

Bioresorbable Magnesium-Based Stent: Real-World Clinical Experience and Feasibility of Follow-Up by Coronary Computed Tomography: A New Window to Look at New Scaffolds
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Quantitative Coronary Angiography Analysis
2.3. Coronary Computed Tomography Angiography Acquisition and Analysis
2.4. Statistical Analysis
3. Results
3.1. Study Population
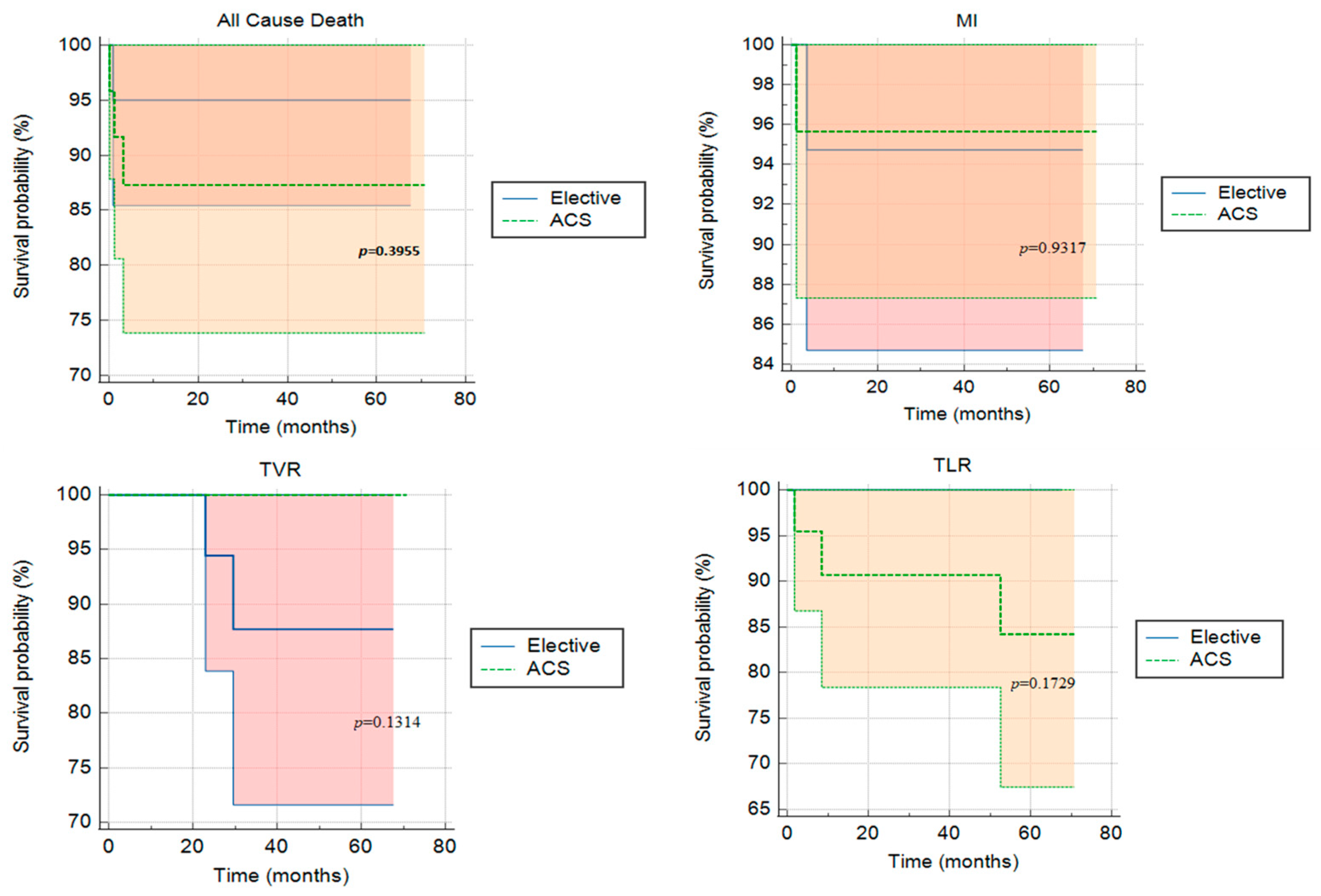
3.2. Clinical and Radiological Outcome
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nathan, A.; Kobayashi, T.; Kolansky, D.M.; Wilensky, R.L.; Giri, J. Bioresorbable Scaffolds for Coronary Artery Disease. Curr. Cardiol. Rep. 2017, 19, 5. [Google Scholar] [CrossRef] [PubMed]
- Tuzcu, E.M.; Kapadia, S. Bioresorbable Scaffold: Balancing Risks to Promissory Benefits? JACC Cardiovasc. Interv. 2017, 10, 1230–1232. [Google Scholar] [CrossRef] [PubMed]
- D’Ascenzo, F.; Barbero, U.; Moretti, C.; Palmerini, T.; Della Riva, D.; Mariani, A.; Omedè, P.; DiNicolantonio, J.J.; Biondi-Zoccai, G.; Gaita, F. Percutaneous Coronary Intervention versus Coronary Artery Bypass Graft for Stable Angina: Meta-Regression of Randomized Trials. Contemp. Clin. Trials 2014, 38, 51–58. [Google Scholar] [CrossRef]
- Bacchi-reggiani, L.; Tat, M.S.; Smits, P.C.; Vlachojannis, G.J. Long-Term Safety of Drug-Eluting and Bare-Metal Stents: Evidence From a Comprehensive Network Meta-Analysis. J. Am. Coll. Cardiol. 2015, 65, 2496–2507. [Google Scholar] [CrossRef] [Green Version]
- Rapetto, C.; Leoncini, M. Magmaris: A New Generation Metallic Sirolimus-Eluting Fully Bioresorbable Scaffold: Present Status and Future Perspectives. J. Thorac. Dis. 2017, 9, S903–S913. [Google Scholar] [CrossRef] [Green Version]
- Sotomi, Y.; Onuma, Y.; Collet, C.; Tenekecioglu, E.; Virmani, R.; Kleiman, N.S.; Serruys, P.W. Bioresorbable Scaffold: The Emerging Reality and Future Directions. Circ. Res. 2017, 120, 1341–1352. [Google Scholar] [CrossRef]
- Bennett, J.; De Hemptinne, Q.; McCutcheon, K. Magmaris Resorbable Magnesium Scaffold for the Treatment of Coronary Heart Disease: Overview of Its Safety and Efficacy. Expert Rev. Med. Devices 2019, 16, 757–769. [Google Scholar] [CrossRef]
- Onuma, Y.; Serruys, P.W. Sustained Safety and Efficacy of the Magnesium Scaffold: Does the Magmaris Scaffold Call for the Return of BRS Research and Randomised Controlled Trials? EuroIntervention 2020, 15, E1307–E1311. [Google Scholar] [CrossRef] [Green Version]
- Ortega-Paz, L.; Capodanno, D.; Gori, T.; Nef, H.; Latib, A.; Caramanno, G.; Di Mario, C.; Naber, C.; Lesiak, M.; Capranzano, P.; et al. Predilation, Sizing and Post-Dilation Scoring in Patients Undergoing Everolimus-Eluting Bioresorbable Scaffold Implantation for Prediction of Cardiac Adverse Events: Development and Internal Validation of the PSP Score. EuroIntervention 2017, 12, 2110–2117. [Google Scholar] [CrossRef] [Green Version]
- Scalone, G.; Brugaletta, S.; Gómez-Monterrosas, O.; Otsuki, S.; Sabate, M. St-Segment Elevation Myocardial Infarction—Ideal Scenario for Bioresorbable Vascular Scaffold Implantation? Circ. J. 2015, 79, 263–270. [Google Scholar] [CrossRef] [Green Version]
