
Formulation and Optimization of Repaglinide Nanoparticles Using Microfluidics for Enhanced Bioavailability and Management of Diabetes
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Preparation of Repaglinide Nanosuspension
2.3. Characterisation, Stability, and Dissolution Studies of Repaglinide Nanocrystals (Rp-Nc)
2.3.1. Determination of Particle Size
2.3.2. Determination of Zeta Potential
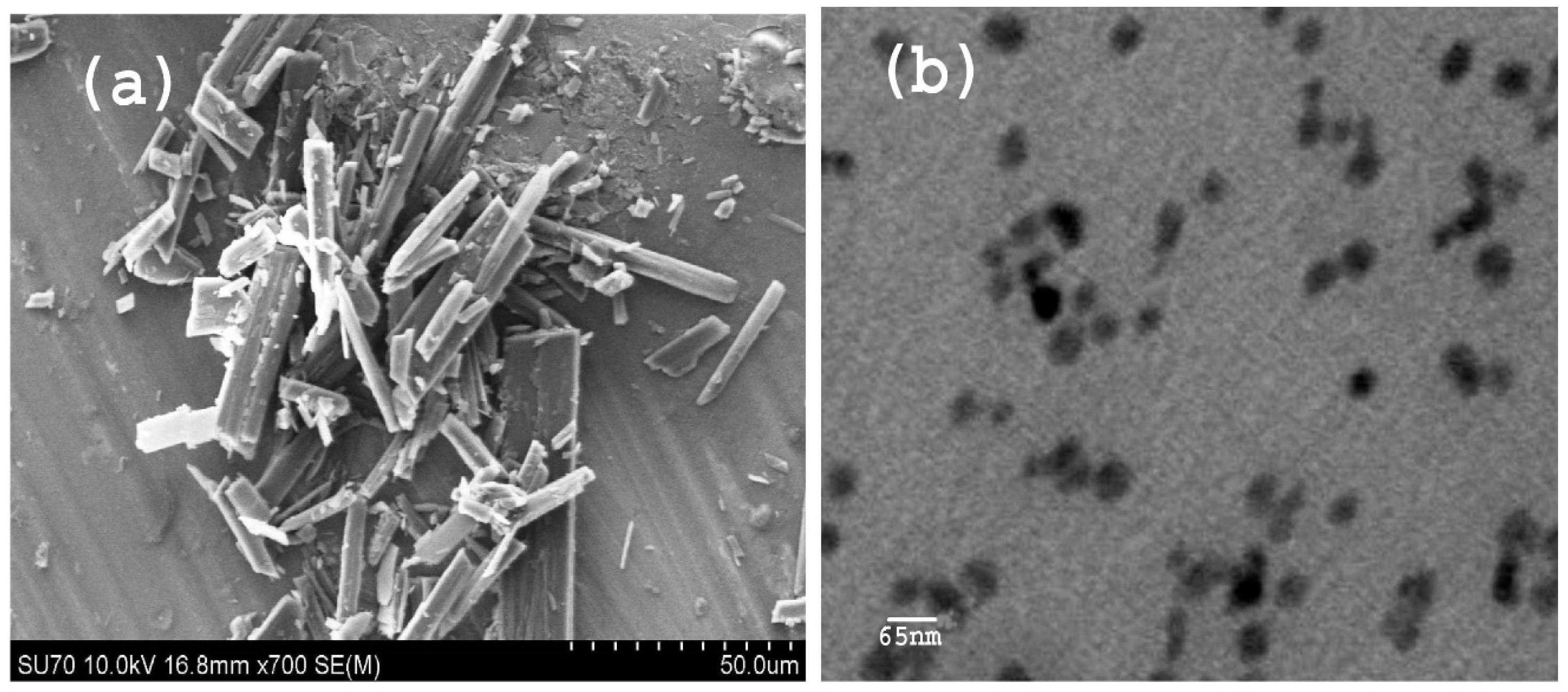
2.3.3. Scanning Electron Microscopy
2.3.4. Transmission Electron Microscopy
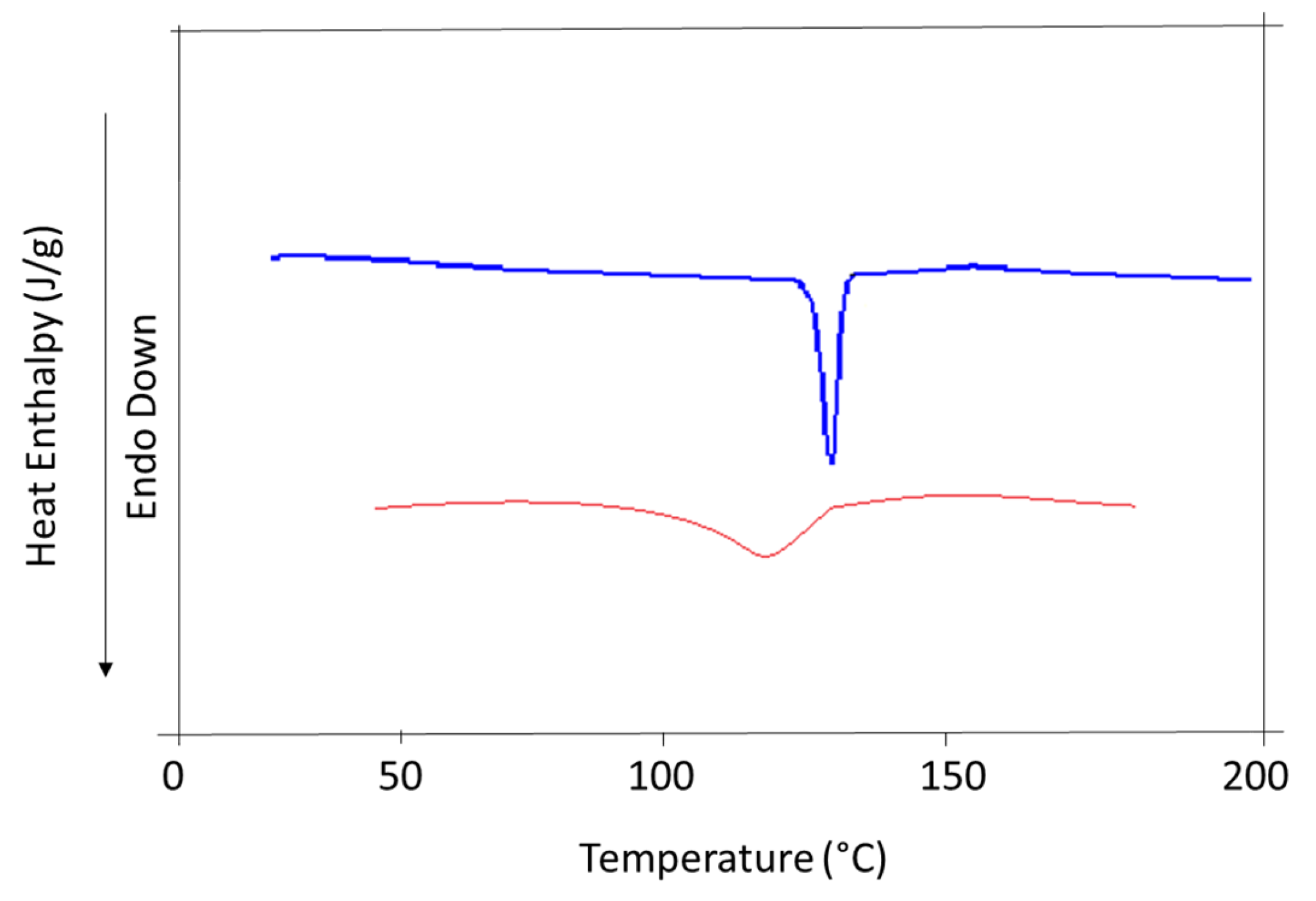
2.3.5. Differential Scanning Calorimetry
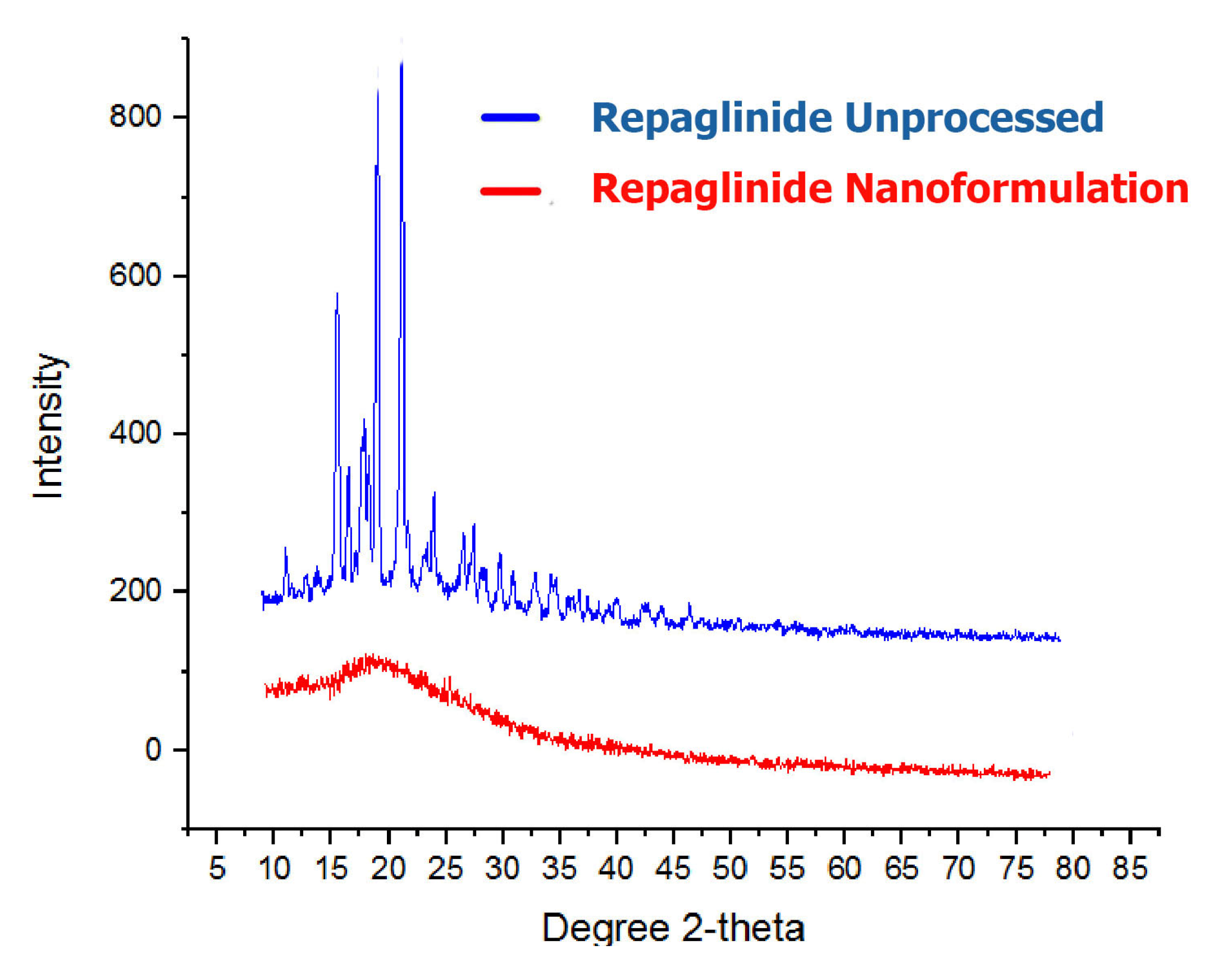
2.3.6. Powder X-ray Diffraction Studies
2.3.7. Saturation Solubility Studies
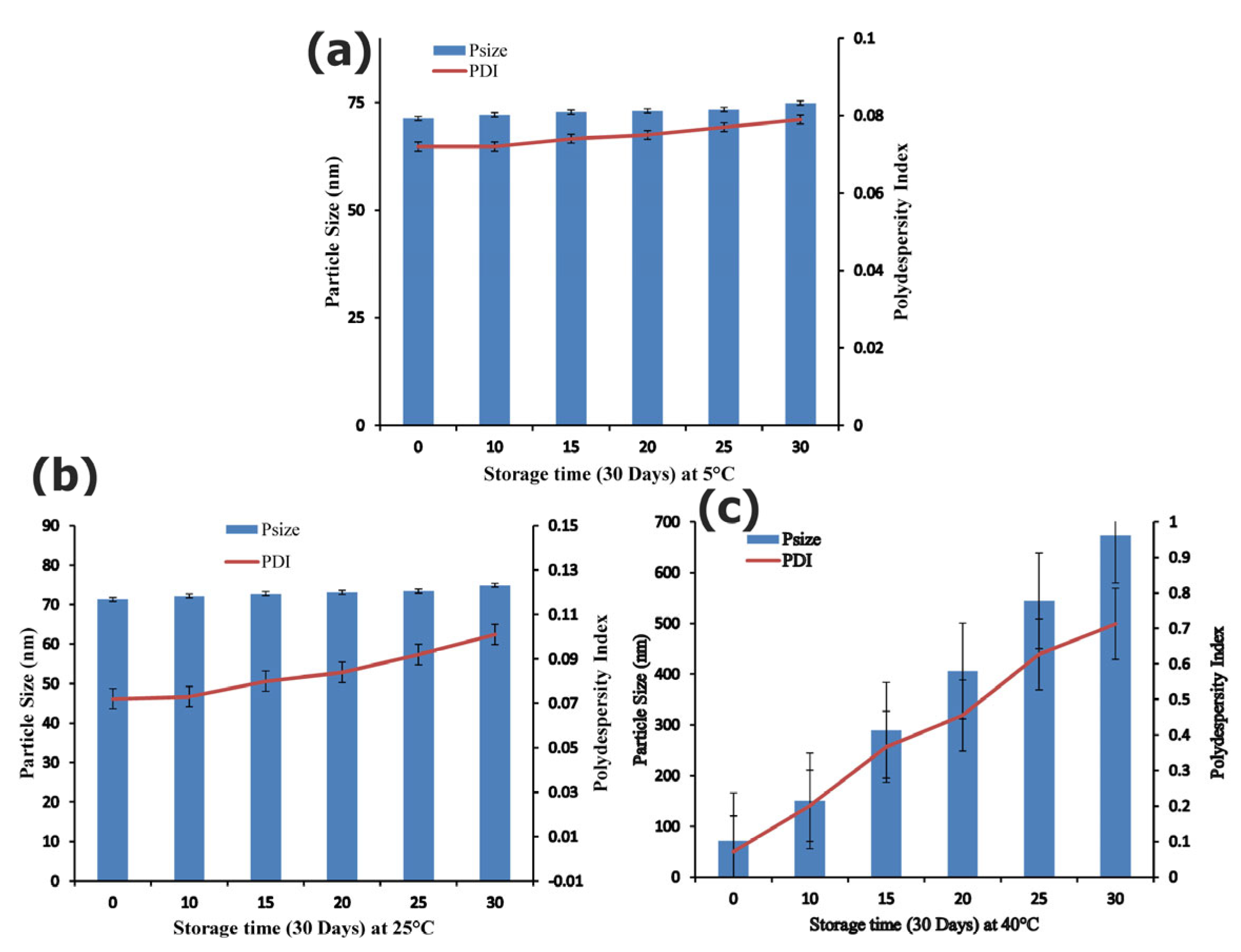
2.3.8. Assessment of Stability Studies
2.3.9. Dissolution Studies
2.4. Animals
2.5. Assessment of Acute Toxicity Study
2.6. Induction of Type II Diabetes
2.7. Experimental Design for Assessment of Antidiabetic Activity
2.8. Estimation of Blood Glucose Level and Body Weight
2.9. Assessment of Serum Profile
2.10. Statistical Analysis
3. Results and Discussion
3.1. Fabrication, Optimisation and Characterisation of Rp Nanoformulation
3.2. Stability Studies
3.3. DSC and P-XRD Studies
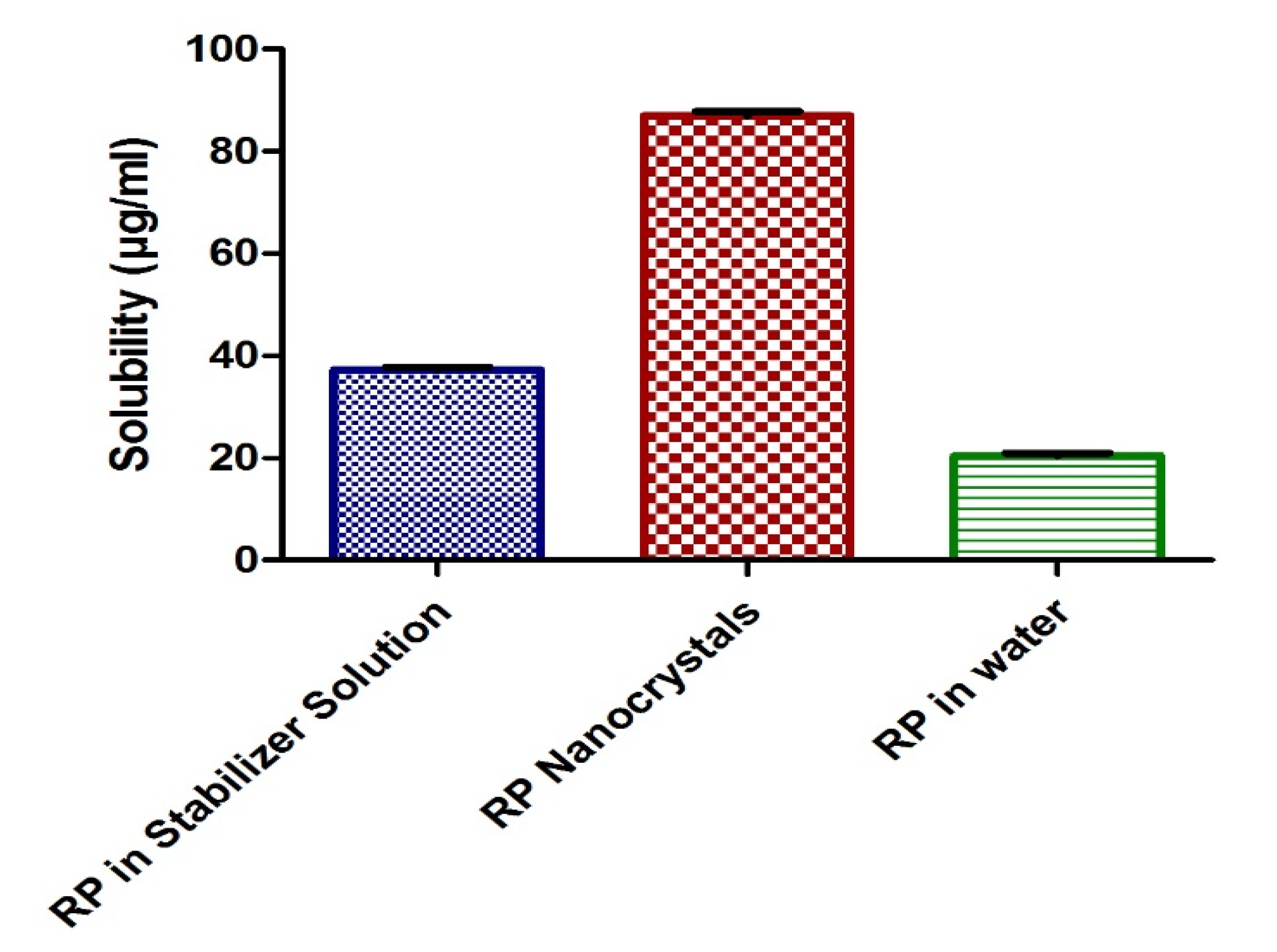
3.4. Solubility Studies
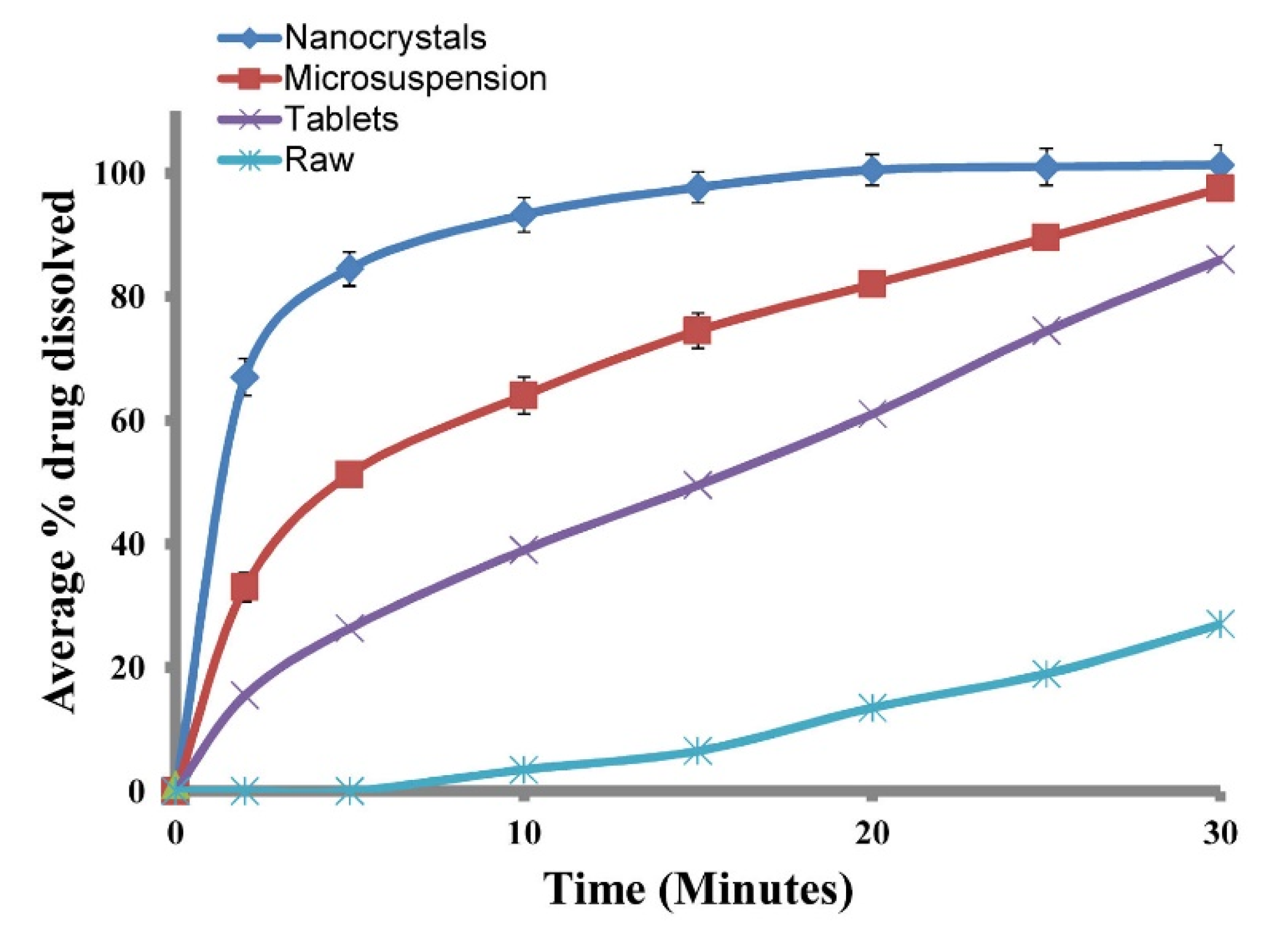
3.5. Dissolution Studies
3.6. Effect on Blood Glucose in Induced Diabetes
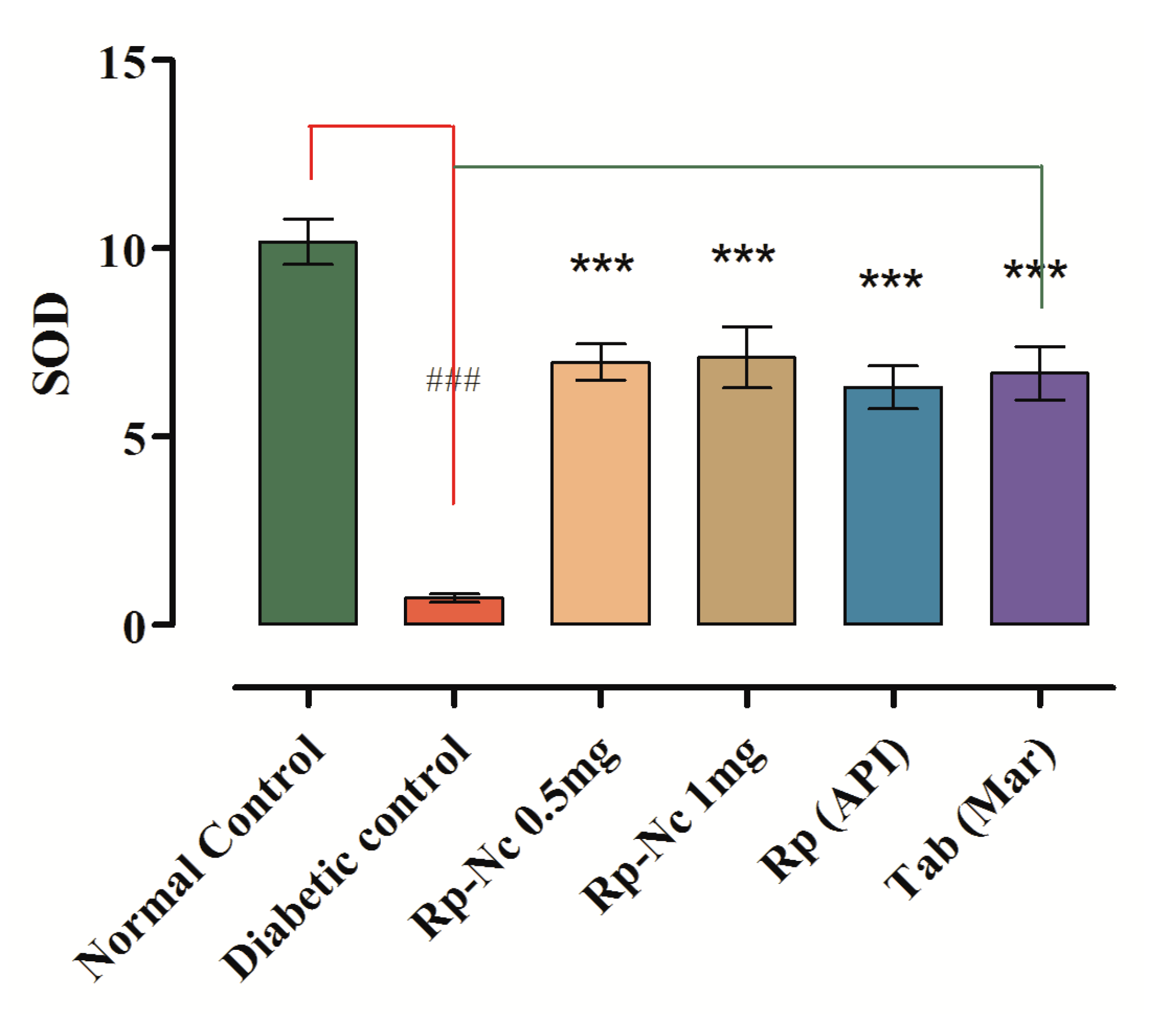
3.7. Antihyperlipidemic Effects of Rp-Nc on Induced Diabetes
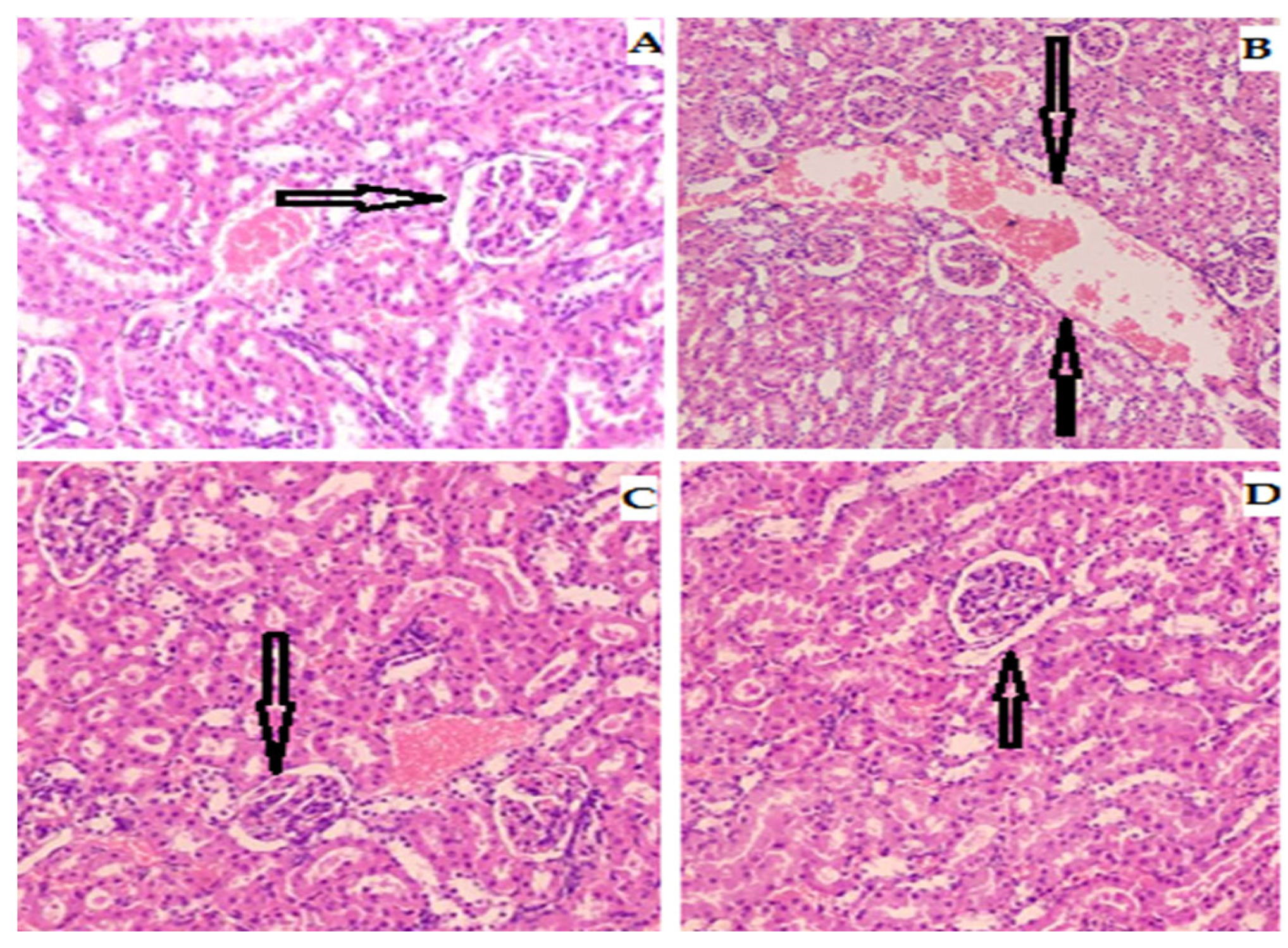
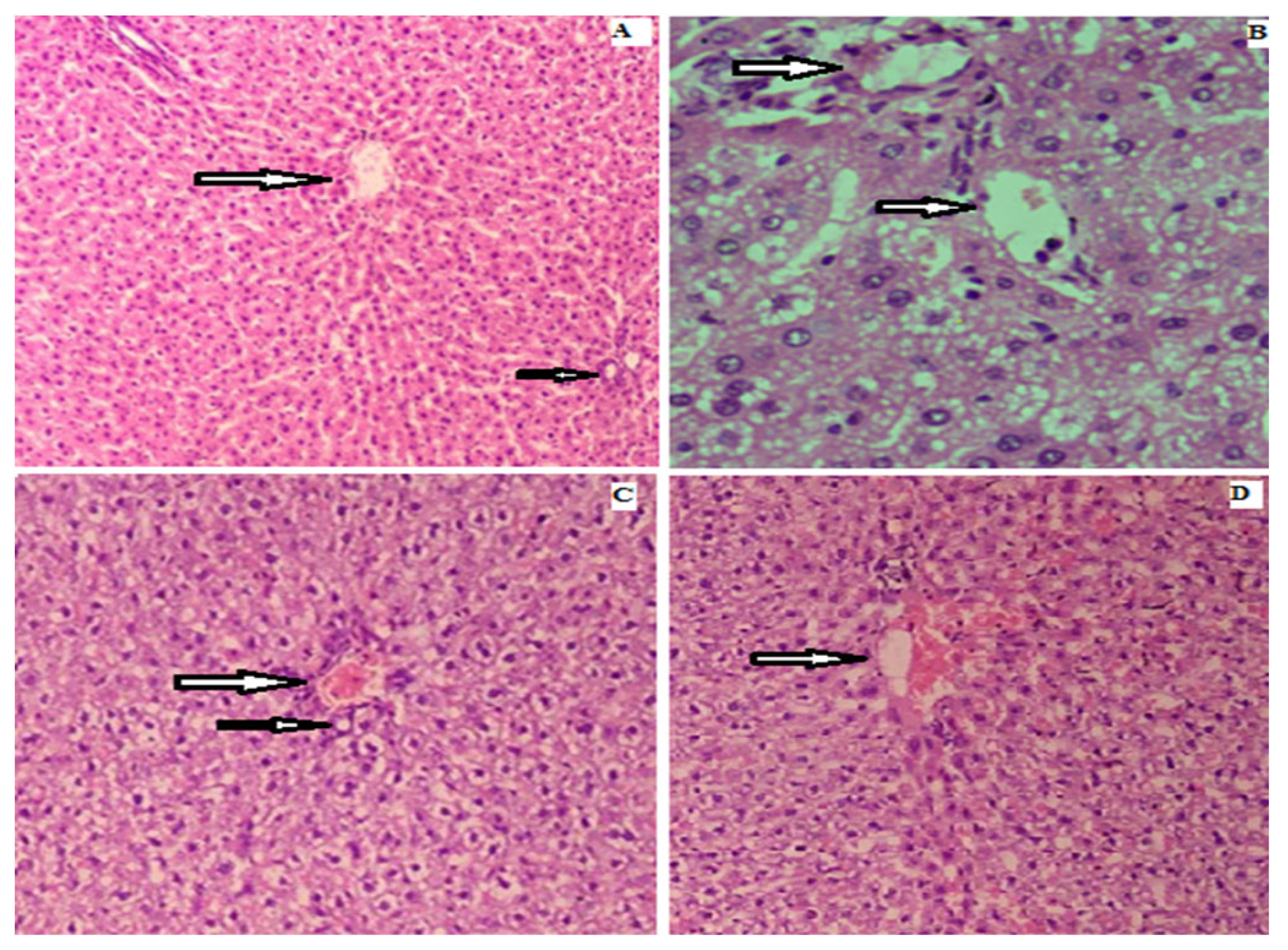
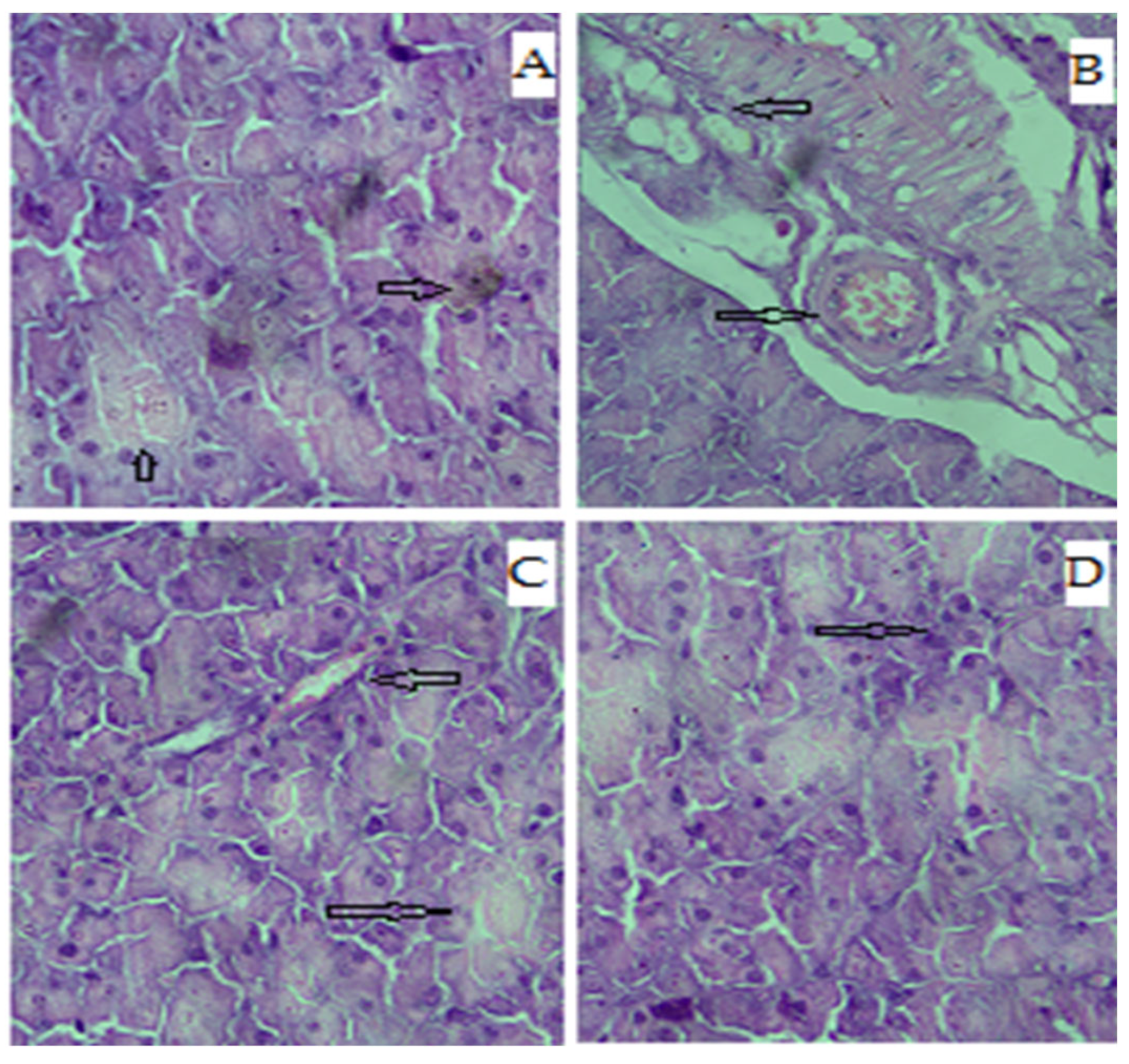
3.8. Effects on Liver
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ríos, J.L.; Francini, F.; Schinella, G.R. Natural products for the treatment of type 2 diabetes mellitus. Planta Med. 2015, 81, 975–994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patle, D.; Vyas, M.; Khatik, G.L. A review on natural products and herbs used in the management of diabetes. Curr. Diabetes Rev. 2021, 17, 186–197. [Google Scholar] [PubMed]
