
Lupus Vasculitis: An Overview

 ,
,  and
and
Abstract
:1. Introduction
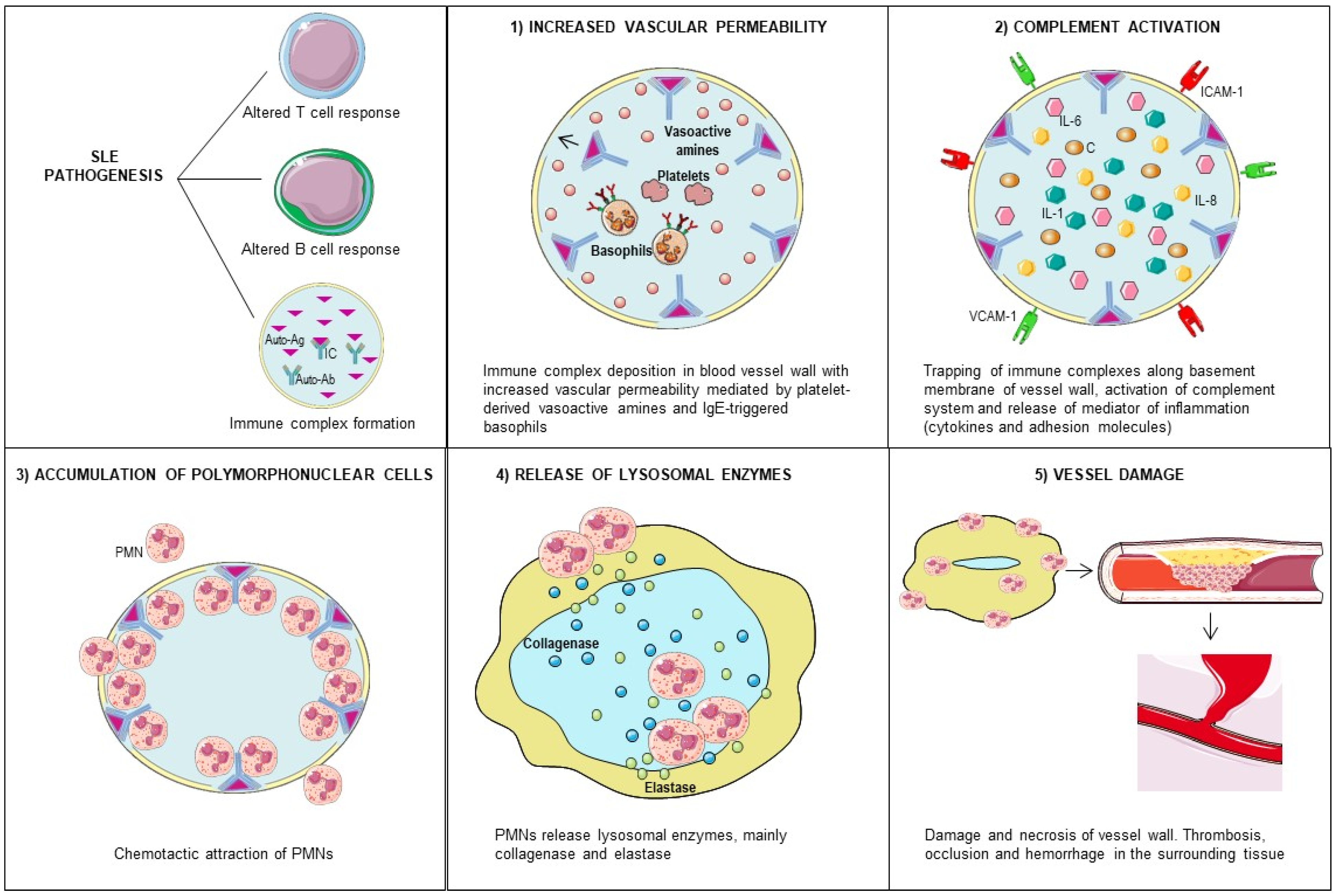
2. Pathogenesis
3. Cutaneous Vasculitis
4. Nervous System Vasculitis
5. Gastrointestinal Vasculitis
6. Renal Vasculitis
7. Retinal Vasculitis
8. Coronary Vasculitis
9. Pulmonary Vasculitis
10. Association between Lupus Vasculitis and Antiphospholipid Syndrome
11. Treatment
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Rahman, A.; Isenberg, D.A. Systemic lupus erythematosus. N. Engl. J. Med. 2008, 358, 929–939. [Google Scholar] [CrossRef] [Green Version]
- Doyle, M.K. Vasculitis associated with connective tissue disorders. Curr. Rheumatol. Rep. 2006, 8, 312–316. [Google Scholar] [CrossRef]
- Leone, P.; Cicco, S.; Vacca, A.; Dammacco, F.; Racanelli, V. Vasculitis in connective tissue diseases. In Systemic Vasculitides: Current Status and Perspectives; Dammcco, F., Ribatti, D., Vacca, A., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 345–359. [Google Scholar]
- Drenkard, C.; Villa, A.R.; Reyes, E.; Abello, M.; Alarcon-Segovia, D. Vasculitis in systemic lupus erythematosus. Lupus 1997, 6, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Casals, M.; Nardi, N.; Lagrutta, M.; Brito-Zeron, P.; Bove, A.; Delgado, G.; Cervera, R.; Ingelmo, M.; Font, J. Vasculitis in systemic lupus erythematosus: Prevalence and clinical characteristics in 670 patients. Medicine (Baltimore) 2006, 85, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Alarcón-Segovia, D.; Drenkard, C. Vasculitis and the antiphospholipid syndrome. Rheumatology (Oxford) 2000, 8, 922–923. [Google Scholar] [CrossRef] [Green Version]
- Kallenberg, C.G.; Heeringa, P. Pathogenesis of vasculitis. Lupus 1998, 7, 280–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pyrpasopoulou, A.; Chatzimichailidou, S.; Aslanidis, S. Vascular disease in systemic lupus erythematosus. Autoimmune Dis. 2012, 2012, 876456. [Google Scholar] [CrossRef] [Green Version]
- Fauci, A.S.; Haynes, B.; Katz, P. The spectrum of vasculitis: Clinical, pathologic, immunologic and therapeutic considerations. Ann. Intern. Med. 1978, 89, 660–676. [Google Scholar] [CrossRef]
- Manderson, A.P.; Botto, M.; Walport, M.J. The role of complement in the development of systemic lupus erythematosus. Annu Rev. Immunol. 2004, 22, 431–456. [Google Scholar] [CrossRef]
- Jennette, J.C. Implications for pathogenesis of patterns of injury in small- and medium-sized-vessel vasculitis. Cleve. Clin. J. Med. 2002, 69 (Suppl. 2), SII33-8. [Google Scholar] [CrossRef]
- Belmont, H.M.; Abramson, S.B.; Lie, J.T. Pathology and pathogenesis of vascular injury in systemic lupus erythematosus. Interactions of inflammatory cells and activated endothelium. Arthritis Rheum 1996, 39, 9–22. [Google Scholar] [CrossRef]
- Cid, M.C. Endothelial cell biology, perivascular inflammation, and vasculitis. Cleve. Clin. J. Med. 2002, 69 (Suppl. 2), SII45–SII49. [Google Scholar] [CrossRef] [PubMed]
- Renaudineau, Y.; Dugue, C.; Dueymes, M.; Youinou, P. Antiendothelial cell antibodies in systemic lupus erythematosus. Autoimmun Rev. 2002, 1, 365–372. [Google Scholar] [CrossRef]
- Cieslik, P.; Hrycek, A.; Klucinski, P. Vasculopathy and vasculitis in systemic lupus erythematosus. Pol. Arch. Med. Wewn. 2008, 118, 57–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manolova, I.; Dancheva, M.; Halacheva, K. Antineutrophil cytoplasmic antibodies in patients with systemic lupus erythematosus: Prevalence, antigen specificity, and clinical associations. Rheumatol. Int. 2001, 20, 197–204. [Google Scholar] [CrossRef]
- Sen, D.; Isenberg, D.A. Antineutrophil cytoplasmic autoantibodies in systemic lupus erythematosus. Lupus 2003, 12, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Jennette, J.C.; Xiao, H.; Falk, R.J. Pathogenesis of vascular inflammation by anti-neutrophil cytoplasmic antibodies. J. Am. Soc. Nephrol. 2006, 17, 1235–1242. [Google Scholar] [CrossRef]
- Wiik, A. What you should know about PR3-ANCA. An introduction. Arthritis Res. 2000, 2, 252–254. [Google Scholar] [CrossRef] [Green Version]
- Levine, J.S.; Branch, D.W.; Rauch, J. The antiphospholipid syndrome. N. Engl. J. Med. 2002, 346, 752–763. [Google Scholar] [CrossRef] [Green Version]
- Meroni, P.L.; Raschi, E.; Camera, M.; Testoni, C.; Nicoletti, F.; Tincani, A.; Khamashta, M.A.; Balestrieri, G.; Tremoli, E.; Hess, D.C. Endothelial activation by aPL: A potential pathogenetic mechanism for the clinical manifestations of the syndrome. J. Autoimmun. 2000, 15, 237–240. [Google Scholar] [CrossRef] [PubMed]
- Praprotnik, S.; Blank, M.; Meroni, P.L.; Rozman, B.; Eldor, A.; Shoenfeld, Y. Classification of anti-endothelial cell antibodies into antibodies against microvascular and macrovascular endothelial cells: The pathogenic and diagnostic implications. Arthritis Rheum. 2001, 44, 1484–1494. [Google Scholar] [CrossRef]
- Mahajan, A.; Herrmann, M.; Munoz, L.E. Clearance Deficiency and Cell Death Pathways: A Model for the Pathogenesis of SLE. Front. Immunol. 2016, 7, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brinkmann, V.; Reichard, U.; Goosmann, C.; Fauler, B.; Uhlemann, Y.; Weiss, D.S.; Weinrauch, Y.; Zychlinsky, A. Neutrophil extracellular traps kill bacteria. Science 2004, 303, 1532–1535. [Google Scholar] [CrossRef]
- Fuchs, T.A.; Abed, U.; Goosmann, C.; Hurwitz, R.; Schulze, I.; Wahn, V.; Weinrauch, Y.; Brinkmann, V.; Zychlinsky, A. Novel cell death program leads to neutrophil extracellular traps. J. Cell Biol. 2007, 176, 231–241. [Google Scholar] [CrossRef]