- Byrne, R.A.; Alfonso, F.; Schneider, S.; Maeng, M.; Wiebe, J.; Kretov, E.; Bradaric, C.; Rai, H.; Cuesta, J.; Rivero, F.; et al. Prospective, Randomized Trial of Bioresorbable Scaffolds vs. Everolimus-Eluting Stents in Patients Undergoing Coronary Stenting for Myocardial Infarction: The Intracoronary Scaffold Assessment a Randomized Evaluation of Absorb in Myocardial Infarction. Eur. Heart J. 2019, 40, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Katagiri, Y.; Onuma, Y.; Asano, T.; Iniguez, A.; Jensen, L.O.; Cequier, À.; Hofma, S.H.; Christiansen, E.H.; Suttorp, M.; Brugaletta, S.; et al. Three-Year Follow-up of the Randomised Comparison between an Everolimus-Eluting Bioresorbable Scaffold and a Durable Polymer Everolimus-Eluting Metallic Stent in Patients with ST-Segment Elevation Myocardial Infarction (TROFI II Trial). EuroIntervention 2018, 14, E1224–E1226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabaté, M.; Windecker, S.; Iñiguez, A.; Okkels-Jensen, L.; Cequier, A.; Brugaletta, S.; Hofma, S.H.; Räber, L.; Christiansen, E.H.; Suttorp, M.; et al. Everolimus-Eluting Bioresorbable Stent vs. Durable Polymer Everolimus-Eluting Metallic Stent in Patients with ST-Segment Elevation Myocardial Infarction: Results of the Randomized ABSORB ST-Segment Elevation Myocardial Infarction-TROFI II Trial. Eur. Heart J. 2016, 37, 229–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on Myocardial Revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [Green Version]
- Bangalore, S.; Bezerra, H.G.; Rizik, D.G.; Armstrong, E.J.; Samuels, B.; Naidu, S.S.; Grines, C.L.; Foster, M.T.; Choi, J.W.; Bertolet, B.D.; et al. The State of the Absorb Bioresorbable Scaffold: Consensus from an Expert Panel. JACC Cardiovasc. Interv. 2017, 10, 2349–2359. [Google Scholar] [CrossRef]
- Iqbal, J.; Onuma, Y.; Ormiston, J.; Abizaid, A.; Waksman, R.; Serruys, P. Bioresorbable Scaffolds: Rationale, Current Status, Challenges, and Future. Eur. Heart J. 2014, 35, 765–776. [Google Scholar] [CrossRef] [Green Version]
- Joner, M.; Ruppelt, P.; Zumstein, P.; Lapointe-Corriveau, C.; Leclerc, G.; Bulin, A.; Castellanos, M.I.; Wittchow, E.; Haude, M.; Waksman, R. Preclinical Evaluation of Degradation Kinetics and Elemental Mapping of First- and Second-Generation Bioresorbable Magnesium Scaffolds. EuroIntervention 2018, 14, e1040–e1048. [Google Scholar] [CrossRef] [Green Version]
- Haude, M.; Ince, H.; Abizaid, A.; Toelg, R.; Lemos, P.A.; Von Birgelen, C.; Christiansen, E.H.; Wijns, W.; Neumann, F.J.; Kaiser, C.; et al. Sustained Safety and Performance of the Second-Generation Drug-Eluting Absorbable Metal Scaffold in Patients with de Novo Coronary Lesions: 12-Month Clinical Results and Angiographic Findings of the BIOSOLVE-II First-in-Man Trial. Eur. Heart J. 2016, 37, 2701–2709. [Google Scholar] [CrossRef] [Green Version]
