
Differences in the Profile of Circulating Immune Cell Subsets in Males with Type 2 Cardiorenal Syndrome versus CKD Patients without Established Cardiovascular Disease

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
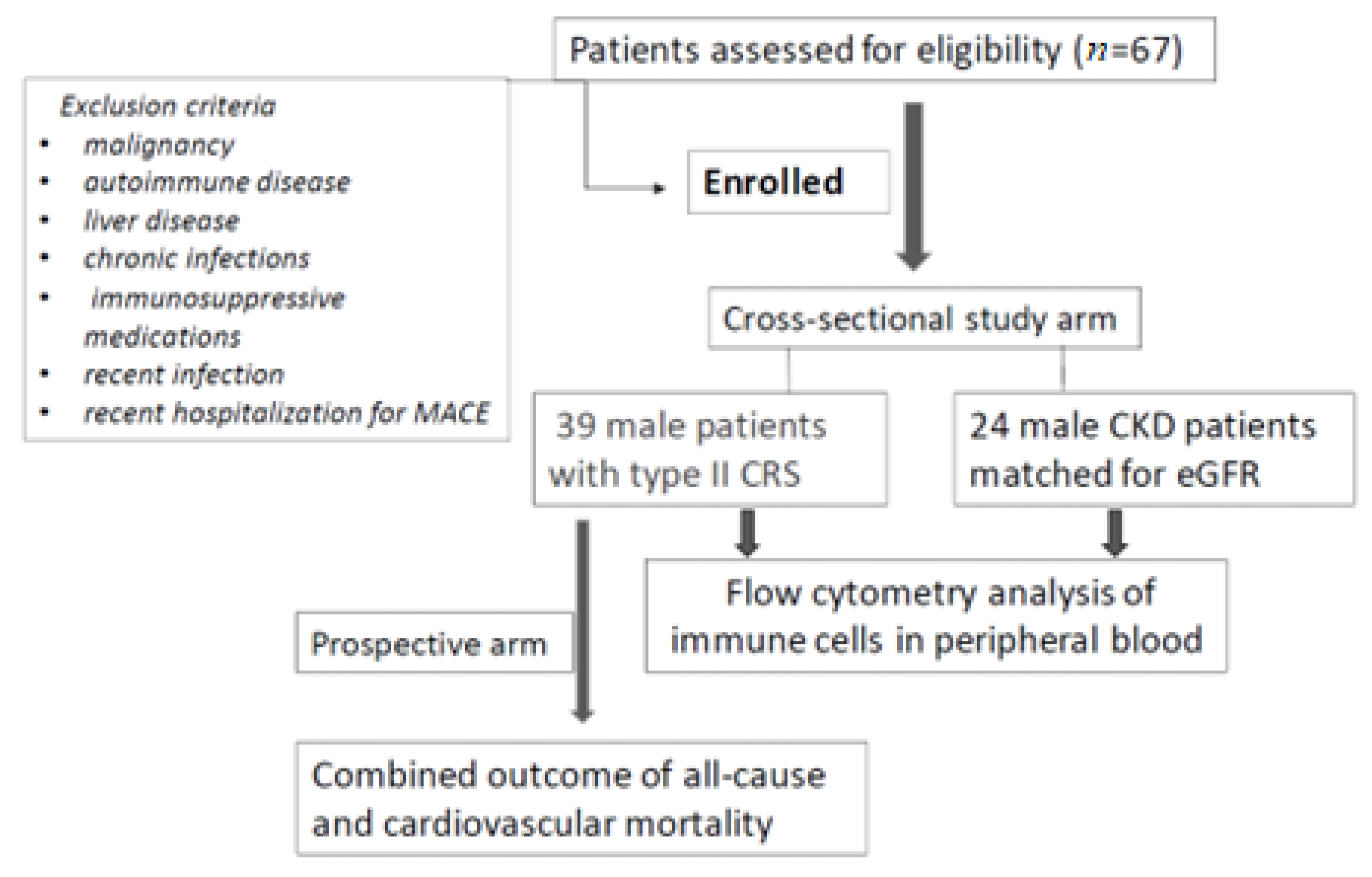
2.1. Study Cohort
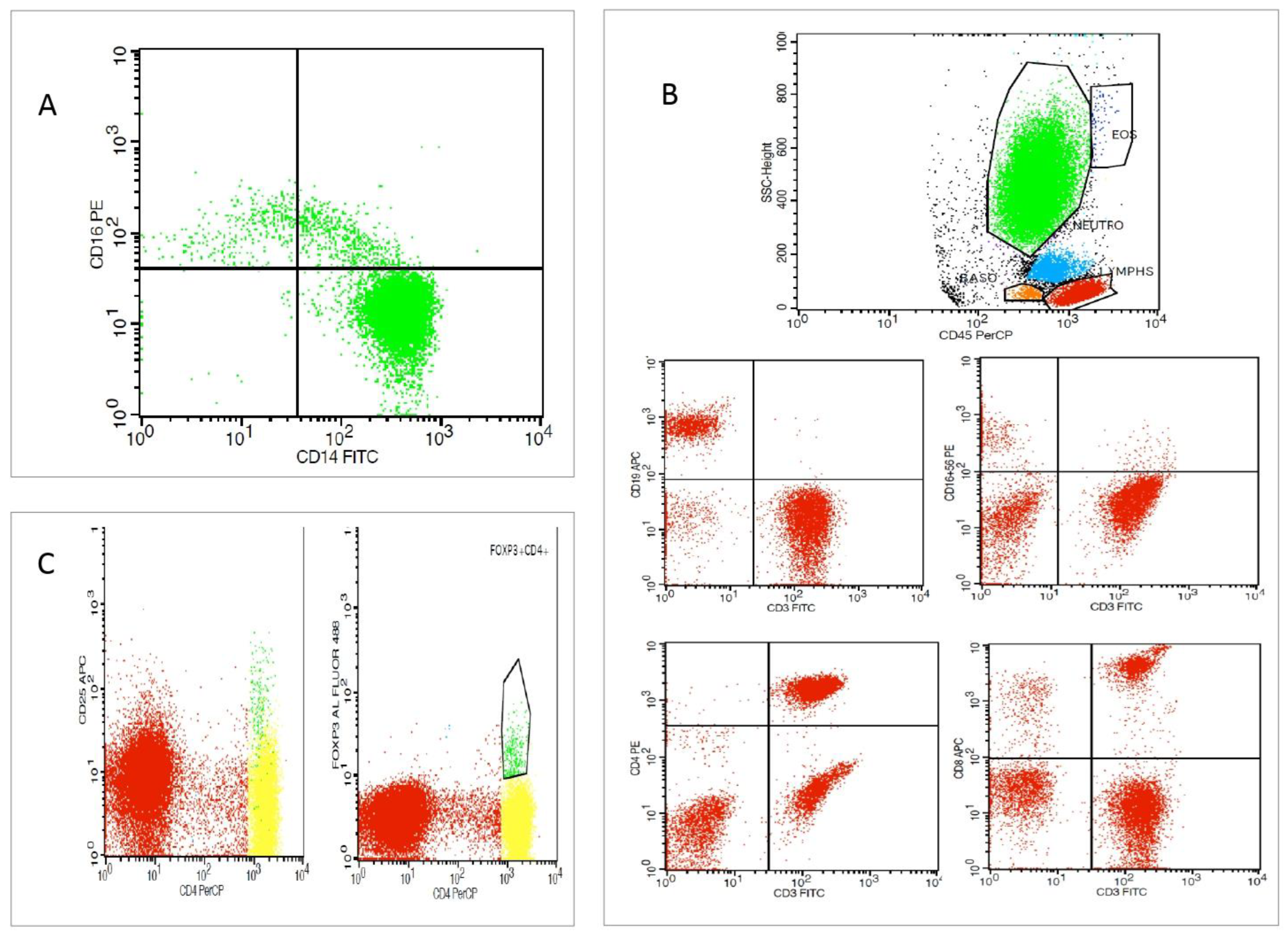
2.2. Evaluation of Specific Immune Cell Subsets
2.3. Clinical and Laboratory Assessment
2.4. Prospective Follow-Up and Study Endpoint
2.5. Statistical Analysis
3. Results
3.1. Differences in the Profile of Immune Cell Subset Expression between Patients with Type 2 CRS versus CKD Patients
3.2. Immune Cell Subset Expression in Patients with Type 2 CRS
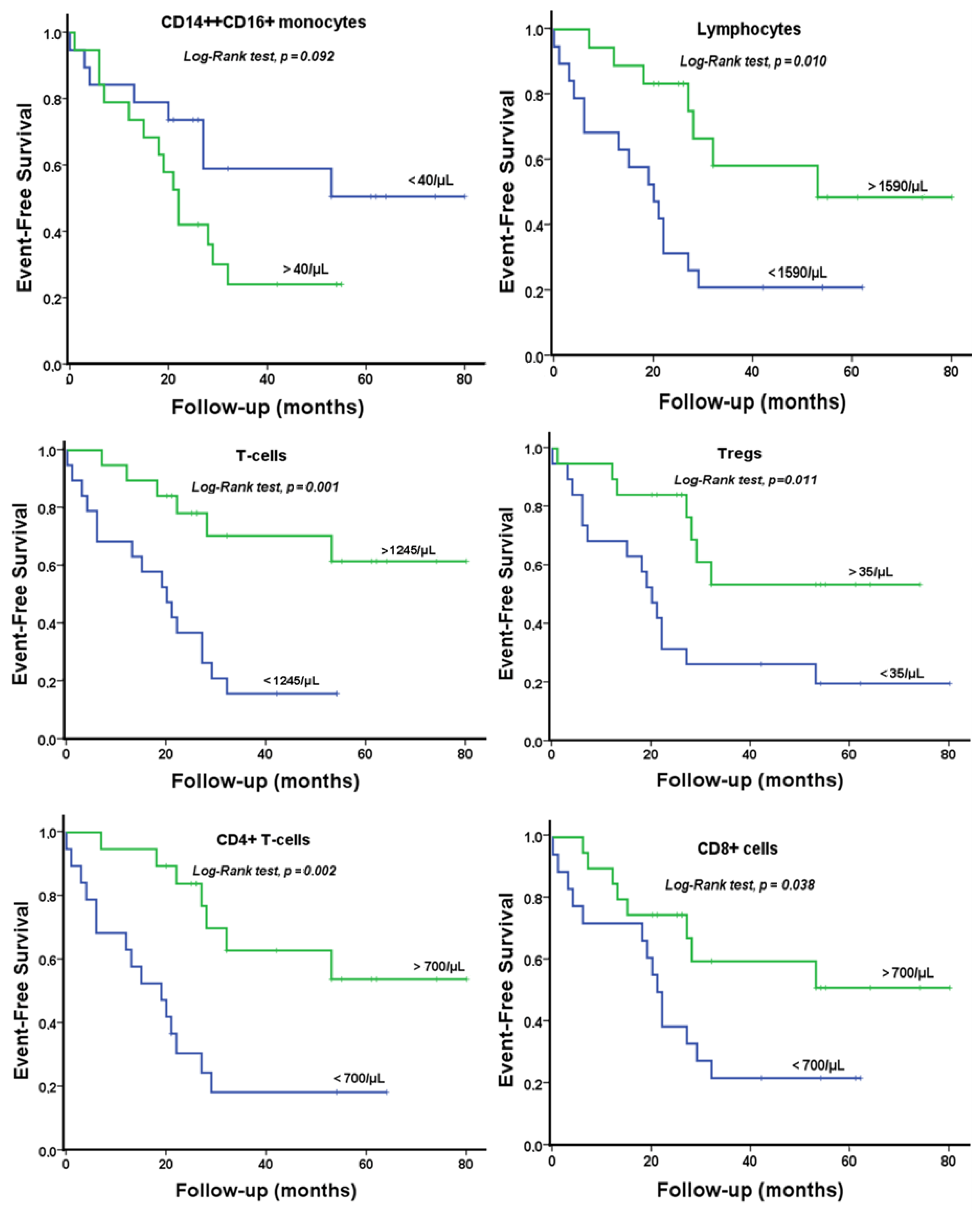
3.3. Survival Analyses in Type 2 CRS Patients Categorized by Circulating Immune Cell Subset Expression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Libby, P.; Mallat, Z.; Weyand, C. Immune and inflammatory mechanisms mediate cardiovascular diseases from head to toe. Cardiovasc. Res. 2021, 117, 2503–2505. [Google Scholar] [CrossRef] [PubMed]
- Zoccali, C. Traditional and emerging cardiovascular and renal risk factors: An epidemiologic perspective. Kidney Int. 2006, 70, 26–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, J.; Mitra, N.; Kanetsky, P.A.; Devaney, J.; Wing, M.R.; Reilly, M.; Shah, V.O.; Balakrishnan, V.S.; Guzman, N.J.; Girndt, M.; et al. CRIC Study Investigators. Association between albuminuria, kidney function, and inflammatory biomarker profile in CKD in CRIC. Clin. J. Am. Soc. Nephrol. 2012, 7, 1938–1946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kato, S.; Chmielewski, M.; Honda, H.; Pecoits-Filho, R.; Matsuo, S.; Yuzawa, Y.; Tranaeus, A.; Stenvinkel, P.; Lindholm, B. Aspects of immune dysfunction in end-stage renal disease. Clin. J. Am. Soc. Nephrol. 2008, 3, 1526–1533. [Google Scholar] [CrossRef] [Green Version]
- Tecklenborg, J.; Clayton, D.; Siebert, S.; Coley, S.M. The role of the immune system in kidney disease. Clin. Exp. Immunol. 2018, 192, 142–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Jager, D.J.; Grootendorst, D.C.; Jager, K.J.; van Dijk, P.C.; Tomas, L.M.; Ansell, D.; Collart, F.; Finne, P.; Heaf, J.G.; De Meester, J.; et al. Cardiovascular and noncardiovascular mortality among patients starting dialysis. JAMA 2009, 302, 1782–1789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dounousi, E.; Duni, A.; Naka, K.K.; Vartholomatos, G.; Zoccali, C. The Innate Immune System and Cardiovascular Disease in ESKD: Monocytes and Natural Killer Cells. Curr. Vasc. Pharmacol. 2021, 19, 63–76. [Google Scholar] [CrossRef]