- Kambas, K.; Mitroulis, I.; Apostolidou, E.; Girod, A.; Chrysanthopoulou, A.; Pneumatikos, I.; Skendros, P.; Kourtzelis, I.; Koffa, M.; Kotsianidis, I.; et al. Autophagy mediates the delivery of thrombogenic tissue factor to neutrophil extracellular traps in human sepsis. PLoS ONE 2012, 7, e45427. [Google Scholar] [CrossRef]
- Frangou, E.; Vassilopoulos, D.; Boletis, J.; Boumpas, D.T. An emerging role of neutrophils and NETosis in chronic inflammation and fibrosis in systemic lupus erythematosus (SLE) and ANCA-associated vasculitides (AAV): Implications for the pathogenesis and treatment. Autoimmun. Rev. 2019, 18, 751–760. [Google Scholar] [CrossRef]
- Kambas, K.; Chrysanthopoulou, A.; Vassilopoulos, D.; Apostolidou, E.; Skendros, P.; Girod, A.; Arelaki, S.; Froudarakis, M.; Nakopoulou, L.; Giatromanolaki, A.; et al. Tissue factor expression in neutrophil extracellular traps and neutrophil derived microparticles in antineutrophil cytoplasmic antibody associated vasculitis may promote thromboinflammation and the thrombophilic state associated with the disease. Ann. Rheum. Dis. 2014, 73, 1854–1863. [Google Scholar] [CrossRef] [Green Version]
- Villanueva, E.; Yalavarthi, S.; Berthier, C.C.; Hodgin, J.B.; Khandpur, R.; Lin, A.M.; Rubin, C.J.; Zhao, W.; Olsen, S.H.; Klinker, M.; et al. Netting neutrophils induce endothelial damage, infiltrate tissues, and expose immunostimulatory molecules in systemic lupus erythematosus. J. Immunol. 2011, 187, 538–552. [Google Scholar] [CrossRef] [Green Version]
- Riemekasten, G.; Ziemer, S.; Haupl, T.; Melzer, C.; Loddenkemper, K.; Hauptmann, S.; Burmester, G.R.; Hiepe, F. Shwartzman phenomenon in a patient with active systemic lupus erythematosus preceding fatal disseminated intravascular coagulation. Lupus 2002, 11, 204–207. [Google Scholar] [CrossRef] [PubMed]
- D’Cruz, D. Vasculitis in systemic lupus erythematosus. Lupus 1998, 7, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Radic, M.; Martinovic Kaliterna, D.; Radic, J. Drug-induced vasculitis: A clinical and pathological review. Neth. J. Med. 2012, 70, 12–17. [Google Scholar] [PubMed]
- Guillevin, L.; Lhote, F.; Gherardi, R. The spectrum and treatment of virus-associated vasculitides. Curr. Opin. Rheumatol. 1997, 9, 31–36. [Google Scholar] [CrossRef]
- Agnello, V.; Chung, R.T.; Kaplan, L.M. A role for hepatitis C virus infection in type II cryoglobulinemia. N. Engl. J. Med. 1992, 327, 1490–1495. [Google Scholar] [CrossRef]
- Kallas, R.; Goldman, D.; Petri, M.A. Cutaneous vasculitis in SLE. Lupus Sci. Med. 2020, 7, e000411. [Google Scholar] [CrossRef]
- Sharma, A.; Dhooria, A.; Aggarwal, A.; Rathi, M.; Chandran, V. Connective Tissue Disorder-Associated Vasculitis. Curr. Rheumatol. Rep. 2016, 18, 31. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, M.V.; Lo, S.C.; de Almeida, C.S.; Shinjo, S.K. Anti-Ro antibody and cutaneous vasculitis in systemic lupus erythematosus. Clin. Rheumatol. 2009, 28, 301–304. [Google Scholar] [CrossRef]
- Garcia-Carrasco, M.; Ramos-Casals, M.; Cervera, R.; Trejo, O.; Yague, J.; Siso, A.; Jimenez, S.; de La Red, G.; Font, J.; Ingelmo, M. Cryoglobulinemia in systemic lupus erythematosus: Prevalence and clinical characteristics in a series of 122 patients. Semin. Arthritis Rheum. 2001, 30, 366–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barile-Fabris, L.; Hernandez-Cabrera, M.F.; Barragan-Garfias, J.A. Vasculitis in systemic lupus erythematosus. Curr. Rheumatol. Rep. 2014, 16, 440. [Google Scholar] [CrossRef]
- Jafri, K.; Patterson, S.L.; Lanata, C. Central Nervous System Manifestations of Systemic Lupus Erythematosus. Rheum. Dis. Clin. N. Am. 2017, 43, 531–545. [Google Scholar] [CrossRef]
- Bortoluzzi, A.; Silvagni, E.; Furini, F.; Piga, M.; Govoni, M. Peripheral nervous system involvement in systemic lupus erythematosus: A review of the evidence. Clin. Exp. Rheumatol. 2019, 37, 146–155. [Google Scholar]
- Gorson, K.C. Vasculitic neuropathies: An update. Neurologist 2007, 13, 12–19. [Google Scholar] [CrossRef]
- Florica, B.; Aghdassi, E.; Su, J.; Gladman, D.D.; Urowitz, M.B.; Fortin, P.R. Peripheral neuropathy in patients with systemic lupus erythematosus. Semin. Arthritis Rheum. 2011, 41, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Toledano, P.; Orueta, R.; Rodriguez-Pinto, I.; Valls-Sole, J.; Cervera, R.; Espinosa, G. Peripheral nervous system involvement in systemic lupus erythematosus: Prevalence, clinical and immunological characteristics, treatment and outcome of a large cohort from a single centre. Autoimmun. Rev. 2017, 16, 750–755. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, M.; Galego, O.; Costa, C.; Jesus, D.; Carvalho, P.; Santiago, M.; Malcata, A.; Ines, L. Central nervous system vasculitis in systemic lupus erythematosus: A case series report in a tertiary referral centre. Lupus 2017, 26, 1440–1447. [Google Scholar] [CrossRef]
- Abdel Razek, A.A.; Alvarez, H.; Bagg, S.; Refaat, S.; Castillo, M. Imaging spectrum of CNS vasculitis. Radiographics 2014, 34, 873–894. [Google Scholar] [CrossRef]
- Schwartz, N.; Stock, A.D.; Putterman, C. Neuropsychiatric lupus: New mechanistic insights and future treatment directions. Nat. Rev. Rheumatol. 2019, 15, 137–152. [Google Scholar] [CrossRef] [PubMed]