- Verheye, S.; Wlodarczak, A.; Montorsi, P.; Bennett, J.; Torzewski, J.; Haude, M.; Vrolix, M.; Buck, T.; Aminian, A.; van der Schaaf, R.J.; et al. Safety and Performance of a Resorbable Magnesium Scaffold under Real-World Conditions: 12-Month Outcomes of the First 400 Patients Enrolled in the BIOSOLVE-IV Registry. EuroIntervention 2019, 15, e1383–e1386. [Google Scholar] [CrossRef] [Green Version]
- Haude, M.; Ince, H.; Kische, S.; Abizaid, A.; Tölg, R.; Alves Lemos, P.; Van Mieghem, N.M.; Verheye, S.; von Birgelen, C.; Christiansen, E.H.; et al. Safety and Clinical Performance of a Drug Eluting Absorbable Metal Scaffold in the Treatment of Subjects with de Novo Lesions in Native Coronary Arteries: Pooled 12-Month Outcomes of BIOSOLVE-II and BIOSOLVE-III. Catheter. Cardiovasc. Interv. 2018, 92, E502–E511. [Google Scholar] [CrossRef] [Green Version]
- Sabaté, M.; Alfonso, F.; Cequier, A.; Romaní, S.; Bordes, P.; Serra, A.; Iñiguez, A.; Salinas, P.; García del Blanco, B.; Goicolea, J.; et al. Magnesium-Based Resorbable Scaffold versus Permanent Metallic Sirolimus-Eluting Stent in Patients with ST-Segment Elevation Myocardial Infarction: The MAGSTEMI Randomized Clinical Trial. Circulation 2019, 140, 1904–1916. [Google Scholar] [CrossRef] [PubMed]
- Dębski, M.; Kruk, M.; Bujak, S.; Dzielińska, Z.; Demkow, M.; Kępka, C. Coronary Computed Tomography Angiography Equals Invasive Angiography for the Prediction of Coronary Revascularization. Adv. Interv. Cardiol. 2019, 3, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Raff, G.L.; Gallagher, M.J.; O’Neill, W.W.; Goldstein, J.A. Diagnostic Accuracy of Noninvasive Coronary Angiography Using 64-Slice Spiral Computed Tomography. J. Am. Coll. Cardiol. 2005, 46, 552–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newby, D.; Williams, M.; Hunter, A.; Pawade, T.; Shah, A.; Flapan, A.; Forbes, J.; Hargreaves, A.; Leslie, S.; Lewis, S.; et al. CT Coronary Angiography in Patients with Suspected Angina Due to Coronary Heart Disease (SCOT-HEART): An Open-Label, Parallel-Group, Multicentre Trial. Lancet 2015, 385, 2383–2391. [Google Scholar] [CrossRef] [Green Version]
- Rixe, J.; Achenbach, S.; Ropers, D.; Baum, U.; Kuettner, A.; Ropers, U.; Bautz, W.; Daniel, W.G.; Anders, K. Assessment of Coronary Artery Stent Restenosis by 64-Slice Multi-Detector Computed Tomography. Eur. Heart J. 2006, 27, 2567–2572. [Google Scholar] [CrossRef]
- Carbone, I.; Francone, M.; Algeri, E.; Granatelli, A.; Napoli, A.; Kirchin, M.A.; Catalano, C.; Passariello, R. Non-Invasive Evaluation of Coronary Artery Stent Patency with Retrospectively ECG-Gated 64-Slice CT Angiography. Eur. Radiol. 2008, 18, 234–243. [Google Scholar] [CrossRef]
- Wlodarczak, A.; Garcia, L.A.I.; Karjalainen, P.P.; Komócsi, A.; Pisano, F.; Richter, S.; Lanocha, M.; Rumoroso, J.R.; Leung, K.F. Magnesium 2000 Postmarket Evaluation: Guideline Adherence and Intraprocedural Performance of a Sirolimus-Eluting Resorbable Magnesium Scaffold. Cardiovasc. Revasculariz. Med. 2019, 20, 1140–1145. [Google Scholar] [CrossRef]
- Blachutzik, F.; Achenbach, S.; Tröbs, M.; Marwan, M.; Weissner, M.; Nef, H.; Schlundt, C. Effect of Non-Compliant Balloon Postdilatation on Magnesium-Based Bioresorbable Vascular Scaffolds. Catheter. Cardiovasc. Interv. 2019, 93, 202–207. [Google Scholar] [CrossRef]
