
The Role of Transcranial Magnetic Stimulation, Peripheral Electrotherapy, and Neurophysiology Tests for Managing Incomplete Spinal Cord Injury

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Healthy Subjects Included in the Study
2.2. Kinesiotherapy
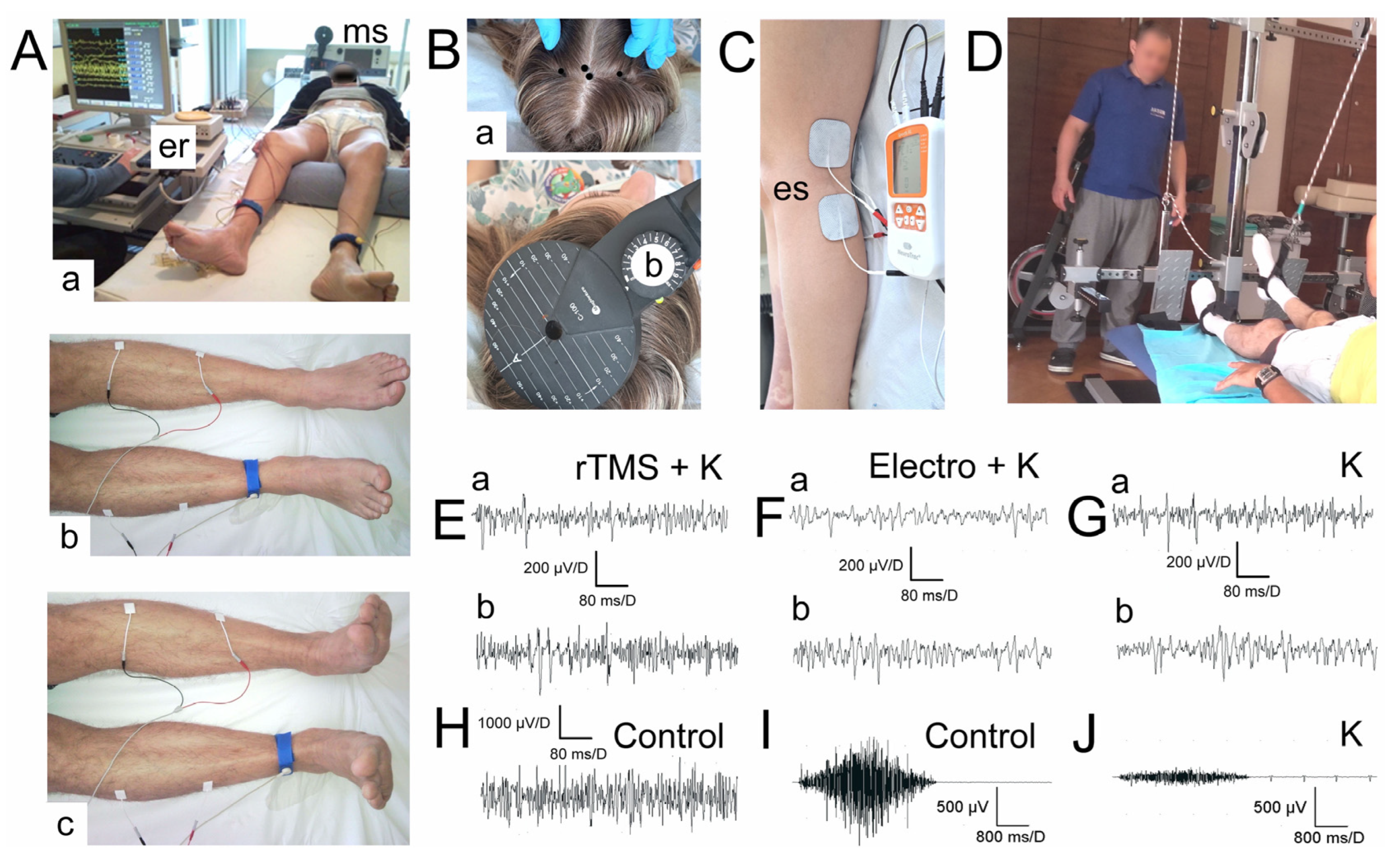
2.3. Transcranial Magnetic Stimulation (TMS)
2.4. Peripheral Electrotherapy
2.5. Neurophysiological Feedback
2.6. Statistical Analysis
3. Results
4. Discussion
5. Summary of Recommendation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bickenbach, J.; Officer, A.; Shakespeare, T.; von Groote, P.; World Health Organization; The International Spinal Cord Society. International Perspectives on Spinal Cord Injury/Edited by Jerome Bickenbach; World Health Organization: Geneva, Switzerland, 2013. Available online: https://apps.who.int/iris/handle/10665/94190 (accessed on 6 December 2022).
