

T2-Low Asthma: A Discussed but Still Orphan Disease
 ,
,
Abstract
:1. Introduction
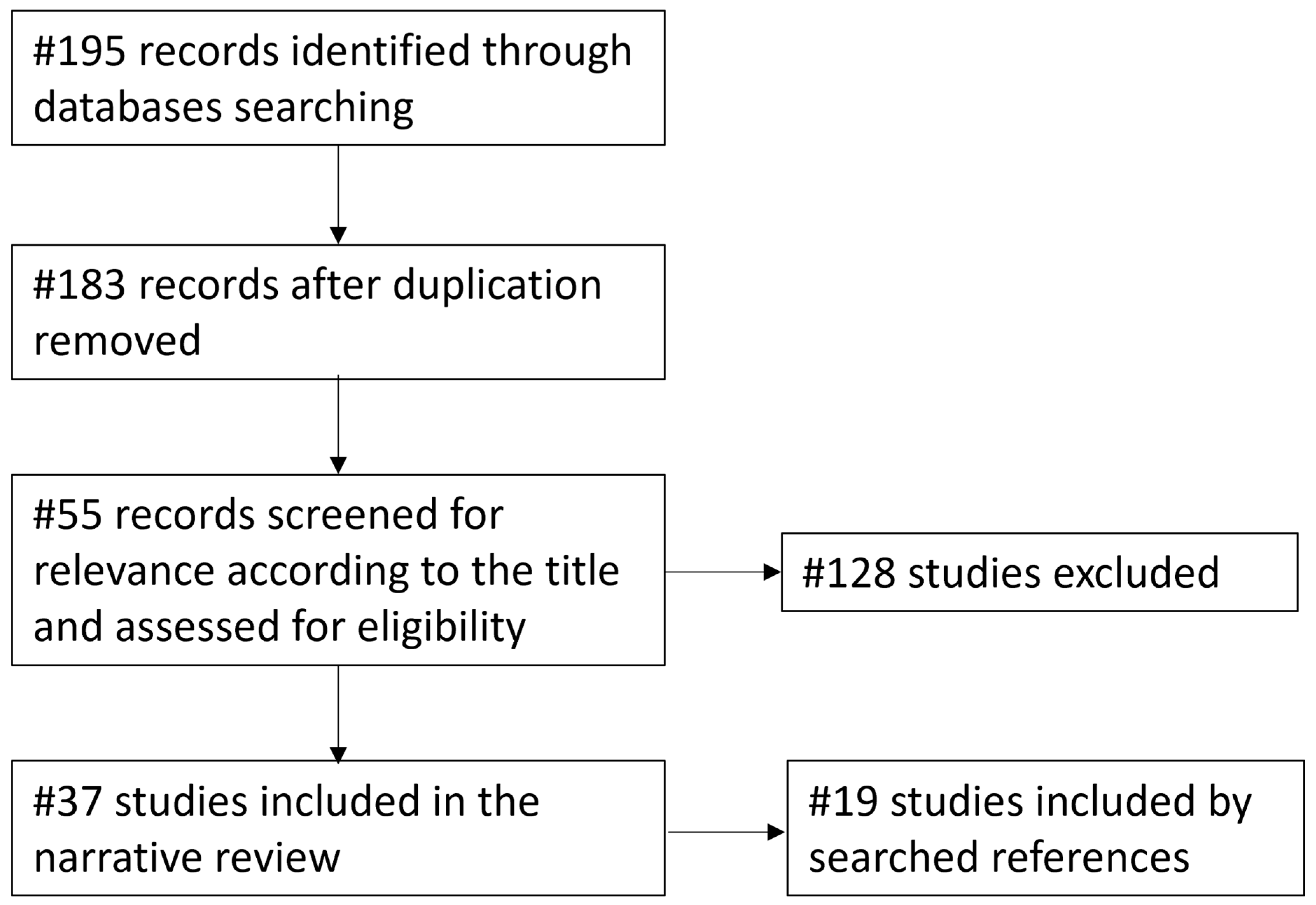
2. Search Strategy
3. Results
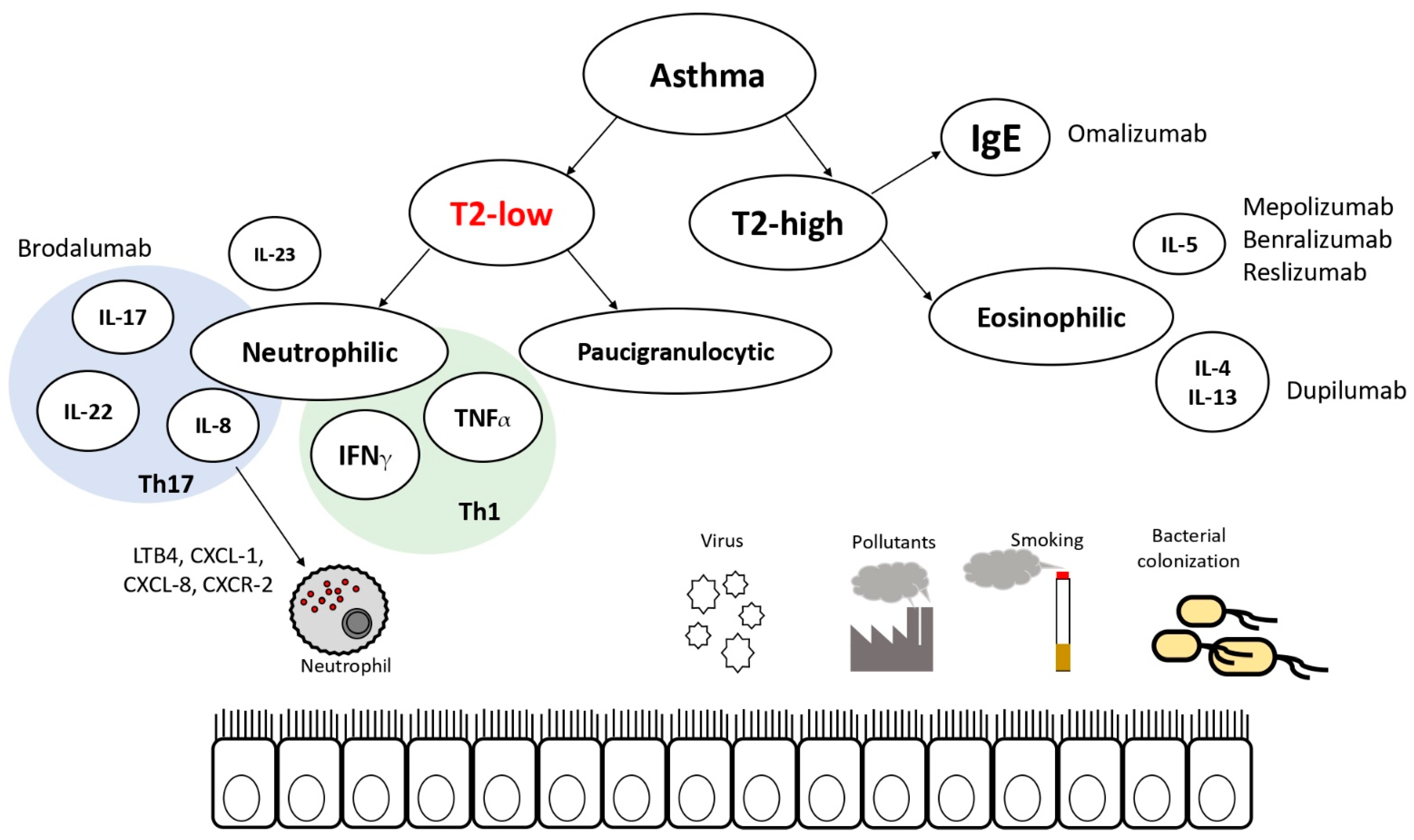
3.1. Markers and Molecular Pathways
3.2. Innate Lymphoid Cells’ Role in T2-Low Asthma
3.3. Neutrophilic Asthma
3.4. Paucigranulocytic Asthma
3.5. Mixed Granulocytic Asthma
3.6. Environmental Triggers
3.7. Clinical Phenotype
3.8. Pathogenes
3.9. Pediatric T2-Low Asthma
3.10. Therapies and Targets
Randomized Controlled Trials
3.11. Promising Drugs
3.12. Physical Therapy and Thermoplasty
3.13. Limits of the Available Evidence
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Papi, A.; Brightling, C.; Pedersen, S.E.; Reddel, H.K. Asthma. Lancet 2018, 391, 783–800. [Google Scholar] [CrossRef] [PubMed]
- Dharmage, S.C.; Perret, J.L.; Custovic, A. Epidemiology of Asthma in Children and Adults. Front. Pediatr. 2019, 1, 246. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Asthma a Gina Pocket Guide for Health Professionals Difficult-To-Treat & Severe Asthma in Adolescent and Adult Patients Diagnosis and Management A Gina Pocket Guide for Health Professionals Difficult-To-Treat & Severe Asthma in Adolescent and Adult Patients Diagnosis and Management. 2019. Available online: www.ginasthma.org (accessed on 9 March 2023).
