureanu, C.; Lighezan, R.; Alexa, A.; Raica, M.; Nicola, T. Amelanotic Vulvar Melanoma: Case Report and Review of the Literature. Rom. J. Morphol. Embryol. 2008, 49, 219–228. [Google Scholar]
- Filippetti, R.; Pitocco, R. Amelanotic Vulvar Melanoma: A Case Report. Am. J. Dermatopathol. 2015, 37, e75–e77. [Google Scholar] [CrossRef]
- Mukeya, G.K.; Kakoka, I.M.; Mwansa, J.C.; Kalau, W.A. Mélanome malin vulvaire: À propos d’un cas observé à l’Hôpital du Cinquantenaire de Lubumbashi. Pan Afr. Med. J. 2020, 36, 124. [Google Scholar] [CrossRef]
- Sinasac, S.E.; Petrella, T.M.; Rouzbahman, M.; Sade, S.; Ghazarian, D.; Vicus, D. Melanoma of the Vulva and Vagina: Surgical Management and Outcomes Based on a Clinicopathologic Reviewof 68 Cases. J. Obstet. Gynaecol. Can. 2019, 41, 762–771. [Google Scholar] [CrossRef]
- Verschraegen, C.F.; Benjapibal, M.; Supakarapongkul, W.; Levy, L.B.; Ross, M.; Atkinson, E.N.; Bodurka-Bevers, D.; Kavanagh, J.J.; Kudelka, A.P.; Legha, S.S. Vulvar Melanoma at the M. D. Anderson Cancer Center: 25 Years Later. Int. J. Gynecol. Cancer 2001, 11, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Vaccari, S.; Barisani, A.; Salvini, C.; Pirola, S.; Preti, E.P.; Pennacchioli, E.; Iacobone, A.D.; Patrizi, A.; Tosti, G. Thin Vulvar Melanoma: A Challenging Diagnosis. Dermoscopic Features of a Case Series. Clin. Exp. Dermatol. 2020, 45, 187–193. [Google Scholar] [CrossRef]
- Pandey, G.; Dave, P.; Patel, S.; Patel, B.; Arora, R.; Parekh, C.; Begum, D. Female Genital Tract Melanoma: Analysis from a Regional Cancer Institute. J. Turk. Soc. Obstet. Gynecol. 2020, 17, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Joste, M.; Dion, L.; Brousse, S.; Nyangoh Timoh, K.; Rousseau, C.; Reilhac, A.; Laviolle, B.; Lesimple, T.; Lavoue, V.; Leveque, J. Vulvar and Vaginal Melanomas: A Retrospective Study Spanning 19 Years from a Tertiary Center. J. Gynecol. Obstet. Hum. Reprod. 2021, 50, 102091. [Google Scholar] [CrossRef] [PubMed]
- Martin-Gorgojo, A.; Comunion-Artieda, A.; Pizarro-Redondo, A.; Bru-Gorraiz, F.-J. A Minute ‘Ugly-Duckling’ Pigmented Lesion on the Arm of a 60-Year-Old Caucasian Female. In Clinical Cases in Melanoma; Springer International Publishing: Cham, Switzerland, 2020; pp. 29–31. [Google Scholar]
- Rogers, T.; Pulitzer, M.; Marino, M.L.; Marghoob, A.A.; Zivanovic, O.; Marchetti, M.A. Early Diagnosis of Genital Mucosal Melanoma: How Good Are Our Dermoscopic Criteria? Dermatol. Pract. Concept. 2016, 6, 43–46. [Google Scholar] [CrossRef] [Green Version]
- Oguri, H.; Izumiya, C.; Maeda, N.; Fukaya, T.; Moriki, T. A Primary Amelanotic Melanoma of the Vagina, Diagnosed by Immunohistochemical Staining with HMB-45, Which Recurred as a Pigmented Melanoma. J. Clin. Pathol. 2004, 57, 986–988. [Google Scholar] [CrossRef] [Green Version]
- Gautam, D.; Ahmed, M. Melanoma Detection and Classification Using SVM Based Decision Support System. In Proceedings of the 2015 Annual IEEE India Conference (INDICON), New Delhi, India, 17–20 December 2015; pp. 1–6. [Google Scholar]