- Tamburino, C.; Latib, A.; Van Geuns, R.J.; Sabate, M.; Mehilli, J.; Gori, T.; Achenbach, S.; Alvarez, M.P.; Nef, H.; Lesiak, M.; et al. Contemporary Practice and Technical Aspects in Coronary Intervention with Bioresorbable Scaffolds: A European Perspective. EuroIntervention 2015, 11, 45–52. [Google Scholar] [CrossRef] [Green Version]
- Tamai, H.; Igaki, K.; Kyo, E.; Kosuga, K.; Kawashima, A.; Matsui, S.; Komori, H.; Tsuji, T.; Motohara, S.; Uehata, H. Initial and 6-Month Results of Biodegradable Poly-l-Lactic Acid Coronary Stents in Humans. Circulation 2000, 102, 399–404. [Google Scholar] [CrossRef] [Green Version]
- Wiebe, J.; Nef, H.M.; Hamm, C.W. Current Status of Bioresorbable Scaffolds in the Treatment of Coronary Artery Disease. J. Am. Coll. Cardiol. 2014, 64, 2541–2551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hideo-Kajita, A.; Garcia-Garcia, H.M.; Kolm, P.; Azizi, V.; Ozaki, Y.; Dan, K.; Ince, H.; Kische, S.; Abizaid, A.; Töelg, R.; et al. Comparison of Clinical Outcomes between Magmaris and Orsiro Drug Eluting Stent at 12 months: Pooled Patient Level Analysis from BIOSOLVE II–III and BIOFLOW II Trials. Int. J. Cardiol. 2020, 300, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Haude, M.; Toelg, R.; Lemos, P.A.; Christiansen, E.H.; Abizaid, A.; von Birgelen, C.; Neumann, F.J.; Wijns, W.; Ince, H.; Kaiser, C.; et al. Sustained Safety and Performance of a Second-Generation Sirolimus-Eluting Absorbable Metal Scaffold: Long-Term Data of the BIOSOLVE-II First-in-Man Trial at 5 Years. Cardiovasc. Revasculariz. Med. 2022, 38, 106–110. [Google Scholar] [CrossRef] [PubMed]
- Neumann, F.J.; Sechtem, U.; Banning, A.P.; Bonaros, N.; Bueno, H.; Bugiardini, R.; Chieffo, A.; Crea, F.; Czerny, M.; Delgado, V.; et al. 2019 ESC Guidelines for the Diagnosis and Management of Chronic Coronary Syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [Green Version]
- Miller, J.M.; Rochitte, C.E.; Dewey, M.; Arbab-Zadeh, A.; Niinuma, H.; Gottlieb, I.; Paul, N.; Clouse, M.E.; Shapiro, E.P.; Hoe, J.; et al. Diagnostic Performance of Coronary Angiography by 64-Row CT. N. Engl. J. Med. 2008, 359, 2324–2336. [Google Scholar] [CrossRef] [Green Version]
- Shaw, L.J.; Hausleiter, J.; Achenbach, S.; Al-Mallah, M.; Berman, D.S.; Budoff, M.J.; Cademartiri, F.; Callister, T.Q.; Chang, H.J.; Kim, Y.J.; et al. Coronary Computed Tomographic Angiography as a Gatekeeper to Invasive Diagnostic and Surgical Procedures: Results from the Multicenter Confirm (Coronary Ct Angiography Evaluation for Clinical Outcomes: An International Multicenter) Registry. J. Am. Coll. Cardiol. 2012, 60, 2103–2114. [Google Scholar] [CrossRef] [Green Version]
- Motoyama, S.; Sarai, M.; Harigaya, H.; Anno, H.; Inoue, K.; Hara, T.; Naruse, H.; Ishii, J.; Hishida, H.; Wong, N.D.; et al. Computed Tomographic Angiography Characteristics of Atherosclerotic Plaques Subsequently Resulting in Acute Coronary Syndrome. J. Am. Coll. Cardiol. 2009, 54, 49–57. [Google Scholar] [CrossRef] [Green Version]