- National Spinal Cord Injury Statistical Center. 2021 Annual Report; National Spinal Cord Injury Statistical Center: Birmingham, AL, USA, 2021. [Google Scholar]
- Laliberte, A.M.; Goltash, S.; Lalonde, N.; Bui, T.V. Propriospinal Neurons: Essential Elements of Locomotor Control in the Intact and Possibly the Injured Spinal Cord. Front. Cell. Neurosci. 2019, 12, 512. [Google Scholar] [CrossRef] [Green Version]
- Alizadeh, A.; Dyck, S.M.; Karimi-Abdolrezaee, S. Traumatic Spinal Cord Injury: An Overview of Pathophysiology, Models and Acute Injury Mechanisms. Front. Neurol. 2019, 10, 282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leemhuis, E.; Favieri, F.; Forte, G.; Pazzaglia, M. Integrated Neuroregenerative Techniques for Plasticity of the Injured Spinal Cord. Biomedicines 2022, 10, 2563. [Google Scholar] [CrossRef] [PubMed]
- Davletshin, E.; Sabirov, D.; Rizvanov, A.; Mukhamedshina, Y. Combined Approaches Leading to Synergistic Therapeutic Effects in Spinal Cord Injury: State of the Art. Front. Biosci. 2022, 27, 334. [Google Scholar] [CrossRef] [PubMed]
- Fawcett, J.W.; Curt, A.; Steeves, J.D.; Coleman, W.P.; Tuszynski, M.H.; Lammertse, D.; Bartlett, P.F.; Blight, A.R.; Dietz, V.; Ditunno, J.; et al. Guidelines for the Conduct of Clinical Trials for Spinal Cord Injury as Developed by the ICCP Panel: Spontaneous Recovery after Spinal Cord Injury and Statistical Power Needed for Therapeutic Clinical Trials. Spinal Cord 2007, 45, 190–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.Y.; Park, C.; Zhang, H.; Rahimpour, S.; Murphy, K.R.; Goodwin, C.R.; Karikari, I.O.; Than, K.D.; Shaffrey, C.I.; Foster, N.; et al. Management of Acute Traumatic Spinal Cord Injury: A Review of the Literature. Front. Surg. 2021, 8, 698736. [Google Scholar] [CrossRef] [PubMed]
- Tabakow, P.; Jarmundowicz, W.; Czapiga, B.; Fortuna, W.; Miedzybrodzki, R.; Czyz, M.; Huber, J.; Szarek, D.; Okurowski, S.; Szewczyk, P.; et al. Transplantation of Autologous Olfactory Ensheathing Cells in Complete Human Spinal Cord Injury. Cell Transplant. 2013, 22, 1591–1612. [Google Scholar] [CrossRef]
- James, N.D.; McMahon, S.B.; Field-Fote, E.C.; Bradbury, E.J. Neuromodulation in the Restoration of Function after Spinal Cord Injury. Lancet Neurol. 2018, 17, 905–917. [Google Scholar] [CrossRef] [Green Version]
- Belci, M.; Catley, M.; Husain, M.; Frankel, H.L.; Davey, N.J. Magnetic brain stimulation can improve clinical outcome in incomplete spinal cord injured patients. Spinal Cord 2004, 42, 417–419. [Google Scholar] [CrossRef]
- Kumru, H.; Murillo, N.; Vidal Samso, J.; Valls-Sole, J.; Edwards, D.; Pelayo, R.; Valero-Cabre, A.; Tormos, J.M.; Pascual-Leone, A. Reduction of Spasticity with Repetitive Transcranial Magnetic Stimulation in Patients with Spinal Cord Injury. Neurorehabilit. Neural Repair 2010, 24, 435–441. [Google Scholar] [CrossRef]
- Kuppuswamy, A.; Balasubramaniam, A.V.; Maksimovic, R.; Mathiasm, C.J.; Gall, A.; Craggs, M.D.; Ellaway, P.H. Action of 5 Hz repetitive transcranial magnetic stimulation on sensory, motor and autonomic function in human spinal cord injury. Clin. Neurophysiol. 2011, 122, 2452–2461. [Google Scholar] [CrossRef] [PubMed]