- Patterson, C.C.; Karuranga, S.; Salpea, P.; Saeedi, P.; Dahlquist, G.; Soltesz, G.; Ogle, G.D. Worldwide estimates of incidence, prevalence and mortality of type 1 diabetes in children and adolescents: Results from the International Diabetes Federation Diabetes Atlas. Diabetes Res. Clin. Pract. 2019, 157, 107842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Y.-C.; Chen, B.-H. A Comparative Study on Improving Streptozotocin-Induced Type 2 Diabetes in Rats by Hydrosol, Extract and Nanoemulsion Prepared from Cinnamon Leaves. Antioxidants 2022, 12, 29. [Google Scholar] [CrossRef] [PubMed]
- Yeung, A.W.K.; Tzvetkov, N.T.; Durazzo, A.; Lucarini, M.; Souto, E.B.; Santini, A.; Gan, R.-Y.; Jozwik, A.; Grzybek, W.; Horbańczuk, J.O. Natural products in diabetes research: Quantitative literature analysis. Nat. Prod. Res. 2021, 35, 5813–5827. [Google Scholar] [CrossRef]
- Rahman, M.M.; Islam, M.R.; Shohag, S.; Hossain, M.E.; Rahaman, M.S.; Islam, F.; Ahmed, M.; Mitra, S.; Khandaker, M.U.; Idris, A.M. The multifunctional role of herbal products in the management of diabetes and obesity: A comprehensive review. Molecules 2022, 27, 1713. [Google Scholar] [CrossRef]
- Vivó-Barrachina, L.; Rojas-Chacón, M.J.; Navarro-Salazar, R.; Belda-Sanchis, V.; Pérez-Murillo, J.; Peiró-Puig, A.; Herran-González, M.; Pérez-Bermejo, M. The Role of Natural Products on Diabetes Mellitus Treatment: A Systematic Review of Randomized Controlled Trials. Pharmaceutics 2022, 14, 101. [Google Scholar] [CrossRef]
- Van Heiningen, P.; Hatorp, V.; Kramer Nielsen, K.; Hansen, K.; Van Lier, J.; De Merbel, N.; Oosterhuis, B.; Jonkman, J. Absorption, metabolism and excretion of a single oral dose of 14C-repaglinide during repaglinide multiple dosing. Eur. J. Clin. Pharmacol. 1999, 55, 521–525. [Google Scholar] [CrossRef]
- Rawat, M.; Jain, A.; Mishra, A.; Muthu, M.; Singh, S. Development of repaglinide loaded solid lipid nanocarrier: Selection of fabrication method. Curr. Drug Deliv. 2010, 7, 44–50. [Google Scholar] [CrossRef]
- Derosa, G.; Mugellini, A.; Ciccarelli, L.; Crescenzi, G.; Fogari, R. Comparison of glycaemic control and cardiovascular risk profile in patients with type 2 diabetes during treatment with either repaglinide or metformin. Diabetes Res. Clin. Pract. 2003, 60, 161–169. [Google Scholar] [CrossRef]
- Poovi, G.; Kishore, N.; Reddy, P.N. In vitro characterization and in vivo toxicity study of repaglinide loaded poly (methyl methacrylate) nanoparticles. Int. J. Pharm. 2010, 396, 194–203. [Google Scholar]
- Auro Pharma Inc. PrAURO-REPAGLINIDE. 2016. Available online: https://pdf.hres.ca/dpd_pm/00034683.PDF (accessed on 1 January 2020).