- Boyette, L.B.; Macedo, C.; Hadi, K.; Elinoff, B.D.; Walters, J.T.; Ramaswami, B.; Chalasani, G.; Taboas, J.M.; Lakkis, F.G.; Metes, D.M. Phenotype, function, and differentiation potential of human monocyte subsets. PLoS ONE 2017, 12, e0176460. [Google Scholar] [CrossRef] [Green Version]
- Liakopoulos, V.; Jeron, A.; Shah, A.; Bruder, D.; Mertens, P.R.; Gorny, X. Hemodialysis-related changes in phenotypical features of monocytes. Sci. Rep. 2018, 8, 13964. [Google Scholar] [CrossRef] [Green Version]
- Ulrich, C.; Heine, G.H.; Seibert, E.; Fliser, D.; Girndt, M. Circulating monocyte subpopulations with high expression of angiotensin-converting enzyme predict mortality in patients with end-stage renal disease. Nephrol. Dial. Transplant. 2010, 25, 2265–2272. [Google Scholar] [CrossRef] [Green Version]
- Laroumanie, F.; Douin-Echinard, V.; Pozzo, J.; Lairez, O.; Tortosa, F.; Vinel, C.; Delage, C.; Calise, D.; Dutaur, M.; Parini, A.; et al. CD4+ T cells promote the transition from hypertrophy to heart failure during chronic pressure overload. Circulation 2014, 129, 2111–2124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winterberg, P.D.; Robertson, J.M.; Kelleman, M.S.; George, R.P.; Ford, M.L. T Cells Play a Causal Role in Diastolic Dysfunction during Uremic Cardiomyopathy. J. Am. Soc. Nephrol. 2019, 30, 407–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caprara, C.; Kinsey, G.R.; Corradi, V.; Xin, W.; Ma, J.Z.; Scalzotto, E.; Martino, F.K.; Okusa, M.D.; Nalesso, F.; Ferrari, F.; et al. The Influence of Hemodialysis on T Regulatory Cells: A Meta-Analysis and Systematic Review. Blood Purif. 2016, 42, 307–313. [Google Scholar] [CrossRef]
- Albany, C.J.; Trevelin, S.C.; Giganti, G.; Lombardi, G.; Scottà, C.F. Getting to the Heart of the Matter: The Role of Regulatory T-Cells (Tregs) in Cardiovascular Disease (CVD) and Atherosclerosis. Front. Immunol. 2019, 10, 2795. [Google Scholar] [CrossRef] [Green Version]