- Goldsmith, S.M.; Solomon, A.R. A Series of Melanomas Smaller than 4 Mm and Implications for the ABCDE Rule. J. Eur. Acad. Dermatol. Venereol. 2007, 21, 929–934. [Google Scholar] [CrossRef]
- Blum, A.; Simionescu, O.; Argenziano, G.; Braun, R.; Cabo, H.; Eichhorn, A.; Kirchesch, H.; Malvehy, J.; Marghoob, A.A.; Puig, S.; et al. Dermoscopy of Pigmented Lesions of the Mucosa and the Mucocutaneous Junction: Results of a Multicenter Study by the International Dermoscopy Society (IDS): Results of a Multicenter Study by the International Dermoscopy Society (IDS). Arch. Dermatol. 2011, 147, 1181–1187. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.-T. Diagnosis, Treatment and Prognosis of Early Melanoma: The Importance of Depth of Microinvasion. Ann. Surg. 1980, 191, 87–97. [Google Scholar] [CrossRef]
- Pflugfelder, A.; Weide, B.; Eigentler, T.K.; Forschner, A.; Leiter, U.; Held, L.; Meier, F.; Garbe, C. Incisional Biopsy and Melanoma Prognosis: Facts and Controversies. Clin. Dermatol. 2010, 28, 316–318. [Google Scholar] [CrossRef] [PubMed]
- Tadiparthi, S.; Panchani, S.; Iqbal, A. Biopsy for Malignant Melanoma—Are We Following the Guidelines? Ann. R. Coll. Surg. Engl. 2008, 90, 322–325. [Google Scholar] [CrossRef] [PubMed]
- Dickson, P.V.; Gershenwald, J.E. Staging and Prognosis of Cutaneous Melanoma. Surg. Oncol. Clin. N. Am. 2011, 20, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Keung, E.Z.; Gershenwald, J.E. The Eighth Edition American Joint Committee on Cancer (AJCC) Melanoma Staging System: Implications for Melanoma Treatment and Care. Expert Rev. Anticancer Ther. 2018, 18, 775–784. [Google Scholar] [CrossRef]
- Gershenwald, J.E.; Scolyer, R.A.; Hess, K.R.; Sondak, V.K.; Long, G.V.; Ross, M.I.; Lazar, A.J.; Faries, M.B.; Kirkwood, J.M.; McArthur, G.A.; et al. Melanoma Staging: Evidence-Based Changes in the American Joint Committee on Cancer Eighth Edition Cancer Staging Manual. CA Cancer J. Clin. 2017, 67, 472–492. [Google Scholar] [CrossRef] [Green Version]
- Hou, J.Y.; Baptiste, C.; Hombalegowda, R.B.; Tergas, A.I.; Feldman, R.; Jones, N.L.; Chatterjee-Paer, S.; Bus-Kwolfski, A.; Wright, J.D.; Burke, W.M. Vulvar and Vaginal Melanoma: A Unique Subclass of Mucosal Melanoma Based on a Comprehensive Molecular Analysis of 51 Cases Compared with 2253 Cases of Nongynecologic Melanoma: Molecular Study of Vulvovaginal Melanoma. Cancer 2017, 123, 1333–1344. [Google Scholar] [CrossRef] [PubMed]
- Coit, D.G.; Andtbacka, R.; Anker, C.J.; Bichakjian, C.K.; Carson, W.E., III; Daud, A.; DiMaio, D.; Fleming, M.D.; Guild, V.; Halpern, A.C.; et al. Melanoma, Version 2.2013: Featured Updates to the NCCN Guidelines. J. Natl. Compr. Canc. Netw. 2013, 11, 395–407. [Google Scholar] [CrossRef] [Green Version]
- Smoller, B.R. Histologic Criteria for Diagnosing Primary Cutaneous Malignant Melanoma. Mod. Pathol. 2006, 19, S34–S40. [Google Scholar] [CrossRef] [PubMed]
- Connolly, K.L.; Nehal, K.S.; Busam, K.J. Lentigo Maligna and Lentigo Maligna Melanoma: Contemporary Issues in Diagnosis and Management. Melanoma Manag. 2015, 2, 171–178. [Google Scholar] [CrossRef]