- Calle-Botero, E.; Abril, A. Lupus Vasculitis. Curr. Rheumatol. Rep. 2020, 22, 71. [Google Scholar] [CrossRef]
- Younger, D.S.; Coyle, P.K. Central Nervous System Vasculitis due to Infection. Neurol. Clin. 2019, 37, 441–463. [Google Scholar] [CrossRef]
- Govoni, M.; Bortoluzzi, A.; Padovan, M.; Silvagni, E.; Borrelli, M.; Donelli, F.; Ceruti, S.; Trotta, F. The diagnosis and clinical management of the neuropsychiatric manifestations of lupus. J. Autoimmun. 2016, 74, 41–72. [Google Scholar] [CrossRef]
- Kroner, P.T.; Tolaymat, O.A.; Bowman, A.W.; Abril, A.; Lacy, B.E. Gastrointestinal Manifestations of Rheumatological Diseases. Am. J. Gastroenterol. 2019, 114, 1441–1454. [Google Scholar] [CrossRef]
- Maruyama, A.; Nagashima, T.; Iwamoto, M.; Minota, S. Clinical characteristics of lupus enteritis in Japanese patients: The large intestine-dominant type has features of intestinal pseudo-obstruction. Lupus 2018, 27, 1661–1669. [Google Scholar] [CrossRef]
- Ju, J.H.; Min, J.K.; Jung, C.K.; Oh, S.N.; Kwok, S.K.; Kang, K.Y.; Park, K.S.; Ko, H.J.; Yoon, C.H.; Park, S.H.; et al. Lupus mesenteric vasculitis can cause acute abdominal pain in patients with SLE. Nat. Rev. Rheumatol. 2009, 5, 273–281. [Google Scholar] [CrossRef]
- Janssens, P.; Arnaud, L.; Galicier, L.; Mathian, A.; Hie, M.; Sene, D.; Haroche, J.; Veyssier-Belot, C.; Huynh-Charlier, I.; Grenier, P.A.; et al. Lupus enteritis: From clinical findings to therapeutic management. Orphanet J. Rare Dis. 2013, 8, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calamia, K.T.; Balabanova, M. Vasculitis in systemic lupus erythematosis. Clin. Dermatol. 2004, 22, 148–156. [Google Scholar] [CrossRef]
- Brewer, B.N.; Kamen, D.L. Gastrointestinal and Hepatic Disease in Systemic Lupus Erythematosus. Rheum. Dis. Clin. N. Am. 2018, 44, 165–175. [Google Scholar] [CrossRef]
- Yuan, S.; Ye, Y.; Chen, D.; Qiu, Q.; Zhan, Z.; Lian, F.; Li, H.; Liang, L.; Xu, H.; Yang, X. Lupus mesenteric vasculitis: Clinical features and associated factors for the recurrence and prognosis of disease. Semin. Arthritis Rheum. 2014, 43, 759–766. [Google Scholar] [CrossRef]
- Lee, C.K.; Ahn, M.S.; Lee, E.Y.; Shin, J.H.; Cho, Y.S.; Ha, H.K.; Yoo, B.; Moon, H.B. Acute abdominal pain in systemic lupus erythematosus: Focus on lupus enteritis (gastrointestinal vasculitis). Ann. Rheum. Dis. 2002, 61, 547–550. [Google Scholar] [CrossRef]
- Xu, D.; Lin, J. Urinary tract involvement in systemic lupus erythematosus: Coexistence with lupus mesenteric vasculitis or intestinal pseudo-obstruction? Semin. Arthritis Rheum. 2015, 44, e9. [Google Scholar] [CrossRef] [PubMed]
- Koo, B.S.; Hong, S.; Kim, Y.J.; Kim, Y.G.; Lee, C.K.; Yoo, B. Lupus enteritis: Clinical characteristics and predictive factors for recurrence. Lupus 2015, 24, 628–632. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.S.; Huang, I.F.; Feng, W.B.; Chiou, Y.H. Recurrent lupus mesenteric vasculitis leading to gastrointestinal perforation and sepsis. Kaohsiung J. Med. Sci. 2015, 31, 440–441. [Google Scholar] [CrossRef] [Green Version]
- Kwok, S.K.; Seo, S.H.; Ju, J.H.; Park, K.S.; Yoon, C.H.; Kim, W.U.; Min, J.K.; Park, S.H.; Cho, C.S.; Kim, H.Y. Lupus enteritis: Clinical characteristics, risk factor for relapse and association with anti-endothelial cell antibody. Lupus 2007, 16, 803–809. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, T.; Kobayashi, S.; Shimizu, H.; Nakajima, M.; Watanabe, S.; Kitami, N.; Sato, N.; Abe, H.; Aoki, Y.; Hoshi, T.; et al. The liver in collagen diseases: Pathologic study of 160 cases with particular reference to hepatic arteritis, primary biliary cirrhosis, autoimmune hepatitis and nodular regenerative hyperplasia of the liver. Liver 2000, 20, 366–373. [Google Scholar] [CrossRef]
- Matsumoto, T.; Yoshimine, T.; Shimouchi, K.; Shiotu, H.; Kuwabara, N.; Fukuda, Y.; Hoshi, T. The liver in systemic lupus erythematosus: Pathologic analysis of 52 cases and review of Japanese Autopsy Registry Data. Hum. Pathol. 1992, 23, 1151–1158. [Google Scholar] [CrossRef]
- Alanazi, T.; Alqahtani, M.; Al Duraihim, H.; Al Khathlan, K.; Al Ahmari, B.; Makanjuola, D.; Afzal, M. Hepatic vasculitis mimicking liver abscesses in a patient with systemic lupus erythematosus. Ann. Saudi Med. 2009, 29, 474–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levitin, P.M.; Sweet, D.; Brunner, C.M.; Katholi, R.E.; Bolton, W.K. Spontaneous rupture of the liver. An unusual complication of SLE. Arthritis Rheum. 1977, 20, 748–750. [Google Scholar] [CrossRef]
- Trambert, J.; Reinitz, E.; Buchbinder, S. Ruptured hepatic artery aneurysms in a patient with systemic lupus erythematosus: Case report. Cardiovasc. Interv. Radiol. 1989, 12, 32–34. [Google Scholar] [CrossRef]
- Nesher, G.; Breuer, G.S.; Temprano, K.; Moore, T.L.; Dahan, D.; Baer, A.; Alberton, J.; Izbicki, G.; Hersch, M. Lupus-associated pancreatitis. Semin. Arthritis Rheum. 2006, 35, 260–267. [Google Scholar] [CrossRef]
- Fessler, B.J.; Hoffman, G.S. Vasculitis. In Systemic Lupus Erythematosus, 5th ed.; Lahita, R.G., Ed.; Academic Press: Cambridge, MA, USA, 2011; pp. 833–845. [Google Scholar]
- Ding, Y.; Tan, Y.; Qu, Z.; Yu, F. Renal microvascular lesions in lupus nephritis. Ren. Fail. 2020, 42, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.H.; Yu, F.; Tan, Y.; Qu, Z.; Chen, M.H.; Wang, S.X.; Liu, G.; Zhao, M.H. Inclusion of renal vascular lesions in the 2003 ISN/RPS system for classifying lupus nephritis improves renal outcome predictions. Kidney Int. 2013, 83, 715–723. [Google Scholar] [CrossRef] [Green Version]
