
Novel Biomarkers for Early Detection of Acute Kidney Injury and Prediction of Long-Term Kidney Function Decline after Partial Nephrectomy
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
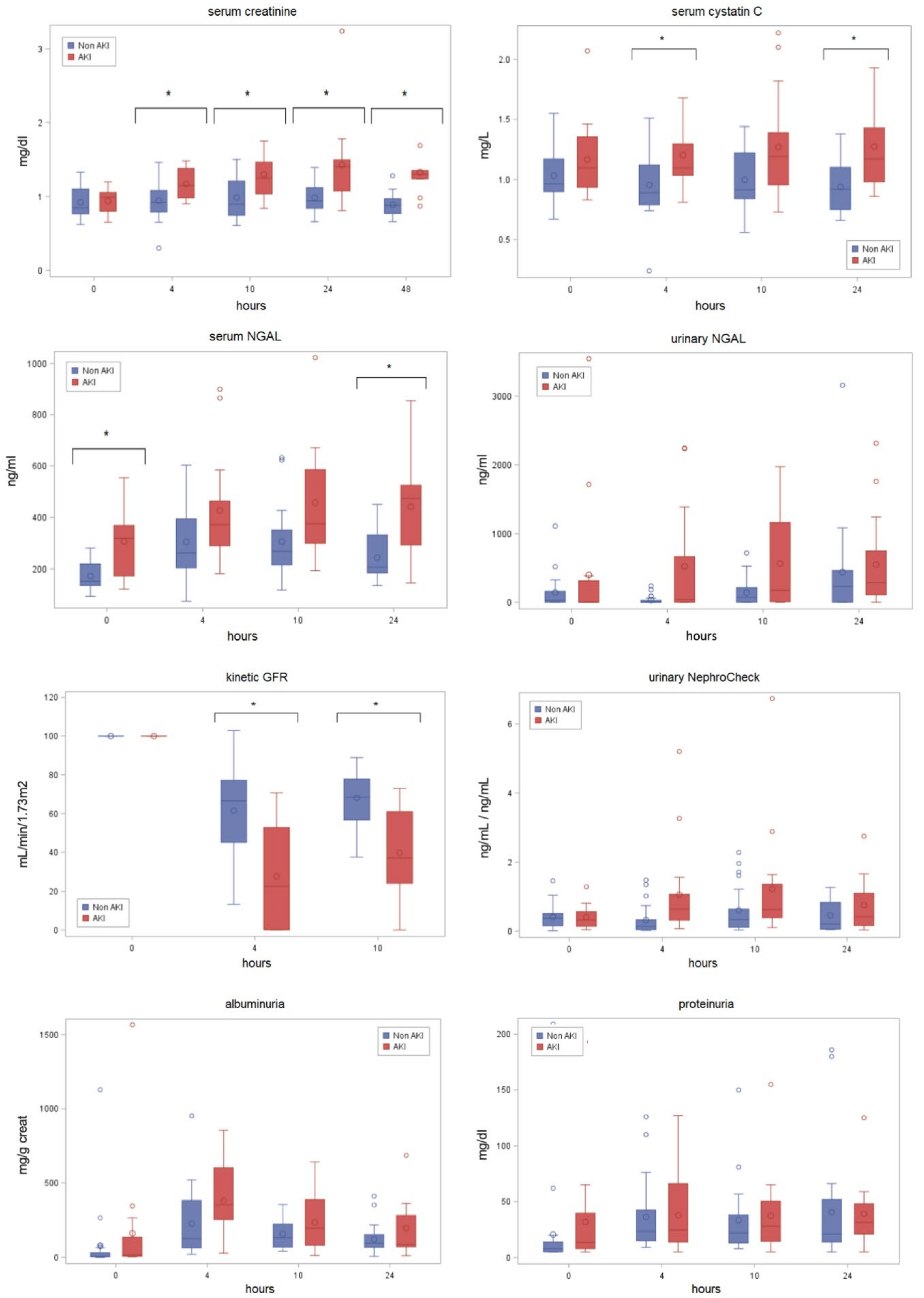
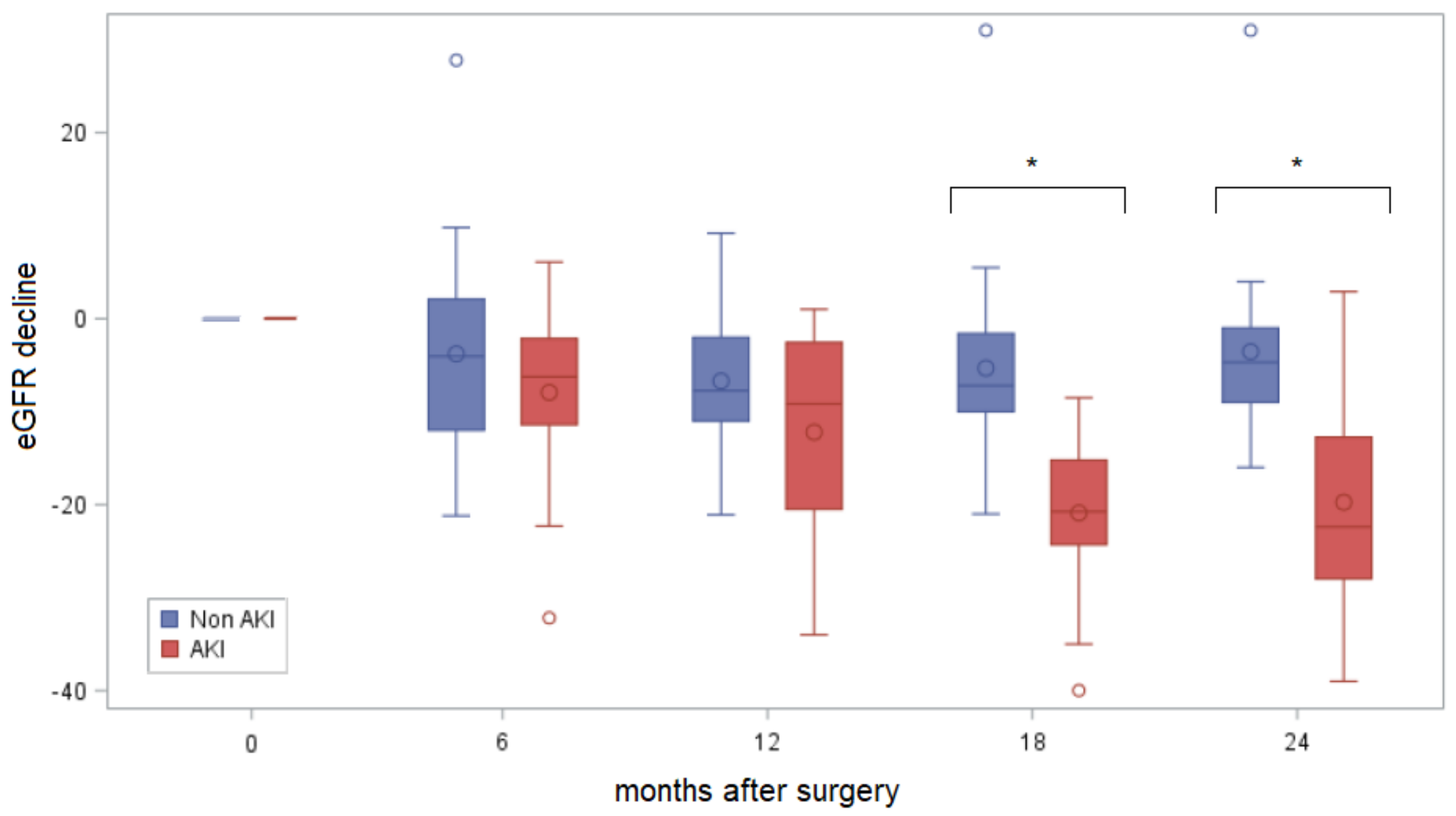
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Capitanio, U.; Larcher, A.; Cianflone, F.; Trevisani, F.; Nini, A.; Mottrie, A.; Mari, A.; Campi, R.; Tellini, R.; Briganti, A.; et al. Hypertension and Cardiovascular Morbidity Following Surgery for Kidney Cancer. Eur. Urol. Oncol. 2020, 3, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Leppert, J.T.; Lamberts, R.W.; Thomas, I.-C.; Chung, B.I.; Sonn, G.A.; Skinner, E.C.; Wagner, T.H.; Chertow, G.M.; Brooks, J.D. Incident CKD after radical or partial nephrectomy. J. Am. Soc. Nephrol. 2018, 29, 207–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nashar, K.; Egan, B.M. Relationship between chronic kidney disease and metabolic syndrome: Current perspectives. Diabetes Metab. Syndr. Obes. 2014, 7, 421–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.; Suk-Ouichai, C.; Dong, W.; Antonio, E.C.; Derweesh, I.H.; Lane, B.R.; Demirjian, S.; Li, J.; Campbell, S.C. Analysis of survival for patients with chronic kidney disease primarily related to renal cancer surgery. BJU Int. 2018, 121, 93–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonelli, A.; Minervini, A.; Sandri, M.; Bertini, R.; Bertolo, R.; Carini, M.; Furlan, M.; Larcher, A.; Mantica, G.; Mari, A.; et al. Below Safety Limits, Every Unit of Glomerular Filtration Rate Counts: Assessing the Relationship Between Renal Function and Cancer-specific Mortality in Renal Cell Carcinoma. Eur. Urol. 2018, 74, 661–667. [Google Scholar] [CrossRef] [PubMed]
- Ljungberg, B.; Albiges, L.; Abu-Ghanem, Y.; Bensalah, K.; Dabestani, S.; Fernández-Pello, S.; Giles, R.H.; Hofmann, F.; Hora, M.; Kuczyk, M.A.; et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2019 Update. Eur. Urol. 2019, 75, 799–810. [Google Scholar] [CrossRef]