- Drazen, J.M.; Israel, E.; Reddel, H.K. Severe and Difficult-to-Treat Asthma in Adults. N. Engl. J. Med. 2017, 10, 965–976. [Google Scholar] [CrossRef]
- Porcaro, F.; Ullmann, N.; Allegorico, A.; Di Marco, A.; Cutrera, R. Difficult and Severe Asthma in Children. Children 2020, 7, 286. [Google Scholar] [CrossRef] [PubMed]
- Ghirardo, S.; Mazzolai, M.; Di Marco, A.; Petreschi, F.; Ullmann, N.; Ciofi Degli Atti, M.L.; Cutrera, R. Biological Treatments and Target Therapies for Pediatric Respiratory Medicine: Not Only Asthma. Front. Pediatr. 2022, 10, 837667. [Google Scholar] [CrossRef]
- Brusselle, G.G.; Koppelman, G.H. Biologic Therapies for Severe Asthma. N. Engl. J. Med. 2022, 386, 157–171. [Google Scholar] [CrossRef]
- Sze, E.; Bhalla, A.; Nair, P. Mechanisms and therapeutic strategies for non-T2 asthma. Allergy 2019, 75, 311–325. [Google Scholar] [CrossRef]
- Aslam, A.; De Luis Cardenas, J.; Morrison, R.; Lagisetty, K.H.; Litmanovich, D. Tracheobronchomalacia and Excessive Dynamic Airway Collapse: Current Concepts and Future Directions. Radiographics 2022, 42, 1012–1027. [Google Scholar] [CrossRef]
- Orlova, G.; Surkova, E. Neutrophilic granule proteins in the occupational pulmonary diseases. Eur. Respir. J. 2013, 42 (Suppl. 57), 4254. [Google Scholar]
- Wenzel, S.E.; Barnes, P.J.; Bleecker, E.R.; Bousquet, J.; Busse, W.; Dahlén, S.E.; Holgate, S.T.; Meyers, D.A.; Rabe, K.F.; Antczak, A.; et al. A Randomized, Double-blind, Placebo-controlled Study of Tumor Necrosis Factor-α Blockade in Severe Persistent Asthma. Am. J. Respir. Crit. Care Med. 2009, 179, 549–558. [Google Scholar] [CrossRef]
- Holgate, S.T.; Noonan, M.; Chanez, P.; Busse, W.; Dupont, L.; Pavord, I.; Hakulinen, A.; Paolozzi, L.; Wajdula, J.; Zang, C.; et al. Efficacy and safety of etanercept in moderate-to-severe asthma: A randomised, controlled trial. Eur. Respir. J. 2011, 37, 1352–1359. [Google Scholar] [CrossRef] [PubMed]
- Niessen, N.M.; Gibson, P.G.; Baines, K.; Barker, D.; Yang, I.A.; Upham, J.W.; Reynolds, P.N.; Hodge, S.; James, A.L.; Jenkins, C.; et al. Sputum TNF markers are increased in neutrophilic and severe asthma and are reduced by azithromycin treatment. Allergy 2021, 76, 2090–2101. [Google Scholar] [CrossRef] [PubMed]
- Simpson, J.L.; Grissell, T.V.; Douwes, J.; Scott, R.J.; Boyle, M.J.; Gibson, P. Innate immune activation in neutrophilic asthma and bronchiectasis. Thorax 2007, 62, 211–218. [Google Scholar] [CrossRef]
- Nair, P.; Gaga, M.; Zervas, E.; Alagha, K.; Hargreave, F.E.; O’Byrne, P.M.; Stryszak, P.; Gann, L.; Sadeh, J.; Chanez, P. Safety and efficacy of a CXCR2 antagonist in patients with severe asthma and sputum neutrophils: A randomized, placebo-controlled clinical trial. Clin. Exp. Allergy 2012, 42, 1097–1103. [Google Scholar] [CrossRef] [PubMed]
- Leaker, B.R.; Barnes, P.J.; O’connor, B. Inhibition of LPS-Induced Airway Neutrophilic Inflammation in Healthy Volunteers with an Oral CXCR2 Antagonist. 2013. Available online: http://respiratory-research.com/content/14/1/137 (accessed on 9 March 2023).
- O’Byrne, P.M.; Metev, H.; Puu, M.; Richter, K.; Keen, C.; Uddin, M.; Larsson, B.; Cullberg, M.; Nair, P. Efficacy and safety of a CXCR2 antagonist, AZD5069, in patients with uncontrolled persistent asthma: A randomised, double-blind, placebo-controlled trial. Lancet Respir. Med. 2016, 4, 797–806. [Google Scholar] [CrossRef]
- Moore, W.C.; Hastie, A.T.; Li, X.; Li, H.; Busse, W.; Jarjour, N.N.; Wenzel, S.E.; Peters, S.P.; Meyers, D.A.; Bleecker, E.R.; et al. Sputum neutrophil counts are associated with more severe asthma phenotypes using cluster analysis. J. Allergy Clin. Immunol. 2013, 133, 1557–1563.e5. [Google Scholar] [CrossRef]
- Chaudhuri, R.; Norris, V.; Kelly, K.; Zhu, C.-Q.; Ambery, C.; Lafferty, J.; Cameron, E.; Thomson, N.C. Effects of a FLAP inhibitor, GSK2190915, in asthmatics with high sputum neutrophils. Pulm. Pharmacol. Ther. 2014, 27, 62–69. [Google Scholar] [CrossRef]