- Saida, T.; Koga, H.; Goto, Y.; Uhara, H. Characteristic Distribution of Melanin Columns in the Cornified Layer of Acquired Acral Nevus: An Important Clue for Histopathologic Differentiation from Early Acral Melanoma. Am. J. Dermatopathol. 2011, 33, 468–473. [Google Scholar] [CrossRef] [PubMed]
- James, W.; Elston, D.; Treat, J.; Rosenbach, M.; Micheletti, R. Melanocytic Nevi and Neoplasms. In Andrews’ Diseases of the Skin; Elsevier: Amsterdam, The Netherlands, 2019. [Google Scholar]
- DeMatos, P.; Tyler, D.; Seigler, H.F. Mucosal Melanoma of the Female Genitalia: A Clinicopathologic Study of Forty-Three Cases at Duke University Medical Center. Surgery 1998, 124, 38–48. [Google Scholar] [CrossRef]
- Petković, M.; Jurakić Tončić, R. Nested Melanoma, a New Morphological Variant of Superficial Spreading Melanoma with Characteristic Dermoscopic Features. Acta Dermatovenerol. Croat. 2017, 25, 80–81. [Google Scholar]
- Urso, C.; Rongioletti, F.; Innocenzi, D.; Batolo, D.; Chimenti, S.; Fanti, P.L.; Filotico, R.; Gianotti, R.; Lentini, M.; Tomasini, C.; et al. Histological Features Used in the Diagnosis of Melanoma Are Frequently Found in Benign Melanocytic Naevi. J. Clin. Pathol. 2005, 58, 409–412. [Google Scholar] [CrossRef] [Green Version]
- Banerjee, S.S.; Harris, M. Morphological and Immunophenotypic Variations in Malignant Melanoma: Variations in Malignant Melanoma. Histopathology 2000, 36, 387–402. [Google Scholar] [CrossRef]
- Nadji, M.; Ganjei, P.; Penneys, N.S.; Morales, A.R. Immunohistochemistry of Vulvar Neoplasms: A Brief Review. Int. J. Gynecol. Pathol. 1984, 3, 41–50. [Google Scholar] [CrossRef]
- Xu, X.; Chu, A.Y.; Pasha, T.L.; Elder, D.E.; Zhang, P.J. Immunoprofile of MITF, Tyrosinase, Melan-A, and MAGE-1 in HMB45-Negative Melanomas. Am. J. Surg. Pathol. 2002, 26, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Cochran, A.J.; Wen, D.R. S-100 Protein as a Marker for Melanocytic and Other Tumours. Pathology 1985, 17, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Wick, M.R.; Swanson, P.E.; Rocamora, A. Recognition of Malignant Melanoma by Monoclonal Antibody HMB-45. An Immunohistochemical Study of 200 Paraffin-Embedded Cutaneous Tumors. J. Cutan. Pathol. 1988, 15, 201–207. [Google Scholar] [CrossRef]
- Orchard, G.E. Comparison of Immunohistochemical Labelling of Melanocyte Differentiation Antibodies Melan-A, Tyrosinase and HMB 45 with NKIC3 and S100 Protein in the Evaluation of Benign Naevi and Malignant Melanoma. Histochem. J. 2000, 32, 475–481. [Google Scholar] [CrossRef]
- Willis, B.C.; Johnson, G.; Wang, J.; Cohen, C. SOX10: A Useful Marker for Identifying Metastatic Melanoma in Sentinel Lymph Nodes. Appl. Immunohistochem. Mol. Morphol. 2015, 23, 109–112. [Google Scholar] [CrossRef]