- Collet, C.; Chevalier, B.; Cequier, A.; Fajadet, J.; Dominici, M.; Helqvist, S.; Van Boven, A.J.; Dudek, D.; McClean, D.; Almeida, M.; et al. Diagnostic Accuracy of Coronary CT Angiography for the Evaluation of Bioresorbable Vascular Scaffolds. JACC Cardiovasc. Imaging 2018, 11, 722–732. [Google Scholar] [CrossRef]
- Ferenț, I.; Mester, A.; Chițu, M.; Benedek, A.; Rațiu, M.; Hodas, R.; Benedek, I. CTA Evaluation of Bioresorbable Scaffolds versus Metallic Coronary Stents—A Feasibility Study. J. Interdiscip. Med. 2018, 3, 152–159. [Google Scholar] [CrossRef] [Green Version]
- Pernigotti, A.; Moscarella, E.; Spitaleri, G.; Scardino, C.; Ishida, K.; Brugaletta, S. Methods to Assess Bioresorbable Vascular Scaffold Devices Behaviour after Implantation. J. Thorac. Dis. 2017, 9, S959–S968. [Google Scholar] [CrossRef] [Green Version]
- Opolski, M.P.; Kepka, C.; Wojakowski, W.; Witkowski, A. Computed Tomography Angiography for Guiding and Follow-up of Magnesium-Bioresorbable Scaffold Implantation. Clin. Res. Cardiol. 2019, 108, 344–346. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.S.; Ramsamy, G. Appearance of Bioresorbable Vascular Scaffolds on Computed Tomography Coronary Angi Ography. Singapore Med. J. 2017, 58, 623–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verheye, S.; Wlodarczak, A.; Montorsi, P.; Torzewski, J.; Bennett, J.; Haude, M.; Starmer, G.; Buck, T.; Wiemer, M.; Nuruddin, A.A.B.; et al. BIOSOLVE-IV-Registry: Safety and Performance of the Magmaris Scaffold: 12-Month Outcomes of the First Cohort of 1075 Patients. Catheter. Cardiovasc. Interv. 2021, 98, E1–E8. [Google Scholar] [CrossRef] [PubMed]
- de Hemptinne, Q.; Xaplanteris, P.; Guédès, A.; Demeure, F.; Vandeloo, B.; Dugauquier, C.; Picard, F.; Warne, D.W.; Pilgrim, T.; Iglesias, J.F.; et al. Magmaris Resorbable Magnesium Scaffold versus Conventional Drug-Eluting Stent in ST-Segment Elevation Myocardial Infarction: 1-Year Results of a Propensity Score Matching Comparison. Cardiovasc. Revasculariz. Med. 2022, 43, 28–35. [Google Scholar] [CrossRef]
- Bossard, M.; Madanchi, M.; Avdijaj, D.; Attinger-Toller, A.; Cioffi, G.M.; Seiler, T.; Tersalvi, G.; Kobza, R.; Schüpfer, G.; Cuculi, F. Long-Term Outcomes After Implantation of Magnesium-Based Bioresorbable Scaffolds—Insights from an All-Comer Registry. Front. Cardiovasc. Med. 2022, 9. [Google Scholar] [CrossRef] [PubMed]
- de Hemptinne, Q.; Picard, F.; Briki, R.; Awada, A.; Silance, P.-G.; Dolatabadi, D.; Debbas, N.; Unger, P. Drug-Eluting Resorbable Magnesium Scaffold Implantation in ST-Segment Elevation Myocardial Infarction: A Pilot Study. J. Invasive Cardiol. 2018, 30, 202–206. [Google Scholar]
- Haude, M.; Ince, H.; Kische, S.; Toelg, R.; Van Mieghem, N.M.; Verheye, S.; von Birgelen, C.; Christiansen, E.H.; Barbato, E.; Garcia-Garcia, H.M.; et al. Sustained Safety and Performance of the Second-Generation Sirolimus-Eluting Absorbable Metal Scaffold: Pooled Outcomes of the BIOSOLVE-II and -III Trials at 3 Years. Cardiovasc. Revasculariz. Med. 2020, 21, 1150–1154. [Google Scholar] [CrossRef]