- Pahl, M.V.; Gollapudi, S.; Sepassi, L.; Gollapudi, P.; Elahimehr, R.; Vaziri, N.D. Effect of end-stage renal disease on B-lymphocyte subpopulations, IL-7, BAFF and BAFF receptor expression. Nephrol. Dial. Transplant. 2010, 25, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Tang, B.; Feng, Z.; Hao, W.; Hu, W. Decreased B lymphocytes subpopulations are associated with higher atherosclerotic risk in elderly patients with moderate-to-severe chronic kidney diseases. BMC Nephrol. 2021, 22, 396. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Tang, B.; He, G.; Feng, Z.; Hao, W.; Hu, W. B lymphocytes subpopulations are associated with cardiac remodeling in elderly patients with advanced chronic kidney disease. Exp. Gerontol. 2022, 163, 111805. [Google Scholar] [CrossRef] [PubMed]
- Backteman, K.; Ernerudh, J.; Jonasson, L. Natural killer (NK) cell deficit in coronary artery disease: No aberrations in phenotype but sustained reduction of NK cells is associated with low-grade inflammation. Clin. Exp. Immunol. 2014, 175, 104–112. [Google Scholar] [CrossRef]
- Ong, S.; Ligons, D.L.; Barin, J.G.; Wu, L.; Talor, M.V.; Diny, N.; Fontes, J.A.; Gebremariam, E.; Kass, D.A.; Rose, N.R.; et al. Natural killer cells limit cardiac inflammation and fibrosis by halting eosinophil infiltration. Am. J. Pathol. 2015, 185, 847–861. [Google Scholar] [CrossRef] [Green Version]
- Vacher-Coponat, H.; Brunet, C.; Lyonnet, L.; Bonnet, E.; Loundou, A.; Sampol, J.; Moal, V.; Dussol, B.; Brunet, P.; Berland, Y.; et al. Natural killer cell alterations correlate with loss of renal function and dialysis duration in uraemic patients. Nephrol. Dial. Transplant. 2008, 23, 1406–1414. [Google Scholar] [CrossRef] [Green Version]
- Ronco, C.; Haapio, M.; House, A.A.; Anavekar, N.; Bellomo, R. Cardiorenal syndrome. J. Am. Coll. Cardiol. 2008, 52, 152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronco, C.; McCullough, P.; Anker, S.D.; Anand, I.; Aspromonte, N.; Bagshaw, S.M.; Bellomo, R.; Berl, T.; Bobek, I.; Cruz, D.N.; et al. Acute Dialysis Quality Initiative (ADQI) consensus group. Cardio-renal syndromes: Report from the consensus conference of the acute dialysis quality initiative. Eur. Heart J. 2010, 31, 703–711. [Google Scholar] [CrossRef] [PubMed]
- Junho, C.V.C.; Trentin-Sonoda, M.; Panico, K.; Dos Santos, R.S.N.; Abrahão, M.V.; Vernier, I.C.S.; Fürstenau, C.R.; Carneiro-Ramos, M.S.H. Cardiorenal syndrome: Long road between kidney and heart. Heart Fail. Rev. 2022, 27, 2137–2153. [Google Scholar] [CrossRef] [PubMed]