- D’Angelo, S.P.; Larkin, J.; Sosman, J.A.; Lebbé, C.; Brady, B.; Neyns, B.; Schmidt, H.; Hassel, J.C.; Hodi, F.S.; Lorigan, P.; et al. Efficacy and Safety of Nivolumab Alone or in Combination with Ipilimumab in Patients with Mucosal Melanoma: A Pooled Analysis. J. Clin. Oncol. 2017, 35, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.; Wu, X.; Yu, J.; Yu, H.; Xu, T.; Brown, K.M.; Bai, X.; Dai, J.; Ma, M.; Tang, H.; et al. Analysis of NRAS Gain in 657 Patients with Melanoma and Evaluation of Its Sensitivity to a MEK Inhibitor. Eur. J. Cancer 2018, 89, 90–101. [Google Scholar] [CrossRef]
- Hintzsche, J.D.; Gorden, N.T.; Amato, C.M.; Kim, J.; Wuensch, K.E.; Robinson, S.E.; Applegate, A.J.; Couts, K.L.; Medina, T.M.; Wells, K.R.; et al. Whole-Exome Sequencing Identifies Recurrent SF3B1 R625 Mutation and Comutation of NF1 and KIT in Mucosal Melanoma. Melanoma Res. 2017, 27, 189–199. [Google Scholar] [CrossRef]
- Lyu, J.; Song, Z.; Chen, J.; Shepard, M.J.; Song, H.; Ren, G.; Li, Z.; Guo, W.; Zhuang, Z.; Shi, Y. Whole-Exome Sequencing of Oral Mucosal Melanoma Reveals Mutational Profile and Therapeutic Targets: WES of OMM Reveals Genomic Alterations. J. Pathol. 2018, 244, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Newell, F.; Kong, Y.; Wilmott, J.S.; Johansson, P.A.; Ferguson, P.M.; Cui, C.; Li, Z.; Kazakoff, S.H.; Burke, H.; Dodds, T.J.; et al. Whole-Genome Landscape of Mucosal Melanoma Reveals Diverse Drivers and Therapeutic Targets. Nat. Commun. 2019, 10, 3163. [Google Scholar] [CrossRef] [PubMed]
- Rouzbahman, M.; Kamel-Reid, S.; Al Habeeb, A.; Butler, M.; Dodge, J.; Laframboise, S.; Murphy, J.; Rasty, G.; Ghazarian, D. Malignant Melanoma of Vulva and Vagina: A Histomorphological Review and Mutation Analysis—A Single-Center Study. J. Low. Genit. Tract Dis. 2015, 19, 350–353. [Google Scholar] [CrossRef]
- Cai, Y.-J.; Ke, L.-F.; Zhang, W.-W.; Lu, J.-P.; Chen, Y.-P. Recurrent KRAS, KIT and SF3B1 Mutations in Melanoma of the Female Genital Tract. BMC Cancer 2021, 21, 677. [Google Scholar] [CrossRef]
- Nassar, K.W.; Tan, A.C. The Mutational Landscape of Mucosal Melanoma. Semin. Cancer Biol. 2020, 61, 139–148. [Google Scholar] [CrossRef]
- Kiuru, M.; Busam, K.J. The NF1 Gene in Tumor Syndromes and Melanoma. Lab. Investig. 2017, 97, 146–157. [Google Scholar] [CrossRef] [Green Version]
- Guillot, B.; Dalac, S.; Delaunay, M.; Baccard, M.; Chevrant-Breton, J.; Dereure, O.; Machet, L.; Sassolas, B.; Zeller, J.; Bernard, P.; et al. Cutaneous Malignant Melanoma and Neurofibromatosis Type 1. Melanoma Res. 2004, 14, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Omholt, K.; Grafström, E.; Kanter-Lewensohn, L.; Hansson, J.; Ragnarsson-Olding, B.K. KIT Pathway Alterations in Mucosal Melanomas of the Vulva and Other Sites. Clin. Cancer Res. 2011, 17, 3933–3942. [Google Scholar]
- Xiao, W.; Du, N.; Huang, T.; Guo, J.; Mo, X.; Yuan, T.; Chen, Y.; Ye, T.; Xu, C.; Wang, W.; et al. TP53 Mutation as Potential Negative Predictor for Response of Anti-CTLA-4 Therapy in Metastatic Melanoma. EBioMedicine 2018, 32, 119–124. [Google Scholar] [CrossRef] [Green Version]
- Ablain, J.; Liu, S.; Moriceau, G.; Lo, R.S.; Zon, L.I. SPRED1 Deletion Confers Resistance to MAPK Inhibition in Melanoma. J. Exp. Med. 2021, 218. [Google Scholar] [CrossRef]