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.P.; Costa, F.; Jeppsson, A.; Jüni, P.; Kastrati, A.; Kolh, P.; Mauri, L.; et al. 2017 ESC Focused Update on Dual Antiplatelet Therapy in Coronary Artery Disease Developed in Collaboration with EACTS. Eur. J. Cardio-Thoracic. Surg. 2018, 53, 34–78. [Google Scholar] [CrossRef] [Green Version]
- Cesaro, A.; Taglialatela, V.; Gragnano, F.; Moscarella, E.; Fimiani, F.; Conte, M.; Barletta, V.; Monda, E.; Limongelli, G.; Severino, S.; et al. Low-Dose Ticagrelor in Patients with High Ischemic Risk and Previous Myocardial Infarction: A Multicenter Prospective Real-World Observational Study. J. Cardiovasc. Pharmacol. 2020, 76, 173–180. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Product | Manufacturer | Polymer | Drug | Strut Thickness (µm) | Resorption Time (Months) | Availability |
|---|---|---|---|---|---|---|
| Absorb | Abbot | PLLA | EES | 150 | 48 | Discontinued |
| Magmaris (DREAMS-2G) | Biotronik | Mg | SES | 150 | 12 | Available |
| DREAMS-3G | Biotronik | BIOmag | SES | 120 | 12 | Under study |
| Fantom | REVA Medical | Tyrosine polycarbonate | SES | 125 | 36 | Available |
| Fortitude | Amaranth | PLLA | SES | 150 | 10 | Available |
| Aptitude | Amaranth | PLLA | SES | 115 | 10 | Under study |
| Magnitude | Amaranth | PLLA | SES | 98 | 36 | Under study |
| MeRes | Meril | PLLA | EES | 100 | 24 | Under study |
| DESolve Cx | ELIXIR | PLLA | NES | 120 | 24 | Available |
| Firesorb | MircoPort | PLLA | SES | 125 | N/A | Under study |
| Mirage | Manli | PLLA | SES | 150 | 14 | Discontinued |
| Xinsorb | Biotech | PLLA | SES | 160 | 24–36 | Under study |
| NeoVas | Lepu | PLLA | SES | 170 | 24–36 | Available |
| Bioheart | Bioheart | PLLA | Rapamycin | 125 | 6 | Under study |
| Art | Terumo | PDLLA | None | 170 | 6 | Available |
| Renuvia | Boston Scientific | PLLA | EES | 120 | 12–24 | Discontinued |
| Unity | Amg | Mg/PLLA | SES | 160 | 12 | Under study |
| Elective | ACS | Total | p-Value | |
|---|---|---|---|---|
| n | 20 (45.4%) | 24 (54.5%) | 44 | |
| Age, years | 60.5 ± 6.0 | 52.8 ± 7.3 | 56.3 ± 7.7 | 0.001 |
| Male | 19 (95.0%) | 17 (70.8%) | 36 (81.8%) | 0.038 |
| Hypertension | 13 (65.0%) | 13 (54.2%) | 27 (61.4%) | NS |
| Diabetes Mellitus | 8 (40.0%) | 8 (33.3%) | 16 (36.4%) | NS |
| PVD | 2 (10.0%) | 1 (4.2%) | 2 (4.5%) | NS |
| Dyslipidemia | 14 (70.0%) | 14 (58.3%) | 29 (65.9%) | NS |
| Renal failure | 2 (10.0%) | 0 (0.0%) | 2 (4.5%) | NS |
| Family History of CAD | 4 (20.0%) | 7 (29.2%) | 11 (25.0%) | NS |
| Current Smoking | 7 (35.0%) | 17 (70.8%) | 23 (52.3%) | 0.017 |
| IVUS | 7 (35.0%) | 2 (8.3%) | 9 (20.5%) | 0.029 |
| Lesions | 25 (48.1%) | 27 (51.9%) | 52 | |
| Treated vessel | ||||
| LAD | 16 (64.0%) | 17 (63.0%) | 33 (63.5%) | NS |
| LCx | 4 (16.0%) | 2 (7.4%) | 6 (11.5%) | NS |
| OM | 2 (8.0%) | 0 (0.0%) | 2 (3.8%) | NS |
| RCA | 3 (12.0%) | 7 (25.9%) | 10 (19.2%) | NS |
| RI | 0 (0.0%) | 1 (3.7%) | 1 (1.9%) | NS |
| ACC/AHA classification | ||||
| A | 10 (40.0%) | 12 (44.4%) | 22 (42.3%) | NS |
| B1 | 12 (48.0%) | 6 (22.2%) | 18 (34.6%) | NS |
| B2 | 3 (12.0%) | 9 (33.3%) | 12 (23.1%) | NS |
| Calcifications | 8 (32.0%) | 11 (40.7%) | 19 (36.5%) | NS |