- Foroumadi, R.; Baeeri, M.; Asgarian, S.; Emamgholipour, Z.; Goli, F.; Firoozpour, L.; Keykhaei, M.; Gholami, M.; Dehpour, A.R.; Abdollahi, M. Antidiabetic and neuroprotective effects of a novel repaglinide analog. J. Biochem. Mol. Toxicol. 2022, 36, e23125. [Google Scholar] [CrossRef]
- Hatorp, V. Clinical pharmacokinetics and pharmacodynamics of repaglinide. Clin. Pharmacokinet. 2002, 41, 471–483. [Google Scholar] [CrossRef]
- Karaźniewicz-Łada, M.; Bąba, K.; Dolatowski, F.; Dobrowolska, A.; Rakicka, M. The polymorphism of statins and its effect on their physicochemical properties. Polim Med 2018, 48, 77–82. [Google Scholar] [CrossRef] [Green Version]
- Yasir, M.; Asif, M.; Kumar, A.; Aggarval, A. Biopharmaceutical classification system: An account. Int. J. PharmTech Res. 2010, 2, 1681–1690. [Google Scholar]
- Amidon, G.L.; Lennernäs, H.; Shah, V.P.; Crison, J.R. A theoretical basis for a biopharmaceutic drug classification: The correlation of in vitro drug product dissolution and in vivo bioavailability. Pharm. Res. 1995, 12, 413–420. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.-Y.; Benet, L.Z. Predicting drug disposition via application of BCS: Transport/absorption/elimination interplay and development of a biopharmaceutics drug disposition classification system. Pharm. Res. 2005, 22, 11–23. [Google Scholar] [CrossRef]
- Löbenberg, R.; Amidon, G.L. Modern bioavailability, bioequivalence and biopharmaceutics classification system. New scientific approaches to international regulatory standards. Eur. J. Pharm. Biopharm. 2000, 50, 3–12. [Google Scholar] [CrossRef]
- Mansouri, M.; Pouretedal, H.R.; Vosoughi, V. Preparation and characterization of ibuprofen nanoparticles by using solvent/antisolvent precipitation. Open Conf. Proc. J. 2011, 2, 88–94. [Google Scholar] [CrossRef] [Green Version]
- Sachan, N.K.; Bhattacharya, A.; Pushkar, S.; Mishra, A. Biopharmaceutical classification system: A strategic tool for oral drug delivery technology. Asian J. Pharm. 2009, 3, 76. [Google Scholar] [CrossRef]
- Lonare, A.A.; Patel, S.R. Antisolvent crystallization of poorly water soluble drugs. Int. J. Chem. Eng. Appl. 2013, 4, 337. [Google Scholar] [CrossRef] [Green Version]
- Surendiran, A.; Sandhiya, S.; Pradhan, S.; Adithan, C. Novel applications of nanotechnology in medicine. Indian J. Med. Res. 2009, 130, 689–701. [Google Scholar] [PubMed]