- Banfi, G.; Bertani, T.; Boeri, V.; Faraggiana, T.; Mazzucco, G.; Monga, G.; Sacchi, G. Renal vascular lesions as a marker of poor prognosis in patients with lupus nephritis. Gruppo Italiano per lo Studio della Nefrite Lupica (GISNEL). Am. J. Kidney Dis. 1991, 2, 240–248. [Google Scholar] [CrossRef]
- Descombes, E.; Droz, D.; Drouet, L.; Grünfeld, J.P.; Lesavre, P. Renal vascular lesions in lupus nephritis. Medicine (Baltimore) 1997, 5, 355–368. [Google Scholar] [CrossRef] [PubMed]
- Broder, A.; Mowrey, W.B.; Khan, H.N.; Jovanovic, B.; Londono-Jimenez, A.; Izmirly, P.; Putterman, C. Tubulointerstitial damage predicts end stage renal disease in lupus nephritis with preserved to moderately impaired renal function: A retrospective cohort study. Semin. Arthritis Rheum. 2018, 47, 545–551. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Han, S.S.; Qin, D.D.; Wu, L.H.; Song, Y.; Yu, F.; Wang, S.X.; Liu, G.; Zhao, M.H. Renal Interstitial Arteriosclerotic Lesions in Lupus Nephritis Patients: A Cohort Study from China. PLoS ONE 2015, 10, e0141547. [Google Scholar] [CrossRef]
- Leatherwood, C.; Speyer, C.B.; Feldman, C.H.; D’Silva, K.; Gomez-Puerta, J.A.; Hoover, P.J.; Waikar, S.S.; McMahon, G.M.; Rennke, H.G.; Costenbader, K.H. Clinical characteristics and renal prognosis associated with interstitial fibrosis and tubular atrophy (IFTA) and vascular injury in lupus nephritis biopsies. Semin. Arthritis Rheum. 2019, 49, 396–404. [Google Scholar] [CrossRef] [PubMed]
- Barber, C.; Herzenberg, A.; Aghdassi, E.; Su, J.; Lou, W.; Qian, G.; Yip, J.; Nasr, S.H.; Thomas, D.; Scholey, J.W.; et al. Evaluation of clinical outcomes and renal vascular pathology among patients with lupus. Clin. J. Am. Soc. Nephrol. 2012, 7, 757–764. [Google Scholar] [CrossRef] [Green Version]
- Abdellatif, A.A.; Waris, S.; Lakhani, A.; Kadikoy, H.; Haque, W.; Truong, L.D. True vasculitis in lupus nephritis. Clin. Nephrol. 2010, 74, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Nag, T.C.; Wadhwa, S. Vascular changes of the retina and choroid in systemic lupus erythematosus: Pathology and pathogenesis. Curr. Neurovasc. Res. 2006, 2, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Chin, D.; Gan, N.Y.; Holder, G.E.; Tien, M.; Agrawal, R.; Manghani, M. Severe retinal vasculitis in systemic lupus erythematosus leading to vision threatening paracentral acute middle maculopathy. Mod. Rheumatol. Case Rep. 2021, 5, 265–271. [Google Scholar] [CrossRef]
- Butendieck, R.R.; Parikh, K.; Stewart, M.; Davidge-Pitts, C.; Abril, A. Systemic lupus erythematosus-associated retinal vasculitis. J. Rheumatol. 2012, 39, 1095–1096. [Google Scholar] [CrossRef] [Green Version]
- Androudi, S.; Dastiridou, A.; Symeonidis, C.; Kump, L.; Praidou, A.; Brazitikos, P.; Kurup, S.K. Retinal vasculitis in rheumatic diseases: An unseen burden. Clin. Rheumatol. 2013, 32, 7–13. [Google Scholar] [CrossRef]
- Caracciolo, E.A.; Marcu, C.B.; Ghantous, A.; Donohue, T.J.; Hutchinson, G. Coronary vasculitis with acute myocardial infarction in a young woman with systemic lupus erythematosus. J. Clin. Rheumatol. 2004, 10, 66–68. [Google Scholar] [CrossRef]
- Sokalski, D.G.; Copsey Spring, T.R.; Roberts, W.N. Large artery inflammation in systemic lupus erythematosus. Lupus 2013, 22, 953–956. [Google Scholar] [CrossRef]
- Nasser, M.; Cottin, V. Alveolar Hemorrhage in Vasculitis (Primary and Secondary). Semin. Respir. Crit. Care Med. 2018, 39, 482–493. [Google Scholar] [CrossRef]
- Wang, C.R.; Liu, M.F.; Weng, C.T.; Lin, W.C.; Li, W.T.; Tsai, H.W. Systemic lupus erythematosus-associated diffuse alveolar haemorrhage: A single-centre experience in Han Chinese patients. Scand. J. Rheumatol. 2018, 47, 392–399. [Google Scholar] [CrossRef]
- Schwab, E.P.; Schumacher, H.R., Jr.; Freundlich, B.; Callegari, P.E. Pulmonary alveolar hemorrhage in systemic lupus erythematosus. Semin. Arthritis Rheum. 1993, 23, 8–15. [Google Scholar] [CrossRef]
- Rocca, P.V.; Siegel, L.B.; Cupps, T.R. The concomitant expression of vasculitis and coagulopathy: Synergy for marked tissue ischemia. J. Rheumatol. 1994, 3, 556–560. [Google Scholar]
- Alarcón-Segovia, D.; Pérez-Vázquez, M.E.; Villa, A.R.; Drenkard, C.; Cabiedes, J. Preliminary classification criteria for the antiphospholipid syndrome within systemic lupus erythematosus. Semin. Arthritis Rheum. 1992, 5, 275–286. [Google Scholar] [CrossRef]
- Cervera, R.; Piette, J.; Font, J.; Khamashta, M.A.; Shoenfeld, Y.; Camps, M.T.; Jacobsen, S.; Lakos, G.; Tincani, A.; Ingelmo, M.; et al. Antiphospholipid syndrome: Clinical and immunologic manifestations and patterns of disease expression in a cohort of 1000 patients. Arthritis Rheum. 2002, 4, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, V.A.; Gotwald, T.; Prior, C.; Oberrnoser, G.; Sepp, N. Acute pulmonary edema, capillaritis and alveolar hemorrhage: Pulmonary manifestations coexistent in antiphospholipid syndrome and systemic lupus erythematosus? Lupus 2005, 14, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Kazzaz, N.M.; Coit, P.; Lewis, E.E.; McCune, W.J.; Sawalha, A.H.; Knight, J.S. Systemic lupus erythematosus complicated by diffuse alveolar haemorrhage: Risk factors, therapy and survival. Lupus Sci. Med. 2015, 2, e000117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrade, C.; Mendonça, T.; Farinha, F.; Correia, J.; Marinho, A.; Almeida, I.; Vasconcelos, C. Alveolar hemorrhage in systemic lupus erythematosus: A cohort review. Lupus 2016, 25, 75–80. [Google Scholar] [CrossRef]