- Schleich, F.; Demarche, S.; Louis, R. Biomarkers in the Management of Difficult Asthma. Curr. Top. Med. Chem. 2016, 16, 1561–1573. [Google Scholar] [CrossRef]
- Simpson, J.L.; Scott, R.; Boyle, M.J.; Gibson, P.G. Inflammatory subtypes in asthma: Assessment and identification using induced sputum. Respirology 2006, 11, 54–61. [Google Scholar] [CrossRef]
- Kim, H.Y.; Umetsu, D.T.; Dekruyff, R.H. Innate lymphoid cells in asthma: Will they take your breath away? Eur. J. Immunol. 2016, 46, 795–806. [Google Scholar] [CrossRef]
- Lloyd, C.M. IL-33 family members and asthma-bridging innate and adaptive immune responses. Curr. Opin. Immunol. 2010, 22, 800–806. [Google Scholar] [CrossRef]
- Ham, J.; Lim, M.; Kim, D.; Kim, H.Y. Memory-like innate lymphoid cells in the pathogenesis of asthma. Front. Immunol. 2022, 13, 1005517. [Google Scholar] [CrossRef] [PubMed]
- Luci, C.; Vieira, E.; Perchet, T.; Gual, P.; Golub, R. Natural Killer Cells and Type 1 Innate Lymphoid Cells Are New Actors in Non-alcoholic Fatty Liver Disease. Front. Immunol. 2019, 10, 1192. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; Guo, X.; Huang, T.; Liu, C. The Role of Group 3 Innate Lymphoid Cells in Lung Infection and Immunity. Front. Cell. Infect. Microbiol. 2021, 11, 586471. [Google Scholar] [CrossRef] [PubMed]
- Vivier, E.; Artis, D.; Colonna, M.; Diefenbach, A.; Di Santo, J.P.; Eberl, G.; Koyasu, S.; Locksley, R.M.; McKenzie, A.N.J.; Mebius, R.E.; et al. Innate Lymphoid Cells: 10 Years on. Cell 2018, 174, 1054–1066. [Google Scholar] [CrossRef] [PubMed]
- Schleich, F.N.; Manise, M.; Sele, J.; Henket, M.; Seidel, L.; Louis, R. Distribution of sputum cellular phenotype in a large asthma cohort: Predicting factors for eosinophilic vs neutrophilic inflammation. BMC Pulm. Med. 2013, 13, 11. [Google Scholar] [CrossRef] [PubMed]
- Nair, P.; Aziz-Ur-Rehman, A.; Radford, K. Therapeutic implications of ‘neutrophilic asthma’. Curr. Opin. Pulm. Med. 2015, 21, 33–38. [Google Scholar] [CrossRef]
- Sabroe, I.; Lloyd, C.; Whyte, M.K.B.; Dower, S.K.; Williams, T.J.; Pease, J. Chemokines, innate and adaptive immunity, and respiratory disease. Eur. Respir. J. 2002, 19, 350–355. [Google Scholar] [CrossRef]
- Chung, K.F. Neutrophilic asthma: A distinct target for treatment? Lancet Respir. Med. 2016, 4, 765–767. [Google Scholar] [CrossRef]
- De Volder, J.; Vereecke, L.; Joos, G.; Maes, T. Targeting neutrophils in asthma: A therapeutic opportunity? Biochem. Pharmacol. 2020, 182, 114292. [Google Scholar] [CrossRef]
- Crisford, H.; Sapey, E.; Geraint, R.; Taylor, S.; Nagakumar, P.; Lokwani, R.; Simpson, J.L. Neutrophils in asthma: The good, the bad and the bacteria. Thorax 2021, 76, 835–844. [Google Scholar] [CrossRef] [PubMed]
- Cowan, D.C.; Cowan, J.O.; Palmay, R.; Williamson, A.; Taylor, D.R. Effects of steroid therapy on inflammatory cell subtypes in asthma. Thorax 2010, 65, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Saffar, A.S.; Ashdown, H.; Gounni, A.S. The Molecular Mechanisms of Glucocorticoids-Mediated Neutrophil Survival. Curr. Drug Targets 2011, 12, 556–562. [Google Scholar] [CrossRef]
- Berry, M.; Morgan, A.; Shaw, D.E.; Parker, D.; Green, R.; Brightling, C.; Bradding, P.; Wardlaw, A.J.; Pavord, I.D. Pathological features and inhaled corticosteroid response of eosinophilic and non-eosinophilic asthma. Thorax 2007, 62, 1043–1049. [Google Scholar] [CrossRef]
- Shimoda, T.; Obase, Y.; Nagasaka, Y.; Nakano, H.; Kishikawa, R.; Iwanaga, T. Airway inflammation phenotype prediction in asthma patients using lung sound analysis with fractional exhaled nitric oxide. Allergol. Int. 2017, 66, 581–585. [Google Scholar] [CrossRef]
- Shaw, D.E.; Berry, M.A.; Hargadon, B.; McKenna, S.; Shelley, M.J.; Green, R.H.; Brightling, C.E.; Wardlaw, A.J.; Pavord, I.D. Association Between Neutrophilic Airway Inflammation and Airflow Limitation in Adults With Asthma. Chest 2007, 132, 1871–1875. [Google Scholar] [CrossRef]