- Demello, A.J. Control and detection of chemical reactions in microfluidic systems. Nature 2006, 442, 394–402. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Chan, H.F.; Leong, K.W. Advanced materials and processing for drug delivery: The past and the future. Adv. Drug Deliv. Rev. 2013, 65, 104–120. [Google Scholar] [CrossRef] [Green Version]
- Plakkot, S.; De Matas, M.; York, P.; Saunders, M.; Sulaiman, B. Comminution of ibuprofen to produce nano-particles for rapid dissolution. Int. J. Pharm. 2011, 415, 307–314. [Google Scholar] [CrossRef]
- Van Eerdenbrugh, B.; Vermant, J.; Martens, J.A.; Froyen, L.; Humbeeck, J.V.; Van den Mooter, G.; Augustijns, P. Solubility increases associated with crystalline drug nanoparticles: Methodologies and significance. Mol. Pharm. 2010, 7, 1858–1870. [Google Scholar] [CrossRef]
- Liu, G.; Xun, S.; Vukmirovic, N.; Song, X.; Olalde-Velasco, P.; Zheng, H.; Battaglia, V.S.; Wang, L.; Yang, W. Polymers with tailored electronic structure for high capacity lithium battery electrodes. Adv. Mater. 2011, 23, 4679–4683. [Google Scholar] [CrossRef] [Green Version]
- Thakkar, H.P.; Patel, B.V.; Thakkar, S.P. Development and characterization of nanosuspensions of olmesartan medoxomil for bioavailability enhancement. J. Pharm. Bioallied Sci. 2011, 3, 426. [Google Scholar] [CrossRef]
- Khan, S.; Matas, M.D.; Zhang, J.; Anwar, J. Nanocrystal preparation: Low-energy precipitation method revisited. Cryst. Growth Des. 2013, 13, 2766–2777. [Google Scholar] [CrossRef]
- Shekunov, B.Y.; Chattopadhyay, P.; Seitzinger, J.; Huff, R. Nanoparticles of poorly water-soluble drugs prepared by supercritical fluid extraction of emulsions. Pharm. Res. 2006, 23, 196–204. [Google Scholar] [CrossRef]
- Lorke, D. A new approach to practical acute toxicity testing. Arch. Toxicol. 1983, 54, 275–287. [Google Scholar] [CrossRef]
- Oguntibeju, O.O.; Meyer, S.; Aboua, Y.G.; Goboza, M. Hypoxis hemerocallidea Significantly Reduced Hyperglycaemia and Hyperglycaemic-Induced Oxidative Stress in the Liver and Kidney Tissues of Streptozotocin-Induced Diabetic Male Wistar Rats. Evid.-Based Complement. Altern. Med. 2016, 2016, 8934362. [Google Scholar] [CrossRef] [Green Version]