- Moss, K.E.; Isenberg, D.A. Comparison of renal disease severity and outcome in patients with primary antiphospholipid syndrome, antiphospholipid syndrome secondary to systemic lupus erythematosus (SLE) and SLE alone. Rheumatology (Oxford) 2001, 40, 863–867. [Google Scholar] [CrossRef] [Green Version]
- Barile-Fabris, L.; Ariza-Andraca, R.; Olguin-Ortega, L.; Jara, L.J.; Fraga-Mouret, A.; Miranda-Limon, J.M.; Fuentes de la Mata, J.; Clark, P.; Vargas, F.; Alocer-Varela, J. Controlled clinical trial of IV cyclophosphamide versus IV methylprednisolone in severe neurological manifestations in systemic lupus erythematosus. Ann. Rheum. Dis. 2005, 64, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Barile, L.A.; Jara, L.J.; Medina-Rodriguez, F.; Garcia-Figueroa, J.L.; Miranda-Limon, J.M. Pulmonary hemorrhage in systemic lupus erythematosus. Lupus 1997, 6, 445–448. [Google Scholar] [CrossRef]
- Micheletti, R.G.; Pagnoux, C. Management of cutaneous vasculitis. Presse Med. 2020, 49, 104033. [Google Scholar] [CrossRef] [PubMed]
- Lopez, L.R.; Davis, K.C.; Kohler, P.F.; Schocket, A.L. The hypocomplementemic urticarial-vasculitis syndrome: Therapeutic response to hydroxychloroquine. J. Allergy Clin. Immunol. 1984, 73, 600–603. [Google Scholar] [CrossRef]
- Callen, J.P. Colchicine is effective in controlling chronic cutaneous leukocytoclastic vasculitis. J. Am. Acad. Dermatol. 1985, 13, 193–200. [Google Scholar] [CrossRef]
- Callen, J.P.; af Ekenstam, E. Cutaneous leukocytoclastic vasculitis: Clinical experience in 44 patients. South Med. J. 1987, 80, 848–851. [Google Scholar] [CrossRef] [PubMed]
- Sais, G.; Vidaller, A.; Jucgla, A.; Gallardo, F.; Peyri, J. Colchicine in the treatment of cutaneous leukocytoclastic vasculitis. Results of a prospective, randomized controlled trial. Arch. Dermatol. 1995, 131, 1399–1402. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Chen, H.; Wang, S.; Zou, Y.; Li, J.; Pan, J.; Wang, X.; Ren, T.; Zhang, Y.; Chen, Z.; et al. Thalidomide treatment in cutaneous lesions of systemic lupus erythematosus: A multicenter study in China. Clin. Rheumatol. 2016, 35, 1521–1527. [Google Scholar] [CrossRef]
- Callen, J.P.; Spencer, L.V.; Burruss, J.B.; Holtman, J. Azathioprine. An effective, corticosteroid-sparing therapy for patients with recalcitrant cutaneous lupus erythematosus or with recalcitrant cutaneous leukocytoclastic vasculitis. Arch. Dermatol. 1991, 127, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Goodfield, M.; Davison, K.; Bowden, K. Intravenous immunoglobulin (IVIg) for therapy-resistant cutaneous lupus erythematosus (LE). J. Dermatolog. Treat 2004, 15, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Stumpf, M.A.M.; Quintino, C.R.; Rodrigues, M.; de Campos, F.P.F.; Maruta, C.W. Cutaneous vasculitis in lupus treated with IV immunoglobulin. Clin. Rheumatol. 2021, 40, 3023–3024. [Google Scholar] [CrossRef]
- Chung, L.; Funke, A.A.; Chakravarty, E.F.; Callen, J.P.; Fiorentino, D.F. Successful use of rituximab for cutaneous vasculitis. Arch. Dermatol. 2006, 142, 1407–1410. [Google Scholar] [CrossRef] [PubMed]
- Fotis, L.; Baszis, K.W.; French, A.R.; Cooper, M.A.; White, A.J. Mesenteric vasculitis in children with systemic lupus erythematosus. Clin. Rheumatol. 2016, 35, 785–793. [Google Scholar] [CrossRef]
- Liu, Y.; Zhu, J.; Lai, J.M.; Sun, X.F.; Hou, J.; Zhou, Z.X.; Yuan, X.Y. Reports of three cases with the initial presentation of mesenteric vasculitis in children with system lupus erythematous. Clin. Rheumatol. 2018, 37, 277–283. [Google Scholar] [CrossRef]
- Medina, F.; Ayala, A.; Jara, L.J.; Becerra, M.; Miranda, J.M.; Fraga, A. Acute abdomen in systemic lupus erythematosus: The importance of early laparotomy. Am. J. Med. 1997, 103, 100–105. [Google Scholar] [CrossRef]
- Narvaez, J.; Rios-Rodriguez, V.; de la Fuente, D.; Estrada, P.; Lopez-Vives, L.; Gomez-Vaquero, C.; Nolla, J.M. Rituximab therapy in refractory neuropsychiatric lupus: Current clinical evidence. Semin. Arthritis Rheum. 2011, 41, 364–372. [Google Scholar] [CrossRef]
- Jiang, Y.P.; Zhao, X.X.; Chen, R.R.; Xu, Z.H.; Wen, C.P.; Yu, J. Comparative efficacy and safety of mycophenolate mofetil and cyclophosphamide in the induction treatment of lupus nephritis: A systematic review and meta-analysis. Medicine (Baltimore) 2020, 99, e22328. [Google Scholar] [CrossRef]
- Tunnicliffe, D.J.; Palmer, S.C.; Henderson, L.; Masson, P.; Craig, J.C.; Tong, A.; Singh-Grewal, D.; Flanc, R.S.; Roberts, M.A.; Webster, A.C.; et al. Immunosuppressive treatment for proliferative lupus nephritis. Cochrane Database Syst. Rev. 2018, 6, CD002922. [Google Scholar] [CrossRef]
- Li, Q.Y.; Yu, F.; Zhou, F.D.; Zhao, M.H. Plasmapheresis Is Associated With Better Renal Outcomes in Lupus Nephritis Patients With Thrombotic Microangiopathy: A Case Series Study. Medicine (Baltimore) 2016, 95, e3595. [Google Scholar] [CrossRef]
- Stolyar, L.; Lahita, R.G.; Panush, R.S. Rituximab use as induction therapy for lupus nephritis: A systematic review. Lupus 2020, 29, 892–912. [Google Scholar] [CrossRef]
- De Holanda, M.I.; Porto, L.C.; Wagner, T.; Christiani, L.F.; Palma, L.M.P. Use of eculizumab in a systemic lupus erythemathosus patient presenting thrombotic microangiopathy and heterozygous deletion in CFHR1-CFHR3. A case report and systematic review. Clin. Rheumatol. 2017, 36, 2859–2867. [Google Scholar] [CrossRef] [PubMed]