- Benito, J.; Kumru, H.; Murillo, N.; Costa, U.; Medina, J.; Tormos, J.; Pascual-Leone, A.; Vidal, J. Motor and Gait Improvement in Patients With Incomplete Spinal Cord Injury Induced by High-Frequency Repetitive Transcranial Magnetic Stimulation. Top. Spinal Cord Inj. Rehabil. 2012, 18, 106–112. [Google Scholar] [CrossRef] [Green Version]
- Wincek, A.; Huber, J.; Leszczyńska, K.; Fortuna, W.; Okurowski, S.; Chmielak, K.; Tabakow, P. The Long-Term Effect of Treatment Using the Transcranial Magnetic Stimulation RTMS in Patients after Incomplete Cervical or Thoracic Spinal Cord Injury. JCM 2021, 10, 2975. [Google Scholar] [CrossRef] [PubMed]
- Huber, J.; Leszczyńska, K.; Wincek, A.; Szymankiewicz-Szukała, A.; Fortuna, W.; Okurowski, S.; Tabakow, P. The Role of Peripheral Nerve Electrotherapy in Functional Recovery of Muscle Motor Units in Patients after Incomplete Spinal Cord Injury. Appl. Sci. 2021, 11, 9764. [Google Scholar] [CrossRef]
- Zheng, Y.; Mao, Y.R.; Yuan, T.F.; Xu, D.S.; Cheng, L.M. Multimodal treatment for spinal cord injury: A sword of neuroregeneration upon neuromodulation. Neural Regen. Res. 2020, 15, 1437–1450. [Google Scholar] [PubMed]
- Vasanthan, L.T.; Nehrujee, A.; Solomon, J.; Tilak, M. Electrical Stimulation for People with Spinal Cord Injury. Cochrane Database Syst. Rev. 2019, 2019, CD013481. [Google Scholar] [CrossRef]
- Wincek, A.; Huber, J.; Leszczyńska, K.; Fortuna, W.; Okurowski, S.; Tabakow, P. The Results of a Long Term Uniform System of Neurorehabilitation in Patients with Incomplete Thoracic Spinal Cord Injury. Ann. Agric. Environ. Med. 2021, 29, 94–102. [Google Scholar] [CrossRef]
- Harvey, L.A. Physiotherapy rehabilitation for people with spinal cord injuries. J. Physiother. 2016, 62, 4–11. [Google Scholar] [CrossRef] [Green Version]
- Awad, B.I.; Carmody, M.A.; Zhang, X.; Lin, V.W.; Steinmetz, M.P. Transcranial Magnetic Stimulation After Spinal Cord Injury. World Neurosurg. 2015, 83, 232–235. [Google Scholar] [CrossRef]
- Rossi, S.; Antal, A.; Bestmann, S.; Bikson, M.; Brewer, C.; Brockmöller, J.; Carpenter, L.L.; Cincotta, M.; Chen, R.; Daskalakis, J.D.; et al. Safety and Recommendations for TMS Use in Healthy Subjects and Patient Populations, with Updates on Training, Ethical and Regulatory Issues: Expert Guidelines. Clin. Neurophysiol. 2021, 132, 269–306. [Google Scholar] [CrossRef]
- Ellaway, P. Induction of Central Nervous System Plasticity by Repetitive Transcranial Magnetic Stimulation to Promote Sensorimotor Recovery in Incomplete Spinal Cord Injury. Front. Integr. Neurosci. 2014, 8, 42. [Google Scholar] [CrossRef] [Green Version]
- Gajewska-Woźniak, O.; Skup, M.; Kasicki, S.; Ziemlińska, E.; Czarkowska-Bauch, J. Enhancing Proprioceptive Input to Motoneurons Differentially Affects Expression of Neurotrophin 3 and Brain-Derived Neurotrophic Factor in Rat Hoffmann-Reflex Circuitry. PLoS ONE 2013, 8, e65937. [Google Scholar] [CrossRef] [PubMed]
- Baldi, J.C.; Jackson, R.D.; Moraille, R.; Mysiw, W.J. Muscle Atrophy Is Prevented in Patients with Acute Spinal Cord Injury Using Functional Electrical Stimulation. Spinal Cord 1998, 36, 463–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, K.M.; Curran, M.W.T.; Gordon, T. The Use of Brief Post-Surgical Low Frequency Electrical Stimulation to Enhance Nerve Regeneration in Clinical Practice: Use of Brief Post-Surgical Low Frequency Electrical Stimulation. J. Physiol. 2016, 594, 3553–3559. [Google Scholar] [CrossRef] [Green Version]