- Kumar, V.; Bhatt, P.C.; Kaithwas, G.; Rashid, M.; Al-abbasi, F.; Khan, J.A.; Anwar, F.; Verma, A. α-Mangostin Mediated Pharmacological Modulation of Hepatic Carbohydrate Metabolism in Diabetes Induced Wistar Rat. Beni-Suef Univ. J. Basic Appl. Sci. 2016, 5, 255–276. [Google Scholar] [CrossRef] [Green Version]
- Doğan, A.; Çelik, İ. Healing effects of sumac (Rhus coriaria) in streptozotocin-induced diabetic rats. Pharm. Biol. 2016, 54, 2092–2102. [Google Scholar] [CrossRef] [Green Version]
- Weibel, D.B.; Whitesides, G.M. Applications of microfluidics in chemical biology. Curr. Opin. Chem. Biol. 2006, 10, 584–591. [Google Scholar] [CrossRef]
- Ali, H.S.; York, P.; Blagden, N. Preparation of hydrocortisone nanosuspension through a bottom-up nanoprecipitation technique using microfluidic reactors. Int. J. Pharm. 2009, 375, 107–113. [Google Scholar] [CrossRef]
- Matteucci, M.E.; Hotze, M.A.; Johnston, K.P.; Williams, R.O. Drug nanoparticles by antisolvent precipitation: Mixing energy versus surfactant stabilization. Langmuir 2006, 22, 8951–8959. [Google Scholar] [CrossRef]
- Xia, D.; Quan, P.; Piao, H.; Piao, H.; Sun, S.; Yin, Y.; Cui, F. Preparation of stable nitrendipine nanosuspensions using the precipitation–ultrasonication method for enhancement of dissolution and oral bioavailability. Eur. J. Pharm. Sci. 2010, 40, 325–334. [Google Scholar] [CrossRef]
- Deng, J.; Huang, L.; Liu, F. Understanding the structure and stability of paclitaxel nanocrystals. Int. J. Pharm. 2010, 390, 242–249. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.Z.; Young, A.L.; Chiang, P.C.; Thurston, A.; Pretzer, D.K. Fluticasone and budesonide nanosuspensions for pulmonary delivery: Preparation, characterization, and pharmacokinetic studies. J. Pharm. Sci. 2008, 97, 4869–4878. [Google Scholar] [CrossRef]
- Jacobs, C.; Müller, R.H. Production and characterization of a budesonide nanosuspension for pulmonary administration. Pharm. Res. 2002, 19, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Zhang, J.; Watanabe, W. Physical and chemical stability of drug nanoparticles. Adv. Drug Del. Rev. 2011, 63, 456–469. [Google Scholar] [CrossRef] [PubMed]
- Freitas, C.; Müller, R.H. Effect of light and temperature on zeta potential and physical stability in solid lipid nanoparticle (SLN™) dispersions. Int. J. Pharm. 1998, 168, 221–229. [Google Scholar] [CrossRef]
- Bunjes, H.; Koch, M.H.; Westesen, K. Effect of particle size on colloidal solid triglycerides. Langmuir 2000, 16, 5234–5241. [Google Scholar] [CrossRef]