- Rangaswami, J.; Bhalla, V.; Blair, J.E.A.; Chang, T.I.; Costa, S.; Lentine, K.L.; Lerma, E.V.; Mezue, K.; Molitch, M.; Mullens, W.; et al. Cardiorenal Syndrome: Classification, Pathophysiology, Diagnosis, and Treatment Strategies: A Scientific Statement from the American Heart Association. Circulation 2019, 139, e840–e878. [Google Scholar] [CrossRef]
- Schiattarella, G.G.; Sequeira, V.; Ameri, P. Distinctive patterns of inflammation across the heart failure syndrome. Heart Fail. Rev. 2021, 26, 1333–1344. [Google Scholar] [CrossRef]
- Putko, B.N.; Wang, Z.; Lo, J.; Anderson, T.; Becher, H.; Dyck, J.R.B.; Kassiri, Z.; Oudit, G.Y.; Alberta HEART Investigators. Circulating levels of tumor necrosis factor-alpha receptor 2 are increased in heart failure with preserved ejection fraction relative to heart failure with reduced ejection fraction: Evidence for a divergence in pathophysiology. PLoS ONE 2014, 9, e99495. [Google Scholar] [CrossRef] [Green Version]
- Markousis-Mavrogenis, G.; Tromp, J.; Ouwerkerk, W.; Devalaraja, M.; Anker, S.D.; Cleland, J.G.; Dickstein, K.; Filippatos, G.S.; van der Harst, P.; Lang, C.C.; et al. The clinical significance of interleukin-6 in heart failure: Results from the BIOSTAT-CHF study. Eur. J. Heart Fail. 2019, 21, 965–973. [Google Scholar] [CrossRef] [Green Version]
- Barisione, C.; Garibaldi, S.; Ghigliotti, G.; Fabbi, P.; Altieri, P.; Casale, M.K.; Spallarossa, P.; Bertero, G.; Balbi, M.; Corsiglia, L.; et al. CD14CD16 monocyte subset levels in heart failure patients. Dis. Markers 2010, 28, 115–124. [Google Scholar] [CrossRef]
- Wrigley, B.J.; Shantsila, E.; Tapp, L.D.; Lip, G.Y. CD14++CD16+ monocytes in patients with acute ischaemic heart failure. Eur. J. Clin. Investig. 2013, 43, 121–130. [Google Scholar] [CrossRef]
- Amir, O.; Spivak, I.; Lavi, I.; Rahat, M.A. Changes in the Monocytic Subsets CD14dimCD16+ and CD14++CD16− in Chronic Systolic Heart Failure Patients. Mediators Inflamm. 2012, 2012, 616384. [Google Scholar] [CrossRef] [Green Version]
- Rogacev, K.S.; Seiler, S.; Zawada, A.M.; Reichart, B.; Herath, E.; Roth, D.; Ulrich, C.; Fliser, D.; Heine, G.H. CD14++CD16+ monocytes and cardiovascular outcome in patients with chronic kidney disease. Eur. Heart J. 2011, 32, 84–92. [Google Scholar] [CrossRef] [Green Version]