- Tliba, O.; Panettieri, R.A., Jr. Paucigranulocytic asthma: Uncoupling of airway obstruction from inflammation. J. Allergy Clin. Immunol. 2019, 143, 1287–1294. [Google Scholar] [CrossRef] [PubMed]
- Prakash, Y.S. Airway smooth muscle in airway reactivity and remodeling: What have we learned? Am. J. Physiol. Cell. Mol. Physiol. 2013, 305, L912–L933. [Google Scholar] [CrossRef]
- Braun, A.; Quarcoo, D.; Schulte-Herbrüggen, O.; Lommatzsch, M.; Hoyle, G.; Renz, H. Nerve Growth Factor Induces Airway Hyperresponsiveness in Mice. Int. Arch. Allergy Immunol. 2001, 124, 205–207. [Google Scholar] [CrossRef]
- Frossard, N.; Freund, V.; Advenier, C. Nerve growth factor and its receptors in asthma and inflammation. Eur. J. Pharmacol. 2004, 500, 453–465. [Google Scholar] [CrossRef]
- Demarche, S.; Schleich, F.; Henket, M.; Paulus, V.; Van Hees, T.; Louis, R. Detailed analysis of sputum and systemic inflammation in asthma phenotypes: Are paucigranulocytic asthmatics really non-inflammatory? BMC Pulm. Med. 2016, 16, 46. [Google Scholar] [CrossRef]
- Pignatti, P.; Visca, D.; Cherubino, F.; Zampogna, E.; Saderi, L.; Zappa, M.; Sotgiu, G.; Spanevello, A. Mixed granulocytic phenotype in asthmatic patients. Eur. Respir. J. 2019, 54 (Suppl. S63), PA2587. [Google Scholar] [CrossRef]
- Kuruvilla, M.E.; Lee, F.E.-H.; Lee, G.B. Understanding Asthma Phenotypes, Endotypes, and Mechanisms of Disease. Clin. Rev. Allergy Immunol. 2018, 56, 219–233. [Google Scholar] [CrossRef]
- Alexis, N.E.; Carlsten, C. Interplay of air pollution and asthma immunopathogenesis: A focused review of diesel exhaust and ozone. Int. Immunopharmacol. 2014, 23, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Spears, M.; McSharry, C.; Chaudhuri, R.; Weir, C.J.; De Wet, C.; Thomson, N.C. Smoking in Asthma Is Associated with Elevated Levels of Corticosteroid Resistant Sputum Cytokines—An Exploratory Study. PLoS ONE 2013, 8, e71460. [Google Scholar] [CrossRef]
- Williams, E.J.; Negewo, N.A.; Baines, K.J. Role of the NLRP3 inflammasome in asthma: Relationship with neutrophilic inflammation, obesity, and therapeutic options. J. Allergy Clin. Immunol. 2021, 147, 2060–2062. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, S.C.; Chinchilli, V.M.; Rollings, N.J.; Boushey, H.A.; Cherniack, R.; Craig, T.J.; Deykin, A.; DiMango, E.; Fish, J.E.; Ford, J.G.; et al. Smoking Affects Response to Inhaled Corticosteroids or Leukotriene Receptor Antagonists in Asthma. Am. J. Respir. Crit. Care Med. 2007, 175, 783–790. [Google Scholar] [CrossRef]
- Hinks, T.S.; Levine, S.J.; Brusselle, G.G. Treatment options in type-2 low asthma. Eur. Respir. J. 2020, 57, 2000528. [Google Scholar] [CrossRef]
- Fitzpatrick, A.M.; Chipps, B.E.; Holguin, F.; Woodruff, P.G. T2-“Low” Asthma: Overview and Management Strategies. J. Allergy Clin. Immunol. Pract. 2020, 8, 452–463. [Google Scholar] [CrossRef]
- Bullone, M.; Carriero, V.; Bertolini, F.; Folino, A.; Mannelli, A.; Di Stefano, A.; Gnemmi, I.; Torchio, R.; Ricciardolo, F.L.M. Elevated serum IgE, oral corticosteroid dependence and IL-17/22 expression in highly neutrophilic asthma. Eur. Respir. J. 2019, 54, 1900068. [Google Scholar] [CrossRef]
- Telenga, E.D.; Tideman, S.W.; Kerstjens, H.A.M.; Ten Hacken, N.H.T.; Timens, W.; Postma, D.S.; van den Berge, M. Obesity in asthma: More neutrophilic inflammation as a possible explanation for a reduced treatment response. Allergy 2012, 67, 1060–1068. [Google Scholar] [CrossRef] [PubMed]
- Wood, L.G.; Li, Q.; Scott, H.A.; Rutting, S.; Berthon, B.; Gibson, P.G.; Hansbro, P.M.; Williams, E.; Horvat, J.; Simpson, J.L.; et al. Saturated fatty acids, obesity, and the nucleotide oligomerization domain–like receptor protein 3 (NLRP3) inflammasome in asthmatic patients. J. Allergy Clin. Immunol. 2018, 143, 305–315. [Google Scholar] [CrossRef]