- Qadeer, Z.A.; Harcharik, S.; Valle-Garcia, D.; Chen, C.; Birge, M.B.; Vardabasso, C.; Duarte, L.F.; Bernstein, E. Decreased Expression of the Chromatin Remodeler ATRX Associates with Melanoma Progression. J. Investig. Dermatol. 2014, 134, 1768–1772. [Google Scholar] [CrossRef] [Green Version]
- Piura, B. Management of Primary Melanoma of the Female Urogenital Tract. Lancet Oncol. 2008, 9, 973–981. [Google Scholar] [CrossRef]
- Breslow, A. Thickness, Cross-Sectional Areas and Depth of Invasion in the Prognosis of Cutaneous Melanoma. Ann. Surg. 1970, 172, 902–908. [Google Scholar] [CrossRef]
- Clark, W.H., Jr.; From, L.; Bernardino, E.A.; Mihm, M.C. The Histogenesis and Biologic Behavior of Primary Human Malignant Melanomas of the Skin. Cancer Res. 1969, 29, 705–727. [Google Scholar]
- Chung, A.F.; Woodruff, J.M.; Lewis, J.L., Jr. Malignant Melanoma of the Vulva: A Report of 44 Cases. Obstet. Gynecol. 1975, 45, 638–646. [Google Scholar] [CrossRef]
- Leitao, M.M., Jr. Management of Vulvar and Vaginal Melanomas: Current and Future Strategies. Am. Soc. Clin. Oncol. Educ. Book 2014, e277–e281. [Google Scholar] [CrossRef]
- Treatment of Vulvar Melanoma. Available online: https://www.cancer.org/cancer/vulvar-cancer/treating/vulvar-melanoma.html (accessed on 26 April 2021).
- Gadducci, A.; Carinelli, S.; Guerrieri, M.E.; Aletti, G.D. Melanoma of the Lower Genital Tract: Prognostic Factors and Treatment Modalities. Gynecol. Oncol. 2018, 150, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Albert, A.; Lee, A.; Allbright, R.; Vijayakumar, S. Vulvar Melanoma: An Analysis of Prognostic Factors and Treatment Patterns. J. Gynecol. Oncol. 2020, 31, e66. [Google Scholar] [CrossRef]
- Cinotti, E.; Chevallier, J.; Labeille, B.; Cambazard, F.; Thomas, L.; Balme, B.; Leccia, M.T.; D’Incan, M.; Vercherin, P.; Douchet, C.; et al. Mucosal Melanoma: Clinical, Histological and c-Kit Gene Mutational Profile of 86 French Cases. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 1834–1840. [Google Scholar] [CrossRef] [PubMed]
- Domingues, B.; Lopes, J.M.; Soares, P.; Pópulo, H. Melanoma Treatment in Review. ImmunoTargets Ther. 2018, 7, 35–49. [Google Scholar] [CrossRef] [Green Version]
- Janco, J.M.; Markovic, S.N.; Weaver, A.L.; Cliby, W.A. Vulvar and Vaginal Melanoma: Case Series and Review of Current Management Options Including Neoadjuvant Chemotherapy. Gynecol. Oncol. 2013, 129, 533–537. [Google Scholar] [CrossRef]
- Tcheung, W.J.; Selim, M.A.; Herndon, J.E., 2nd; Abernethy, A.P.; Nelson, K.C. Clinicopathologic Study of 85 Cases of Melanoma of the Female Genitalia. J. Am. Acad. Dermatol. 2012, 67, 598–605. [Google Scholar] [CrossRef] [PubMed]
- Handolias, D.; Hamilton, A.L.; Salemi, R.; Tan, A.; Moodie, K.; Kerr, L.; Dobrovic, A.; McArthur, G.A. Clinical Responses Observed with Imatinib or Sorafenib in Melanoma Patients Expressing Mutations in KIT. Br. J. Cancer 2010, 102, 1219–1223. [Google Scholar] [CrossRef] [Green Version]
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved Survival with Ipilimumab in Patients with Metastatic Melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef]