- Duni, A.; Vartholomatos, G.; Balafa, O.; Ikonomou, M.; Tseke, P.; Lakkas, L.; Rapsomanikis, K.P.; Kitsos, A.; Theodorou, I.; Pappas, C.; et al. The Association of Circulating CD14++CD16+ Monocytes, Natural Killer Cells and Regulatory T Cells Subpopulations with Phenotypes of Cardiovascular Disease in a Cohort of Peritoneal Dialysis Patients. Front. Med. 2021, 20, 724316. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, C.; Heine, G.H.; Gerhart, M.K.; Köhler, H.; Girndt, M. Proinflammatory CD14+CD16+ monocytes are associated with subclinical atherosclerosis in renal transplant patients. Am. J. Transplant. 2008, 8, 103–110. [Google Scholar] [CrossRef]
- Rogacev, K.S.; Cremers, B.; Zawada, A.M.; Seiler, S.; Binder, N.; Ege, P.; Große-Dunker, G.; Heisel, I.; Hornof, F.; Jeken, J.; et al. CD14++CD16+ monocytes independently predict cardiovascular events: A cohort study of 951 patients referred for elective coronary angiography. J. Am. Coll. Cardiol. 2012, 60, 1512–1520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeng, Y.; Lim, P.S.; Wu, M.Y.; Tseng, T.; Chen, C.S.; Chen, H.P.; Wu, T. Proportions of Proinflammatory Monocytes Are Important Predictors of Mortality Risk in Hemodialysis Patients. Mediators Inflamm. 2017, 2017, 1070959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahid, F.; Lip, G.Y.H.; Shantsila, E. Role of Monocytes in Heart Failure and Atrial Fibrillation. J. Am. Heart Assoc. 2018, 7, e007849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, W.; Zhang, Z.; Fu, C.; Ma, G. Intermediate monocytes lead to enhanced myocardial remodelling in STEMI patients with diabetes. Int. Heart J. 2015, 56, 22–28. [Google Scholar] [CrossRef] [Green Version]
- Westermann, D.; Lindner, D.; Kasner, M.; Zietsch, C.; Savvatis, K.; Escher, F.; Von Schlippenbach, J.; Skurk, C.; Steendijk, P.; Riad, A.; et al. Cardiac inflammation contributes to changes in the extracellular matrix in patients with heart failure and normal ejection fraction. Circ. Heart Fail. 2011, 4, 44–52. [Google Scholar] [CrossRef] [Green Version]
- Vredevoe, D.L.; Widawski, M.; Fonarow, G.C.; Hamilton, M.; Martínez-Maza, O.; Gage, J.R. Interleukin-6 (IL-6) expression and natural killer (NK) cell dysfunction and anergy in heart failure. Am. J. Cardiol. 2004, 93, 1007–1011. [Google Scholar] [CrossRef]
- Selathurai, A.; Deswaerte, V.; Kanellakis, P.; Tipping, P.; Toh, B.; Bobik, A.; Kyaw, T. Natural killer (NK) cells augment atherosclerosis by cytotoxic-dependent mechanisms. Cardiovasc. Res. 2014, 102, 128–137. [Google Scholar] [CrossRef] [Green Version]