- Valleri, M.; Mura, P.; Maestrelli, F.; Cirri, M.; Ballerini, R. Development and evaluation of glyburide fast dissolving tablets using solid dispersion technique. Drug Dev. Ind. Pharm. 2004, 30, 525–534. [Google Scholar] [CrossRef]
- O’Mahony, M.; Leung, A.K.; Ferguson, S.; Trout, B.L.; Myerson, A.S. A Process for the Formation of Nanocrystals of Active Pharmaceutical Ingredients with Poor Aqueous Solubility in a Nanoporous Substrate. Org. Process Res. Dev. 2014, 19, 1109–1118. [Google Scholar] [CrossRef]
- Ali, H.S.; York, P.; Ali, A.M.; Blagden, N. Hydrocortisone nanosuspensions for ophthalmic delivery: A comparative study between microfluidic nanoprecipitation and wet milling. J. Control. Release 2011, 149, 175–181. [Google Scholar] [CrossRef]
- Müller, R.H.; Peters, K. Nanosuspensions for the formulation of poorly soluble drugs: I. Preparation by a size-reduction technique. Int. J. Pharm. 1998, 160, 229–237. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stabilizer/Surfactants | Concentration Stabilizer/Surfactants (%age w/w) | Flow Rate (µL/min) of Solvent/Antisolvent | Mean Particle Size (nm)/PDI | PDI |
|---|---|---|---|---|
| HPMC 15cps | 1 | 50:80 | 960 ± 44 | 0.89 ± 36 |
| PVP-K30 | 1 | 50:80 | 867 ± 21 | 0.94 ± 30 |
| PVA | 1 | 50:80 | 169 ± 34 | 0.32 ± 34 |
| HPMC + PVP-K30 | 0.5 + 0.5 | 50:80 | 902 ± 44 | 1 ± 45 |
| HPMC + P-F127 | 0.5 + 1 | 50:80 | 766 ± 54 | 1 ± 22 |
| HPMC + PVA | 0.5 + 0.5 | 50:80 | 937 ± 52 | 1 ± 43 |
| PVA + PVP-K30 | 1 + 1 | 50:80 | 633 ± 35 | 1 ± 24 |
| PVA + P-F127 | 1 + 2 | 50:80 | 413 ± 33 | 0.9 ± 33 |
| PVA + P-F68 | 1 + 2 | 50:80 | 783 ± 31 | 0.682 ± 31 |
| Concentration of PVA 1% (%ag w/w) | Flow Rate (µL/min) of Solvent/Antisolvent | Mean Particle Size (nm)/ | PDI |
|---|---|---|---|
| 1 | 50:50 | 245.32 ± 31 | 0.501 ± 22 |
| - | 50:60 | 223.44 ± 31 | 0.33 ± 32 |
| - | 50:70 | 209.91 ± 32 | 0.32 ± 43 |
| - | 50:80 | 180.33 ± 22 | 0.32 ± 34 |
| - | 50:90 | 134.31 ± 12 | 0.12 ± 13 |
| - | 50:100 | 113.99 ± 13 | 0.13 ± 23 |
| - | 50:110 | 91.43 ± 25 | 0.099 ± 22 |
| - | 50:120 | 71.31 ± 11 | 0.072 ± 12 |
| - | 50:130 | 77.25 ± 23 | 0.090 ± 22 |
| - | 50:140 | 81.33 ± 14 | 0.13 ± 34 |
| - | 50:150 | 141.13 ± 32 | 0.17 ± 41 |
| - | 50:160 | 199.43 ± 26 | 0.32 ± 32 |
| Blood Glucose Level/Day (mg/dL) | ||||||
|---|---|---|---|---|---|---|