- Kern, H.; Carraro, U.; Adami, N.; Biral, D.; Hofer, C.; Forstner, C.; Mödlin, M.; Vogelauer, M.; Pond, A.; Boncompagni, S.; et al. Home-Based Functional Electrical Stimulation Rescues Permanently Denervated Muscles in Paraplegic Patients with Complete Lower Motor Neuron Lesion. Neurorehabilit. Neural Repair 2010, 24, 709–721. [Google Scholar] [CrossRef]
- Günter, C.; Delbeke, J.; Ortiz-Catalan, M. Correction to: Safety of Long-Term Electrical Peripheral Nerve Stimulation: Review of the State of the Art. J. NeuroEng. Rehabil. 2020, 17, 77. [Google Scholar] [CrossRef]
- Lee, M.; Kiernan, M.C.; Macefield, V.G.; Lee, B.B.; Lin, C.S.-Y. Short-Term Peripheral Nerve Stimulation Ameliorates Axonal Dysfunction after Spinal Cord Injury. J. Neurophysiol. 2015, 113, 3209–3218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pieber, K.; Herceg, M.; Paternostro-Sluga, T.; Schuhfried, O. Optimizing Stimulation Parameters in Functional Electrical Stimulation of Denervated Muscles: A Cross-Sectional Study. J. NeuroEng. Rehabil. 2015, 12, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nardone, R.; Höller, Y.; Thomschewski, A.; Brigo, F.; Orioli, A.; Höller, P.; Golaszewski, S.; Trinka, E. RTMS Modulates Reciprocal Inhibition in Patients with Traumatic Spinal Cord Injury. Spinal Cord 2014, 52, 831–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Araújo, A.V.L.; Barbosa, V.R.N.; Galdino, G.S.; Fregni, F.; Massetti, T.; Fontes, S.L.; de Oliveira Silva, D.; da Silva, T.D.; Monteiro, C.B.D.M.; Tonks, J.; et al. Effects of High-Frequency Transcranial Magnetic Stimulation on Functional Performance in Individuals with Incomplete Spinal Cord Injury: Study Protocol for a Randomized Controlled Trial. Trials 2017, 18, 522. [Google Scholar] [CrossRef] [Green Version]
- Chail, A.; Saini, R.; Bhat, P.; Srivastava, K.; Chauhan, V. Transcranial Magnetic Stimulation: A Review of Its Evolution and Current Applications. Ind. Psychiatry J. 2018, 27, 172. [Google Scholar] [PubMed]
- Arora, T.; Desai, N.; Kirshblum, S.; Chen, R. Utility of Transcranial Magnetic Stimulation in the Assessment of Spinal Cord Injury: Current Status and Future Directions. Front. Rehabil. Sci. 2022, 3, 1005–1111. [Google Scholar] [CrossRef] [PubMed]
- Perez, M.A.; Field-Fote, E.C.; Floeter, M.K. Patterned Sensory Stimulation Induces Plasticity in Reciprocal Ia Inhibition in Humans. J. Neurosci. 2003, 23, 2014–2018. [Google Scholar] [CrossRef] [Green Version]
- Wincek, A.; Wietrzak, P.; Mielewczyk, Z.; Kędzia, G.; Mieczyński, K.; Leszczyńska, K. Review of effective nerve electrostimulation parameters applied for treatment of patients after incomplete spinal cord injuries. Issue Rehabil. Orthop. Neurophysiol. Sport Promot. 2020, 31, 25–33. [Google Scholar]
- Brihmat, N.; Allexandre, D.; Saleh, S.; Zhong, J.; Yue, G.H.; Forrest, G.F. Stimulation Parameters Used During Repetitive Transcranial Magnetic Stimulation for Motor Recovery and Corticospinal Excitability Modulation in SCI: A Scoping Review. Front. Hum. Neurosci. 2022, 16, 800349. [Google Scholar] [CrossRef] [PubMed]
- Balbinot, G. Surface EMG in Subacute and Chronic Care after Traumatic Spinal Cord Injuries. Trauma Care 2022, 2, 381–391. [Google Scholar] [CrossRef]