- Vaduganathan, M.; Ambrosy, A.P.; Greene, S.J.; Mentz, R.J.; Subacius, H.P.; Maggioni, A.P.; Swedberg, S.; Nodari, S.; Zannad, F.; Konstam, M.A.; et al. Predictive value of low relative lymphocyte count in patients hospitalized for heart failure with reduced ejection fraction: Insights from the EVEREST trial. Circ. Heart Fail. 2012, 5, 750–758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levey, A.S.; Cattran, D.; Friedman, A.; Miller, W.G.; Sedor, J.; Tuttle, K.; Kasiske, B.; Hostetter, T. Proteinuria as a surrogate outcome in CKD: Report of a scientific workshop sponsored by the National Kidney Foundation and the US Food and Drug Administration. Am. J. Kidney Dis. 2009, 54, 205–226. [Google Scholar] [CrossRef] [Green Version]
- Pattarabanjird, T.; Li, C.; McNamara, C. B cells in Atherosclerosis: Mechanisms and Potential Clinical Applications. JACC Basic Transl. Sci. 2021, 6, 546–563. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, N.; Noma, T.; Ishihara, Y.; Miyauchi, Y.; Takabatake, W.; Oomizu, S.; Yamaoka, G.; Ishizawa, M.; Namba, T.; Murakami, K.; et al. Prognostic value of circulating regulatory T cells for worsening heart failure in heart failure patients with reduced ejection fraction. Int. Heart J. 2014, 55, 271–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bansal, S.S.; Ismahil, M.A.; Goel, M.; Zhou, G.; Rokosh, G.; Hamid, T.; Prabhu, S.D. Dysfunctional and Proinflammatory Regulatory T-Lymphocytes Are Essential for Adverse Cardiac Remodeling in Ischemic Cardiomyopathy. Circulation 2019, 139, 206–221. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Xia, N.; Cheng, X. Regulatory T Cells in Chronic Heart Failure. Front. Immunol. 2021, 12, 732794. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All Patients (N = 63) | CRS Patients (N = 39) | CKD Patients (N = 24) | p-Value * | |
|---|---|---|---|---|
| Age (years) | 72 ± 10 | 66 ± 10 | 0.01 | |
| DM, N (%) | 31 (47.7) | 22 (56.4) | 9 (37.5) | 0.15 |
| eGFR (mL/min/1.73 m2) | 35 ± 15 | 37 ± 14 | 33 ± 16 | 0.18 |
| UPCR (g protein/g creatinine) | 0.39 (0.12–1.13) | 0.19 (0.10–0.52) | 1.03 (0.17–2.09) | 0.02 |
| Hemoglobin (g/dL) | 12.3(11.0–14.4) | 11.8 (11.0–14.4) | 13 (11.1–14.6) | 0.78 |
| Uric Acid (mg/dL) | 7.0 (5.9–8.4) | 6.9 (5.5–7.8) | 7.9 (6.05–8.9) | 0.17 |
| ESR (mm/h) | 33 ± 18 | 33 ± 19 | 32 ± 15 | 0.87 |
| CRP (mg/L) | 4 (2–8) | 4 (2–8) | 4 (3–8) | 0.92 |
| Glucose (mg/dL) | 107 (93–137) | 120 (98–160) | 99 (91–113) | 0.007 |
| Albumin (g/dL) | 4 (3.7–4.4) | 3.9 (3.7–4.3) | 4.2 (3.7–4.5) | 0.26 |