- Fu, J.-J.; Baines, K.J.; Wood, L.; Gibson, P. Systemic Inflammation Is Associated with Differential Gene Expression and Airway Neutrophilia in Asthma. OMICS A J. Integr. Biol. 2013, 17, 187–199. [Google Scholar] [CrossRef] [PubMed]
- Alhamdan, F.; Marsh, L.M.; Pedersen, F.; Alhamwe, B.A.; Thölken, C.; Pfefferle, P.; Bahmer, T.; Greulich, T.; Potaczek, D.P.; Garn, H. Differential Regulation of Interferon Signaling Pathways in CD4+ T Cells of the Low Type-2 Obesity-Associated Asthma Phenotype. Int. J. Mol. Sci. 2021, 22, 10144. [Google Scholar] [CrossRef]
- Cardet, J.C.; Ash, S.; Kusa, T.; Camargo, C.A.; Israel, E. Insulin resistance modifies the association between obesity and current asthma in adults. Eur. Respir. J. 2016, 48, 403–410. [Google Scholar] [CrossRef]
- Gibson, P.G.; McDonald, V.M.; Marks, G.B. Asthma in older adults. Lancet 2010, 376, 803–813. [Google Scholar] [CrossRef]
- Dunn, R.M.; Busse, P.J.; Wechsler, M.E. Asthma in the elderly and late-onset adult asthma. Allergy 2017, 73, 284–294. [Google Scholar] [CrossRef]
- Schmitt, V.; Rink, L.; Uciechowski, P. The Th17/Treg balance is disturbed during aging. Exp. Gerontol. 2013, 48, 1379–1386. [Google Scholar] [CrossRef] [PubMed]
- Nyenhuis, S.M.; Schwantes, E.A.; Evans, M.D.; Mathur, S.K. Airway neutrophil inflammatory phenotype in older subjects with asthma. J. Allergy Clin. Immunol. 2010, 125, 1163–1165. [Google Scholar] [CrossRef]
- Tattersfield, A.E.; Postma, D.S.; Barnes, P.J.; Svensson, K.; Bauer, C.; O’Byrne, P.M.; Lofdahl, C.; Pauwels, R.A.; Ullman, A. Exacerbations of Asthma. Am. J. Respir. Crit. Care Med. 1999, 160, 594–599. [Google Scholar] [CrossRef]
- Abdel-Aziz, M.I.; Brinkman, P.; Vijverberg, S.J.H.; Neerincx, A.H.; Riley, J.H.; Bates, S.; Hashimoto, S.; Kermani, N.Z.; Chung, K.F. Djukanovic, R.; et al. Sputum microbiome profiles identify severe asthma phenotypes of relative stability at 12 to 18 months. J. Allergy Clin. Immunol. 2021, 147, 123–134. [Google Scholar] [CrossRef]
- Green, B.J.; Wiriyachaiporn, S.; Grainge, C.; Rogers, G.B.; Kehagia, V.; Lau, L.; Carroll, M.P.; Bruce, K.D.; Howarth, P.H. Potentially Pathogenic Airway Bacteria and Neutrophilic Inflammation in Treatment Resistant Severe Asthma. PLoS ONE 2014, 9, e100645. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Jiang, Y.; Wang, C. Does IL-17 Respond to the Disordered Lung Microbiome and Contribute to the Neutrophilic Phenotype in Asthma? Mediat. Inflamm. 2016, 2016, 6470364. [Google Scholar] [CrossRef]
- Gallucci, M.; Pedretti, M.; Giannetti, A.; di Palmo, E.; Bertelli, L.; Pession, A.; Ricci, G. When the Cough Does Not Improve: A Review on Protracted Bacterial Bronchitis in Children. Front. Pediatr. 2020, 8, 433. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; He, X.Y.; Baines, K.J.; Gunawardhana, L.P.; Simpson, J.L.; Li, F.; Gibson, P.G. Different inflammatory phenotypes in adults and children with acute asthma. Eur. Respir. J. 2011, 38, 567–574. [Google Scholar] [CrossRef]
- Grunwell, J.R.; Giacalone, V.D.; Stephenson, S.; Margaroli, C.; Dobosh, B.S.; Brown, M.R.; Fitzpatrick, A.M.; Tirouvanziam, R. Neutrophil Dysfunction in the Airways of Children with Acute Respiratory Failure Due to Lower Respiratory Tract Viral and Bacterial Coinfections. Sci. Rep. 2019, 9, 2874. [Google Scholar] [CrossRef]
- Eller, M.C.N.; Vergani, K.P.; Saraiva-Romanholo, B.M.; Antonangelo, L.; Leone, C.; Rodrigues, J.C. Can inflammatory markers in induced sputum be used to detect phenotypes and endotypes of pediatric severe therapy-resistant asthma? Pediatr. Pulmonol. 2018, 53, 1208–1217. [Google Scholar] [CrossRef] [PubMed]
- Bossley, C.J.; Fleming, L.; Gupta, A.; Regamey, N.; Frith, J.; Oates, T.; Tsartsali, L.; Lloyd, C.M.; Bush, A.; Saglani, S. Pediatric severe asthma is characterized by eosinophilia and remodeling without TH2 cytokines. J. Allergy Clin. Immunol. 2012, 129, 974–982.e13. [Google Scholar] [CrossRef]