- Korupolu, R.; Stampas, A.; Singh, M.; Zhou, P.; Francisco, G. Electrophysiological Outcome Measures in Spinal Cord Injury Clinical Trials: A Systematic Review. Top. Spinal Cord Inj. Rehabil. 2019, 25, 340–354. [Google Scholar] [CrossRef]
- Zholudeva, L.V.; Qiang, L.; Marchenko, V.; Dougherty, K.J.; Sakiyama-Elbert, S.E.; Lane, M.A. The Neuroplastic and Therapeutic Potential of Spinal Interneurons in the Injured Spinal Cord. Trends Neurosci. 2018, 41, 625–639. [Google Scholar] [CrossRef] [Green Version]
- Gordon, T. Electrical Stimulation to Enhance Axon Regeneration After Peripheral Nerve Injuries in Animal Models and Humans. Neurotherapeutics 2016, 13, 295–310. [Google Scholar] [CrossRef] [Green Version]
- Grau, J.W. Learning from the Spinal Cord: How the Study of Spinal Cord Plasticity Informs Our View of Learning. Neurobiol. Learn. Mem. 2014, 108, 155–171. [Google Scholar] [CrossRef] [Green Version]
- Wise, Y. Electrical Stimulation and Motor Recovery. Cell Transplant. 2015, 24, 429–446. [Google Scholar]
- Curt, A.; Schwab, M.E.; Dietz, V. Providing the Clinical Basis for New Interventional Therapies: Refined Diagnosis and Assessment of Recovery after Spinal Cord Injury. Spinal Cord 2004, 42, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curt, A.; Van Hedel, H.J.A.; Klaus, D.; Dietz, V.; EM-SCI Study Group. Recovery from a Spinal Cord Injury: Significance of Compensation, Neural Plasticity, and Repair. J. Neurotrauma 2008, 25, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.; Xiang, Z.; Yan, R.; Zhao, M.; Wu, Y.; Zhong, J.; Guo, L.; Li, H.; Wang, J.; Wu, J.; et al. Motor Recovery at 6 Months after Admission Is Related to Structural and Functional Reorganization of the Spine and Brain in Patients with Spinal Cord Injury: Neural Correlates of Motor Recovery After SCI. Hum. Brain Mapp. 2016, 37, 2195–2209. [Google Scholar] [CrossRef]
- Kubaszewski, Ł.; Wojdasiewicz, P.; Rożek, M.; Słowińska, I.E.; Romanowska-Próchnicka, K.; Słowiński, R.; Poniatowski, Ł.A.; Gasik, R. Syndromes with chronic non-bacterial osteomyelitis in the spine. Reumatologia 2015, 53, 328–336. [Google Scholar] [CrossRef] [Green Version]
- Tykocki, T.; Poniatowski, Ł.A.; Czyz, M.; Wynne-Jones, G. Oblique corpectomy in the cervical spine. Spinal Cord 2018, 56, 426–435. [Google Scholar] [CrossRef] [Green Version]
- De Miguel-Rubio, A.; Muñoz-Pérez, L.; Alba-Rueda, A.; Arias-Avila, M.; Rodrigues-de-Souza, D.P. A Therapeutic Approach Using the Combined Application of Virtual Reality with Robotics for the Treatment of Patients with Spinal Cord Injury: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 8772. [Google Scholar] [CrossRef]


{kind=link}
| Variable Patients Group | Age (Years) | Height (cm) | Weight (kg) | Averaged Time from Injury (Months) | Averaged Observation Time (Before–After) (Months) | ASIA AIS Score | Injury Level |
|---|---|---|---|---|---|---|---|
| rTMS + K 12♀, 23♂ N = 35 | 23–51 38.1 ± 3.5 | 157–178 170.1 ± 2.9 | 50–86 60.7 ± 4.1 | 6.7 ± 1.4 | 8.9 | C = 26 D = 9 | C4–C8 = 18 Th1–Th12 = 17 |
| Electro + K 23♀, 42♂ N = 65 | 25–56 37.2 ± 4.1 | 161–184 172.1 ± 3.6 | 50–85 62.1 ± 4.3 | 7.4 ± 1.9 | 9.9 | C = 54 D = 11 | C4–C8 = 29 Th1–Th12 = 36 |
| K 18♀, 37♂ N = 55 | 24–53 37.4 ± 3.6 | 159–183 173.2 ± 3.6 | 49–84 63.5 ± 3.7 | 7.1 ± 1.8 | 8.7 | C = 46 D = 9 | C4–C8 = 27 Th1–Th12 = 28 |