- Antonelli, A.; Allinovi, M.; Cocci, A.; Russo, G.I.; Schiavina, R.; Rocco, B.; Giovannalberto, P.; Celia, A.; Galfano, A.; Varca, V.; et al. The Predictive Role of Biomarkers for the Detection of Acute Kidney Injury After Partial or Radical Nephrectomy: A Systematic Review of the Literature. Eur. Urol. Focus 2020, 6, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Patel, H.D.; Pierorazio, P.M.; Johnson, M.H.; Sharma, R.; Iyoha, E.; Allaf, M.E.; Bass, E.B.; Sozio, S.M. Renal Functional Outcomes after Surgery, Ablation, and Active Surveillance of Localized Renal Tumors: A Systematic Review and Meta-Analysis. Clin. J. Am. Soc. Nephrol. 2017, 12, 1057–1069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pierorazio, P.M.; Johnson, M.H.; Patel, H.D.; Sozio, S.; Sharma, R.; Iyoha, E.; Bass, E.; Allaf, M.E. Management of Renal Masses and Localized Renal Cancer: Systematic Review and Meta-Analysis. J. Urol. 2016, 196, 989–999. [Google Scholar] [CrossRef] [Green Version]
- Schmid, M.; Krishna, N.; Ravi, P.; Meyer, C.P.; Becker, A.; Dalela, D.; Sood, A.; Chun, F.K.-H.; Kibel, A.S.; Menon, M.; et al. Trends of acute kidney injury after radical or partial nephrectomy for renal cell carcinoma. Urol. Oncol. 2016, 34, 293.e1–293.e10. [Google Scholar] [CrossRef] [PubMed]
- Schmid, M.; Abd-El-Barr, A.E.R.; Gandaglia, G.; Sood, A.; Olugbade, K.; Ruhotina, N.; Sammon, J.D.; Varda, B.; Chang, S.L.; Kibel, A.S.; et al. Predictors of 30-day acute kidney injury following radical and partial nephrectomy for renal cell carcinoma. Urol. Oncol. 2014, 32, 1259–1266. [Google Scholar] [CrossRef]
- Peired, A.J.; Antonelli, G.; Angelotti, M.L.; Allinovi, M.; Guzzi, F.; Sisti, A.; Semeraro, R.; Conte, C.; Mazzinghi, B.; Nardi, S.; et al. Acute kidney injury promotes development of papillary renal cell adenoma and carcinoma from renal progenitor cells. Sci. Transl. Med. 2020, 12, eaaw6003. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Bellomo, R.; Ronco, C.; Kellum, J.A.; Mehta, R.L.; Palevsky, P.; Acute Dialysis Quality Initiative Workgroup. Acute renal failure-definition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care 2004, 8, R204–R212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horiguchi, Y.; Uchiyama, A.; Iguchi, N.; Sakai, K.; Hiramatsu, D.; Ueta, K.; Ohta, N.; Fujino, Y. Perioperative fluid balance affects staging of acute kidney injury in postsurgical patients: A retrospective case-control study. J. Intensiv. Care 2014, 2, 26. [Google Scholar] [CrossRef] [Green Version]