| Groups/Treatment | 1st | 7th | 14th | 21st | 28th | |
| Normal control | 104.34 ± 3.89 | 102.67 ± 3.66 | 105.80 ± 3.89 | 109.04 ± 3.61 | 107.22 ± 3.50 | |
| Diabetic control | 498.07 ± 4.91 !!! | 501.45 ± 4.70 !!! | 504.39 ± 4.91 !!! | 490.72 ± 5.02 !!! | 486.65 ± 4.78 !!! | |
| Rp-Nc | 0.5 | 503.09 ± 5.11 | 397.38 ± 4.86 ** | 276.90 ± 4.67 *** | 170.81 ± 4.71 *** | 124.05 ± 3.07 *** |
| 1 | 499.37 ± 4.89 | 371.41 ± 4.59 ** | 239.75 ± 4.82 *** | 142.49 ± 4.66 *** | 115.54 ± 3.02 *** | |
| Rp (API) | 1 | 507.06 ± 5.09 | 412.16 ± 4.93 * | 294.61 ± 4.79 ** | 167.05 ± 4.58 *** | 121.42 ± 3.44 *** |
| Tab (Mar) | 1 | 497.46 ± 4.96 | 409.68 ± 5.09 * | 298.12 ± 4.88 ** | 171.59 ± 4.71 *** | 120.70 ± 3.60 *** |
| Changes in Weight of Animals/Day | ||||||
|---|---|---|---|---|---|---|
| Groups/Dose mg/kg | 1st | 7th | 14th | 21st | 28th | |
| Normal control | 190.11 ± 4.78 | 187.91 ± 4.71 | 192.08 ± 4.91 | 191.96 ± 4.89 | 196.41 ± 5.11 | |
| Diabetic control | 188.77 ± 5.10 | 182.69 ± 4.95 !!! | 176.21 ± 4.91 !!! | 158.93 ± 4.70 !!! | 147.16 ± 4.89 !!! | |
| Rp-Nc | 0.5 | 187.62 ± 4.97 | 187.02 ± 4.77 * | 184.21 ± 4.69 ** | 180.61 ± 4.91 *** | 176.44 ± 4.90 *** |
| 1 | 190.30 ± 4.42 | 188.21 ± 4.89 * | 186.05 ± 5.10 ** | 179.67 ± 4.82 * | 182.91 ± 4.88 ** | |
| Rp (API) | 1 | 186.59 ± 4.82 | 190.11 ± 4.94 * | 179.88 ± 4.98 ** | 177.29 ± 4.79 * | 173.86 ± 4.78 *** |
| Tab (Mar) | 1 | 191.03 ± 4.51 | 189.71 ± 4.94 * | 182.55 ± 4.79 ** | 183.08 ± 4.74 *** | 179.50 ± 4.68 * |
| Groups/Dose mg/kg | Total CH (mg/dL) | LDL (mg/dL) | TG (mg/dL) | HDL (mg/dL) | |
|---|---|---|---|---|---|
| Normal control | 68.25 ± 3.19 | 28.91 ± 1.91 | 71.98 ± 2.97 | 36.81 ± 2.48 | |
| Diabetic control | 235.49 ± 4.03 !!! | 112.50 ± 2.73 !!! | 196.33 ± 4.10 !!! | 20.11 ± 1.73 !!! | |
| RpNc | 0.5 | 78.09 ± 3.24 *** | 32.04 ± 1.61 *** | 84.17 ± 3.71 *** | 29.01 ± 1.87 *** |
| 1 | 74.40 ± 3.11 *** | 30.11 ± 1.87 *** | 76.06 ± 2.96 *** | 33.10 ± 2.29 *** | |
| Rp (API) | 1 | 81.11 ± 3.19 *** | 29.93 ± 1.94 *** | 85.37 ± 3.29 *** | 28.03 ± 2.01 *** |
| Tab (Mar) | 1 | 80.70 ± 3.06 *** | 28.55 ± 2.01 *** | 86.03 ± 3.11 *** | 27.55 ± 1.88 *** |
| Groups/Dose mg/kg | Insulin Level (μU/mL/day) | HbA1c(%) | ||
|---|---|---|---|---|
| 0 | 28 | -- | ||
| Normal control | 17.11 ± 0.29 | 18.05 ± 0.44 | 4.11 | |
| Diabetic control | 8.91 ± 0.48 | 7.98 ± 0.37 !!! | 10.61 !!! | |