| rTMS 12♀, 22♂ N = 34 | 25–58 38.1 ± 3.3 | 163–180 174.2 ± 3.2 | 51–84 64.6 ± 3.7 | 6.9 ± 1.6 | 8.4 | C = 24 D = 10 | C4–C8 = 15 Th1–Th12 = 19 |
| Electro 19♀, 34♂ N = 53 | 24–60 38.1 ± 4.0 | 158–179 175.4 ± 3.8 | 50—80 62.8 ± 3.6 | 6.7± 1.2 | 8.7 | C = 45 D = 8 | C4–C8 = 24 Th1–Th12 = 29 |
| p-value (difference) rTMS + K vs. Electro + K Electro + K vs. K rTMS + K vs. K rTMS + K vs. rTMS rTMS vs. Electro rTMS vs. K Electro vs. K | NS NS NS NS NS NS NS | NS NS 0.05 0.05 NS NS 0.05 | 0.05 NS 0.05 0.05 0.05 NS NS | 0.05 NS 0.05 NS NS NS NS | NS 0.05 NS NS NS NS NS | NA NA NA NA NA NA NA | NA NA NA NA NA NA NA |
| Groups of Patients | rTMS + K | Electro + K | K | rTMS | Electro | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Parameter | Before | After | Before | After | Before | After | Before | After | Before | After |
| TA sEMG Amplitude (μV) Frequency index | 50–2100 232.7 ± 94.5 1–3 1.5 ± 0.6 | 50–2300 343.0 ± 79.2 1–3 1.7 ± 0.5 | 50–2000 191.4 ± 94.7 1–3 1.4 ± 0.5 | 50–2400 344.2 ± 88.3 1–3 1.8 ± 0.5 | 50–1900 221.0 ± 87.1 1–3 1.4 ± 0.5 | 50–2000 259.3 ± 93.8 1–3 1.5 ± 0.6 | 50–2000 229.3 ± 83.1 1–3 1.5 ± 0.4 | 50–2300 311.9 ± 81.6 1–3 1.7 ± 0.6 | 50–2000 210.5 ± 85.6 1–3 1.5 ± 0.5 | 50–2300 290.6 ± 82.1 1–3 1.8 ± 0.5 |
| Neurophysiological improvement (before vs. after) Amplitude (μV) Frequency index | 0.008 0.05 | 32.1% 11.7% | 0.009 0.04 | 44.4% 22.2% | 0.05 NS | 14.8% 6.6% | 0.03 0.05 | 26.4% 11.7% | 0.03 0.05 | 27.5% 16.6% |
| Recording | Parameter | Healthy Volunteers (Control) | |
|---|---|---|---|
| TA sEMG | Amplitude (µV) | 600–2450 | 785.3 ± 100.2 |
| Frequency index | 3–3 | 3.0 ± 0.5 | |
| Reference | No of Patients Who Received Stimulation | Stimulation Algorithm | Interval between Trains of Stimuli | Intensity of Stimulation, Maximal % Stimulus Output | Number of Sessions Per Day, Week, Month | Evaluation Method of Effectiveness |
|---|---|---|---|---|---|---|
| Belci et al., 2004 [11] | 4 | 10 Hz 720 pulses in total | 100 ms | 90% | 5 sessions of 1 h, one per day | ASIA scale 5 days of sham rTMS delivered over the occipital cortex |
| Kumru et al., 2010 [12] | 15 | 20 Hz 40 pulses in a train 1600 pulses in total | 28 s | 90% | 15 sessions, 5 per week, 3 weeks of observation in total | Clinical evaluation of spasticity, EMG Sham stimulation with a coil disconnected from the main stimulator unit |
| Kuppuswamy et al., 2011 [13] | 15 | 5 Hz 900 pulses in total | 8 s | 80% | 5 days, 1 per day (sham or active, randomly) | ASIA scale, upper limb functional tests, MEP, autonomic measures; sham stimulation with only 5% of real stimulator output |
| Benito et al., 2012 [14] | 7 | 20 Hz 40 pulses in a train, 1800 pulses in total, 20 trains | 28 s | 90% | 15 days, 1 per day (sham or active) | Functional gait assessment and clinical spasticity assessment Double-blind, sham-controlled trial; sham stimulation with a coil disconnected from the main stimulator unit |
| Nardone et al., 2014 [31] | 9 | 20 Hz 1600 pulses in total | 28 s | 100% | 4 days, 1 session per day | Clinical evaluation of spasticity, EMG Sham stimulation with a coil disconnected from the main stimulator unit |