- Ronco, C.; Kellum, J.A.; Haase, M. Subclinical AKI is still AKI. Crit. Care 2012, 16, 313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parikh, C.R.; Puthumana, J.; Shlipak, M.G.; Koyner, J.L.; Thiessen-Philbrook, H.; McArthur, E.; Kerr, K.; Kavsak, P.; Whitlock, R.P.; Garg, A.X.; et al. Relationship of kidney injury biomarkers with long-term cardiovascular outcomes after cardiac surgery. J. Am. Soc. Nephrol. 2017, 28, 3699–3707. [Google Scholar] [CrossRef] [Green Version]
- Coca, S.G.; Garg, A.X.; Thiessen-Philbrook, H.; Koyner, J.L.; Patel, U.D.; Krumholz, H.M.; Shlipak, M.G.; Parikh, C.R. Urinary biomarkers of AKI and mortality 3 years after cardiac surgery. J. Am. Soc. Nephrol. 2014, 25, 1063–1071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- KDIGO AKI Work Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar]
- Zhang, D.; Yuan, Y.; Guo, L.; Wang, Q. Comparison of urinary TIMP-2 and IGFBP7 cut-offs to predict acute kidney injury in critically ill patients. Medicine 2019, 98, e16232. [Google Scholar] [CrossRef] [PubMed]
- Briguori, C.; Visconti, G.; Rivera, N.V.; Focaccio, A.; Golia, B.; Giannone, R.; Castaldo, D.; De Micco, F.; Ricciardelli, B.; Colombo, A. Cystatin C and contrast-induced acute kidney injury. Circulation 2010, 121, 2117–2122. [Google Scholar] [CrossRef] [PubMed]
- Yin, L.; Li, G.; Liu, T.; Yuan, R.; Zheng, X.; Xu, G.; Xu, Y.; Che, J.; Liu, X.; Ma, X.; et al. Probucol for the prevention of cystatin C-based contrast-induced acute kidney injury following primary or urgent angioplasty: A randomized, controlled trial. Int. J. Cardiol. 2013, 167, 426–429. [Google Scholar] [CrossRef]
- Chen, S. Retooling the creatinine clearance equation to estimate kinetic GFR when the plasma creatinine is changing acutely. J. Am. Soc. Nephrol. 2013, 24, 877–888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapman, D.; Moore, R.; Klarenbach, S.; Braam, B. Residual renal function after partial or radical nephrectomy for renal cell carcinoma. Can. Urol. Assoc. J. 2010, 4, 337–343. [Google Scholar] [CrossRef]