| Total Proteins (g/dL) | 7.0 (6.4–7.6) | 6.9 (6.3–7.5) | 7.2 (6.7–7.6) | 0.17 |
| Total cholesterol (mg/dL) | 161 ± 44 | 147 ± 40 | 184 ± 41 | 0.001 |
| Triglycerides (mg/dL) | 125 (94–178) | 104 (77–155) | 150 (118–216) | 0.006 |
| LDL cholesterol (mg/dL) | 94 ± 40 | 84 ± 35 | 110 ± 44 | 0.01 |
| HDL cholesterol (mg/dL) | 38 ± 10 | 37 ± 11 | 40 ± 10 | 0.29 |
| Ferritin (ng/mL) | 76 (43–114) | 63 (36–115) | 88 (58–112) | 0.31 |
| Calcium (mg/dL) | 9.4 (9.0–9.7) | 9.4 (9.1–9.7) | 9.4 (8.7–9.6) | 0.16 |
| Phosphorus (mg/dL) | 3.7 ± 0.7 | 3.7 ± 0.6 | 3.7 ± 0.8 | 0.83 |
| iPTH (pg/mL) | 130 (86–235) | 134 (92–176) | 128 (62–281) | 0.55 |
| hsTNI (ng/mL) | / | 25.3 (16.4–42.4) | / | / |
| BNP (pg/mL) | / | 324 (184–797) | / | / |
| Statins N (%) | 49 (79.0) | 32 (84.2) | 17 (70.8) | 0.22 |
| ACEI/ARB N (%) | 30 (48.4) | 14 (36.8) | 16 (66.7) | 0.02 |
| B-blockers N (%) | 44 (71) | 34 (89.5) | 10 (41.7) | 0.000 |
| All Patients (N = 63) | CRS Patients (N = 39) | CKD Patients (N = 24) | p-Value * | |
|---|---|---|---|---|
| WBC (N) | 7730 (IQR 6224–9495) | 8360 (IQR 6730–9940) | 7330 (IQR 6070–8830) | 0.15 |
| Monocytes (N) | 500 (IQR 400–650) | 600 (IQR 400–700) | 500 (IQR 400–600) | 0.06 |
| Monocytes (%) | 6.5 (5.4–7.9) | 6.5 (IQR 5.4–8.1) | 6.6 (IQR 5.3–7.8) | 0.64 |
| CD14++CD16- (N) | 427 ± 167 | 450 ± 184 | 391 ± 132 | 0.14 |
| CD14++CD16- (%) | 81.4 ± 8.9 | 80.6 ± 10 | 82.6 ± 6.9 | 0.35 |
| CD14++CD16+ (N) | 38 (IQR 22–62) | 41 (IQR 24–78) | 35 (IQR 18–43) | 0.04 |
| CD14++CD16+ (%) | 7.4 (IQR 5.4–11.2) | 8 (IQR 5.6–12.0) | 7.3 (IQR 4.7–9.6) | 0.30 |
| CD14+CD16++ (N) | 25 (IQR 14–35) | 22 (IQR 12–36) | 25 (IQR 19–32) | 0.80 |
| CD14+CD16++ (%) | 4.6 (IQR 3.0–6.7) | 4.2 (IQR 2.7–6.6) | 5.1 (IQR 4.0–6.7) | 0.14 |
| Lymphocytes (N) | 1699 ± 658 | 1557 ± 691 | 1920 ± 545 | 0.03 |
| Lymphocytes (%) | 21.3 ± 8.7 | 18.7 ± 8.3 | 25.3 ± 8.0 | 0.002 |
| T-lymphocytes (N) | 1320 ± 500 | 1227 ± 510 | 1465 ± 455 | 0.06 |
| T-lymphocytes (%) | 79.6 ± 9.7 | 81.7 ± 8.7 | 76.3 ± 10.3 | 0.03 |
| B-lymphocytes (N) | 75 (IQR 37–140) | 68 (IQR 31–104) | 87 (IQR 58–163) | 0.08 |
| B-lymphocytes (%) | 4.7 (2.9–8.3) | 4.2 (IQR 2.2–9.0) | 5.1 (IQR 3.4–7.9) | 0.57 |
| NK cells (N) | 182 (124–328) | 148 (IQR 103–258) | 324 (IQR 179–368) | 0.001 |
| NK cells (%) | 1.7 (IQR 8.2–18.3) | 10.7 (IQR 7.1–16.6) | 16.5 (IQR 11.2–19.6) | 0.01 |
| CD4+ T-Cells (N) | 787 ± 312 | 732 ± 308 | 873 ± 304 | 0.08 |