- Cocorocchio, E.; Pala, L.; Conforti, F.; Guerini-Rocco, E.; De Pas, T.; Ferrucci, P.F. Successful Treatment with Avapritinib in Patient with Mucosal Metastatic Melanoma. Ther. Adv. Med. Oncol. 2020, 12, 1758835920946158. [Google Scholar] [CrossRef]
- Brand, E.; Fu, Y.S.; Lagasse, L.D.; Berek, J.S. Vulvovaginal Melanoma: Report of Seven Cases and Literature Review. Gynecol. Oncol. 1989, 33, 54–60. [Google Scholar] [CrossRef]
- Landthaler, M.; Braun-Falco, O.; Richter, K.; Baltzwr, J.; Zander, J. Maligne Melanome Der Vulva. DMW 1985, 110, 789–794. [Google Scholar] [CrossRef] [PubMed]
- Lotem, M.; Anteby, S.; Peretz, T.; Ingber, A.; Avinoach, I.; Prus, D. Mucosal Melanoma of the Female Genital Tract Is a Multifocal Disorder. Gynecol. Oncol. 2003, 88, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Tsvetkov, C.; Gorchev, G.; Tomov, S.; Hinkova, N.; Nikolova, M.; Veselinova, T. Primary malignant melanoma of the vagina and treatment options: A case report. Akush. Ginekol. 2014, 53, 35–40. [Google Scholar]
- Irvin, W.P., Jr.; Legallo, R.L.; Stoler, M.H.; Rice, L.W.; Taylor, P.T., Jr.; Andersen, W.A. Vulvar Melanoma: A Retrospective Analysis and Literature Review. Gynecol. Oncol. 2001, 83, 457–465. [Google Scholar] [CrossRef]
- Schiavone, M.B.; Broach, V.; Shoushtari, A.N.; Carvajal, R.D.; Alektiar, K.; Kollmeier, M.A.; Abu-Rustum, N.R.; Leitao, M.M., Jr. Combined Immunotherapy and Radiation for Treatment of Mucosal Melanomas of the Lower Genital Tract. Gynecol. Oncol. Rep. 2016, 16, 42–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-Bosquet, J.; García Jiménez, A.; Gil Moreno, A.; Xercavins, J. Malignant Vulvo-Vaginal Melanoma: A Report of 7 Cases. Eur. J. Gynaecol. Oncol. 1997, 18, 63–67. [Google Scholar]





| Number of Patients | Tumor Localisation | Main Signs and Symptoms | Others Signs and Symptoms | References |
|---|---|---|---|---|
| 51 | Labia minora | Pain, Palpable mass, Genital bleeding, Pruritus | Dysuria, Ulceration | [57] |
| 20 | Labia majora | Genital bleeding, Pruritus, Palpable mass | Pain, Dysuria, Unhealing sore, Urinary difficulties | [36] |
| 10 | Labia majora | Pruritus | - | [47] |
| 11 | Not specified | Pruritus, Pain, Genital bleeding | - | [26] |
| 14 | Labia minora | Pruritus | - | [58] |
| 31 | Vagina | Genital bleeding, Pain, Palpable mass | Abnormal vaginal secretion, Urinary difficulties | [59] |
| 33 | Not specified | Palpable mass, Genital bleeding, Pain, Pruritus | Abnormal vaginal secretion, Dysuria, Dyspareunia, Ulceration | [60] |
| 198 | Unilateral, Clitoris | Genital bleeding, Pain, Pruritus | - | [15] |
| Level of Invasion | Clark Classification—Level of Invasion of Cutaneous Melanoma | Chung Classification—Level of Invasion of Mucosal Melanoma |
|---|---|---|
| I | Lesions involving only the epidermis (in situ melanoma) | Tumor confined to the epithelium |
| II | Invasion of the papillary dermis—does not reach the papillary-reticular dermal interface | Tumor penetrates the basement membrane and invades at a depth of <1 mm |