- Fleming, L.; Tsartsali, L.; Wilson, N.; Regamey, N.; Bush, A. Sputum inflammatory phenotypes are not stable in children with asthma. Thorax 2012, 67, 675–681. [Google Scholar] [CrossRef]
- Nagakumar, P.; Denney, L.; Fleming, L.; Bush, A.; Lloyd, C.M.; Saglani, S. Type 2 innate lymphoid cells in induced sputum from children with severe asthma. J. Allergy Clin. Immunol. 2015, 137, 624–626.e6. [Google Scholar] [CrossRef]
- Andersson, C.K.; Adams, A.; Nagakumar, P.; Bossley, C.; Gupta, A.; De Vries, D.; Adnan, A.; Bush, A.; Saglani, S.; Lloyd, C.M. Intraepithelial neutrophils in pediatric severe asthma are associated with better lung function. J. Allergy Clin. Immunol. 2016, 139, 1819–1829.e11. [Google Scholar] [CrossRef] [PubMed]
- Grunwell, J.R.; Stephenson, S.T.; Tirouvanziam, R.; Brown, L.A.S.; Brown, M.R.; Fitzpatrick, A.M. Children with Neutrophil-Predominant Severe Asthma Have Proinflammatory Neutrophils With Enhanced Survival and Impaired Clearance. J. Allergy Clin. Immunol. Pract. 2019, 7, 516–525.e6. [Google Scholar] [CrossRef] [PubMed]
- Steinke, J.W.; Lawrence, M.G.; Teague, W.G.; Braciale, T.J.; Patrie, J.T.; Borish, L. Bronchoalveolar lavage cytokine patterns in children with severe neutrophilic and paucigranulocytic asthma. J. Allergy Clin. Immunol. 2020, 147, 686–693.e3. [Google Scholar] [CrossRef] [PubMed]
- Wei, Q.; Liao, J.; Jiang, M.; Liu, J.; Liang, X.; Nong, G. Relationship between Th17-mediated immunity and airway inflammation in childhood neutrophilic asthma. Allergy, Asthma Clin. Immunol. 2021, 17, 4. [Google Scholar] [CrossRef] [PubMed]
- Gibson, P.G.; Yang, I.A.; Upham, J.W.; Reynolds, P.N.; Hodge, S.; James, A.L.; Jenkins, C.; Peters, M.J.; Marks, G.B.; Baraket, M.; et al. Effect of azithromycin on asthma exacerbations and quality of life in adults with persistent uncontrolled asthma (AMAZES): A randomised, double-blind, placebo-controlled trial. Lancet 2017, 390, 659–668. [Google Scholar] [CrossRef]
- Taylor, S.L.; Leong, L.E.X.; Mobegi, F.M.; Choo, J.M.; Wesselingh, S.; Yang, I.A.; Upham, J.W.; Reynolds, P.N.; Hodge, S.; James, A.L.; et al. Long-Term Azithromycin Reduces Haemophilus influenzae and Increases Antibiotic Resistance in Severe Asthma. Am. J. Respir. Crit. Care Med. 2019, 200, 309–317. [Google Scholar] [CrossRef]
- Cogen, J.D.; Onchiri, F.; Emerson, J.; Gibson, R.L.; Hoffman, L.R.; Nichols, D.P.; Rosenfeld, M. Chronic Azithromycin Use in Cystic Fibrosis and Risk of Treatment-Emergent Respiratory Pathogens. Ann. Am. Thorac. Soc. 2018, 15, 702–709. [Google Scholar] [CrossRef]
- Choi, Y.; Shin, S.H.; Lee, H.; Cho, H.K.; Im, Y.; Kang, N.; Choi, H.S.; Park, H.Y. Favorable Response to Long-Term Azithromycin Therapy in Bronchiectasis Patients with Chronic Airflow Obstruction Compared to Chronic Obstructive Pulmonary Disease Patients without Bronchiectasis. Int. J. Chronic Obstr. Pulm. Dis. 2021, 16, 855–863. [Google Scholar] [CrossRef]
- Follows, R.M.; Snowise, N.G.; Ho, S.-Y.; Ambery, C.L.; Smart, K.; McQuade, B.A. Efficacy, safety and tolerability of GSK2190915, a 5-lipoxygenase activating protein inhibitor, in adults and adolescents with persistent asthma: A randomised dose-ranging study. Respir. Res. 2013, 14, 54. [Google Scholar] [CrossRef]
- Osei, E.T.; Brandsma, C.-A.; Timens, W.; Heijink, I.H.; Hackett, T.-L. Current perspectives on the role of interleukin-1 signalling in the pathogenesis of asthma and COPD. Eur. Respir. J. 2019, 55, 1900563. [Google Scholar] [CrossRef]
- Badi, Y.; Pavel, A.B.; Riley, J.H.; Chung, K.F.; Guttman-Yassky, E.; Adcock, I.M. Is Fezakinumab, an anti-IL22 antibody, a putative novel therapy for a subset of severe asthma? Eur. Respir. J. 2019, 54 (Suppl. S63), OA1606. [Google Scholar] [CrossRef]