| De Araujo et al., 2017 [32] | 10 | 5 Hz 50 pulses in a train 12 trains | 10 s | 100% | 10 sessions over 2 weeks | ASIA scale, Fugl–Meyer scale, Modified Ashworth Scale, socio-demographic questionnaire, Mini-Mental State Examination, EMG, EEG 5 sessions active and 5 blind for each person, with a two-week washout period |
| Wincek et al., 2021 [32] | 26 | 15–25 Hz 40 pulses in a train, 20 trains 1600 pulses in total | 28 s | 38–40% | 3–5 sessions per month for 5 months | sEMG, MEP; results were compared to patients treated with kinesiotherapy alone |
| Reference | No of Patients | Place of Stimulation | Stimulation Frequency (Hz) and Train Duration (s) | Single Stimulus Duration and Strength (mA), Interval between Trains of Stimuli | Observation Time (Months), Numbers of Session | Evaluation Method of Effectiveness | Additional Comments |
|---|---|---|---|---|---|---|---|
| Baldi et al., 1998 [25] | 26 | hip extensors, knee extensors and knee flexors | 60 Hz | 0.375 ms 140 mA | 6 months 3 times per week 30 min per day | Total body lean body mass, lower limb lean body mass, and gluteal lean body mass assessed by using dual-energy X-ray absorptiometry | All the parameters were fixed and the same for all the patients |
| Kern et al., 2010 [27] | 22 | leg muscles | - | 12–150 ms 250 mA | 2 years 5 times a week 30 min per day | EMG, knee torque measurement every 12 weeks, muscle cross-sectional area measured by computed tomography, muscle biopsies | Home-based therapy |
| Pieber et al., 2015 [30] | 24 | tibialis anterior muscle | 1 Hz | 200 ms 500 ms 8 mA | 4 sessions, 1–2 min each | Medical Research Council Scale Intensity was recorded in absolute values in mA and relatively provided in percentage to the first stimulation of each patient. | - |
| Lee et al., 2015 [29] | 22 | median and common peroneal nerves | 100 Hz 2 s | 0.4 ms 12–30 mA | 6 weeks, 5 days a week 30 min per day | EMG ENG non-stimulated leg used as a control | All the parameters were fixed and the same for all the patients |
| Zheng et al., 2020 [17] | 5 | knee extensors | 30 Hz | 30–99 mA | 12 weeks of therapy, sessions twice a week | Quadriceps femoris torque, blood lipid profilin, c-reactive protein, spasticity evaluation, quality of life index | - |
| Huber et al., 2021 [16] | 42 | peroneal and tibial nerves | 20–70 Hz 2–3 s | 11–22 ms 18–45 mA 2–3 s | 6–14 months, 5 days a week, 15–20 min per day | EMG ENG Results were compared to patients treated with kinesiotherapy alone | Home-based therapy Stimulus strength was the only parameter adjusted by patients |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leszczyńska, K.; Huber, J. The Role of Transcranial Magnetic Stimulation, Peripheral Electrotherapy, and Neurophysiology Tests for Managing Incomplete Spinal Cord Injury. Biomedicines 2023, 11, 1035. https://doi.org/10.3390/biomedicines11041035
Leszczyńska K, Huber J. The Role of Transcranial Magnetic Stimulation, Peripheral Electrotherapy, and Neurophysiology Tests for Managing Incomplete Spinal Cord Injury. Biomedicines. 2023; 11(4):1035. https://doi.org/10.3390/biomedicines11041035
Chicago/Turabian StyleLeszczyńska, Katarzyna, and Juliusz Huber. 2023. "The Role of Transcranial Magnetic Stimulation, Peripheral Electrotherapy, and Neurophysiology Tests for Managing Incomplete Spinal Cord Injury" Biomedicines 11, no. 4: 1035. https://doi.org/10.3390/biomedicines11041035