- Aguirre-Valencia, D.; Naranjo-Escobar, J.; Posso-Osorio, I.; Macia-Mejia, M.C.; Nieto-Aristizabal, I.; Barrera, T.; Obando, M.A.; Tobon, G.J. Therapeutic Plasma Exchange as Management of Complicated Systemic Lupus Erythematosus and Other Autoimmune Diseases. Autoimmune Dis. 2019, 2019, 5350960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alabed, I.B. Treatment of diffuse alveolar hemorrhage in systemic lupus erythematosus patient with local pulmonary administration of factor VIIa (rFVIIa): A case report. Medicine (Baltimore) 2014, 93, e72. [Google Scholar] [CrossRef]
- Pais, F.; Fayed, M.; Evans, T. The Successful Use of Extracorporeal Membrane Oxygenation in Systemic Lupus Erythematosus-Induced Diffuse Alveolar Haemorrhage. Eur. J. Case Rep. Intern. Med. 2017, 4, 000515. [Google Scholar] [CrossRef] [Green Version]
- Shi, D.; Wang, D.; Li, X.; Zhang, H.; Che, N.; Lu, Z.; Sun, L. Allogeneic transplantation of umbilical cord-derived mesenchymal stem cells for diffuse alveolar hemorrhage in systemic lupus erythematosus. Clin. Rheumatol. 2012, 31, 841–846. [Google Scholar] [CrossRef]
- Ali Dhirani, N.; Ahluwalia, V.; Somani, S. Case of combination therapy to treat lupus retinal vasculitis refractory to steroids. Can. J. Ophthalmol. 2017, 52, e13–e15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damato, E.; Chilov, M.; Lee, R.; Singh, A.; Harper, S.; Dick, A. Plasma exchange and rituximab in the management of acute occlusive retinal vasculopathy secondary to systemic lupus erythematosus. Ocul. Immunol. Inflamm. 2011, 19, 379–381. [Google Scholar] [CrossRef]
- Hickman, R.A.; Denniston, A.K.; Yee, C.S.; Toescu, V.; Murray, P.I.; Gordon, C. Bilateral retinal vasculitis in a patient with systemic lupus erythematosus and its remission with rituximab therapy. Lupus 2010, 19, 327–329. [Google Scholar] [CrossRef] [PubMed]
- Papadaki, T.G.; Zacharopoulos, I.P.; Papaliodis, G.; Iaccheri, B.; Fiore, T.; Foster, C.S. Plasmapheresis for lupus retinal vasculitis. Arch. Ophthalmol. 2006, 124, 1654–1656. [Google Scholar] [CrossRef] [Green Version]
- Donnithorne, K.J.; Read, R.W.; Lowe, R.; Weiser, P.; Cron, R.Q.; Beukelman, T. Retinal vasculitis in two pediatric patients with systemic lupus erythematosus: A case report. Pediatr. Rheumatol. Online J. 2013, 11, 25. [Google Scholar] [CrossRef] [Green Version]
- Shriki, J.; Shinbane, J.S.; Azadi, N.; Su, T.I.; Hirschbein, J.; Quismorio, F.P., Jr.; Bhargava, P. Systemic lupus erythematosus coronary vasculitis demonstrated on cardiac computed tomography. Curr. Probl. Diagn. Radiol. 2014, 43, 294–297. [Google Scholar] [CrossRef] [PubMed]
- Nandkeolyar, S.; Kim, H.B.; Doctorian, T.; Stoletniy, L.N.; Sandhu, V.K.; Yu, M.; Zuppan, C.W.; Razzouk, A.; Hilliard, A.; Parwani, P. A case report of heart transplant for ischaemic cardiomyopathy from lupus coronary vasculitis. Eur. Heart J. Case Rep. 2019, 3, 1–7. [Google Scholar] [CrossRef]
- Fanouriakis, A.; Kostopoulou, M.; Alunno, A.; Aringer, M.; Bajema, I.; Boletis, J.N.; Cervera, R.; Doria, A.; Gordon, C.; Govoni, M.; et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann. Rheum. Dis. 2019, 78, 736–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uthman, I. Pharmacological therapy of vasculitis: An update. Curr. Opin. Pharmacol. 2004, 4, 177–182. [Google Scholar] [CrossRef]
- Yang, L.; Zeng, Y.P. Cutaneous Vasculitis in Systemic Lupus Erythematosus. JAMA Dermatol. 2021, 157, 991. [Google Scholar] [CrossRef] [PubMed]
- Guttman-Yassky, E.; Brunner, P.M.; Neumann, A.U.; Khattri, S.; Pavel, A.B.; Malik, K.; Singer, G.K.; Baum, D.; Gilleaudeau, P.; Sullivan-Whalen, M.; et al. Efficacy and safety of fezakinumab (an IL-22 monoclonal antibody) in adults with moderate-to-severe atopic dermatitis inadequately controlled by conventional treatments: A randomized, double-blind, phase 2a trial. J. Am. Acad. Dermatol. 2018, 78, 872–881 e876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papp, K.A.; Menter, M.A.; Raman, M.; Disch, D.; Schlichting, D.E.; Gaich, C.; Macias, W.; Zhang, X.; Janes, J.M. A randomized phase 2b trial of baricitinib, an oral Janus kinase (JAK) 1/JAK2 inhibitor, in patients with moderate-to-severe psoriasis. Br. J. Dermatol. 2016, 174, 1266–1276. [Google Scholar] [CrossRef]
- MacDonald, K.P.A.; Betts, B.C.; Couriel, D. Reprint of: Emerging Therapeutics for the Control of Chronic Graft-versus-Host Disease. Biol. Blood Marrow Transpl. 2018, 24, S7–S14. [Google Scholar] [CrossRef] [Green Version]
- Smith, E.M.D.; Lythgoe, H.; Hedrich, C.M. Vasculitis in Juvenile-Onset Systemic Lupus Erythematosus. Front. Pediatr. 2019, 7, 149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fontana, F.; Alfano, G.; Cappelli, G. The treatment of lupus nephritis, between consolidated strategies and new therapeutic options: A narrative review. G Ital. Nefrol. 2021, 38. [Google Scholar]
- El-Husseini, A.; Hannan, S.; Awad, A.; Jennings, S.; Cornea, V.; Sawaya, B.P. Thrombotic microangiopathy in systemic lupus erythematosus: Efficacy of eculizumab. Am. J. Kidney Dis. 2015, 65, 127–130. [Google Scholar] [CrossRef]