| CD4+ T-cells (%) | 47.5 ± 10.6 | 48.6 ± 10.4 | 45.7 ± 10.9 | 0.30 |
| CD8+ T-cells (N) | 508 (IQR 353–750) | 411 (IQR 224–720) | 585 (IQR 447–786) | 0.14 |
| CD8+ T-cells (%) | 29.9 (IQR 23.5–37.9) | 28.5 (IQR 23.3–38.0) | 31.5 (IQR 24.4–36.8) | 0.73 |
| Tregs (%) | 2.4 (IQR 1.7–3.3) | 2.7 (IQR 2.0–3.9) | 2.0 (IQR 1.6–2.6) | 0.03 |
| T Regs (N) | 37 (IQR 25–51) | 36 (IQR 24–49) | 40 (IQR 26–61) | 0.94 |
| Monocytes (N) | Lymphocytes (N) | CD8+ T-cells (%) |
| ESR r = 0.485 p = 0.00 | eGFR r = 0.427 p = 0.007 | HDL cholesterol r = 0.333, p = 0.04 |
| CRP r = 0.402 p = 0.001 | ||
| CD14++CD16- (N) | T-lymphocytes (N) | B-lymphocytes (N) |
| ESR r = 0.353, p = 0.030 | eGFR r = 0.425 p = 0.007 | Total cholesterol r = −0.336 p = 0.03 |
| LDL cholesterol r = −0.388, p = 0.01 | ||
| CD14++CD16+ (N) | CD4+ T-cells (N) | B-lymphocytes (%) |
| ESR r = 0.378, p = 0.020 | eGFR r = 0.439 p = 0.005 | Total cholesterol r = −0.470 p = 0.003 |
| CRP r = 0.476 p = 0.002 | LDL cholesterol r = −0.441, p = 0.0005 | |
| CD14++CD16+ (%) | CD8+ T-cells (N) | Tregs (%) |
| CRP r = 0.319, p = 0.040 | HDL cholesterol r = 0.318, p = 0.04 | Triglycerides r = −0.377, p = 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duni, A.; Kitsos, A.; Bechlioulis, A.; Markopoulos, G.S.; Lakkas, L.; Baxevanos, G.; Mitsis, M.; Vartholomatos, G.; Naka, K.K.; Dounousi, E. Differences in the Profile of Circulating Immune Cell Subsets in Males with Type 2 Cardiorenal Syndrome versus CKD Patients without Established Cardiovascular Disease. Biomedicines 2023, 11, 1029. https://doi.org/10.3390/biomedicines11041029
Duni A, Kitsos A, Bechlioulis A, Markopoulos GS, Lakkas L, Baxevanos G, Mitsis M, Vartholomatos G, Naka KK, Dounousi E. Differences in the Profile of Circulating Immune Cell Subsets in Males with Type 2 Cardiorenal Syndrome versus CKD Patients without Established Cardiovascular Disease. Biomedicines. 2023; 11(4):1029. https://doi.org/10.3390/biomedicines11041029
Chicago/Turabian StyleDuni, Anila, Athanasios Kitsos, Aris Bechlioulis, Georgios S. Markopoulos, Lampros Lakkas, Gerasimos Baxevanos, Michail Mitsis, George Vartholomatos, Katerina K. Naka, and Evangelia Dounousi. 2023. "Differences in the Profile of Circulating Immune Cell Subsets in Males with Type 2 Cardiorenal Syndrome versus CKD Patients without Established Cardiovascular Disease" Biomedicines 11, no. 4: 1029. https://doi.org/10.3390/biomedicines11041029