| Procedure characteristics | ||||
| n | 25 | 27 | 52 | |
| Pre-dilation diameter (mm) | 2.65 ± 0.42 | 2.44 ± 0.30 | 2.55 ± 0.38 | 0.048 |
| Mg-BRS diameter (mm) | 3.10 ± 0.20 | 3.20 ± 0.25 | 3.15 ± 0.23 | NS |
| Mg-BRS length (mm) | 20.0 ± 4.6 | 21.3 ± 3.8 | 20.7 ± 4.2 | NS |
| Mg-BRS inflation pressure (atm) | 14.7 ± 1.0 | 15.1 ± 1.6 | 14.9 ± 1.4 | NS |
| Post-dilation balloon diameter (mm) | 3.38 ± 0.27 | 3.42 ± 0.29 | 3.41 ± 0.28 | NS |
| Post-dilation inflation pressure (atm) | 18.5 ± 2.6 | 18. ± 2.1 | 18.5 ± 2.3 | NS |
| Post-procedure medications | ||||
| Clopidogrel | 16 (80.0%) | 7 (29.2%) | 23 (52.3%) | 0.001 |
| Ticagrelor | 4 (20.0%) | 17 (70.8%) | 21 (47.7%) | 0.001 |
| Events | 4 (20.0%) | 6 (25.0%) | 10 (22.7%) | NS |
| Cardiac death | 1 (5.0%) | 3 (12.5%) | 4 (9.1%) | NS |
| TV MI | 1 (5.0%) | 1 (4.2%) | 2 (4.5%) | NS |
| TV-R | 2 (10.0%) | 0 (0.0%) | 2 (4.5%) | NS |
| CD-TLR | 0 (0.0%) | 3 (12.5%) | 3 (6.8%) | NS |
| UA | NSTEMI | STEMI | Total | p Value | |
|---|---|---|---|---|---|
| n | 5 (20.8%) | 10 (41.7%) | 9 (37.5%) | 24 | |
| Age, years | 56.4 ± 2.9 | 51.1 ± 7.8 | 52.8 ± 2.4 | 52.3 ± 1.5 | NS |
| Male | 4 (80.0%) | 6 (60.0%) | 7 (77.8%) | 17 (70.8%) | NS |
| Hypertension | 3 (60.0%) | 5 (50.0% | 5 (55.6%) | 13 (54.2%) | NS |
| Diabetes Mellitus | 1 (20.0%) | 4 (40.0%) | 3 (33.3%) | 8 (33.3%) | NS |
| PVD | 0 (0.0%) | 0 (0.0%) | 1 (11.1%) | 1 (4.2%) | NS |
| Dyslipidemia | 1 (20.0%) | 9 (90.0%) | 4 (44.4%) | 14 (58.3%) | 0.02 |
| Renal failure | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| Family history | 1 (20.0%) | 4 (40.0%) | 2 (22.2%) | 7 (29.2%) | NS |
| Smoking | 3 (60.0%) | 7 (70.0%) | 7 (77.8%) | 17 (70.8%) | NS |
| IVUS | 0 (0.0%) | 2 (20.0%) | 0 (0.0%) | 2 (8.3%) | NS |
| Lesions | 5 | 12 | 11 | 28 | |
| Treated vessel | |||||
| LAD | 1 (20.0%) | 9 (75.0%) | 7 (63.6%) | 17 (60.7%) | NS |
| LCx | 1 (20.0%) | 0 (0.0%) | 1 (9.1%) | 2 (7.1%) | NS |
| OM | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| RCA | 3 (60.0%) | 3 (25.0%) | 2 (18.3%) | 8 (28.6%) | NS |
| RI | 0 (0.0%) | 0 (0.0%) | 1 (9.1%) | 1 (3.6%) | NS |
| ACC/AHA classification | |||||
| A | 4 (80.0%) | 8 (66.7%) | 1 (9.1%) | 13 (46.4%) | |
| B1 | 1 (20.0%) | 2 (16.7%) | 3 (27.3%) | 6 (21.4%) | |
| B2 | 0 (20.0%) | 2 (16.7%) | 7 (63.6%) | 9 (32.2%) | |
| Calcifications | 1 (20.0%) | 4 (33.3%) | 6 (54.5%) | 11 (39.3%) | NS |
| Procedure characteristics | |||||
| n | 4 | 12 | 11 | 27 | |
| Pre-dilation balloon diameter (mm) | 2.62 ± 0.18 | 2.45 ± 0.27 | 2.39 ± 0.34 | 2.44 ± 0.30 | NS |
| Mg-BVS diameter (mm) | 3.37 ± 0.25 | 3.21 ± 0.26 | 3.13 ± 0.23 | 3.20 ± 0.25 | NS |
| Mg-BVS length (mm) | 21.2 ± 4.8 | 20.8 ± 4.2 | 21.8 ± 3.4 | 21.3 ± 3.8 | NS |
| Mg-BVS inflation pressure (atm) | 15.5 ± 1.0 | 14.9 ± 2.2 | 15.1 ± 1.0 | 15.1 ± 1.6 | NS |
| Post-dilation balloon diameter (mm) | 3.69 ± 0.24 | 3.42 ± 0.29 | 3.34 ± 0.26 | 3.41 ± 0.28 | NS |
| Post-dilation inflation pressure (atm) | 18.5 ± 1.9 | 18.5 ± 1.9 | 18.2 ± 2.7 | 18.5 ± 2.3 | NS |
| Post-procedure medications | |||||
| Clopidogrel | 5 (100.0%) | 1 (10.0%) | 1 (11.1%) | 7 (29.2%) | 0.00 |