- Dooley, M.A.; Houssiau, F.; Aranow, C.; D’Cruz, D.P.; Askanase, A.; Roth, D.A.; Zhong, Z.J.; Cooper, S.; Freimuth, W.W.; Ginzler, E.M.; et al. Effect of belimumab treatment on renal outcomes: Results from the phase 3 belimumab clinical trials in patients with SLE. Lupus 2013, 22, 63–72. [Google Scholar] [CrossRef]
- Lei, Y.; Loutan, J.; Anders, H.J. B-cell depletion or belimumab or voclosporin for lupus nephritis? Curr. Opin. Nephrol. Hypertens. 2021, 30, 237–244. [Google Scholar] [CrossRef]
- Rovin, B.H.; Teng, Y.K.O.; Ginzler, E.M.; Arriens, C.; Caster, D.J.; Romero-Diaz, J.; Gibson, K.; Kaplan, J.; Lisk, L.; Navarra, S.; et al. Efficacy and safety of voclosporin versus placebo for lupus nephritis (AURORA 1): A double-blind, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet 2021, 397, 2070–2080. [Google Scholar] [CrossRef]
- Al-Adhoubi, N.K.; Bystrom, J. Systemic lupus erythematosus and diffuse alveolar hemorrhage, etiology and novel treatment strategies. Lupus 2020, 29, 355–363. [Google Scholar] [CrossRef]
- Kim, D.; Choi, J.; Cho, S.K.; Choi, C.B.; Kim, T.H.; Jun, J.B.; Yoo, D.H.; Bae, S.C.; Sung, Y.K. Clinical characteristics and outcomes of diffuse alveolar hemorrhage in patients with systemic lupus erythematosus. Semin. Arthritis Rheum. 2017, 46, 782–787. [Google Scholar] [CrossRef] [PubMed]
- Luqmani, R.A. State of the art in the treatment of systemic vasculitides. Front. Immunol. 2014, 5, 471. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Uncomplicated vascular immune deposits | Immune deposits in the wall of small renal arteries without inflammation, necrosis, or thrombosis are more commonly associated with active glomerular proliferative forms of lupus nephritis. By the light microscopy examination of renal biopsy specimens, the normal histology is assessed. By immunofluorescence microscopy, staining for IgG, IgA, IgM, and various complement components (often C1q or C3) can be observed in the vessel wall. By electron microscopy, the deposits are electron dense, with a granular texture, and are most commonly observed below an intact vascular endothelium or within the basement membranes. |
| Arteriosclerosis | It is characterized by an increased arterial wall thickness and reduction of the vascular lumen due to fibrotic intimal thickening and replication of the internal elastic lamina. |
| Noninflammatory necrotizing vasculopathy | It may be considered a complication of more severe forms of immune complex deposition. The immune complex deposits can cause luminal narrowing or occlusion and are accompanied by necrotizing damage, frequently found in preglomerular arterioles and less in interlobular arteries. Abundant glassy eosinophilic materials may occupy the lumen and intima and, sometimes, may extend into the media. The endothelium is usually swollen or denuded, and the elastic membrane is often disrupted. The inflammatory infiltrate is rare. IgG, IgM, and IgA positivity can be detected by immunofluorescence microscopy in the vessel wall and in the lumen, as well as complement components and fibrin-related antigens. By electron microscopy, swelling or loss of the endothelium can be seen along with abundant intraluminal and mural deposits of granular electron-dense materials. |
| Thrombotic microangiopathy | It is most frequent in SLE patients with thrombotic thrombocytopenic purpura or anticardiolipin syndrome. In the early phase, there is swelling of the endothelial cells and subendothelial space. During the acute phase, a severe narrowing or total occlusion of the arteriolar lumen may be found. Fibrinoid necrosis may also be detect. The chronic phase presents swelling of the intima of the interlobular arteries associated with mucoid intimal edema and/or “onion skin” pattern lesions as result of the cellular intimal proliferation. By immunofluorescence microscopy, fibrinogen or fibrin in the walls of arterioles and small arteries can be observed, as well as IgM, IgG, IgA, C3, and C1q positivity. Electron microscopy may highlight the swelling and detachment of the endothelium from the underlying structures and an expanded intima. |
| True renal vasculitis | It is the least common renal lupus vascular lesion that usually involves small arteries, most commonly intralobular arteries. Histologically, it is indistinguishable from the polyarteritis nodosa. Morphologically, these lesions are characterized by neutrophils and mononuclear leukocytes that eccentrically or circumferentially infiltrate the intima and media. In the acute phase, this infiltration is often associated with fibrinoid necrosis and rupture of the elastic lamellae. Immunofluorescence reveals strong staining for fibrin-related antigens, with weak and variable staining for immunoglobulin and the complement. |
| Vascular Manifestation | Type of Study | No. of Patients | Treatment | % Response (or Remission) | Adverse Events | Ref. |
|---|---|---|---|---|---|---|
| Cutaneous | Case report | 1 | Hydroxychloroquine (200–400 mg/day) | 100 | N.R. | [98] |
| Case series | 13 | Colchicine (0.5–0.6 mg twice daily) | 69 | Mild (adominal cramping and diarrhea) | [99] | |
| Clinical experience | 10 | 70 | Mild | [100] | ||
| Prospective randomized controlled trial | 41 | 29 | Mild | [101] | ||
| Multicenter study | 69 | Thalidomide (50 mg/day) | 100 | Mild (drowsiness and constipation) | [102] | |
| Case series | 6 | Azathioprine (2 mg/kg/day) | 33 | Leukopenia, hepatic injury, hypersensitivity reaction, and infections | [103] | |