| III | Invasion fills and expands the papillary dermis but does not extend to reticular dermis | Tumor invades at a depth of 1–2 mm |
| IV | Invasion into the reticular dermis but not into the subcutaneous tissue | Tumor invades at a depth of >2 mm, but without reaching the subcutaneous fat |
| V | Invasion through the reticular dermis into the subcutaneous tissue | Tumor penetrates the subcutaneous fat |
| STAGE | T (Tumor) | N (Nodules) | M (Metastasis) |
|---|---|---|---|
| 0 | Tis | N0 | M0 |
| IA | T1a | N0 | M0 |
| IB | T1b, T2a | N0 | M0 |
| IIA | T2b, T3a | N0 | M0 |
| IIB | T3b, T4a | N0 | M0 |
| IIC | T4b | N0 | M0 |
| IIIA | T1a/b, T2a | N1, N2a | M0 |
| IIIB | T0 | N1b, N1c | M0 |
| T1a/b, T2a | N1b/c, N2b | M0 | |
| T2b, T3a | N1a-N2b | M0 | |
| IIIC | T0 | N2b/c, N3b/c | M0 |
| T1a-T3a | N2c, N3 | M0 | |
| T3b, T4a | N ≥ N1 | M0 | |
| T4b | N1a-N2c | M0 | |
| IIID | T4b | N3 | M0 |
| IV | Any T, Tis | Any N | M1 |
| Tumor Width | Margins | Reference |
|---|---|---|
| <2 mm | 0.5 cm | [103] |
| 2 mm | 1 cm | |
| >2 mm | 2 cm | |
| <1 mm | 1 cm | [98] |
| 1–4 mm | 2 cm | |
| invasion of subcutaneous fat/fascia, any size | >1 cm | |
| in situ | 0.5 cm | [15] |
| <2 mm | 1 cm | |
| >2 mm | 2 cm |
| Number of Patients | Mean Depth Invasion | Management | Median Survival (Months) | Reccurence | Reference |
|---|---|---|---|---|---|
| 13 | Not provided | Not provided | 15 | Not provided | [119] |
| 7 | 8 mm | Wide local excision | 31 | 71% | [118] |
| 14 | 3.23 mm | 13% Radical surgery and lymphadenectomy 27% Wide local excision and lymph node evaluation 53% Wide local excision | Not provided | 42% | [122] |
| 9 | 4 mm | Radical surgery and lymphadenectomy | 78 | 32–43% (in situ) | [120] |
| 85 | 3.2 mm | 12.9% Chemotherapy 24.7% Immunotherapy (IL-2, IFN, vaccine trials) 2.35% Chemotherapy and Immunotherapy 15.29% Radiotherapy 78.8% Surgery | 62.4 | Not provided | [114] |
| 48 | >3 mm | 29.58% Wide local excision and lymphadenectomy 21.42% Radical surgery (8% pelvic exenteration) | 39.6 | Not provided | [113] |
| 1917 | Not provided | 95.044% Surgery 10.38% Radiation 9.99% Immunotherapy 5.32% Chemotherapy | Not provided | Not provided | [110] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dobrică, E.-C.; Vâjâitu, C.; Condrat, C.E.; Crețoiu, D.; Popa, I.; Gaspar, B.S.; Suciu, N.; Crețoiu, S.M.; Varlas, V.N. Vulvar and Vaginal Melanomas—The Darker Shades of Gynecological Cancers. Biomedicines 2021, 9, 758. https://doi.org/10.3390/biomedicines9070758
Dobrică E-C, Vâjâitu C, Condrat CE, Crețoiu D, Popa I, Gaspar BS, Suciu N, Crețoiu SM, Varlas VN. Vulvar and Vaginal Melanomas—The Darker Shades of Gynecological Cancers. Biomedicines. 2021; 9(7):758. https://doi.org/10.3390/biomedicines9070758
Chicago/Turabian StyleDobrică, Elena-Codruța, Cristina Vâjâitu, Carmen Elena Condrat, Dragoș Crețoiu, Ileana Popa, Bogdan Severus Gaspar, Nicolae Suciu, Sanda Maria Crețoiu, and Valentin Nicolae Varlas. 2021. "Vulvar and Vaginal Melanomas—The Darker Shades of Gynecological Cancers" Biomedicines 9, no. 7: 758. https://doi.org/10.3390/biomedicines9070758