| Ticagrelor | 0 (0.0%) | 9 (90.0%) | 8 (88.9%) | 17 (70.8%) | 0.00 |
| Events | 2 (40.0%) | 2 (20.0%) | 2 (22.2%) | 6 (25.0%) | NS |
| Cardiac death | 1 (20.0%) | 0 (0.0%) | 2 (22.2%) | 3 (12.5%) | NS |
| TV MI | 0 (0.0%) | 0 (0.0%) | 1 (11.1%) | 1 (4.2%) | NS |
| TVR | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | NS |
| CD-TLR | 1 (20.0%) | 2 (20.0%) | 0 (0.0%) | 3 (12.5%) | NS |
| Elective | ACS | Total | p Value | |
|---|---|---|---|---|
| n | 24 | 27 | 51 | |
| Pre-treatment | ||||
| Lesion diameter (mm) | 1.0 ± 0.4 | 1.2 ± 0.4 | 1.1 ± 0.4 | NS |
| Proximal vessel diameter (mm) | 2.7 ± 0.4 | 2.8 ± 0.6 | 2.7 ± 0.5 | NS |
| Distal vessel diameter (mm) | 2.4 ± 0.5 | 2.4 ± 0.5 | 2.4 ± 0.5 | NS |
| Mean Area (mm2) | 4.7 ± 2.0 | 5.5 ± 1.6 | 5.2 ± 1.8 | NS |
| Post stenting | ||||
| Minimal diameter (mm) | 2.4 ± 0.4 | 2.4 ± 0.5 | 2.4 ± 0.5 | NS |
| Proximal vessel diameter (mm) | 3.0 ± 0.5 | 2.9 ± 0.6 | 2.9 ± 0.5 | NS |
| Distal vessel diameter (mm) | 2.7 ± 0.5 | 2.9 ± 1.5 | 2.8 ± 1.1 | NS |
| Minimal surface area (MSA) (mm2) | 4.0 ± 1.8 | 4.3 ± 2.2 | 4.2 ± 2.0 | NS |
| Mean proximal to distal surface area (mm2) | 6.6 ± 2.0 | 6.6 ± 2.3 | 6.6 ± 2.1 | NS |
| Elective | ACS | Total | p Value | |
|---|---|---|---|---|
| n | 15 | 17 | 32 | |
| Date difference (months) | 7.1 ± 4.5 | 5.6 ± 2.5 | 6.4 ± 3.7 | NS |
| Proximal vessel diameter (mm) | 4.0 ± 0.3 | 3.8 ± 0.7 | 3.9 ± 0.5 | NS |
| Distal vessel diameter (mm) | 3.3 ± 0.6 | 3.1 ± 0.6 | 3.2 ± 0.6 | NS |
| Proximal surface area (mm2) | 9.4 ± 1.9 | 10.0 ± 3.7 | 9.7 ± 2.9 | NS |
| Distal surface area (mm2) | 7.4 ± 2.1 | 7.1 ± 2.9 | 7.2 ± 2.5 | NS |
| In-stent minimal diameter (mm) | 2.4 ± 0.4 | 2.4 ± 0.7 | 2.4 ± 0.6 | NS |
| In-stent maximal diameter (mm) | 4.1 ± 0.5 | 3.9 ± 0.9 | 4.0 ± 0.8 | NS |
| Minimal in-stent surface area (MSA) (mm2) | 6.1 ± 1.2 | 6.8 ± 2.6 | 6.5 ± 2.0 | NS |
| Maximal in-stent surface area (mm2) | 11.3 ± 2.5 | 10.9 ± 3.4 | 11.1 ± 3.0 | NS |
| Mean proximal to distal surface area (mm2) | 8.4 ± 1.6 | 8.5 ± 2.9 | 8.4 ± 2.3 | NS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghafari, C.; Brassart, N.; Delmotte, P.; Brunner, P.; Dghoughi, S.; Carlier, S. Bioresorbable Magnesium-Based Stent: Real-World Clinical Experience and Feasibility of Follow-Up by Coronary Computed Tomography: A New Window to Look at New Scaffolds. Biomedicines 2023, 11, 1150. https://doi.org/10.3390/biomedicines11041150
Ghafari C, Brassart N, Delmotte P, Brunner P, Dghoughi S, Carlier S. Bioresorbable Magnesium-Based Stent: Real-World Clinical Experience and Feasibility of Follow-Up by Coronary Computed Tomography: A New Window to Look at New Scaffolds. Biomedicines. 2023; 11(4):1150. https://doi.org/10.3390/biomedicines11041150
Chicago/Turabian StyleGhafari, Chadi, Nicolas Brassart, Philippe Delmotte, Philippe Brunner, Sarah Dghoughi, and Stéphane Carlier. 2023. "Bioresorbable Magnesium-Based Stent: Real-World Clinical Experience and Feasibility of Follow-Up by Coronary Computed Tomography: A New Window to Look at New Scaffolds" Biomedicines 11, no. 4: 1150. https://doi.org/10.3390/biomedicines11041150