| Clinical trial | 12 | Immunoglobulin (1 g/kg for 2 consecutive days followed by 400 mg/kg monthly) | >75 | N.R | [104] | |
| Case report | 1 | Patient died from septic shock | [105] | |||
| Case series | 2 | Rituximab | 100 | N.R. | [106] | |
| Gastrointestinal | Retrospective cohort study | 97 | Cyclophosphamide (500–1000 mg/m2) and prednisone (>30 mg) Mycophenolate mofetil (2 g/day) Corticosteroid only | 84.5 | Severe adverse events occurred in 15 patients | [57] |
| Retrospective study | 38 | Methylprednisolone (1 mg/kg/day) | 100 | N.R. | [58] | |
| Case series | 5 | Cyclophosphamide and corticosteroids | 80 | N.R. | [107] | |
| Rituximab | 20 | |||||
| Case series | 3 | Methylprednisolone (20 mg/kg/day for 5 days) and cyclophosphamide (1 g/m2) | 100 | N.R. | [108] | |
| Case series | 19 | Methylprednisolone pulse therapy (1 g/day for 3 days), followed by cyclophosphamide (1 g/m2 intravenously) in 4 cases. | 90 | N.R. | [109] | |
| Nervous system | Controlled clinical trial | 32 | Cyclophosphamide (0.75 g/m2 monthly for 1 year and then every 3 months for another year). Methylprednisolone (1 g daily for 3 days, monthly for 4 months, then bimonthly for 6 months and subsequently every 3 months for 1 year) Oral prednisone on the fourth day of treatment (1 mg/kg/day) | 75 | Infections of the gastrointestinal, urinary and upper respiratory tract. Herpes zoster | [95] |
| Case report and review of 34 cases | 35 | Rituximab and concomitant treatment with corticosteroids, methylprednisolone, cyclophosphamide or azathioprine | 50 | Herpes zoster Infections | [110] | |
| Renal | Meta-analysis (18 studies) | 1989 | Mycophenolate mofetil and cyclophosphamide | N.R. | Infections | [111] |
| Meta-analysis (74 studies) | 5175 | High-dose steroids with cyclophosphamide or mycophenolate mofetil as induction therapy, and low-dose steroids combined with varying regimens of azathioprine or mycophenolate mofetil for the maintenance phase | N.R. | Diarrhea | [112] | |
| Retrospective study | 61 | Cyclophosphamide or mycophenolate mofetil in combination with glucocorticoids for the induction phase. Mycophenolate mofetil or azathioprine combined with low-dose glucocorticoid regimens for the maintence phase. | N.R. | No severe adverse events | [113] | |
| 9 | Plasmapheresis and baseline immunosuppressive therapy | 33 | None | |||
| Systematic review (31 studies) | 1259 | Rituximab alone or in combination with cyclophosphamide or mycophenolate mofetil | 77 Caucasian 38 East-Asian 28 Hispanic | N.R. | [114] | |
| Systematic review (15 studies) and case report | 20 | Eculizumab | 85 | N.R. | [115] | |
| Pulmonary | Case series | 16 | High-dose corticosteroid, followed by pulse methylprednisolone, plasmapheresis, pulse cyclophosphamide, and rituximab | N.R. | Infections | [86] |
| Case series | 34 | High dose of methylprednisolone (>3 g) and cyclophosphamide | N.R. | N.R. | [96] | |
| Retrospective clinical trials | 40 SLE (11 DHA) | Therapeutic plasma exchange | N.R. | Mild (bleeding) | [116] | |
| Case control study | 22 | Various combinations of corticosteroids, plasmapheresis, cyclophosphamide, rituximab, and mycophenolate mofetil. | N.R. | N.R. | [92] | |
| Case report | 1 | rFVIIa 75 μg/kg | N.R. | None | [117] | |
| Case report | 1 | Extracorporeal Membrane Oxygenation | N.R. | None | [118] | |
| Retrospective study | 4 | Umbilical cord-derived mesenchymal stem cell transplantation | N.R. | None | [119] | |
| Retinal | Case report | 1 | Plasmapheresis and the bilateral administration of intravitreal ranibizumab (0.5 mg) and rituximab | N.R. | None | [120] |
| Case report | 1 | Plasmapheresis, followed by rituximab and mycophenolate mofetil | 100 | None | [121] | |
| Case report | Rituximab (1 g) and cyclophosphamide (10 mg/kg) | 100 | None | [122] | ||
| Case series | 2 | Plasmapheresis, followed by a single intravenous infusion of cyclophosphamide (750 mg) Plasmapheresis and methotrexate (15 mg weekly) | N.R. | None | [123] | |
| Case series | 2 | Panretinal photocoagulation, rituximab (750 mg/m2 × 2 weeks), and cyclophosphamide (750 mg/m2 per dose) with a concurrent pulse of methylprednisolone (1000 mg) Methylprednisolone (1000 mg) plus rituximab (750 mg/m2 × 2 weeks) and monthly cyclophosphamide (750 mg/m2 × 7 months). | N.R. | N.R. | [124] | |
| Coronary | Case report | 1 | Prednisone (60 mg once a day) and cyclophosphamide (1300 mg monthly) | 100 | N.R. | [83] |
| Case report | 1 | Methylprednisolone (1 g) and cyclophosphamide (1 g) | 100 | N.R. | [125] | |
| Case report | 1 | Methylprednisolone 1000 mg daily for 3 days, followed by 1-mg/kg/day prednisone in addition to a single dose of intravenous cyclophosphamide 860 mg and oral hydroxychloroquine 400 mg daily. Orthotopic heart transplant | 0 | N.R. | [126] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leone, P.; Prete, M.; Malerba, E.; Bray, A.; Susca, N.; Ingravallo, G.; Racanelli, V. Lupus Vasculitis: An Overview. Biomedicines 2021, 9, 1626. https://doi.org/10.3390/biomedicines9111626
Leone P, Prete M, Malerba E, Bray A, Susca N, Ingravallo G, Racanelli V. Lupus Vasculitis: An Overview. Biomedicines. 2021; 9(11):1626. https://doi.org/10.3390/biomedicines9111626
Chicago/Turabian StyleLeone, Patrizia, Marcella Prete, Eleonora Malerba, Antonella Bray, Nicola Susca, Giuseppe Ingravallo, and Vito Racanelli. 2021. "Lupus Vasculitis: An Overview" Biomedicines 9, no. 11: 1626. https://doi.org/10.3390/biomedicines9111626