- Molinari, L.; Sakhuja, A.; Kellum, J.A. Perioperative Renoprotection: General Mechanisms and Treatment Approaches. Anesth. Analg. 2020, 131, 1679–1692. [Google Scholar] [CrossRef] [PubMed]
- Tourojman, M.; Kirmiz, S.; Boelkins, B.; Noyes, S.L.; Davis, A.T.; O’Donnell, K.; Tobert, C.M.; Lane, B.R. Impact of Reduced Glomerular Filtration Rate and Proteinuria on Overall Survival of Patients with Renal Cancer. J. Urol. 2016, 195, 588–593. [Google Scholar] [CrossRef]
- Ostermann, M.; Zarbock, A.; Goldstein, S.; Kashani, K.; Macedo, E.; Murugan, R.; Bell, M.; Forni, L.; Guzzi, L.; Joannidis, M.; et al. Recommendations on Acute Kidney Injury Biomarkers from the Acute Disease Quality Initiative Consensus Conference: A Consensus Statement. JAMA. Netw. Open 2020, 3, e2019209. [Google Scholar] [CrossRef] [PubMed]
- Matsushita, K.; Mahmoodi, B.K.; Woodward, M. Comparison of risk prediction using the CKD-EPI equation and the MDRD study equation for estimated glomerular filtration rate. JAMA 2012, 307, 1941–1951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siew, E.D.; Matheny, M.E.; Ikizler, T.A. Commonly used surrogates for baseline renal function affect the classification and prognosis of acute kidney injury. Kidney Int. 2010, 77, 536–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siew, E.D.; Matheny, M.E. Choice of reference serum creatinine in defining acute kidney injury. Nephron 2015, 131, 107–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnold, J.; Sims, D.; Gill, P. Acute kidney injury calculated using admission serum creatinine underestimates 30-day and 1-year mortality after acute stroke. Clin. Kidney J. 2019, 13, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Aloe, R.; Storelli, A. Evaluation of NGAL TestTM, a fully-automated neutrophil gelatinase-associated lipocalin (NGAL) immunoassay on Beckman Coulter AU 5822. Clin. Chem. Lab. Med. 2011, 50, 1581–1584. [Google Scholar] [PubMed]