- Guttman-Yassky, E.; Brunner, P.M.; Neumann, A.U.; Khattri, S.; Pavel, A.B.; Malik, K.; Singer, G.K.; Baum, D.; Gilleaudeau, P.; Sullivan-Whalen, M.; et al. Efficacy and safety of fezakinumab (an IL-22 monoclonal antibody) in adults with moderate-to-severe atopic dermatitis inadequately controlled by conventional treatments: A randomized, double-blind, phase 2a trial. J. Am. Acad. Dermatol. 2018, 78, 872–881.e6. [Google Scholar] [CrossRef] [PubMed]
- Amarnani, A.; Rosenthal, K.S.; Mercado, J.M.; Brodell, R.T. Concurrent treatment of chronic psoriasis and asthma with ustekinumab. J. Dermatol. Treat. 2013, 25, 63–66. [Google Scholar] [CrossRef]
- Lucas, S.R.; Platts-Mills, T.A. Physical activity and exercise in asthma: Relevance to etiology and treatment. J. Allergy Clin. Immunol. 2005, 115, 928–934. [Google Scholar] [CrossRef]
- Oberle, A.J.; Mathur, P. Precision medicine in asthma. Curr. Opin. Pulm. Med. 2017, 23, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Rogers, G.B.; van der Gast, C.J.; Serisier, D.J. Predominant pathogen competition and core microbiota divergence in chronic airway infection. ISME J. 2014, 9, 217–225. [Google Scholar] [CrossRef]
- Nair, P.; Prabhavalkar, K.S. Neutrophilic Asthma and Potentially Related Target Therapies. Curr. Drug Targets 2020, 21, 374–388. [Google Scholar] [CrossRef]
- Vats, R.; Kaminski, T.W.; Brzoska, T.; Leech, J.A.; Tutuncuoglu, E.; Katoch, O.; Jonassaint, J.; Tejero, J.; Novelli, E.M.; Pradhan-Sundd, T.; et al. Liver-to-lung microembolic NETs promote gasdermin D–dependent inflammatory lung injury in sickle cell disease. Blood 2022, 140, 1020–1037. [Google Scholar] [CrossRef]
- Qu, M.; Chen, Z.; Qiu, Z.; Nan, K.; Wang, Y.; Shi, Y.; Shao, Y.; Zhong, Z.; Zhu, S.; Guo, K.; et al. Neutrophil extracellular traps-triggered impaired autophagic flux via METTL3 underlies sepsis-associated acute lung injury. Cell Death Discov. 2022, 8, 375. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Main Study (and Related Articles) | Year | Biomarkers | Treatment | Conclusion |
|---|---|---|---|---|
| Wenzel [11] | 2009 | TNF | Golimumab | No clinical efficacy |
| Holgate (Howarth, Berry, Morjaria) [12] | 2011 | TNF | Etanercept | No clinical efficacy |
| Niessen (Gibson, Brusselle, Taylor) [13] | 2020 | TNF | Macrolides (azithromycin) | Dysregulated TNF in pt. with NA is suppressed by azithromycin |
| Simpson [14] | 2008 | Unknown | Macrolides (clarithromycin) | Modulation of airways neutrophil accumulation and activation |
| Brusselle [7] | 2013 | Unknown | Macrolides (azithromycin) | Reduction in severe exacerbation |
| Nair [15] | 2012 | CXCR2 | CXCR2 receptor antagonist (SCH527123) | Reduction in sputum neutrophils in patients with SA and sputum neutrophils |
| Leaker [16] | 2013 | CXCR2 | CXCR2 antagonist (AZD8309) | Inhibition of LPS-induced inflammation |
| O’Byrne (Watz) [17] | 2016 | CXCR2 | CXCR2 antagonist (AZD5069) | Reduction in mucosal, sputum and blood neutrophils without clinical efficacy |
| Busse [18] | 2013 | IL-17 | Anti-IL-17R (Brodalumab) | No clinical efficacy |
| Chaudhuri (Follows) [19] | 2014 | 5-lipoxygenase-activating protein (FLAP) | FLAP inhibitor (GSK2190915) | No effect on sputum cell counts or clinical endpoints in patients with asthma and sputum neutrophils |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peri, F.; Amaddeo, A.; Badina, L.; Maschio, M.; Barbi, E.; Ghirardo, S. T2-Low Asthma: A Discussed but Still Orphan Disease. Biomedicines 2023, 11, 1226. https://doi.org/10.3390/biomedicines11041226
Peri F, Amaddeo A, Badina L, Maschio M, Barbi E, Ghirardo S. T2-Low Asthma: A Discussed but Still Orphan Disease. Biomedicines. 2023; 11(4):1226. https://doi.org/10.3390/biomedicines11041226
Chicago/Turabian StylePeri, Francesca, Alessandro Amaddeo, Laura Badina, Massimo Maschio, Egidio Barbi, and Sergio Ghirardo. 2023. "T2-Low Asthma: A Discussed but Still Orphan Disease" Biomedicines 11, no. 4: 1226. https://doi.org/10.3390/biomedicines11041226