| Rp-Nc | 0.5 | 8.74 ± 0.51 | 18.82 ± 0.69 *** | 4.32 *** |
| 1 | 8.94 ± 0.68 | 18.63 ± 0.41 *** | 4.21 *** | |
| Rp (API) | 1 | 8.78 ± 0.39 | 17.84 ± 0.51 *** | 5.02 *** |
| Tab (Mar) | 1 | 8.70 ± 0.45 | 18.01 ± 0.71 *** | 4.87 *** |
| Groups/Dose mg/kg | (ALP) IU | SGPT | Urea | Serum Creatinine (mg/dL) | |
|---|---|---|---|---|---|
| Normal control | 118.60 ± 2.86 | 60.48 ± 3.91 | 21.30 ± 1.88 | 0.63 ± 0.24 | |
| Diabetic control | 238.54 ± 4.11 !!! | 97.62 ± 4.08 !!! | 316.54 ± 4.03 !!! | 3.22 ± 0.51 !!! | |
| Rp-Nc | 0.5 | 152.82 ± 4.08 ** | 62.50 ± 3.70 *** | 64.18 ± 2.78 *** | 0.77 ± 0.48 *** |
| 1 | 147.17 ± 3.87 *** | 59.47 ± 3.59 *** | 61.30 ± 2.66 *** | 0.74 ± 0.36 *** | |
| Rp (API) | 1 | 159.30 ± 3.72 ** | 64.58 ± 3.66 ** | 66.15 ± 2.71 ** | 0.80 ± 0.31 *** |
| Groups/Dose mg/kg | SOD (mU/mg Protein) | CAT (mU/mg Protein) | TBARS (nmol MDA/mg Protein) | |
|---|---|---|---|---|
| Normal control | 10.18 ± 0.61 | 22.07 ± 0.82 | 1.35 ± 0.28 | |
| Diabetic control | 0.72 ± 0.11 !!! | 2.18 ± 0.29 !!! | 3.51 ± 0.43 !!! | |
| Rp-Nc | 0.5 | 6.98 ± 0.48 *** | 15.44 ± 1.03 *** | 2.48 ± 0.38 ** |
| 1 | 7.11 ± 0.81 *** | 16.29 ± 1.24 *** | 2.13 ± 0.29 *** | |
| Rp (API) | 1 | 6.31 ± 0.57 ** | 15.20 ± 1.01 ** | 2.55 ± 0.37 ** |
| Tab (Mar) | 1 | 6.69 ± 0.71 ** | 14.97 ± 1.08 ** | 2.51 ± 0.41 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmad, M.; Khan, S.; Shah, S.M.H.; Zahoor, M.; Hussain, Z.; Hussain, H.; Shah, S.W.A.; Ullah, R.; Alotaibi, A. Formulation and Optimization of Repaglinide Nanoparticles Using Microfluidics for Enhanced Bioavailability and Management of Diabetes. Biomedicines 2023, 11, 1064. https://doi.org/10.3390/biomedicines11041064
Ahmad M, Khan S, Shah SMH, Zahoor M, Hussain Z, Hussain H, Shah SWA, Ullah R, Alotaibi A. Formulation and Optimization of Repaglinide Nanoparticles Using Microfluidics for Enhanced Bioavailability and Management of Diabetes. Biomedicines. 2023; 11(4):1064. https://doi.org/10.3390/biomedicines11041064
Chicago/Turabian StyleAhmad, Mubashir, Shahzeb Khan, Syed Muhammad Hassan Shah, Muhammad Zahoor, Zahid Hussain, Haya Hussain, Syed Wadood Ali Shah, Riaz Ullah, and Amal Alotaibi. 2023. "Formulation and Optimization of Repaglinide Nanoparticles Using Microfluidics for Enhanced Bioavailability and Management of Diabetes" Biomedicines 11, no. 4: 1064. https://doi.org/10.3390/biomedicines11041064