- Liu, Y.; Chen, K.H.; Chen, S.Q. Predictive value of post-procedural early (within 24 h) increase in cystatin C for contrast-induced acute kidney injury and mortality following coronary angiography or intervention. Oncotarget 2017, 8, 109762–109771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kashani, K.; Al-Khafaji, A.; Ardiles, T. Discovery and validation of cell cycle arrest biomarkers in human acute kidney injury. Crit. Care 2013, 17, R25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, C.; Zhou, J.; Lu, Z.X. Simultaneous treatment of ureteropelvic junction obstruction complicated by renal calculi with robotic laparoscopic surgery and flexible cystoscope. World J. Urol. 2019, 37, 2217–2223. [Google Scholar] [CrossRef] [PubMed]
- Dewitte, A.; Joannès-Boyau, O.; Sidobre, C. Kinetic eGFR and novel AKI biomarkers to predict renal recovery. Clin. J. Am. Soc. Nephrol. 2015, 10, 1900–1910. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Tot | AKI | Non-AKI | p-Value | |
|---|---|---|---|---|
| Patients, n (%) | 38 | 16 (42%) | 22 (58%) | |
| Age (years) | 69.5 (62.0; 75.5) | 68.5 (62; 75.7) | 70 (62; 75.5) | 0.76 |
| Male gender, n (%) | 27 (71) | 13 (81.3) | 14 (63.6) | 0.30 |
| Preoperative comorbidities | ||||
| BMI | 26.3 (24.6; 29.4) | 27.3 (25.3; 29.3) | 26 (23.9; 29.4) | 0.98 |
| CKD, n (%) | 10 (26) | 5 (31.3) | 5 (22.7) | 0.83 |
| Diabetes, n (%) | 6 (16) | 2 (12.5) | 4 (18.2) | 1.0 |
| Heart disease, n (%) | 11 (29) | 3 (18.8) | 8 (36.4) | 0.30 |
| Hypertension, n (%) | 22 (58) | 10 (62.5) | 12 (54.5) | 0.52 |
| Preoperative laboratory values | ||||
| Hemoglobin (g/dL) | 14.5 (13.6; 15.5) | 14.6 (13.6; 15.8) | 14.5 (13.6; 15.5) | 0.69 |
| Serum creatinine (mg/dL) | 0.88 (0.78; 1.06) | 0.99 (0.8; 1.06) | 0.85 (0.77; 1.1) | 0.79 |
| Preoperative eGFR (mL/min/1.73 m2) | 78.6 (67.4; 85.0) | 72 (68; 84.6) | 79 (64; 86) | 0.94 |
| Preoperative biomarker values | ||||
| Cystatin C (mg/L) | 0.98 (0.92; 1.26) | 1.10 (0.94; 1.36) | 0.97 (0.90; 1.17) | 0.14 |
| Serum NGAL (ng/mL) | 180.8 (142.6; 299.5) | 319.5 (173.5; 370) | 152 (136; 219.5) | 0.002 |
| Urinary NGAL (ng/mL) | 4.0 (0.0; 227.9) | 0.0 (0.0; 314.7) | 25.2 (0.0; 161.3) | 0.87 |
| NephroCheck® Test | 0.35 (0.15; 0.53) | 0.33 (0.14; 0.56) | 0.38 (0.15; 0.51) | 0.98 |
| Proteinuria (mg/dL) | 10.5 (5; 16) | 13.5 (8; 39.5) | 8 (5; 14) | 0.09 |
| Proteinuria/Creatininuria | 0.13 (0.08; 0.26) | 0.15 (0.10; 0.35) | 0.11 (0.06; 0.22) | 0.21 |
| Albuminuria (mg/g) | 9.3 (4.9; 63) | 16.3 (6.7; 135.4) | 7.5 (3.7; 30.4) | 0.08 |
| Surgical parameters | ||||
| Tumor size (cm) | 3.5 (2.8; 4.8) | 3.1 (2.4; 4.3) | 3.8 (2.8; 4.8) | 0.32 |
| PADUA score | 8 (7; 10) | 8.5 (7; 10.5) | 8 (7; 9) | 0.53 |
| Warm ischemia time (min) | 12.5 (0; 20) | 13.5 (0; 21) | 12.5 (0; 20) | 0.80 |
| Operative time (min) | 170 (130; 195) | 175 (135; 208) | 170 (120; 190) | 0.76 |
| Outcome | ||||
| 12-month eGFR decline | −8.0 (−14; −2.1) | −9.15 (−20.5; −2.6) | −7.75 (−11; −2) | 0.07 |
| 24-month eGFR decline | −11.5 (−19.5; −5.0) | −20.75 (−24.3; −15.2) | −7.20 (−10; −1.6) | <0.0001 |
| 4 h after Surgery | 10 h after Surgery | |
|---|---|---|
| Serum creatinine increase > 0.3 sensitivity specificity | 25% ---- | 38% ---- |
| Urinary NephroCheck > 0.3 sensitivity specificity | 81% 73% | 88% 50% |
| kineticGFR reduction ≥ 50% sensitivity specificity | 56% 82% | 56% 100% |
| Serum Cystatin C increase ≥ 10% sensitivity specificity | 31% 96% | 50% 96% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Allinovi, M.; Sessa, F.; Villa, G.; Cocci, A.; Innocenti, S.; Zanazzi, M.; Tofani, L.; Paparella, L.; Curi, D.; Cirami, C.L.; et al. Novel Biomarkers for Early Detection of Acute Kidney Injury and Prediction of Long-Term Kidney Function Decline after Partial Nephrectomy. Biomedicines 2023, 11, 1046. https://doi.org/10.3390/biomedicines11041046
Allinovi M, Sessa F, Villa G, Cocci A, Innocenti S, Zanazzi M, Tofani L, Paparella L, Curi D, Cirami CL, et al. Novel Biomarkers for Early Detection of Acute Kidney Injury and Prediction of Long-Term Kidney Function Decline after Partial Nephrectomy. Biomedicines. 2023; 11(4):1046. https://doi.org/10.3390/biomedicines11041046
Chicago/Turabian StyleAllinovi, Marco, Francesco Sessa, Gianluca Villa, Andrea Cocci, Samantha Innocenti, Maria Zanazzi, Lorenzo Tofani, Laura Paparella, Dritan Curi, Calogero Lino Cirami, and et al. 2023. "Novel Biomarkers for Early Detection of Acute Kidney Injury and Prediction of Long-Term Kidney Function Decline after Partial Nephrectomy" Biomedicines 11, no. 4: 1046. https://doi.org/10.3390/biomedicines11041046